TITLE: Antiemetics For Adults Experiencing Opioid-Induced Nausea: A Review of Clinical and Cost-Effectiveness, Benefits and Harms, and Guidelines DATE: 09 April 2014 CONTEXT AND POLICY ISSUES The side effects of opioid analgesia include sedation, cognitive impairment, constipation, and nausea and vomiting. Opioid-induced nausea and vomiting occurs in many clinical settings, the most studied of which is postoperative nausea and vomiting (PONV). 1 Postoperative opioids are one of the primary drivers of PONV, meaning opioid-based analgesia can often achieve pain control at the expense of nausea and vomiting. 2,2 PONV is the most common reason for dissatisfaction with opioid-based analgesia. 3 There are several risk factors associated with an increased incidence of PONV. These risk factors include female sex, history of PONV, nonsmoking, younger age, and possibly American Society of Anesthesiologists (ASA) physical status. 1 The type of surgery also presents different risks for PONV although this may be related to the associated length of anesthesia and dose of opioid. 1 The Apfel score is a simplified risk score based on four risk factors: female sex, history of PONV, nonsmoking status and use of postoperative opioids. 4 The emetogenic effects of opioids can be both treated and prevented with antiemetics. 5 There are many classes of effective antiemetics including 5HT 3 receptor antagonists, NK-1 receptor antagonists, corticosteroids, butyrophenones, antihistamines, anticholinergic and phenothiazines. 1 Ondansetron is the most well studied 5HT 3 receptor antagonist and is considered by some to be the ‘gold standard’ to which other antiemetics are compared. 1 Dimenhydrinate is an antihistamine commonly used as an antiemetic. 1 The purpose of this report is to retrieve and review existing evidence comparing the efficacy of different antiemetics for treatment of opioid-induced nausea. This report also aims to retrieve and review the evidence regarding the clinical effectiveness, benefits and harms, cost- effectiveness and evidence-based guidelines regarding the use of dimenhydrinate and ondansetron for adult patients experiencing opioid-induced nausea. Disclaimer: The Rapid Response Service is an information service for those involved in planning and providing health care in Canada. Rapid responses are based on a limited literature search and are not comprehensive, systematic reviews. The intent is to provide a list of sources of the best evidence on the topic that CADTH could identify using all reasonable efforts within the time allowed. Rapid responses should be considered along with other types of information and health care considerations. The information included in this response is not intended to replace professional medical advice, nor should it be construed as a recommendation for or against the use of a particular health technology. Readers are also cautioned that a lack of good quality evidence does not necessarily mean a lack of effectiveness particularly in the case of new and emerging health technologies, for which little information can be found, but which may in future prove to be effective. While CADTH has taken care in the preparation of the report to ensure that its contents are accurate, complete and up to date, CADTH does not make any guarantee to that effect. CADTH is not liable for any loss or damages resulting from use of the information in the report. Copyright: This report contains CADTH copyright material and may contain material in which a third party owns copyright. This report may be used for the purposes of research or private study only. It may not be copied, posted on a web site, redistributed by email or stored on an electronic system without the prior written permission of CADTH or applicable copyright owner. Links: This report may contain links to other information available on the websites of third parties on the Internet. CADTH does not have control over the content of such sites. Use of third party sites is governed by the owners’ own terms and conditions.
Transcript
TITLE: Antiemetics For Adults Experiencing Opioid-Induced Nausea: A Review of
Clinical and Cost-Effectiveness, Benefits and Harms, and Guidelines DATE: 09 April 2014 CONTEXT AND POLICY ISSUES The side effects of opioid analgesia include sedation, cognitive impairment, constipation, and nausea and vomiting. Opioid-induced nausea and vomiting occurs in many clinical settings, the most studied of which is postoperative nausea and vomiting (PONV).1 Postoperative opioids are one of the primary drivers of PONV, meaning opioid-based analgesia can often achieve pain control at the expense of nausea and vomiting.2,2 PONV is the most common reason for dissatisfaction with opioid-based analgesia.3 There are several risk factors associated with an increased incidence of PONV. These risk factors include female sex, history of PONV, nonsmoking, younger age, and possibly American Society of Anesthesiologists (ASA) physical status.1 The type of surgery also presents different risks for PONV although this may be related to the associated length of anesthesia and dose of opioid.1 The Apfel score is a simplified risk score based on four risk factors: female sex, history of PONV, nonsmoking status and use of postoperative opioids.4 The emetogenic effects of opioids can be both treated and prevented with antiemetics.5 There are many classes of effective antiemetics including 5HT3 receptor antagonists, NK-1 receptor antagonists, corticosteroids, butyrophenones, antihistamines, anticholinergic and phenothiazines.1 Ondansetron is the most well studied 5HT3 receptor antagonist and is considered by some to be the ‘gold standard’ to which other antiemetics are compared.1 Dimenhydrinate is an antihistamine commonly used as an antiemetic.1 The purpose of this report is to retrieve and review existing evidence comparing the efficacy of different antiemetics for treatment of opioid-induced nausea. This report also aims to retrieve and review the evidence regarding the clinical effectiveness, benefits and harms, cost-effectiveness and evidence-based guidelines regarding the use of dimenhydrinate and ondansetron for adult patients experiencing opioid-induced nausea.
Disclaimer: The Rapid Response Service is an information service for those involved in planning and providing health care in Canada. Rapid responses are based on a limited literature search and are not comprehensive, systematic reviews. The intent is to provide a list of sources of the best evidence on the topic that CADTH could identify using all reasonable efforts within the time allowed. Rapid responses should be considered along with other types of information and health care considerations. The information included in this response is not intended to replace professional medical advice, nor should it be construed as a recommendation for or against the use of a particular health technology. Readers are also cautioned that a lack of good quality evidence does not necessarily mean a lack of effectiveness particularly in the case of new and emerging health technologies, for which little information can be found, but which may in future prove to be effective. While CADTH has taken care in the preparation of the report to ensure that its contents are accurate, complete and up to date, CADTH does not make any guarantee to that effect. CADTH is not liable for any loss or damages resulting from use of the information in the report. Copyright: This report contains CADTH copyright material and may contain material in which a third party owns copyright. This report may be used for the purposes of research or private study only. It may not be copied, posted on a web site, redistributed by email or stored on an electronic system without the prior written permission of CADTH or applicable copyright owner. Links: This report may contain links to other information available on the websites of third parties on the Internet. CADTH does not have control over the content of such sites. Use of third party sites is governed by the owners’ own terms and conditions.
RESEARCH QUESTIONS 1. What is the comparative clinical effectiveness of different anti-emetics for the treatment of
adult patients experiencing opioid-induced nausea? 2. What is the clinical effectiveness of dimenhydrinate and ondansetron as antiemetics for
adult patients experiencing opioid-induced nausea? 3. What are the benefits and harms of using dimenhydrinate and ondansetron as antiemetics
for adult patients experiencing opioid-induced nausea? 4. What is the cost-effectiveness of using dimenhydrinate and ondansetron as antiemetics for
adult patients experiencing opioid-induced nausea? 5. What are the guidelines associated with the use of dimenhydrinate and ondansetron as
antiemetics for adult patients experiencing opioid-induced nausea? KEY FINDINGS While antiemetic comparative studies were identified, evidence to support an overall clinically superior antiemetic was lacking. The evidence presented in this report supports the use of dimenhydrinate and ondansetron as antiemetics for the treatment and prevention of opioid-induced nausea, however evidence for consistent quantitative clinical effectiveness was not identified. The focus on patients with risk factors for postoperative nausea and vomiting (PONV) and the lack of quantitative agreement between studies suggests that the findings may not be directly applicable to alternative clinical settings. Broad consensus was identified regarding common adverse events of ondansetron including headache, drowsiness and dizziness. While no serious adverse events were reported, the identified trials lack the statistical power for the detection of possible rare adverse events. There were no cost-effectiveness studies identified examining the use of dimenhydrinate or ondansetron. Two guidelines were identified that include evidence-based recommendations for dimenhydrinate and ondansetron dose and timing for the treatment and prevention of PONV. Additionally, identified guidelines and randomized controlled trials (RCTs) provide evidence for antiemetic combinations with cumulative beneficial effects, including combinations with ondansetron. METHODS Literature Search Strategy A limited literature search was conducted on key resources including PubMed, The Cochrane Library (2014, Issue 3), University of York Centre for Reviews and Dissemination (CRD) databases, Canadian and major international health technology agencies, as well as a focused Internet search. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2009 and March 12, 2014.
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 2
Selection Criteria and Methods One reviewer screened the titles and abstracts of the retrieved publications and evaluated the full-text publications for the final article selection, according to selection criteria presented in Table 1. Table 1: Selection Criteria Population
Clinical Effectiveness (emetic symptom reduction) Health Benefits and Adverse events Cost-effectiveness Guidelines
Study Designs
Health Technology Assessments (HTA)/ Systematic review (SR)/Meta-analysis (MA); Randomized controlled trials (RCTs); Economic Evaluations; Non-randomized studies; and Guidelines
Exclusion Criteria Studies were excluded if they did not meet the selection criteria, were duplicates or were published prior to 2009. When examining which antiemetic is most clinically effective, evidence from placebo-controlled trials was excluded for ease of direct and accurate comparison between interventions. Placebo controlled trial studies were only included when dimenhydrinate or ondansetron were being investigated to address questions 2 and 3. Critical Appraisal of Individual Studies The quality of the RCTs included in this report was assessed using the Downs and Black checklist.6 Strengths and limitations were described narratively and tabulated instead of assigning a numerical score for each study. Critical appraisal of guidelines used the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument.7 Scope and purpose, stakeholder involvement, rigor of development, clarity and presentation, applicability and editorial independence were the domains of the AGREE instrument evaluated in this report. The strengths and limitations of the guidelines were described narratively instead of assigning an AGREE numerical score. SUMMARY OF EVIDENCE Quantity of Research Available The literature search strategy identified 268 articles. Following screening titles and available abstracts, 31 full text articles were retrieved. One additional potentially relevant article was identified in the grey literature. Upon review, two guidelines and 16 RCTs and one retrospective case-control study (RCS) met the selection criteria (Table 1). The excluded 13 studies consisted
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 3
of seven that examined an irrelevant intervention, two were correspondence, two examined an irrelevant outcome, one was an editorial and one was a duplicate publication. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart describes the selection procedure of the included studies of this review (Appendix 1). No systematic reviews, meta-analyses or cost-effectiveness studies met the inclusion criteria. Summary of Study Characteristics Clinical effectiveness Included RCT and RCS characteristics are tabulated in Appendix 2, Table A2.1. Study design Sixteen RCTs3,4,8-21 and one RCS22 were identified as meeting the selection criteria (Table 1). Population All identified studies examined adult patients recently anesthetized for a surgical procedure and then administered opioid analgesia. The identified RCTs and RCS examine PONV resulting from specified surgical procedures.3,4,8-22 The surgical procedures examined in each RCT and RCS is tabulated in Appendix 2 Table A2.1. In ten of the identified RCTs, patient inclusion criteria specified certain established risk factors for PONV,3,4,12-15,17,18,20,21 while the RCS did not specify risk factors in the patient inclusion criteria.22 As tabulated in Appendix 2 Table A2.1, specific risk factors of inclusion criteria were female4,17 and both female and non-smoker.3,12-15,18,20,21 ASA physical status was part of the inclusion criteria of 13 identified RCTs.3,4,10-12,14-21 American Society of Anesthesiologists (ASA) physical status I and II includes normal healthy patients and patients with mild systemic disease and are included in nine RCTs,3,4,10,12,14-18 while ASA physical status III (patients with a non-life-threatening severe systemic disease), are included in addition to patients with ASA physical status I and II in four RCTs.11,19-21 Intervention and Comparators The RCTs and RCS examine comparative antiemetic effectiveness for treatment and prevention of PONV after analgesia with remifentanil,8,11-13,16,19,21 fentanyl,3,8-19 oxycodone,9,21 morphine,4,9,11,14,17,18,22 tramadol,19 hydromorphone,20 and/or piritramide21. Twelve of the RCTs examine antiemetic effectiveness for treatment and prevention of PONV during patient controlled analgesia (PCA), specifically with the opioids fentanyl,3,8,9,12,13,15,16 morphine,14,17,18 tramadol,19 and hydromorphone.20 One study was identified that specifically examined the effectiveness of dimenhydrinate for the prevention of PONV.17 Dimenhydrinate was also used as a rescue antiemetic in three included studies.11,19,21 Ondansetron was used for the treatment and/or prevention of PONV in 13 studies.3,4,11,12,14,14-16,18-22 In three studies, while ondansetron is used as a combination antiemetic, it is used in all study groups and therefore the effectiveness is not being tested.11,16,22 In five RCTs ondansetron was used in combination with other antiemetics including dexamethasone,11,14,16,22 haloperidol,11,21 aprepitant,22 metoclopramide,22 diphenhydramine,22
