37
Antianginal Drugs Dr. Kaukab Azim. MBBS, PhD 1
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | coral-wilkerson |
| View: | 252 times |
| Download: | 0 times |

1
Antianginal Drugs
Dr. Kaukab Azim. MBBS, PhD

2
Drug List
Nitrates and nitrites Beta Blockers Calcium Channel Blockers
Amyl nitriteNitroglycerineIsosorbide mononitrate
PropranololMetoprololAtenolol
NifedipineNicardipineDiltiazemVerapamil
Note: More drugs have been mentioned in other slides

3
Angina PectorisDefinition• A clinical syndrome due to myocardial ischemia characterized by episodes of
precordial discomfort or pressure, typically precipitated by exertion or stress and relieved by rest or drugs.
Types• Exertional angina, (or angina of effort) which is typically triggered by physical
activity, persists few minutes and subsides with rest (this form constitutes about 90% of angina cases).
• Vasospastic angina (or Prinzmetal’s angina, or variant angina) which tends to occur regularly at certain times of the day and is characterized by pain at rest.
Evolution• Stable, when its characteristics are constant for a given individual.• Unstable (also called crescendo angina, acute coronary insufficiency,
preinfarction angina or intermediate syndrome), when there is an increased frequency, intensity or duration of attacks, or changes in precipitating factors. It must be treated as a medical urgency.