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 4
procholoperazine22 and/or midazolam.21 The effectiveness of ondansetron in the treatment and/or prevention of PONV is examined in comparison to palonosetron,3,12 haloperidol,14 ramosetron,15,20 midazolam,18 metoclopramide,19 pentazocine,4 and placebo21 in the included studies. Seven of the studies administered antiemetics through PCA, delivering analgesics and antiemetics simultaneously.3,8,12,13,15,16,18 No identified report compared different antiemetic doses. Interventions and comparators, including antiemetic doses, of the identified studies are tabulated in Appendix 2 Table A2.1. Outcomes The most relevant outcomes examined in the included RCTs and RCS are PONV occurrence,3,8-22 nausea score,3,4,8,9,13,16,20-22 and requirement for antiemetic rescue.3,8-14,14-
16,19,20,22 Other outcomes reported in the identified studies are pain scores,3,4,8-10,13-22 opioid consumption,3,8,9,11,17-20 sedation score,14,17,18,21 time to first antiemetic rescue,11 volume of IV fluids,11 length of hospital stay,11 patient overall satisfaction,22 vomiting score,4,21 respiratory depression,22 pruritus score,4 PONV prophylaxis quality,21 blood pressure,4 heart rate,4 respiratory rate,4 oxygen saturation,4 shivering score,4 plasma concentrations of ondansetron and O-demethyltramadol,19 incidence of PCA discontinuation16 and recovery time.14 The pain, nausea and vomiting scores were based on subjective scales and reported by the patient or determined by an attending investigator or nurse.3,4,8-10,13-22 A requirement for antiemetic rescue was recorded upon a predefined condition, when treatment or prophylaxis of PONV was failing, when nausea score was above a certain threshold, or by patient request. Patients were then given additional antiemetic that was not part of the study.3,8-14,14-16,19,20,22 Adverse events, other than those specified as an outcome, were mentioned in 14 studies.3,4,8,9,11-18,20,21 The frequency and type of adverse event was quantified in nine studies.3,4,8,9,12,13,15,16,18 One study quantified adverse effects of ondansetron against placebo.18 No identified studies examined the adverse effects of dimenhydrinate. Guidelines and Recommendations Included guideline characteristics are tabulated in Appendix 2, Table A2.2. Origin of reports The most recent guidelines identified are from the Society of Ambulatory Anesthesiology (SAA) in the United States. These consensus guidelines were published in 2014.1 The other identified guidelines were published in English in 2010 in Germany.5 No Canadian guidelines were identified. Interventions Both guidelines focus on antiemetic use for treatment and prevention of PONV. The two guidelines included in this report do not distinguish between PONV resulting from different surgical procedures. The identified guidelines have recommendations for the treatment and prevention of PONV including doses and timing of antiemetics.1,5 Both guidelines reported a level of evidence for dose and timing of both dimenhydrinate and ondansetron for the prevention of PONV.1,5 One guideline1 provided a treatment algorithm, although not explicitly linked to evidence, that includes dimenhydrinate and ondansetron in the treatment and prevention of
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 5
PONV. Both guidelines also provide a level of evidence for antiemetic drug combinations for PONV.1,5 Grading of recommendations and levels of evidence The consensus guidelines from the Society for Ambulatory Anesthesiology have levels of evidence rated A to D with subcategories,1 while the guidelines from Germany published in 2010 have recommendations graded A to D and levels of evidence rated 1 to 4. The grading systems used to assign levels of evidence and strength of recommendations for the included guidelines are summarized in Appendix 3. Summary of Critical Appraisal While the quality of the included RCTs and RCS varies, many of these studies were of a relatively high standard. All 17 of the identified studies focused on antiemetic use in PONV prevention and treatment.3,4,8-22 Eight RCTs had a CONSORT diagram describing patient disposition,3,4,8,9,11,14,17,19 all seventeen studies tabulated patient characteristics,3,4,8-22 and thirteen discussed study limitations.3,4,8,9,12-17,19,21,22 Methods such as allocation concealment,3,4,8,9,17,19,21 role of blinded investigators,3,4,8,9,11-17,19-21 and randomization3,4,8,9,11,13-
17,19,21 were described in seven, fourteen and twelve RCTs, respectively. Fifteen RCTs clearly defined patient eligibility,3,4,8,9,11-21 thirteen clearly defined the study interventions3,4,8,9,11-13,15-
18,20,21 and fourteen had clearly defined outcomes.3,4,8,9,11-13,15-18,20-22 Adverse events were discussed to varying degrees in the identified studies. Seven studies discussed adverse events,3,9-11,14,20,21 while another seven discussed and quantified the adverse events associated with the intervention.4,8,12,13,15,16,18 While many of the RCTs had a small number of patients and all were a single center study,3,4,8-22 fourteen RCTs did a power calculation to ensure an adequate sample size based on detecting a minimum difference between the interventions.4,8,9,11-21 A COI statement was present in eight of the included studies. 3,8,9,11,14,16,20,22 A summary of critical appraisal of RCTs and RCS using the Downs and Black checklist6 is available in Appendix 4. The two included guidelines have different strengths and limitations.1,5 One guideline has levels of evidence and grades of recommendations clearly defined, however many graded recommendations are unclear. These guidelines, published in Germany, do not describe a systematic literature search, nor describe representative stakeholders in its development.5 The consensus guidelines from the Society for Ambulatory Anesthesiology (SAA) published in 2014 lack graded recommendations and a summary of limitations. These recommendations contain evidence for doses and timing for 18 antiemetics for the treatment and prevention of PONV. Explicit scope, goals, target audience and literature exclusion criteria are strengths of these consensus guidelines.1 Both guidelines provide a conflict of interest (COI) statement.1,5 A summary of the identified guideline strengths and limitations is provided in Appendix 5. Summary of Findings The statistically significant findings and author’s conclusions of the included RCTs and RCS are summarized in Appendix 6. There is significant heterogeneity in the included studies in regard to interventions, comparators and outcomes therefore findings are reported here as statistically significant or not, without quantitative comparisons between studies.
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 6
Eleven identified studies included the use of ondansetron as an antiemetic for the treatment and prevention of PONV.3,4,11,12,14,14-16,19-22 The dose and timing of ondansetron administration used in these studies is summarized in Appendix 2 Table A2.1. Three studies reported PONV prevention outcomes comparing ondansetron to placebo.18,19,21 Two studies compared ondansetron alone to placebo and both demonstrated a statistically significant reduction in PONV,18,19 one found a reduction in nausea,18 while the other found a reduction in vomiting.19 The third, Dagtekin et al., 2009 found that when combined with intraoperative midazolam and postoperative haloperidol, the addition of postoperative ondansetron compared to placebo resulted in a statistically significant reduction in PONV, vomiting and pain scores.21 Five included studies examined the antiemetic effectiveness of ondansetron in combination with various additional antiemetics.11,14,16,21,22 Three RCTs and one RCS, examined the effect of ondansetron with dexamethasone.11,14,16,22 Two RCTs found that the addition of dexamethasone resulted in a statistically significant reduction in PONV,14,16 and one found a reduction in antiemetic rescue requirement.14 One RCT examined antiemetic effectiveness of ondansetron alone compared to ondansetron with dexamethasone and compared to ondansetron with haloperidol and dexamethasone.11 The addition of dexamethasone resulted in decreased nausea occurrence, while the addition of haloperidol to the combination had a statistically significant improvement in nausea occurrence, vomiting occurrence, the requirement for rescue antiemetics, time to first antiemetic rescue, and the consumption of both opioid and IV fluids as compared to ondansetron alone.11 No statistically significant differences were found between haloperidol with dexamethasone and ondansetron with dexamethasone.14 The included RCS demonstrated that a combination of ondansetron and dexamethasone significantly reduces PONV occurrence when aprepitant is included as compared to either metoclopramide, diphenhydramine, or prochlorperazine although the exact comparator was unclear.22 All identified RCTs found antiemetic effectiveness of dexamethasone with ondansetron is superior to ondansetron alone.11,14,16 Furthermore the further addition of certain antiemetics to ondansetron and dexamethasone may have cumulative benefits in PONV outcomes.11,22 The results for antiemetic combinations with ondansetron from the identified RCTs are summarized in Appendix 8. The effectiveness of ondansetron in the treatment and/or prevention of PONV is examined in comparison to palonosetron,3,12 haloperidol,14 ramosetron,15,20 midazolam,18 metoclopramide,19 and pentazocine4 in the identified studies. Two studies comparing the palonosetron and ondansetron in the prevention of PONV included similar high-risk PONV patients, and similar doses and timing of antiemetics and the same opioid.3,12 The studies differed in the surgery performed. Both studies found statistically significant differences favouring the use of palonosetron for the prevention of PONV including reduced vomiting occurrence,3,12 reduced PONV,3 nausea severity,3 and the use of rescue antiemetics.3 One study concluded the two antiemetics had similar preventative effects on PONV,12 while the authors of the other RCT concluded that palonosetron was superior to ondansetron in high-risk patients receiving fentanyl-based IV-PCA.3 One RCT investigated a comparison of dexamethasone with haloperidol and dexamethasone with ondansetron. The two combinations demonstrated no statistically significant differences in PONV related outcomes.14 Two RCTs found statistically significant superiority of ramosetron as compared to ondansetron.15,20 One of these RCTs reported a significant difference between 24 and 48 hours post-surgery where no PONV was observed in 98.3% with ramosetron and 86.7% with ondansetron, while the other RCT in the same time interval observed no PONV in 54% with ramosetron and 24% with ondansetron.15,20
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 7
The latter RCT examining ramosetron and ondansetron also observed decreased nausea scores and less PONV in the intervals 2-6 hours and 6-24 hours post-surgery.20 Also observed in this study was less rescue antiemetic requirement 24-48 hours post-surgery and higher patient overall satisfaction with ramosetron.20 A comparison of ondansetron with midazolam was investigated in one RCT.18 No statistically significant differences in PONV related outcomes were found, however midazolam had a higher incidence of a mild sedative effect.18 A comparison of ondansetron to metoclopramide revealed no statistically significant differences between the two antiemetics in PONV outcomes in this study.19 A comparison study of pentazocine and ondansetron demonstrated a statistically significant difference in pruritus score favouring pentazocine, without any additional differences in PONV outcomes.4 Two studies have suggested antiemetic superiority of palonosetron and two studies suggested antiemetic superiority of ramosetron over ondansetron in the prevention of PONV.3,12,15,20 One study examined the antiemetic efficacy of diphenhydramine.17 The author’s statistical analysis of the results did not test the significance of the difference between the placebo 54.2% nausea occurrence, and diphenhydramine, 30.6% nausea occurrence. A statistically significant decrease in nausea occurrence was reported when a combination of diphenhydramine and metoclopramide were used as PONV prophylaxis as compared to single agents diphenhydramine, metoclopramide, or placebo.17 Other comparative RCTs for the treatment and prevention of PONV included in this review examine ramosetron and palonosetron,8 ramosetron with dexamethasone and ramosetron alone,9,13 and naloxone and metoclopramide.10 Ramosetron was more effective at reducing PONV occurrence, pain scores and nausea scores than palonosetron.8 A combination of ramosetron and dexamethasone was more effective at reducing the occurrence of nausea,9,13 the occurrence of vomiting,9,13 pain scores,9 nausea scores,9 the requirement of rescue antiemetics,9 and opioid consumption than ramosetron alone.9 One RCT focused on acute PONV treatment and reported the superiority of naloxone as compared to metoclopramide in the complete response (end of PONV) in 5 min.10 None of the identified studies reported any statistically significant differences in regards to antiemetic related adverse events. The identified RCS and one RCT did not mention any adverse event related information,19,22 eight RCTs discussed at least one aspect of adverse events without quantification,3,9-11,14,17,20,21 and seven RCTs quantified the occurrence of adverse events.4,8,12,13,15,16,18 The most commonly reported adverse events included headache,8,12,13,15,16 dizziness,4,8,12,13,15,16,18 and drowsiness.8,12,13,16 The single highest reported adverse event was a 30% incidence of dizziness reported by Kim et al. (2013) in the ondansetron group which was not statistically significantly different than the incidence of dizziness in the palonosetron group.23 One concern raised by authors in two RCTs was the potential for the corticosteroid dexamethasone to interfere with wound healing.9,13 In one of these reports the authors conclusions was, ”More large prospective series are needed to ascertain whether corticosteroid use is associated with increased risks for wound complications in patients undergoing TKA.” One RCT excluded one patient in a study arm of 32 patients receiving dexamethasone due to post-operative dehiscence of the suture line.11 No studies were identified that examined the cost-effectiveness of antiemetics. One RCT stated that the combination of haloperidol with dexamethasone was more cost-effective than ondansetron with dexamethasone, however the statement was not based upon a cost-effectiveness analysis.14
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 8
Relevant recommendations of the included guidelines are summarized in Appendix 7. The levels of evidence and grades of recommendations mentioned below are described in Appendix 3. The two identified guidelines have recommendations for the dose and timing of antiemetic administration for the treatment and prevention of PONV.1,5 However, the German guidelines found grade D evidence to state that antiemetics with grade A proven efficacy for PONV can essentially also be considered effective for the indication “opioid-induced nausea and opioid-induced vomiting”.5 Both guidelines contain recommendations for dimenhydrinate and ondansetron for PONV but do not suggest any antiemetic superiority. There is consensus in the two guidelines that the highest quality of evidence supports a dose of 4mg IV ondansetron at the end of surgery for the prevention of PONV.1,5 The guidelines from the SAA also found an A1 level of evidence to support a 8mg ondansetron disintegrating tablet (ODT) for the same purpose.1 Grade A evidence supports a relative risk reduction for PONV of approximately 26% for ondansetron.5 One guideline stated that antiemetic combinations that include a 5HT3 receptor antagonist, such as ondansetron, with dexamethasone or droperidol (A1 level of evidence) or with both dexamethasone and droperidol (A2 level of evidence) are more effective than a single antiemetic.1 The SAA guidelines recommend a dose of 1mg/kg IV dimenhydrinate (level of evidence A1), for the treatment and prevention of PONV, however the guidelines found insufficient evidence for recommending the timing of dimenhydrinate administration.1 The German guidelines found grade A evidence to support a dose of 62 mg and grade B evidence of efficacy for PONV treatment and prevention with dimenhydrinate.5 The SAA guidelines present evidence for PONV treatment and prevention with the following antiemetics: aprepitant, casopitant, dexamethasone, dimenhydrinate, dolasetron, droperidol, ephedrine, granisetron, haloperidol, methylprednisolone, ondansetron, palonosetron, perphenazine, promethazine, ramosetron, rolapitant, scopolamine, and tropisetron including doses and timing of administration relative to surgery.1 Neither identified guideline recommends a single superior antiemetic for treatment and prevention of PONV.1,5 The German guidelines from 2010 report grade A evidence to state that only 5HT3 receptor antagonists have been fully researched for PONV treatment and confirmed as being effective, however the German guidelines also supported grade A evidence for a multimodal approach and found grade A evidence to support cumulative effects of combination therapies including ondansetron, dexamethasone, and droperidol.5 Level A1 evidence was identified in the SAA guidelines for combination therapies that include a 5HT3 receptor antagonist with dexamethasone or with droperidol.1 Neither guideline presented levels of evidence or graded recommendations regarding the frequency or type of adverse events associated with the identified antiemetics. A safety concern for perioperative dexamethasone was raised in the SAA guidelines but found the data inconclusive regarding an increased the risk of wound infection with 4 to 8mg perioperative administration of dexamethasone.1 There is consensus of the two guidelines that at the minimum effective doses antiemetics present limited adverse effects, most commonly headache, drowsiness, and dizziness.1,5 Adverse events are tabulated in the German guidelines without levels of evidence. This guideline reports headaches, constipation, and raised liver enzymes as adverse events, and increased QT interval on ECG as a contraindication for ondansetron.5 The SAA guideline cites one meta-analysis (published 1997) that found the number-needed-to-harm with a single dose of ondansetron (4mg) was 36 for headache, 31 for elevated liver enzymes, and 23 for constipation.1 Concern is raised in one guideline regarding 5HT3 receptor antagonists effect on QTc interval, however no recommendations, evidence level,
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 9
or quantitative information is presented.1 Adverse events of dimenhydrinate are reported as sedation with no reported contraindications.5 Limitations Evidence identified in this report focuses on PONV which has additional contributing factors to emetic symptoms and may have limited applicability to other clinical settings of opioid-induced nausea. While the rate of PONV varies for different surgical procedures,24 in this report PONV is considered an equivalent condition regardless of the surgical procedure. Additionally many of the identified studies focus on patients with risk factors for PONV perhaps further limiting the applicability of some of the findings. The included studies are all small single-center studies that may lack the power to identify infrequent adverse events. The included studies did not include all of the available antiemetics, and no comparison studies covered all of the included antiemetics. The included studies also contained significant differences in the interventions, comparators and outcomes therefore a conclusion regarding the most efficacious antiemetic drug cannot be made with the identified evidence. CONCLUSIONS AND IMPLICATIONS FOR DECISION OR POLICY MAKING The studies identified for this report focus on antiemetic treatment and prevention of PONV. Antiemetics that have demonstrated efficacy for treatment and prevention of PONV have been described as effective for the treatment and prevention of the indications, “opioid-induced nausea” and “opioid induced vomiting.”5 The evidence identified here is suggestive that a combination of ramosetron and dexamethasone, a combination of aprepitant, dexamethasone and ondansetron, and/or naloxone alone as the most effective antiemetics for the treatment and prevention of PONV and, by extension, for opioid-induced nausea.9,10,13,22. The included studies are small, with large quantitative differences in outcome measures between studies, and necessary studies required to establish a single superior antiemetic are not available (e.g. large trials directly comparing available combinations, or network meta-analyses indirectly comparing available anti-emetics) there the evidence presented in this report is suggestive but insufficient to make definitive conclusions regarding comparative antiemetic efficacy. It is important to note that ramosetron and aprepitant are not marketed in Canada.25 The consensus of the relevant included studies and guidelines is that ondansetron is an effective antiemetic.1,5,18,19,21 Furthermore the identified studies and guidelines support cumulative antiemetic efficacy when ondansetron is administered in combination with dexamethasone,1,5,11,14,16,22 dexamethasone and haloperidol,11 droperidol,1,5 and aprepitant.11 This improvement is not associated with a reported increase in the frequency of adverse events in these studies. Insufficient evidence was identified regarding the antiemetic efficacy of diphenhydramine in the included RCTs. One identified study found diphenhydramine in combination with metoclopramide resulted in a statistically significant improvement for PONV prevention than diphenhydramine alone.17 The identified guidelines both report high quality evidence, that did not meet the inclusion criteria of this report, supporting the use of diphenhydramine and dosing
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 10
for prevention and treatment of PONV.1,5 No guidelines supported antiemetic combinations including diphenhydramine. Commonly reported adverse events in the identified studies include headache, dizziness and drowsiness. No serious adverse events were reported to be associated with antiemetic administration. The included studies were relatively small, single-center studies that often focused on a specific patient population with risk factors for PONV therefore less frequent adverse events may not have been detected. Both guidelines raised concerns regarding the effect of 5HT3 receptor antagonists on QTc interval however no graded recommendations, levels of evidence or quantitative data were presented.1,5 Two RCTs raised concerns about the potential for dexamethasone to interfere with wound healing but the identified evidence did not report any such adverse events.9,13 Insights into the cost-effectiveness of ondansetron or diphenhydramine were not possible as no cost-effectiveness studies were identified. PREPARED BY: Canadian Agency for Drugs and Technologies in Health Tel: 1-866-898-8439 www.cadth.ca
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 11
LIST OF ABBREVIATIONS AGREE=Appraisal of Guidelines for Research and Evaluation ASA=American Society of Anesthesiologists AUC=area under the time concentration curve COI=conflict of interest EREM=extended-release epidural morphine IQR=inquartile range IV-PCA=intravenous patient controlled analgesia MCP=metoclopramide NR=not reported OAA/S=observer’s assessment of alertness/sedation PACU=post anesthesia care unit PCA=patient controlled analgesia PCEA=patient controlled epidural analgesia RCS=retrospective case-controlled study PONV=postoperative nausea and vomiting PRISMA=Preferred Reporting Items for Systematic Reviews and Meta-Analyses PVRS=pain verbal rating score RCT=randomized controlled trial SAA=Society for Ambulatory Anesthesiology SD=standard deviation SOP=standard operating procedure TKA=total knee arthroplasty UMSS=University of Michigan Sedation Scale USD=United States Dollars VAS=verbal analogue scale VDS=verbal descriptive scale VNRS=verbal numerical rating scale
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 12
REFERENCES 1. Gan TJ, Diemunsch P, Habib AS, Kovac A, Kranke P, Meyer TA, et al. Consensus
guidelines for the management of postoperative nausea and vomiting. Anesth Analg [Internet]. 2014 Jan [cited 2014 Mar 18];118(1):85-113. Available from: http://www.anzca.edu.au/resources/endorsed-guidelines/related-documents/2014-consensus-guidelines-for-the-management-of-ponv.pdf
2. Apfel CC, Jukar-Rao S. Is palonosetron also effective for opioid-induced and post-discharge nausea and vomiting? Br J Anaesth. 2012 Mar;108(3):371-3.
3. Moon YE, Joo J, Kim JE, Lee Y. Anti-emetic effect of ondansetron and palonosetron in thyroidectomy: a prospective, randomized, double-blind study. Br J Anaesth [Internet]. 2012 Mar [cited 2014 Mar 17];108(3):417-22. Available from: http://bja.oxfordjournals.org/content/108/3/417.full.pdf+html
4. Tamdee D, Charuluxananan S, Punjasawadwong Y, Tawichasri C, Patumanond J, Sriprajittichai P. A randomized controlled trial of pentazocine versus ondansetron for the treatment of intrathecal morphine-induced pruritus in patients undergoing cesarean delivery. Anesth Analg. 2009 Nov;109(5):1606-11.
5. Rusch D, Eberhart LH, Wallenborn J, Kranke P. Nausea and vomiting after surgery under general anesthesia: an evidence-based review concerning risk assessment, prevention, and treatment. Dtsch Arztebl Int [Internet]. 2010 Oct [cited 2014 Mar 17];107(42):733-41. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2977990/pdf/Dtsch_Arztebl_Int-107-0733.pdf
6. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health [Internet]. 1998 Jun [cited 2014 Apr 9];52(6):377-84. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1756728/pdf/v052p00377.pdf
7. Brouwers M, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, et al. AGREE II: advancing guideline development, reporting and evaluation in healthcare. CMAJ [Internet]. 2010 Dec [cited 2014 Apr 9];182(18):E839-E842. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3001530/pdf/182e839.pdf
8. Roh GU, Yang SY, Shim JK, Kwak YL. Efficacy of Palonosetron Versus Ramosetron on Preventing Opioid-Based Analgesia Related Nausea and Vomiting Following Lumbar Spinal Surgery: A Prospective, Randomized, and Double-Blind Trial. Spine (Phila Pa 1976 ). 2014 Jan 29. Epub ahead of print.
9. Koh IJ, Chang CB, Lee JH, Jeon YT, Kim TK. Preemptive low-dose dexamethasone reduces postoperative emesis and pain after TKA: a randomized controlled study. Clin Orthop Relat Res. 2013 Sep;471(9):3010-20.
10. Dabbous A, Souki M, Baraka A, Jabbour-Khoury S. Naloxone versus metoclopramide for the treatment of established postoperative nausea and vomiting in patients following
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 13
general anesthesia with fentanyl supplementation--pilot study. Middle East J Anesthesiol. 2012 Oct;21(6):851-6.
11. Benevides ML, Oliveira SS, de Aguilar-Nascimento JE. The combination of haloperidol, dexamethasone, and ondansetron for prevention of postoperative nausea and vomiting in laparoscopic sleeve gastrectomy: a randomized double-blind trial. Obes Surg. 2013 Sep;23(9):1389-96.
12. Kim YY, Moon SY, Song DU, Lee KH, Song JW, Kwon YE. Comparison of palonosetron with ondansetron in prevention of postoperative nausea and vomiting in patients receiving intravenous patient-controlled analgesia after gynecological laparoscopic surgery. Korean J Anesthesiol [Internet]. 2013 Feb [cited 2014 Mar 17];64(2):122-6. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3581780/pdf/kjae-64-122.pdf
13. Yang SY, Jun NH, Choi YS, Kim JC, Shim JK, Ha SH, et al. Efficacy of dexamethasone added to ramosetron for preventing postoperative nausea and vomiting in highly susceptible patients following spine surgery. Korean J Anesthesiol. 2012 Mar;62(3):260-5. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3315657
14. Wang PK, Tsay PJ, Huang CC, Lai HY, Lin PC, Huang SJ, et al. Comparison of dexamethasone with ondansetron or haloperidol for prevention of patient-controlled analgesia-related postoperative nausea and vomiting: a randomized clinical trial. World J Surg. 2012 Apr;36(4):775-81.
15. Lee JW, Park HJ, Choi J, Park SJ, Kang H, Kim EG. Comparison of ramosetron's and ondansetron's preventive anti-emetic effects in highly susceptible patients undergoing abdominal hysterectomy. Korean J Anesthesiol [Internet]. 2011 Dec [cited 2014 Mar 17];61(6):488-92. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3249571/pdf/kjae-61-488.pdf
16. Song JW, Park EY, Lee JG, Park YS, Kang BC, Shim YH. The effect of combining dexamethasone with ondansetron for nausea and vomiting associated with fentanyl-based intravenous patient-controlled analgesia. Anaesthesia. 2011 Apr;66(4):263-7.
17. Lu CW, Jean WH, Wu CC, Shieh JS, Lin TY. Antiemetic efficacy of metoclopramide and diphenhydramine added to patient-controlled morphine analgesia: a randomised controlled trial. Eur J Anaesthesiol. 2010 Dec;27(12):1052-7.
18. Huh BK, Jung S, White W, Jeon Y. Anti-emetic effect of midazolam added to morphine patient-controlled analgesia after total abdominal hysterectomy. Anaesth Intensive Care. 2010 May;38(3):481-5.
19. Rauers NI, Stuber F, Lee EH, Musshoff F, Fimmers R, Barann M, et al. Antagonistic effects of ondansetron and tramadol? A randomized placebo and active drug controlled study. J Pain. 2010 Dec;11(12):1274-81.