4
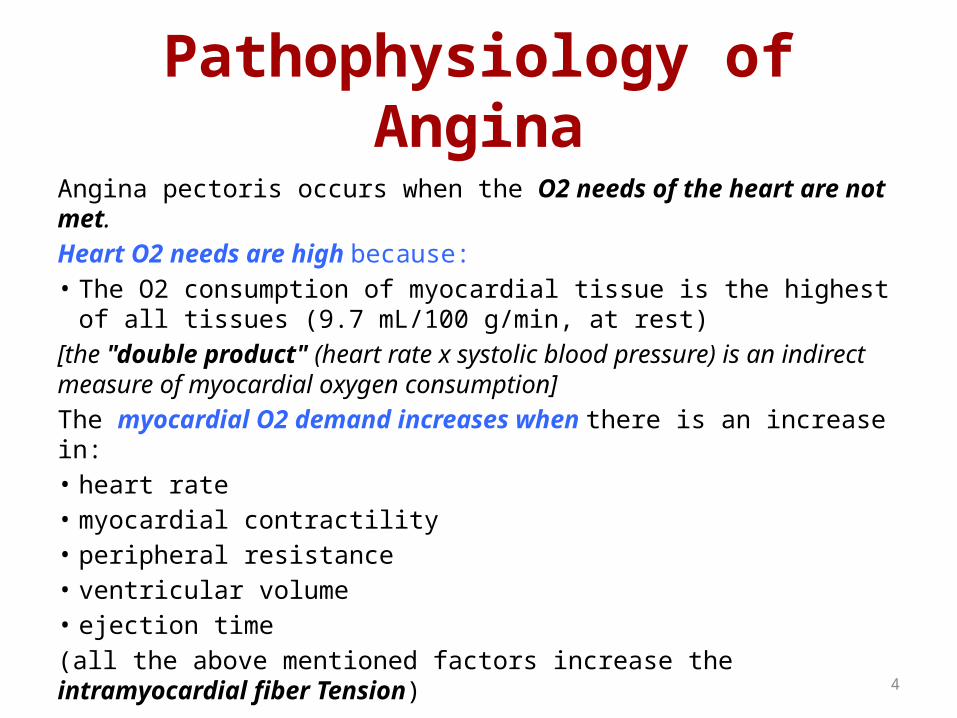
Pathophysiology of AnginaAngina pectoris occurs when the O2 needs of the heart are not met.Heart O2 needs are high because:• The O2 consumption of myocardial tissue is the highest of all tissues
(9.7 mL/100 g/min, at rest)[the "double product" (heart rate x systolic blood pressure) is an indirect measure of myocardial oxygen consumption]The myocardial O2 demand increases when there is an increase in:• heart rate• myocardial contractility• peripheral resistance• ventricular volume• ejection time(all the above mentioned factors increase the intramyocardial fiber Tension)
5
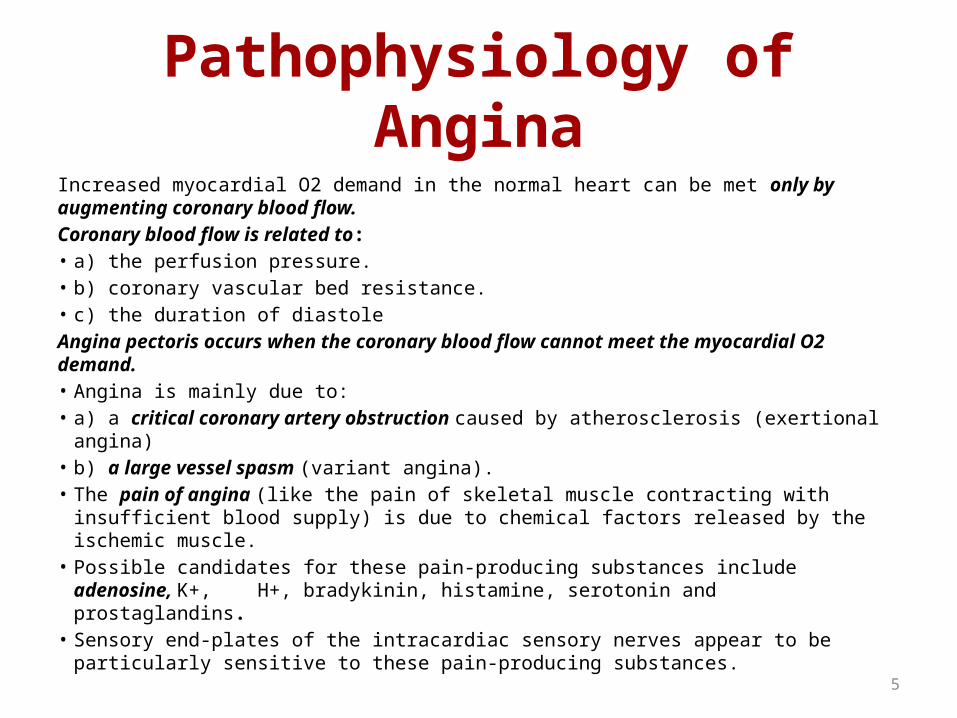
Pathophysiology of AnginaIncreased myocardial O2 demand in the normal heart can be met only by augmenting coronary blood flow.Coronary blood flow is related to:• a) the perfusion pressure.• b) coronary vascular bed resistance.• c) the duration of diastoleAngina pectoris occurs when the coronary blood flow cannot meet the myocardial O2 demand.• Angina is mainly due to:• a) a critical coronary artery obstruction caused by atherosclerosis (exertional angina)• b) a large vessel spasm (variant angina).• The pain of angina (like the pain of skeletal muscle contracting with insufficient blood