20. Hahm TS, Ko JS, Choi SJ, Gwak MS. Comparison of the prophylactic anti-emetic efficacy of ramosetron and ondansetron in patients at high-risk for postoperative nausea and vomiting after total knee replacement. Anaesthesia. 2010 May;65(5):500-4.
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 14
21. Dagtekin O, Wiese P, Wolter K, Hermann MM, Pietruck C, Kampe S. Haloperidol versus haloperidol plus ondansetron for the prophylaxis of postoperative nausea and vomiting after ophthalmologic surgery. Pharmacology. 2009;83(4):205-10.
22. Hartrick CT, Tang YS, Hunstad D, Pappas J, Muir K, Pestano C, et al. Aprepitant vs. multimodal prophylaxis in the prevention of nausea and vomiting following extended-release epidural morphine. Pain Pract. 2010 May;10(3):245-8.
23. Vale C, Oliveira F, Assuncao J, Fontes-Ribeiro C, Pereira F. Co-administration of ondansetron decreases the analgesic efficacy of tramadol in humans. Pharmacology. 2011;88(3-4):182-7.
24. Ruiz JR, Kee SS, Frenzel JC, Ensor JE, Selvan M, Riedel BJ, et al. The effect of an anatomically classified procedure on antiemetic administration in the postanesthesia care unit. Anesth Analg. 2010 Feb 1;110(2):403-9.
25. Health Canada. Notice of compliance (NOC) database [Internet]. Ottawa: Health Canada; 1994 -; 2012 [cited 2014 Apr 9]. Available from: http://webprod5.hc-sc.gc.ca/noc-ac/index-eng.jsp
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 15
Benevides et al., 201311 Parallel group RCT Timepoints 0-2, 2-12, 12-24, 24-36 hours post-surgery
Adult patients undergoing general anesthesia for laparoscopic sleeve gastrectomy ASA physical status I-III (n=60)
Opioid: Intraoperative: Fentanyl & remifentanil Postoperative: Morphine for maintenance of PVRS<4 Antiemetic: Intraoperative: Haloperidol (2mg) Dexamethasone (8mg)
Opioid: Intraoperative: Fentanyl & remifentanil Postoperative: Morphine for maintenance of PVRS<4 Antiemetic: Intraoperative: With and without Dexamethasone (8mg) 20-30min prior to
• PONV occurrence • Rescue antiemetic requirement • Time to first antiemetic rescue • Adverse events • Morphine consumption • Volume of IV fluids • Length of hospital stay
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 17
Study Design, Followup timepoints
Patient Characteristics, Sample Size
Intervention Comparator(s) Outcomes
20-30min prior to end of surgery Ondansetron (8mg)
end of surgery Ondansetron (8mg)
Kim et al., 201312 Parallel group RCT Timepoints 2, 24, 48, 72 hours post-surgery
Adult female non-smokers undergoing general anesthesia for gynecological laparoscopic surgery ASA physical status I&II (n=100)
Huh et al., 201018 Parallel group RCT Timepoints: 1, 4, 8, 16, 24 hours post-surgery
Adult female non-smokers undergoing general anesthesia for abdominal hysterectomy ASA physical status I or II (n=90)
Opioid: Intraoperative: Fentanyl Postoperative: Morphine IV-PCA Antiemetic: Upon first request: Midazolam (1mg) Postoperative: Midazolam IV-PCA
Opioid: Intraoperative: Fentanyl Postoperative: Morphine IV-PCA Antiemetic: Upon first request: Ondansetron (4mg) or placebo Postoperative: Ondansetron IV-PCA or placebo
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 21
Study Design, Followup timepoints
Patient Characteristics, Sample Size
Intervention Comparator(s) Outcomes
Haloperidol (10µg/kg) with Ondansetron (0.1mg/kg)
Haloperidol (10µg/kg)
• Adverse events
Hartrick et al., 201022 Sequential, open-label, matched case-control study Timepoints: Up to 48hours
Adult patients undergoing general anesthesia for TKA ASA physical status NR (n=24)
Opioid: EREM Antiemetic: IV Ondansetron (4mg) and Dexamethasone (4-6mg) and oral Aprepitant (40mg)
Opioid: EREM Antiemetic: IV Ondansetron (4mg) and Dexamethasone (4-6mg) and either Metoclopramide (10mg), Diphenhydramine (25mg) or Prochlorperazine (5mg)
Rusch et al., 20105 Germany, 2010 Antiemetic doses and
timing for prevention of PONV in adult patients
Recommendations Graded A-D Levels of Evidence Rated 1-4
Basis for incorporation into German SOPs
PONV=postoperative nausea and vomiting; SOP=standard operating procedure
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 23
Appendix 3: Guideline Grading of Recommendations and Levels of Evidence
Recommendation Level of Evidence Society for Ambulatory Anesthesiology, 20141 N/A A Supportive Literature
A1: multiple RCTs and supported by MA A2: multiple RCTs no MAs A3: one RCT B Suggestive Literature B1: case controlled observational studies B2: observational studies B3: case reports C Equivocal Literature C1: MAs find no significant differences (p>0.01) C2: RCTs find no significant differences OR RCTs support inconsistent findings C3: Observational studies findings are inconsistent D Insufficient Evidence from Literature
Rusch et al., 20105 A: At least one MA, systematic review of RCTs or RCT rated as 1++, consistent evidence rated as 1+ B: Evidence overall consistent studies of 2++, or extrapolated evidence from 1++ or 1+ C:Evidence overall consistent studies of 2+, or extrapolated evidence from 2++ D: Evidence 3 or 4, or extrapolated evidence from 2+ Good practice point: Expert opinion
1++: High quality MAs, systematic reviews of RCTs or RCTs with very low bias risk 1+: Well conducted MAs, systematic reviews of RCTs or RCTs with low bias risk 1-: MAs, systematic review of RCTs or RCTs with high bias risk 2++: High quality systematic reviews of case control or cohort studies with very low bias risk 2+: Well conducted case control or cohort studies with low bias risk 2-: Case control or cohort studies with high bias risk and/or significant risk that relationship is not causal 3: Non-analytic studies 4: Expert opinion
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 24
Appendix 4: Summary of Critical Appraisal of RCTs and RCS using the Downs and Black checklist6
Strengths Limitations Roh et al., 20148 • CONSORT diagram • Patient characteristics tabulated with PONV risk factors • Allocation concealment methods described • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Time dependent results graphed • Statistical power determined a priori, based on previous published results, to determine number of patients required • Comprehensive discussion on study limitations • Adverse events discussed and quantified • Statement of no conflict of interest
• Focus on PONV not specifically opioid-induced nausea • Single center study
Koh et al., 20139 • CONSORT diagram • Patient characteristics tabulated with PONV risk factors – no significant differences between groups • Allocation concealment methods described • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Time dependent results graphed • Statistical power determined a priori, based on previous published results, to determine number of patients required • Comprehensive discussion on study limitations • Adverse events discussed • Statement of no conflict of interest
• Focus on PONV not specifically opioid-induced nausea • Patient inclusion criteria potentially limits applicability of results especially outside of PONV • Single center study
Benevides et al., 201311 • CONSORT diagram • Patient characteristics tabulated with Apfel score - no significant differences between groups • Statistical methods described • Randomization methods described • Role of blinded investigators outlined
• Focus on PONV not specifically opioid-induced nausea • Single center study • Allocation concealment methods unclear • No explicit discussion of study limitations • Inclusion of patients of ASA physical status III – severe systemic disease- may confound
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 25
Strengths Limitations • Clearly defined patient eligibility, intervention and outcomes • Time dependent results graphed • Statistical power determined a priori to determine number of patients required • Adverse events discussed • Statement of no conflict of interest
findings and limit applicability to other settings
Kim et al., 201312 • Patient characteristics, age, height and weight, tabulated no significant differences between groups • Statistical methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Statistical power determined a priori to determine number of patients required • Discussion of study limitations • Adverse events tabulated
• Focus on PONV not specifically opioid-induced nausea • Patient inclusion criteria potentially limits applicability of results especially outside of PONV • Single center study • Randomization and allocation concealment methods not described • No COI statement
Dabbous et al., 201210 • Patient characteristics tabulated with PONV risk factors – no significant differences between groups • Statistical methods described • Examines acute antiemetic rescue of PONV • Adverse events discussed
• Focus on PONV not specifically opioid-induced nausea • Inconsistent surgical intervention • Unclear blinding, allocation and randomization methods • Small single center pilot study • No explicit discussion of study limitations • No COI statement
Yang et al., 201213 • Patient characteristics tabulated with PONV risk factors – no significant differences between groups • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Time dependent results tabulated • Statistical power determined a priori to determine number of patients required • Discussion on study limitations • Adverse event occurrence recorded
• Focus on PONV not specifically opioid-induced nausea • Patient inclusion criteria potentially limits applicability of results especially outside of PONV • Single center study • No COI statement
Wang et al., 201214 • CONSORT diagram • Patient characteristics tabulated with Apfel score • Statistical methods described • Randomization methods described
• Focus on PONV not specifically opioid-induced nausea • Inconsistent surgical intervention • Single center study
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 26
Strengths Limitations • Role of blinded investigators outlined • Clearly defined patient eligibility • Time dependent results tabulated • Statistical power determined a priori to determine number of patients required • Adverse events mentioned • Statement of no conflict of interest • Discussion on study limitations Moon et al., 20123 • CONSORT diagram • Patient characteristics tabulated • Allocation concealment and randomization methods described • Statistical methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Time dependent results graphed • Statement of no conflict of interest • Comprehensive discussion on study limitations • Adverse events discussed
• Focus on PONV not specifically opioid-induced nausea • Statistical power of study not examined • Single center study
Lee et al., 201115 • Patient characteristics tabulated with PONV risk factors – no significant differences between groups • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Time dependent results tabulated • Statistical power determined a priori, based on a preliminary study, to determine number of patients required • Comprehensive discussion on study limitations • Adverse events quantified
• Focus on PONV not specifically opioid-induced nausea • Patient inclusion criteria potentially limits applicability of results especially outside of PONV • Single center study • No COI statement
Song et al., 201116 • Patient characteristics tabulated with PONV risk factors • Allocation concealment methods described • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Statistical power determined a priori, based
• Focus on PONV not specifically opioid-induced nausea • Single center study
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 27
Strengths Limitations on a preliminary study, to determine number of patients required • Statement of no conflict of interest • Study limitations mentioned • Adverse events discussed and quantified Lu et al., 201017 • CONSORT diagram • Patient characteristics tabulated with PONV risk factors – significant differences calculated • Allocation concealment methods described • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Time dependent results graphed and tabulated • Statistical power determined a priori, based on preliminary results, to determine number of patients required • Comprehensive discussion on study limitations
• Focus on PONV not specifically opioid-induced nausea • Patient inclusion criteria potentially limits applicability of results especially outside of PONV • Single center study • No COI statement
Huh et al., 201018 • Patient characteristics tabulated – no significant differences between groups • Allocation concealment methods described • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Time dependent results graphed • Statistical power determined a priori, based on previous published results, to determine number of patients required • Adverse events discussed and quantified
• Focus on PONV not specifically opioid-induced nausea • Patient inclusion criteria potentially limits applicability of results especially outside of PONV • Single center study • No COI statement
Rauers et al., 201019 • CONSORT diagram • Patient characteristics tabulated with Apfel scores– no significant differences between groups • Allocation concealment methods described • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility • Time dependent results graphed
• Focus on PONV and drug interactions not specifically opioid-induced nausea • Inclusion of patients of ASA physical status III – severe systemic disease- may confound findings and limit applicability to other settings • Relevant outcomes not clearly defined • No COI statement • Adverse events not discussed
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 28
Strengths Limitations • Statistical power determined a priori to determine number of patients required • Discussion on study limitations Hahm et al., 201020 • Patient characteristics tabulated • Allocation concealment methods described • Statistical methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Time dependent results graphed • Statistical power determined a priori, based on pilot study, to determine number of patients required • Comprehensive discussion on study limitations • Adverse events discussed • Statement of no conflict of interest
• Focus on PONV not specifically opioid-induced nausea • Inclusion of patients of ASA physical status III – severe systemic disease- may confound findings and limit applicability to other settings • Randomization method not described • Single center study
Tamdee et al., 20094 • CONSORT diagram • Patient characteristics tabulated • Allocation concealment methods described • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Statistical power determined a priori to determine number of patients required • Comprehensive discussion on study limitations • Adverse events discussed and quantified