supply) is due to chemical factors released by the ischemic muscle.• Possible candidates for these pain-producing substances include adenosine, K+, H+,
bradykinin, histamine, serotonin and prostaglandins.• Sensory end-plates of the intracardiac sensory nerves appear to be particularly
sensitive to these pain-producing substances.
6
7
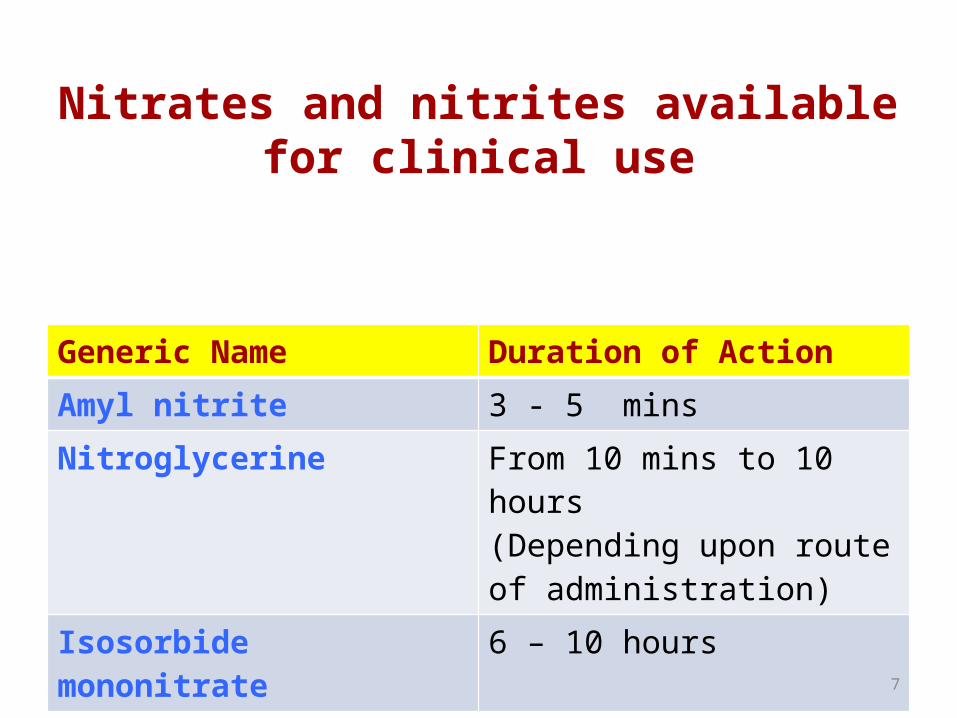
Nitrates and nitrites available for clinical use
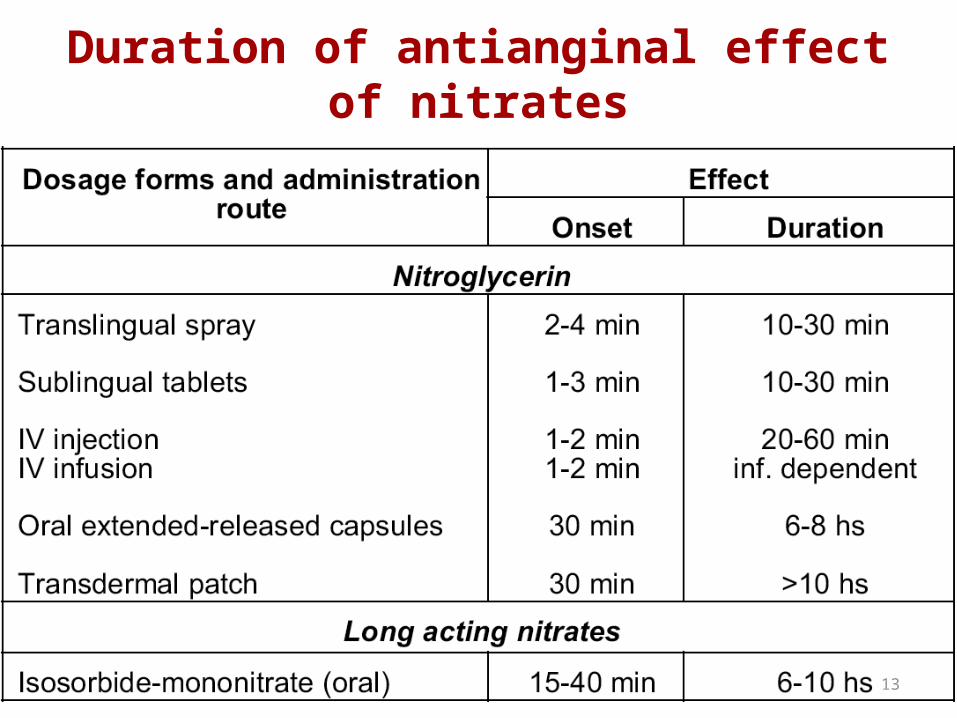
Generic Name Duration of ActionAmyl nitrite 3 - 5 minsNitroglycerine From 10 mins to 10 hours
(Depending upon route of administration)
Isosorbide mononitrate 6 – 10 hours
8
Mechanism of action of nitrates and congeners
Nitrates are denitrated (by glutathione S-transferase), thereby releasing free nitrite ions (this reaction requires -SH groups).
• Nitrite ion is converted to nitric oxide (NO), which activates a cytosolic form of guanylyl-cyclase (this reaction requires -SH groups).
• cGMP synthesis is increased in smooth muscle.
This increase in turn triggers the following cascade of events:
Activation of protein kinase G………….leading to Increased dephosphorylation of myosin light chain………….leading to relaxation of smooth muscle
Two consequences of this mechanism of action are:1) NO stimulates guanylyl-cyclase in platelets as in smooth muscle.2) A decreased availability of tissue -SH groups reduces the action of nitrates (at least partially).