• Focus on opioid-induced pruritus not specifically opioid-induced nausea • Patient inclusion criteria potentially limits applicability of results especially outside of PONV • Single center study • No COI statement
Dagtekin et al., 200921 • Patient characteristics power determined • Study limitations mentioned tabulated • Allocation concealment methods described • Statistical methods described • Randomization methods described • Role of blinded investigators outlined • Clearly defined patient eligibility, intervention and outcomes • Time dependent results tabulated • Statistical • Adverse events discussed
• Focus on PONV not specifically opioid-induced nausea • Patient inclusion criteria potentially limits applicability • Single center study • Unclear COI statement
Hartrick et al., 201022 • Patient characteristics tabulated with PONV risk factors – no significant differences between pairs
• Not a RCT (retrospective matched-case control study (RCS)) • Focus on PONV not specifically opioid-induced
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 29
Strengths Limitations • Statistical methods described • Clearly defined patient outcomes • Comprehensive discussion on study limitations • COI statement
nausea • Single center study • No mention of adverse events
ASA=American Society of Anesthesiologists; COI=conflict of interest; NR=not reported; RCS=retrospective case controlled study; PONV=postoperative nausea and vomiting; RCT=randomized controlled trial;
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 30
Appendix 4: Summary of Critical Appraisal of Guidelines Using AGREE7
Strengths Limitations Society for Ambulatory Anesthesiology, 20141 • Evidence levels for doses and timing for 18 different antiemetics • Evidence levels and antiemetic tabulated • Detailed COIs for individual contributors • Explicit scope, goals and target audience • Stakeholder representation in guideline development group • Literature search methodology outlined • Exclusion criteria
• Recommendations not graded • Focus is PONV not opioid-induced nausea • No summary of limitations
Rusch et al., 20105 • Levels of evidence and grades of recommendations explicitly linked • COI statement
• Literature search not systematic • No predefined inclusion/exclusion criteria or date limits for literature search • No explicitly stated goals or target audience • Limited representation of stakeholders in guideline development • Focus is PONV not opioid-induced nausea
COI=conflict of interest; PONV=postoperative nausea and vomiting;
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 31
Clinical Effectiveness “In conclusion, despite its theoretical advantages in terms of receptor affinity and action duration, palonosetron was inferior to ramosetron in preventing PONV in patients receiving IV-PCA opioid following lumbar spinal surgery. In addition, increased PONV was translated to increased intensities of postoperative pain in the palonosetron group favoring the use of ramosetron for antiemetic prophylaxis in patients receiving opioid-based analgesia after lumbar spinal surgery.” (pp. 12 of accepted manuscript) Adverse Events “The incidences of adverse events were similar between the groups …” (pp. 8 of accepted manuscript)
Koh et al., 20139 Clinical Effectiveness R-Ramosetron RD-Ramosetron with Dexamethasone Statistically significant differences (p<0.05) Nausea occurrence 0~6hrs (P = 0.028) 0~72hrs (P = 0.004) RD 22% RD 24% R 37% R 40% Vomiting occurrence 0~6hrs (P < 0.001) 0~72hrs (P = 0.001) RD 3% RD 7% R 21% R 21% Pain (VAS scale 0-10 (mean) 6~24hrs (P < 0.001) RD 2.4 R 4.0 Nausea (VAS scale 0-10 (mean)
Clinical Effectiveness “The [dexamethasone with ramosetron (Dexa-Ra)] group had a lower incidence of PONV during the entire 72-hour evaluation period and experienced less severe nausea for the first 6 hours after TKA, although not between 6 to 72 hours. Overall use of a rescue antiemetic was less frequent, and complete response was more frequent in the Dexa-Ra group. Patients in the Dexa-Ra group experienced lower pain and consumed less opioids during the 6- to 24-hour period and during the overall study period. No differences were found in wound complications between the groups, and each group had one case of periprosthetic joint infection.” (pp. 3010)
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 32
Main Relevant Study Findings Author’s Conclusions 0~6hrs (P < 0.001) RD 1.6 R 2.6 Rescue Antiemetic 0~6hrs (P = 0.004) 0~72hrs (P = 0.001) RD 15% RD 17% R 31% R 35% Opioid Consumption (mean) 6~24hrs (P < 0.001) 0~72hrs (P = 0.004) RD 73.5µg RD 406.2µg R 128.3µg R 500.1µg Adverse Events No statistically significant differences in wound compilations or infections
Adverse Events “More large prospective series are needed to ascertain whether corticosteroid use is associated with increased risks for wound complications in patients undergoing TKA.” (pp. 3017)
Benevides et al., 201311 Clinical Effectiveness HDO-haloperidol, dexamethasone, ondansetron DO-dexamethasone, ondansetron O-ondansetron Statistically significant differences (p<0.05) Nausea occurrence 0~2hrs (P = 0.016) 0~36hrs (P = 0.015) HDO 23.7% HDO 53.3% O 56.7% O 86.7% 12~24hrs (P = 0.008) 12~24hrs (P = 0.009) HDO 23.3% DO 26.7% O 60% O 60% Vomiting occurrence 0~36hrs (P = 0.015) HDO 20% O 53.3% Rescue Antiemetic (number received median [IQR]) 0~36hrs (P = 0.002) HDO 0.5 [1-0] O 2 [4-1] Time to First Rescue Antiemetic (% no antiemetic) 0~36hrs (P = 0.006) HDO 50% O 20% Opioid Consumption (mean ± SD)
Clinical Effectiveness “The combination of haloperidol, dexamethasone, and ondansetron reduced PONV and the necessity of rescue antiemetics and also reduced morphine consumption and the volume of fluids infused postoperatively.” (pp. 1389) Adverse Events “There were few adverse events observed and these were small in magnitude. The most common adverse events observed were headache and dizziness (data not shown).” (pp. 1393)
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 33
Main Relevant Study Findings Author’s Conclusions 0~36hrs (P = 0.007) 0~36hrs (P = 0.01) HDO 4.4 ± 6.1mg HDO 4.4 ± 6.1mg O 8.8 ± 7.5mg DO 7.8 ± 6.6mg Intravenous Fluids (mean ± SD) 0~36hrs (P = 0.026) HDO 4.85 ± 1.09L O 5.79 ± 1.77L Adverse Events No statistically significant differences in wound complications or infections Length of Hospital Stay No statistically significant differences Kim et al., 201312 Clinical Effectiveness Statistically significant differences (p<0.05) Vomiting occurrence 0~72hrs (P = 0.025) Palonosetron 4.0% Ondansetron 18.0% Adverse Events No statistically significant differences
Clinical Effectiveness “In conclusion, bolus of palonosetron 0.075 mg had preventive effects on PONV similar to a bolus of ondansetron 8 mg and continuous i.v. administration of an addition of ondansetron 16 mg in the IV-PCA in high-risk patients who were using IV-PCA after gynecological laparoscopic surgery.” (pp. 125) Adverse Events “There were postoperative side-effects such as headache, dizziness, and drowsiness, but they did not differ significantly between the ondansetron group and the palonosetron group …” (pp. 124)
Dabbous et al., 201210 Clinical Effectiveness Statistically significant differences (p<0.05) Complete response (end of PONV) 5 min post antiemetic administration (p<0.05) Naloxone 27% Metoclopramide 5% No additional statistically significant differences in pain score, nausea score or rescue antiemetic requirements.
Clinical Effectiveness “Single low dose naloxone (0.5mcg/kg) was found to be effective in relieving PONV in the PACU, in patients receiving general anesthesia including fentanyl supplementation, without increasing pain scores. The total response was comparable to metoclopramide. However, the complete response at 5 minutes was even better with naloxone.” (pp. 855)
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 34
Main Relevant Study Findings Author’s Conclusions Adverse Events Not reported
Yang et al., 201213 Clinical Effectiveness R-Ramosetron RD-Ramosetron with Dexamethasone Statistically significant differences (p<0.05) Nausea occurrence (VRS ≥ 4) 0~48hrs (P = 0.029) 0~6hrs (P = 0.032) RD 20% RD 14% R 40% R 32% Vomiting occurrence 0~48hrs (P = 0.037) RD 11% R 26% No additional significant differences in pain scores, rescue antiemetic requirement or adverse events.
Clinical Effectiveness “Combination of ramosetron and dexamethasone significantly reduced the incidence of moderate to severe nausea and vomiting compared to ramosetron alone, although the overall incidence of PONV was similar in both groups in highly susceptible patients for PONV using fentanyl-based IV PCA following spinal surgery using volatile anesthetics.” (pp. 264) Adverse Events “The number of patients who experienced antiemetics-related adverse events during postoperative period was similar between the groups.” (pp. 263) “There were no side effects such as increased risk of infection and wound dehiscence associated with the use of a single dose of dexamethasone” (pp. 263)
Wang et al., 201214 Clinical Effectiveness HD-haloperidol, dexamethasone DO-dexamethasone, ondansetron D-dexamethasone Statistically significant differences (p<0.05) Total PONV 2~24hrs 2~24hrs HD 26% DO 26% D 45% D 45% 0~24hrs 0~24hrs HD 35% DO 30% D 57% D 57% Rescue Antiemetics 0~24hrs 0~24hrs HD 26% DO 19% D 45% D 45%
Clinical Effectiveness “In conclusion, the prophylactic intravenous administration of dexamethasone 5 mg with haloperidol 2 mg or ondansetron 4 mg provides a better antiemetic effect than dexamethasone 5 mg alone in patients who received morphine PCA for postoperative pain management.” (pp. 780) Cost Effectiveness “Our hospital pharmacy’s acquisition cost for 4 mg ondansetron with an 8 mg ampule of dexamethasone is 7.4 USD, whereas one 2 mg of dose of haloperidol with an 8 mg ampule of dexamethasone is 1 USD. If open but unfinished ampules are discarded, the
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 35
Main Relevant Study Findings Author’s Conclusions Complete Response (no PONV, no rescue antiemetic) 0~24hrs 0~24hrs HD 65% DO 70% D 43% D 43% No additional statistically significant differences in pain score, sedation score, adverse events or recovery time.
cost for a 5 mg ampule of haloperidol with an 8 mg ampule of dexamethasone only rises to 1.4 USD. However, the cost for an 8 mg ampule of ondansetron with an 8 mg ampule of dexamethasone rises to 14 USD.”…” Furthermore, haloperidol 2 mg plus dexamethasone 5 mg is more cost-effective than ondansetron 4 mg plus dexamethasone 5 mg for this purpose.” (pp. 780) Adverse Events “In our study, group HD did not show any of the potential side effects of haloperidol, although the sample size of group DH might not be big enough to reveal any complication.” (pp. 780)
Moon et al., 20123 Clinical Effectiveness Statistically significant differences (p<0.05) PONV occurrence 0~24hrs (P = 0.045) Ondansetron 62% Palonosetron 42% Nausea severity (score as a percentage method NR) 2~24hrs (P = 0.03) graphed data Ondansetron ~55% Palonosetron ~35% Vomiting 2~24hrs (P < 0.05) graphed data Ondansetron ~25% Palonosetron ~10% Rescue Antiemetics 2~24hrs (P < 0.05) graphed data Ondansetron ~25% Palonosetron ~10% No additional statistically significant differences in pain score, adverse events or opioid consumption.
Clinical Effectiveness “In conclusion, palonosetron was superior to ondansetron in high-risk patients receiving fentanyl-based i.v. PCA between 2 and 24 h after thyroidectomy. Palonosetron can be considered a promising anti-emetic drug for this subset of patients using opioid-based PCA.” (pp. 421) Adverse Events “The incidence of side-effects, such as headache, dizziness, or drowsiness, was similar between groups …” (pp. 419)
Lee et al., 201115 Clinical Effectiveness Statistically significant differences (p<0.05) Complete Response (no nausea)
Clinical Effectiveness “In conclusion, ramosetron at 0.3 mg is more effective in preventing
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 36
Main Relevant Study Findings Author’s Conclusions 24~48hrs (P = 0.03) Ramosetron 98.3% Ondansetron 86.7% No additional statistically significant differences in pain scores, rescue antiemetic requirements or adverse events.
delayed PONV in highly susceptible women undergoing abdominal hysterectomy compared with ondansetron (4 mg).” (pp. 491) Adverse Events “There were no significant differences in … side effects of the 5-HT3 antagonists such as headache and dizziness between the 2 groups.” (pp. 490)
Song et al., 201116 DO-dexamethasone, ondansetron D-dexamethasone Clinical Effectiveness Statistically significant differences (p<0.05) Severe PONV occurrence (VNRS ≥ 7/11) 0~48hrs (P = 0.028) 6~24hrs (P = 0.032) DO 10% DO 3% O 25% O 18% No additional statistically significant differences in pain, nausea, rescue antiemetics, adverse events or PCA discontinuation
Clinical Effectiveness “In conclusion, we found that combining dexamethasone and ondansetron is more effective in reducing the severity of PONV than ondansetron alone in patients receiving a fentanyl-based PCA after video assisted thoracoscopic surgery.” (pp. 266) Adverse Events “There were no differences in the incidences of headache, dizziness or drowsiness between the groups” (pp. 265)
Lu et al., 201017 Clinical Effectiveness M-Morphine MM-Morphine Metoclopramide MD-Morphine Diphenhydramine MMD-Morphine Metoclopramide Diphenhydramine Statistically significant differences (p<0.05) Nausea occurrence (P compared to MMD) M 54.2% (P < 0.001) MM 44.9% (P = 0.003) MD 30.6% (P = 0.039) MMD 16.3% Vomiting occurrence (P = 0.006) M 35.4% MMD 10.2% Pain Score (VAS) 0~72hrs (P < 0.001) Multiple timepoints MMD < MD, MM & M
Clinical Effectiveness “In conclusion, the addition of metoclopramide and diphenhydramine to PCA in patients treated with dexamethasone at anesthesia induction can reduce opioid-related side effects and improve analgesia in women receiving abdominal total hysterectomy.”…”Further research is necessary to establish the optimal ratio of a mixture of metoclopramide, diphenhydramine and morphine to prevent postoperative nausea and vomiting.” (pp. 1057) Adverse Events Not reported
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 37
Main Relevant Study Findings Author’s Conclusions No additional statistically significant differences in sedation scores or morphine consumption. Huh et al., 201018 Clinical Effectiveness Statistically significant differences (p<0.05) PONV occurrence 0~24hrs (P < 0.05) 0~24hrs (P < 0.05) Ondansetron 36.7% Midazolam 26.7% Control 70% Control 70% Nausea occurrence 0~24hrs (P < 0.05) 0~24hrs (P < 0.05) Ondansetron 13.3% Midazolam 10% Control 40% Control 40% Incidence of mild sedation greater in Midazolam group (P < 0.05) No additional statistically significant differences in pain scores, rescue antiemetic requirements, adverse events or morphine consumption.
Clinical Effectiveness “In conclusion, in this study midazolam was as effective as ondansetron in preventing opioid-induced nausea and vomiting following total abdominal hysterectomy and had acceptable side-effects.” (pp. 484) Adverse Events “The side-effects of anti-emetics may limit their use. The prominent side-effects of midazolam and morphine are sedation and respiratory depression, so co-administration might produce synergistic effects. In our study mild sedation was more common in the midazolam group but did not reduce morphine use …” (pp. 484)
Rauers et al., 201019 Clinical Effectiveness Statistically significant differences (p<0.05) Complete response (no PONV) 0~8hrs (P = 0.046) Ondansetron 85% Placebo 66.7% Vomiting 0~8hrs (P = 0.01) 0~8hrs (P = 0.01) Ondansetron 5.0% Metoclopramide 5.1% Placebo 18.6% Placebo 18.6% (+)O-demethyltramadol plasma concentration CYP2D6 genotypes (mean AUC ± SD) 0~3hrs (P < 0.001) No functional copy 22.2 ± 21.4 ng h/mL Heterozygotes 38.0 ± 12.5 ng h/mL Two active alleles 47.3 ± 11.0 ng h/mL CYP2D6 duplication/multiduplication 279.1 ± 11.7ng h/mL No additional statistically significant differences in pain scores, rescue antiemetic requirements, or opioid consumption.
Clinical Effectiveness “Response rate to antiemetic prophylaxis was superior in patients receiving ondansetron (85.0%) compared with placebo (66.7%, P = .046), with no difference to metoclopramide (69.5%). Less vomiting was reported in the immediate postoperative hours in the verum groups (ondansetron 5.0%, metoclopramide 5.1%) compared with placebo (18.6%; P = .01).” (pp. 1274) “In this postoperative setting after major abdominal surgery, tramadol’s analgesic effect was not decreased by co-administration of ondansetron compared with placebo or MCP, nor was the frequency of PONV increased.” (pp. 1279) Adverse Events Not reported
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 38
Main Relevant Study Findings Author’s Conclusions Hahm et al., 201020 Clinical Effectiveness R-Ramosetron O-Ondansetron Statistically significant differences (p<0.05) Nausea score (VAS (0-10)) (median (IQR[range]) 2~6hrs (P = 0.004) 6~24hrs (P = 0.008) R 0 (0-2[0-8]) R 0 (0-4.5[0-10]) O 3 (0-6.5[0-10]) O 5 (0-10[0-10]) 24~48hrs (P = 0.016) R 0 (0-4.5[0-10]) O 3 (0-6[0-10]) Complete Response (no PONV and no rescue antiemetic) - graphed data 2~6hrs (P < 0.05) 6~24hrs (P < 0.05) R ~74% R ~62% O ~36% O ~33% 24~48hrs (P < 0.05) R ~54% O ~24% Rescue antiemetic requirement - graphed data 24~48hrs (P < 0.05) R ~60% O ~29% Overall Satisfaction 1-10 scale (median (IQR[range]) (P = 0.016) R 9 (7-9[2-10]) O 4 (0-5[0-10]) No additional statistically significant differences in pain scores, adverse events or opioid consumption.
Clinical Effectiveness “In conclusion, ramosetron was more effective than ondansetron in preventing PONV in high-risk patients undergoing unilateral total knee replacement.” (pp. 503) Adverse Events “The most common adverse effects were headache, dizziness, and drowsiness; there were no differences in the incidence of these events in the two groups.” (pp. 502)
Tamdee et al., 20094 Clinical Effectiveness Statistically significant differences (p<0.05) Pruritus score ≤ 2/4 (P < 0.001) Pentazocine 96.1% Ondansetron 80.8% No additional statistically significant differences in pain scores, nausea and vomiting, adverse events, blood pressure, heart rate, respiratory rate, O2 saturation or shivering score.