9
Pharmacodynamics of nitrates and congeners
Cardiovascular actions1) After therapeutic doses: Marked relaxation of large veins (the main effect) which leads to:a. Decreased preload and cardiac output (in the absence of cardiac failure).b. Decreased blood pressure (slightly).c. Improved perfusion of subendocardial regions (due to the lowering of left
ventricular end-diastolic pressure, which reduces subendocardial compression)Relaxation of large arteries (less pronounced than vein relaxation) which leads to increased blood flow in:
d. the skin (face and thorax) and the brain.e. large epicardial vessels (autoregulation in small vessels is not impaired)f. large collateral vessels (perfusion of ischemic regions is increased)2) After higher doses:
Relaxation of all segment of the vascular system which leads to:g. Reflex tachycardia and reflex increase in cardiac contractilityh. Postural hypotension
10
Pharmacodynamics of nitrates and congeners
Other actionsRelaxation of smooth muscle of:1. the bronchi (small effect)2. the biliary system (rapid reduction of biliary pressure)3. the gastrointestinal tract (sphincteral and non sphincteral)4. the genitourinary tract (small effect)
• Decreased platelet aggregation (likely due to the increase in cGMP)
• Increased methemoglobin formation (with nitrites, not with therapeutic doses of nitrates) due to the formation of nitrite ion that can oxidize the ferrous ion of hemoglobin to the ferric state.
11
Pharmacokinetics of nitrates and congeners
ABSORPTION• Bioavailability:
• Oral: generally low (but isosorbide mononitrate > 95%)• Sublingual: 10-60 %• Transdermal: 50-90 %
DISTRIBUTION• In all body tissues including brain.BIOTRANSFORMATION• > 99%, mainly in liver (by a high capacity nitrate-reductase).Half-life: very variable• sublingual nitroglycerin: 2-3 min• oral isosorbide mononitrate: 4-5 hours
12
Nitrates Tolerance and Dependence
• Frequently repeated exposures to nitrates leads to a decrease in most of their pharmacological effects.
• Tolerance to a nitrate results in tolerance (at least partial) to all other compounds of the class.
• The amount of tolerance is a function of the dosage and the frequency of administration, and it exhibits a very high individual variability.
• Since tolerance appears rapidly (24 hours) and disappears rapidly (6-10 hours), brief periods of no therapy (hours of overnight) can be sufficient to permit recovery.
• Nitrate can cause dependence. In fact sudden death or myocardial infarction have occurred after a few days' break in long-term exposure to an organic nitrate.
13
Duration of antianginal effect of nitrates
14
Adverse effects of NitratesCentral nervous system• Throbbing headache (> 50%, can be severe)• Dizziness, vertigo, lightheadedness (5%)• Syncope (. 4%, with high doses).Cardiovascular system• Flushing of the face (common, with rapid-acting preparations, likely due to the
local production of prostaglandins).• Palpitations (with high doses).• Postural hypotension (frequent).• Profound hypotension (if taken concomitantly with sildenafil, a specific cGMP
phosphodiesterase-5 inhibitor. The interaction can be life-threatening).Other systems• Skin rashes, contact dermatitis (rare)• Methemoglobinemia (with nitrite, or with toxic doses of nitrates) (very rare)• Withdrawal reactions (digital vasospasm, coronary spasms, myocardial
ischemia, myocardial infarction)• Drug abuse (with amyl nitrite)
15
Nitrates: Contraindications and Precautions
• Angina due to hypertrophic Cardiomyopathy• Constrictive pericarditis• Increased intracranial pressure• Severe hypotension (systolic < 90 mm Hg)• Hypovolemic states• Hyperthyroidism• Severe hepatic disease
16
Therapeutic uses of nitratesAngina pectoris
a) Treatment (or prevention) of the acute attack.Nitroglycerin (sublingual route) or amyl nitrite (inhalant route). [pain is relieved; protection lasts 30-40 min].b) Chronic prophylaxisNitroglycerin (oral, transdermal), other nitrates (oral) [attacks are reduced or eliminated].
Main mechanisms of antianginal effects:a) In exertional angina: decreased myocardial O2 demandb) In variant angina: increased myocardial O2 supply (they are not the treatment of choice)c) In unstable angina: The main mechanism is still uncertain (decreased myocardial O2 demand, increased myocardial O2 supply, and decreased platelet aggregation, all might contribute to the therapeutic efficacy).
High doses may cause undesirable effects due to:reflex tachycardiareflex increase in cardiac contractility
17
Therapeutic uses of Nitrates
Heart failureUnlike in normal subjects, nitrates can increase stroke volume and cardiac output in patients with systolic heart failure (the decreased preload lowers the ventricular filling pressure, so allowing a more efficient ventricular contraction).
They are not used routinely in heart failure but can be used when:① symptoms of pulmonary congestion predominate
(redistribution of blood volume away from the chest relieves the congestion. This improves exercise tolerance even when cardiac output is not increased)
② pulmonary edema occurs or is impending.
18
Therapeutic uses of Nitrates
Myocardial infarction• It has been shown that IV infusion of nitrates lead
only to a minor reduction in short-term mortality.• Therefore they are not recommended for routine
use, but it is reasonable to use IV nitroglycerin in more complicated patients, such as those with impending heart failure or hypertension.
Cyanide poisoning