Clinical Effectiveness “Prophylactic ondansetron has been shown to decrease the incidence of intrathecal morphine-induced nausea and vomiting, and there was no difference in the incidence of PONV between the two groups.” (pp. 1610) Adverse Events “No hallucinations, extrapyramidal
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 39
Main Relevant Study Findings Author’s Conclusions effects, dizziness, or respiratory depression were observed in either group.” (pp. 1608)
Dagtekin et al., 200921 Clinical Effectiveness H-Haloperidol HO-Haloperidol with Ondansetron Statistically significant differences (p<0.05) PONV occurrence 0~24hrs (P = 0.008) H 57% HO 23% Vomiting occurrence 0~24hrs (P = 0.009) H 20% HO 0% Pain Scores (VAS (0-10)) (mean ± SD) 0hrs (P = 0.032) 2hrs (P = 0.032) H 2.97 ± 1.847 H 2.70 ± 1.765 HO 2.00 ± 1.554 HO 1.70 ± 1.622 4hrs (P = 0.032) H 2.27 ± 1.837 HO 1.23 ± 1.278 No additional statistically significant differences in sedation score or adverse events.
Clinical Effectiveness “The single use of haloperidol had a limited efficacy for the prophylaxis of PONV after ophthalmologic surgery in a study population with an increased risk for PONV.” … “Better results were obtained with the combination therapy of haloperidol with ondansetron, especially for vomiting.” (pp. 209) Adverse Events “No differences in adverse effects were observed in the treatment groups.” (pp. 209)
Hartrick et al., 201022 Clinical Effectiveness Statistically significant differences (p<0.05) PONV occurrence 0-48hrs (P = 0.039) Ondansetron and dexamethasone with aprepitant 25% with either metoclopramide, diphenhydramine or prochlorperazine 75% No additional statistically significant differences in pain scores, rescue antiemetics or respiratory depression.
Clinical Effectiveness “…aprepitant significantly reduced the incidence of PONV compared with a multimodal antiemetic regime in this study…” (pp. 248) “The results of this pilot study will be used to determine the study size needed for the prospective randomized controlled trial.” (pp. 248) Adverse Events Not reported
AUC=area under the time concentration curve; IQR=inquartile range; IV-PCA=intravenous patient controlled analgesia; MCP=metoclopramide; PACU=post anesthesia care unit; PONV=postoperative nausea and vomiting; SD=standard deviation; USD=United States Dollars; VAS=verbal analogue scale; VRNS= verbal numerical rating scale; VRS= verbal rating scale
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 40
Appendix 7: Summary of Recommendations by Source (for grading schemes see Appendix 3)
Society for Ambulatory Anesthesiology, 20141 Antiemetic Doses and Timing for PONV prevention in Adults Dimenhydrinate 1mg/kg IV [A1] not enough data to suggest optimal timing Ondansetron 4mg IV, 8mg ODT [A1] at end of surgery [A1] Pharmacologic Combination Therapy for Adults 5HT3 receptor antagonist + dexamethasone [A1] 5HT3 receptor antagonist + droperidol [A1] 5HT3 receptor antagonist + dexamethasone + droperidol [A2] Ondansetron + casopitant or TDS [A1] Prevention and Treatment Algorithms (not explicitly linked to evidence or opioid use) PONV-Prevention (with no prevention in low risk patients)
Low Risk Medium Risk High Risk Prophylaxis None Dexamethasone
(4mg) Ondansetron (4mg)
Dexamethasone (4mg) Ondansetron (4mg)
Treatment Droperidol (1mg) Droperidol (1mg) Droperidol (1mg) If Treatment ineffective
Dimenhydrinate (1mg/kg)
Dimenhydrinate (1mg/kg)
Dimenhydrinate (1mg/kg)
PONV-Prevention and Treatment Algorithms (including prevention in low risk patients)
Low Risk Medium Risk High Risk Prophylaxis Dexamethasone
Rusch et al., 20105 Antiemetic Doses and Timing for PONV prevention in Adults Dimenhydrinate 62mg [grade A] intraoperatively [grade D] Ondansetron 4mg [grade A] at end of surgery [grade B] “Antiemetics with proven efficacy [grade A] for PONV can essentially also be considered effective for the indication “opioid-induced nausea and opioid-induced vomiting” [grade D].” “Only 5HT3 receptor antagonists have been fully researched for PONV treatment and confirmed as being effective [grade A]. They are, therefore, first-line drugs for treatment of PONV, especially when no prophylaxis has been administered beforehand [grade D].” “The data available on all the other drug based and non-drug-based methods described above is less extensive, although dexamethasone [grade A], haloperidol [grade A], dimenhydrinate
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 41
[grade B] and promethazine [grade C] have been shown to be effective in treating PONV.” “For dexamethasone, droperidol and ondansetron, a comparable antiemetic efficacy with a relative risk reduction (RRR) for PONV of approximately 26% has been demonstrated [grade A].” “The effects of a combination of these antiemetic measures (dexamethasone, droperidol, ondansetron and TIVA) are cumulative [grade A]” “For reasons of practicability, the same doses as those used for prevention are also recommended for treatment [grade D], even though for some substances (e.g. ondansetron) it has been shown that lower doses are also effective for treatment.” COI=conflict of interest; ODT=ondansetron disintegrating tablet; PONV=postoperative nausea and vomiting; TDS= transdermal scopolamine; TIVA=total intravenous anesthesia;
Anti-Emetics For Adults Experiencing Opioid-Induced Nausea 42
Appendix 8: Summary of Statistically Significant Findings (P < 0.05) from RCT Data on Ondansetron Antiemetic Combinations
Ti
me
post
sur
gery
Ond
anse
tron
Dex
amet
haso
ne
Hal
oper
idol
Ond
anse
tron
D
exam
etha
sone
Hal
oper
idol
D
exam
etha
sone
Hal
oper
idol
D
exam
etha
sone
O
ndan
setr
on
Hal
oper
idol
O
ndan
setr
on
Benevides et al., 201311 Nausea Occurrence Percent of patients
0-2hrs 56.7% 23.7% 0-36hrs 86.7% 53.3%
12-24hrs 60% 23.3% 12-24hrs 60% 26.70%
Vomiting Occurrence Percent of patients
0-36hrs 53.3% 20% Rescue Antiemetic Number received [IQR]
0-36hrs 2 [4-1] 0.5 [1-0] Time to First Rescue Percent no antiemetic











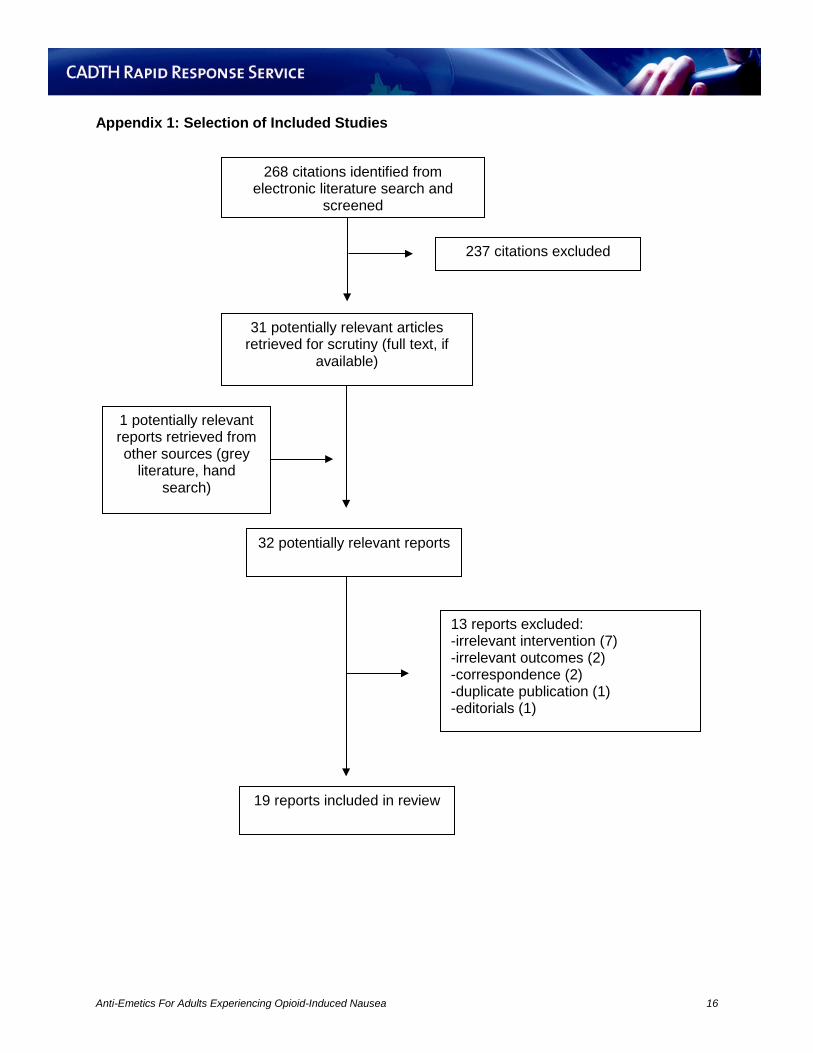

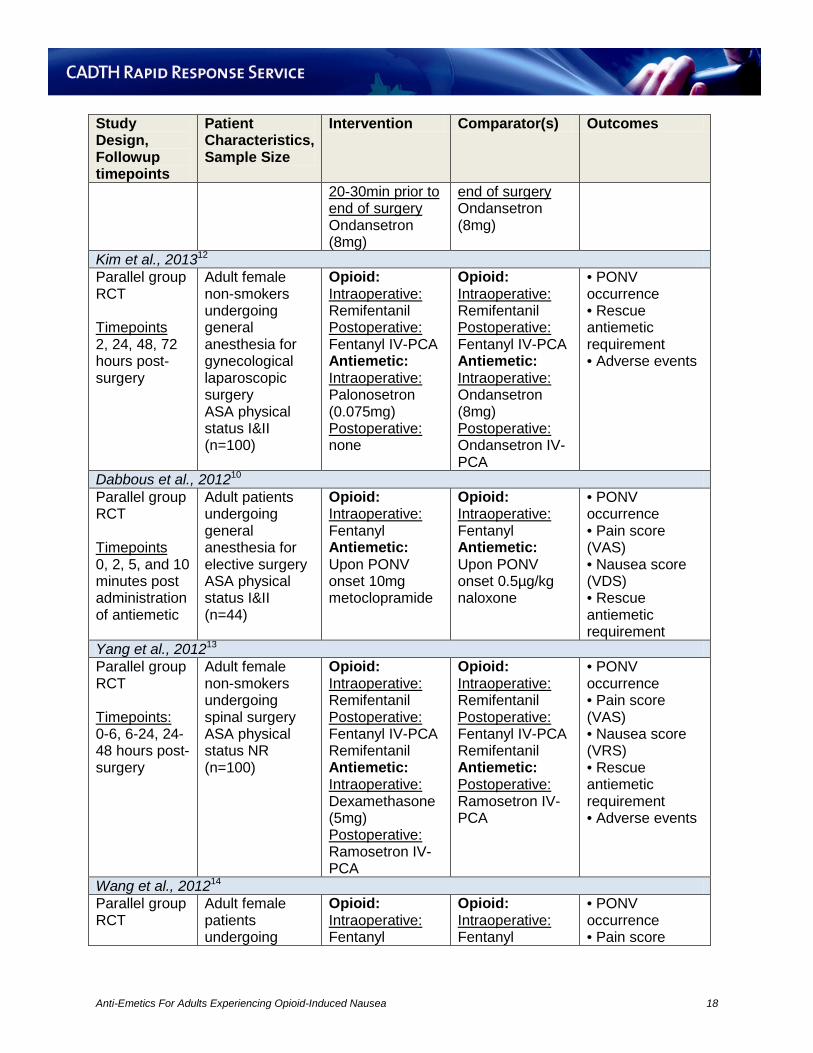

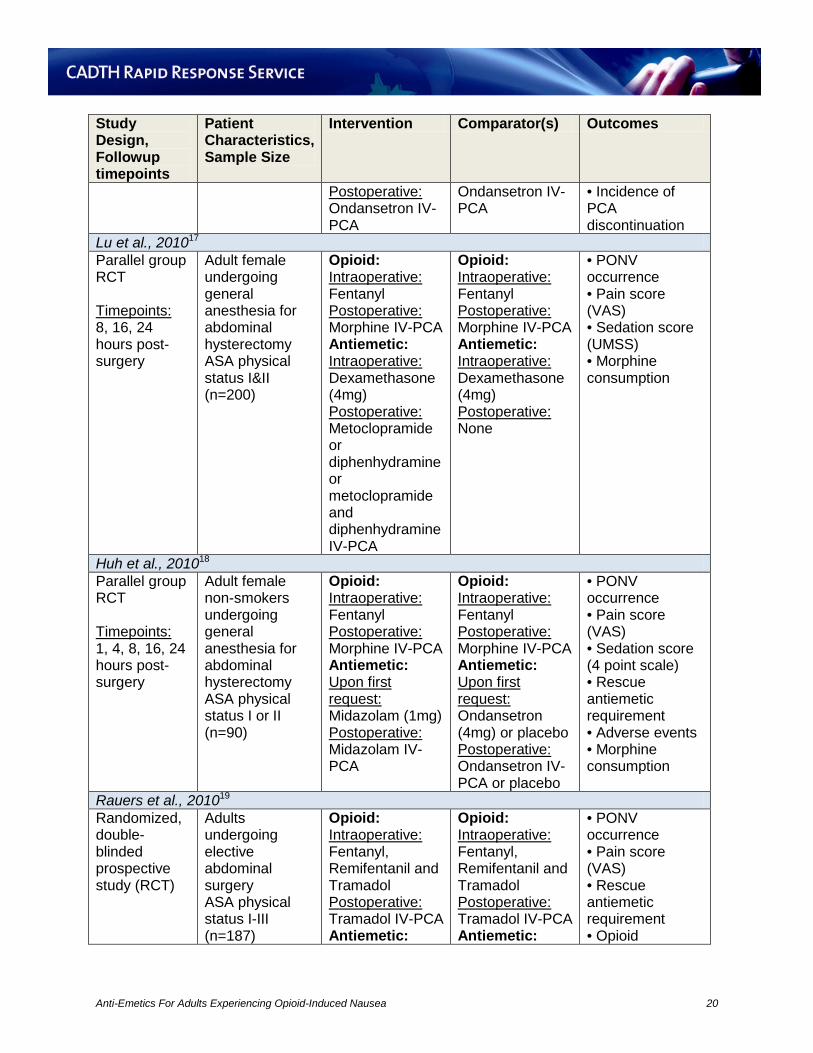



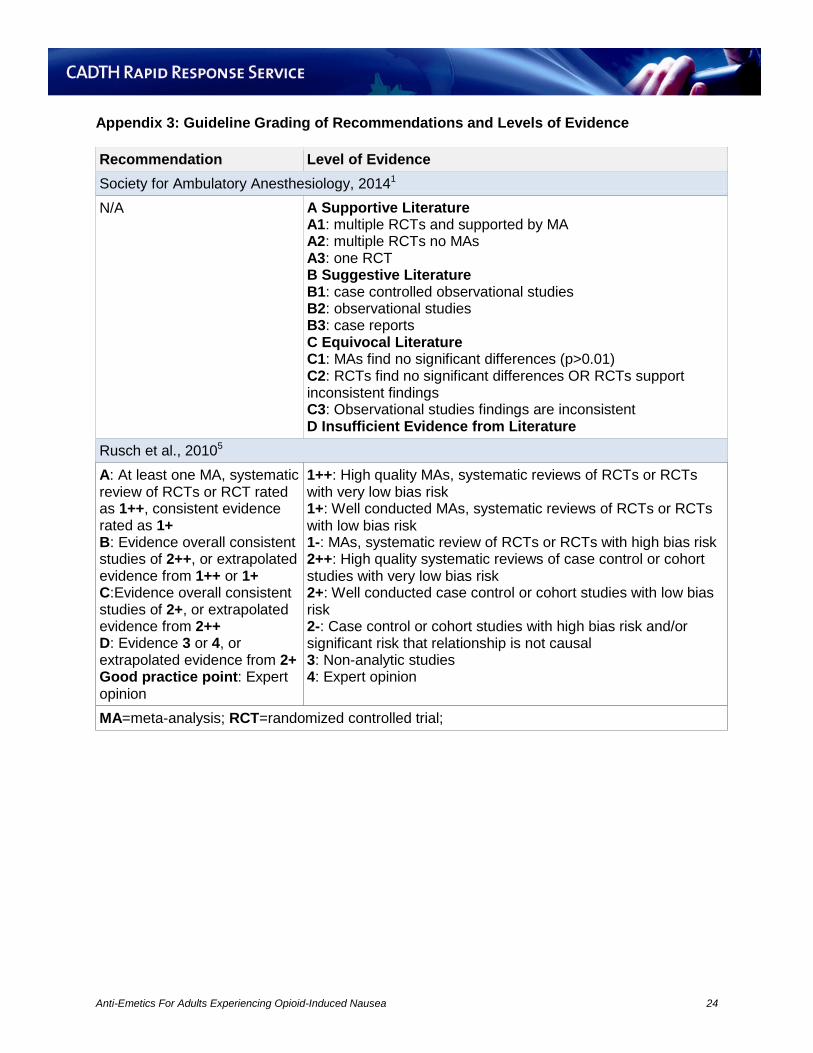

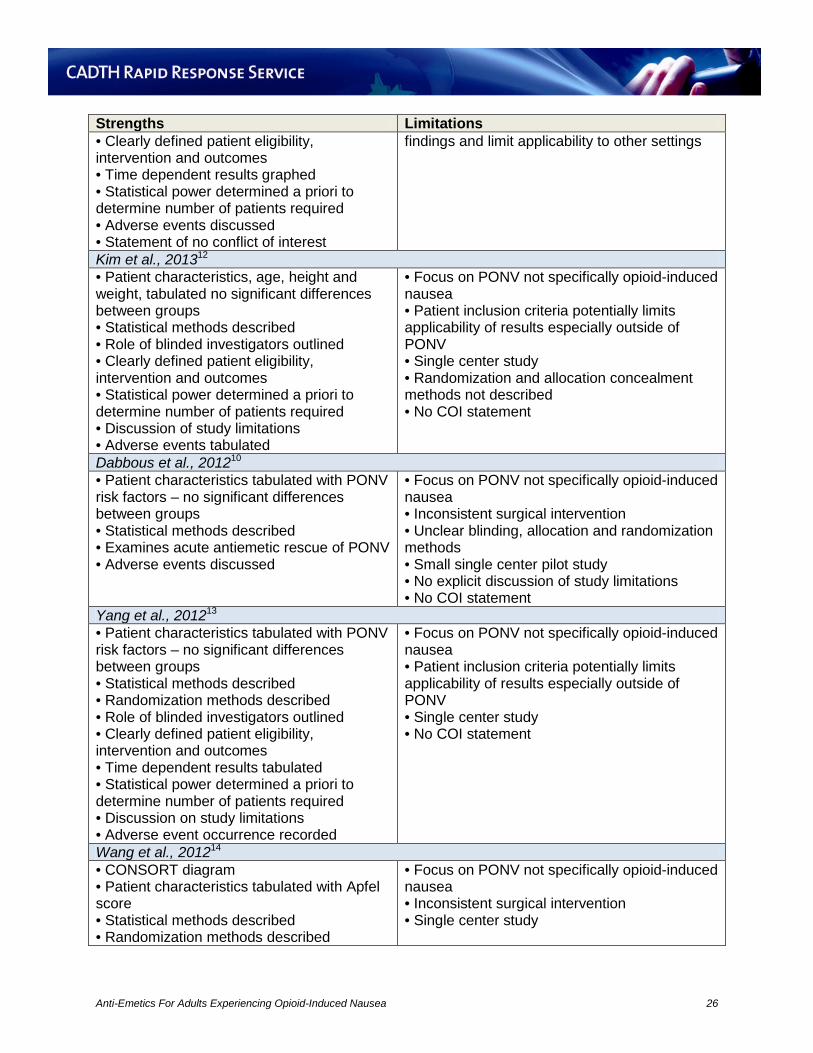


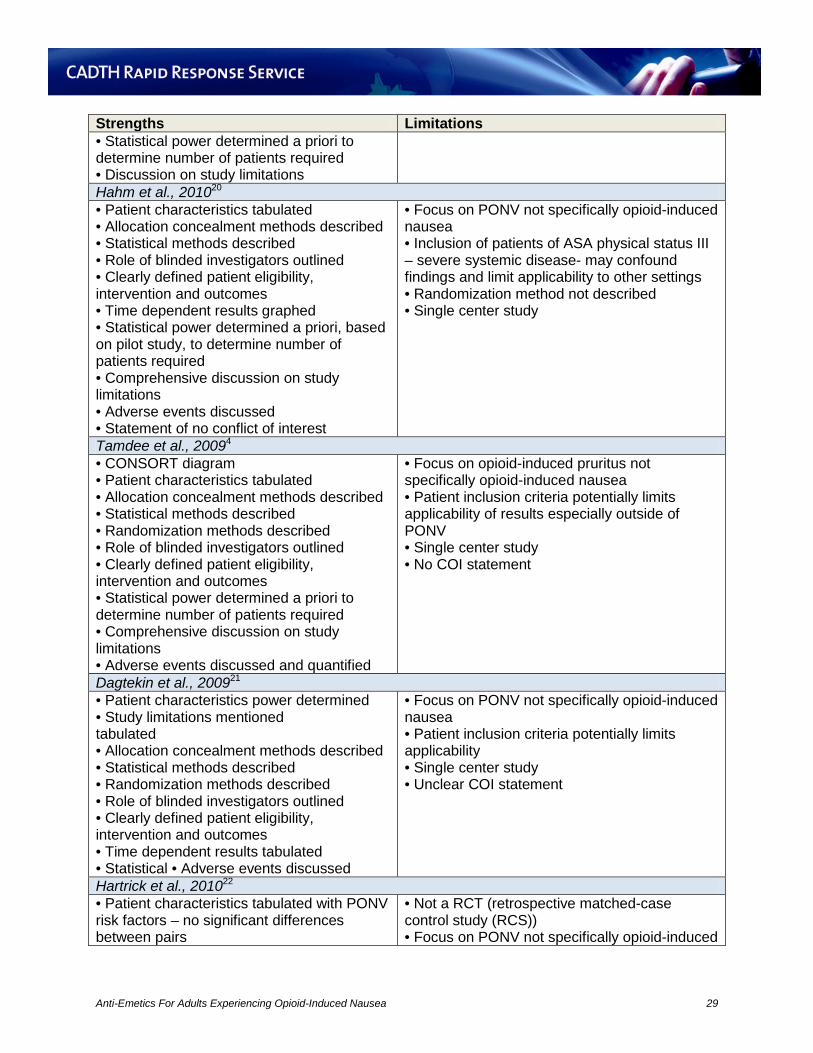


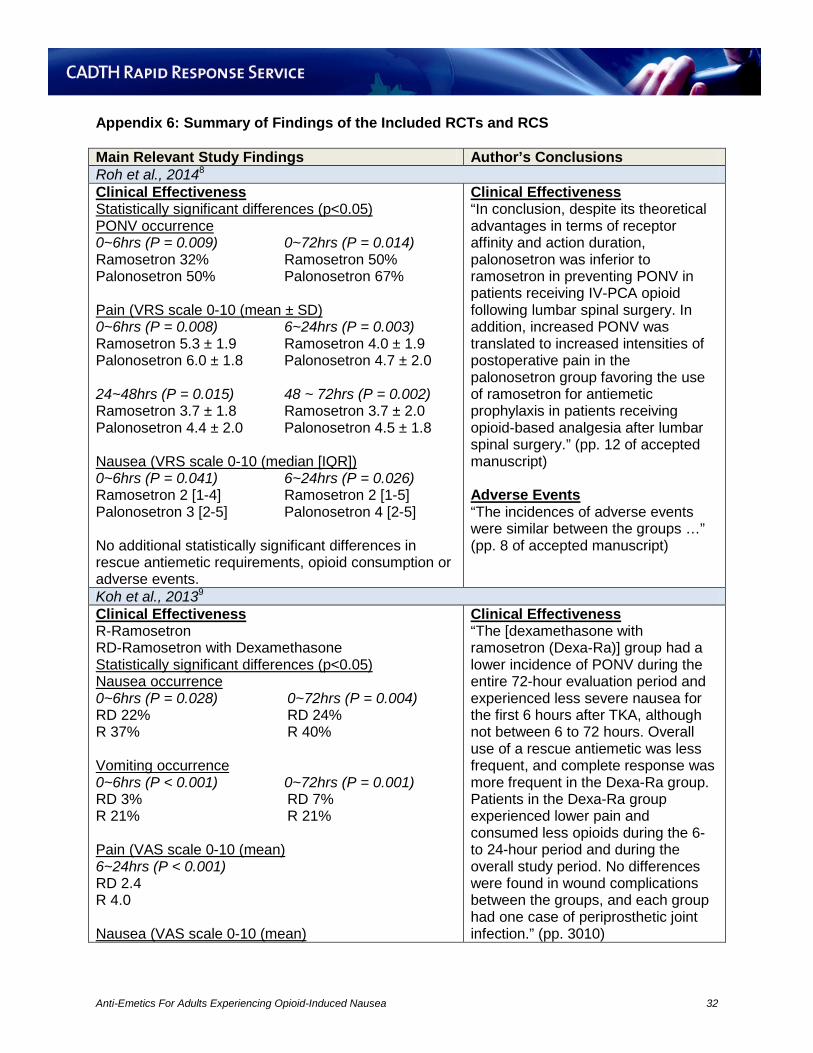

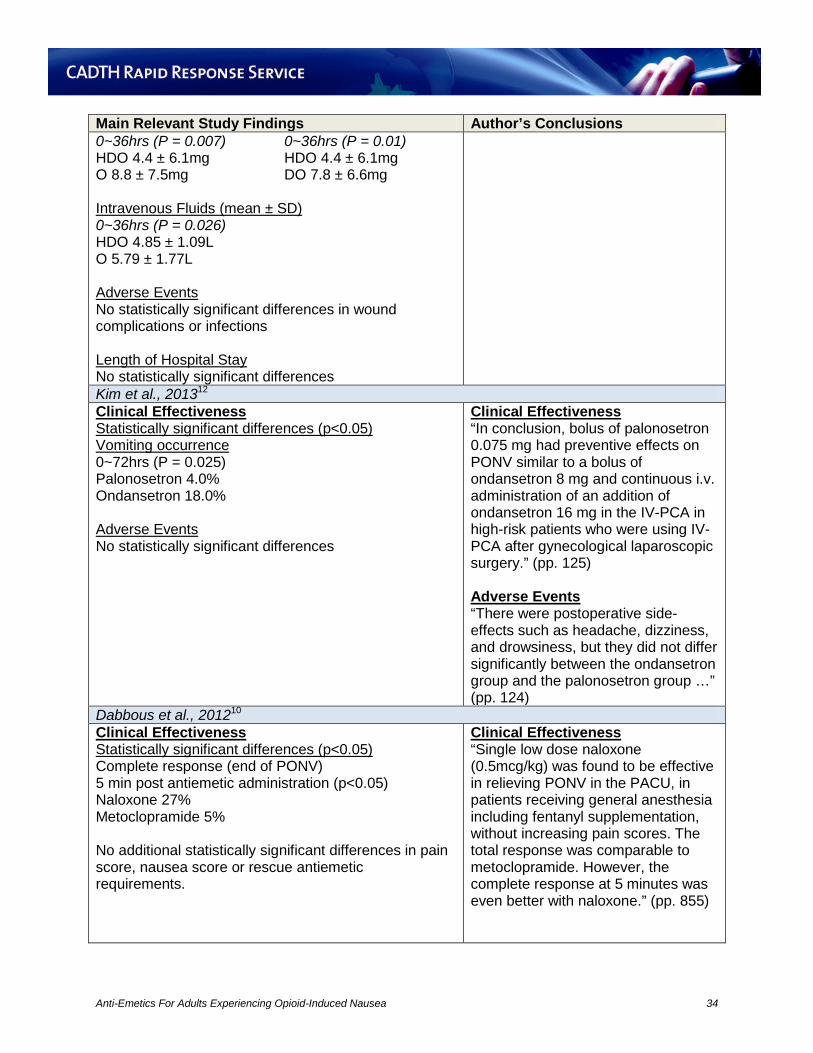
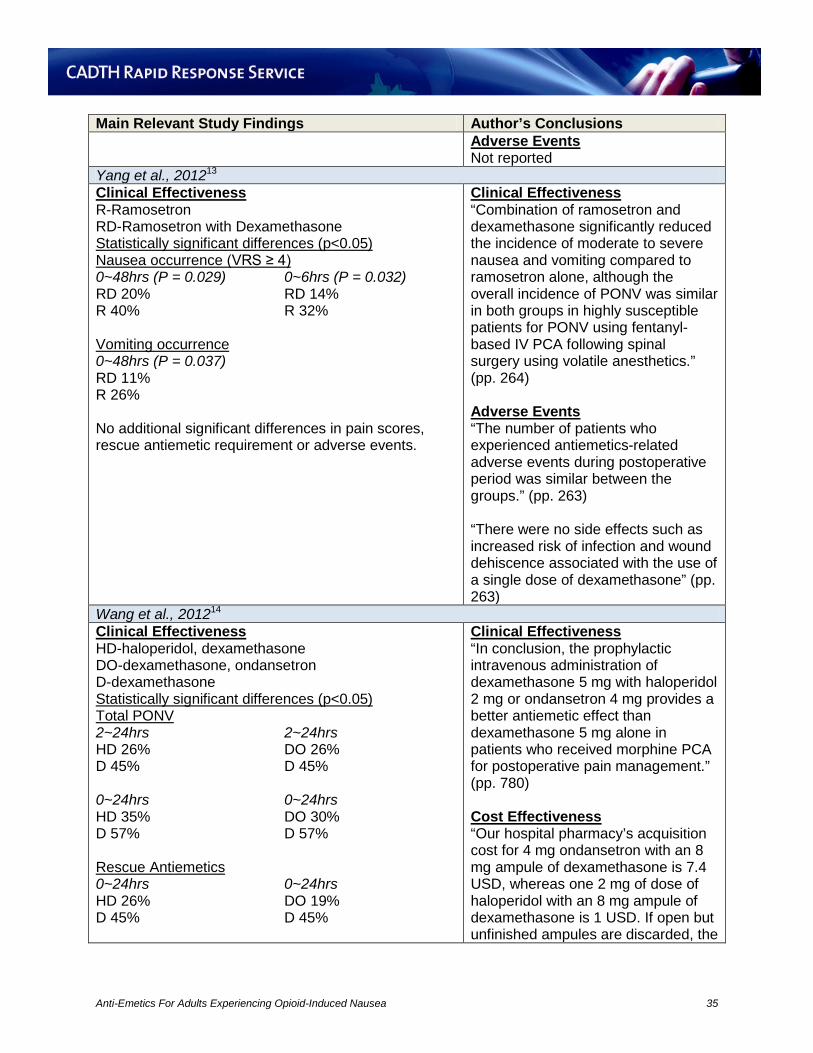



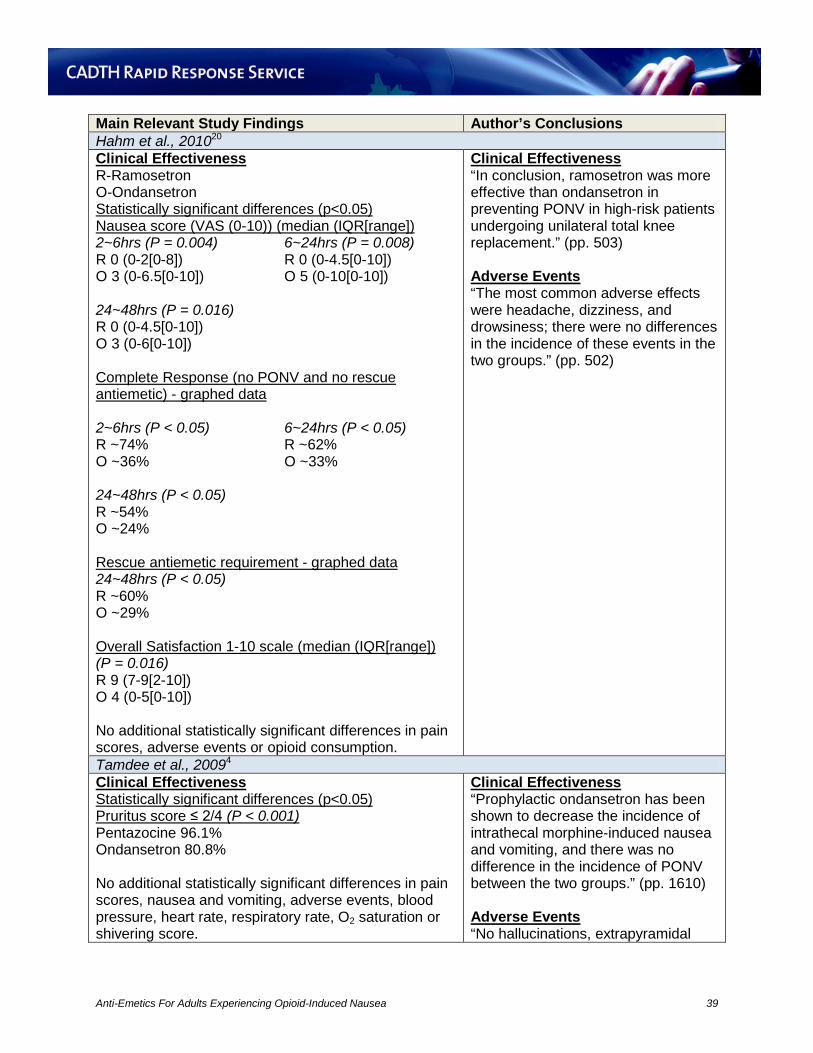









![[PPT]Anti-emetics and pro kinetics - Geegroupf2.yolasite.com/resources/Anti-emetics and pro... · Web view4. First generation H1-antagonists Drugs: meclizine, diphenhydramine and](https://static.documents.pub/doc/80x56/5aaeb49c7f8b9a59478c6939/pptanti-emetics-and-pro-kinetics-and-proweb-view4-first-generation-h1-antagonists.jpg)