19
Beta blockers
20
Beta-blockers in Angina1) Therapeutic doses of beta-blockers are effective in angina because:
a) They decrease cardiac O2 demand (the main mechanism) by:reducing heart ratereducing cardiac contractilitylowering blood pressure
b) They increase myocardial perfusion in certain parts of the heart (mainly subendocardial regions) due to an augmented diastolic perfusion time.
Therefore:a) They are effective in chronic prophylaxis of exertional angina and in the acute treatment of unstable angina.b) They are not effective in variant angina (where instead they may be dangerous, by causing coronary vasoconstriction).
2) High doses may cause undesirable effects due to: increased end diastolic volume increased ejection time

21
Beta-blockers in Myocardial Infarction
Beta-blockers without sympathomimetic activity have been clearly demonstrated to reduce mortality in myocardial infarction. They should be given early and continued indefinitely.
The mortality reduction is likely due to the following reasons:1) They decrease myocardial oxygen demand (by decreasing heart contractility and rate)2) They decrease the risk of ventricular fibrillation (by decreasing heart conduction and automaticity).3) They limit the infarct size (so decreasing the risk of myocardial rupture)4) They reduce myocardial remodeling (which is enhanced by catecholamines and angiotensin II).
Warning! withdrawal effects after chronic use of beta blockers in ischemic heart disease are well documented. In risk patients abrupt withdrawal may cause hypertension, angina, myocardial infarction, and sudden death.

22
To understand the rest of the lecture, you must know the role of calcium in muscle contraction
and relaxation
Calcium Channel Blockers
23
The Calcium Channels
There are two types of calcium channels
a) Ligand-gated (or "receptor-operated"): they are coupled to excitatory receptors either directly or via G proteins and open when the receptor is activated.
b) Voltage-gated (or "potential-operated"): they open when the cell is depolarized.
24
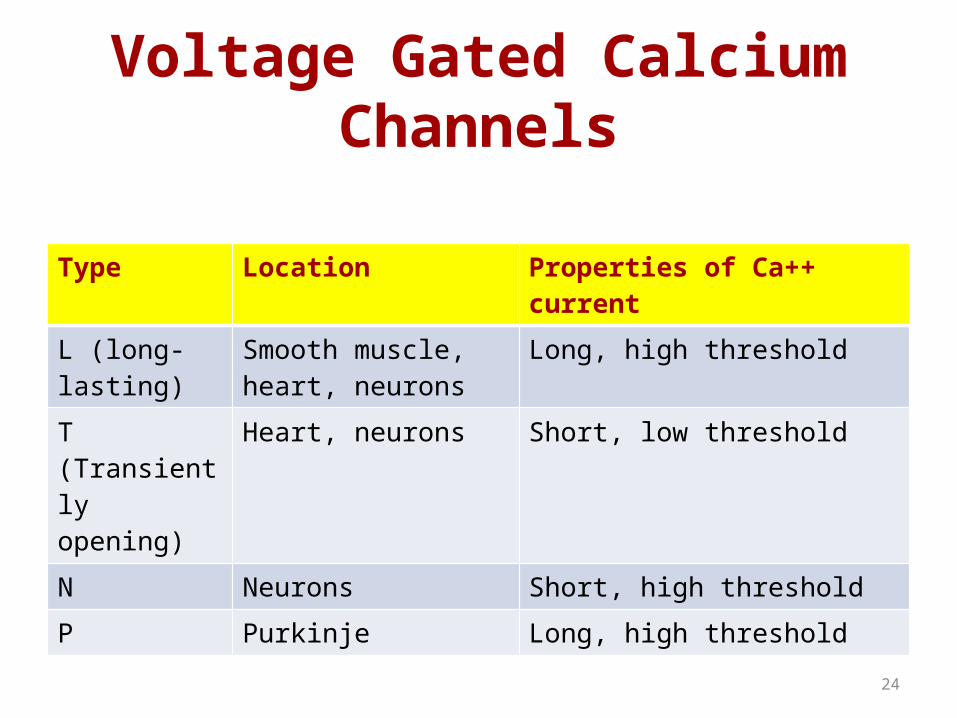
Voltage Gated Calcium Channels
Type Location Properties of Ca++ currentL (long-lasting) Smooth muscle, heart,
neuronsLong, high threshold
T (Transiently opening)
Heart, neurons Short, low threshold
N Neurons Short, high thresholdP Purkinje Long, high threshold

25
Classification of Ca++ Channel Blocking Drugs
Dihydropyridines Others
Drug Vascular Selectivity Drug Vascular
SelectivityNifedipine High Verapamil LowNicardipine Very High Diltiazem Low
Bepridil Absent

26
Pharmacodynamics
Mechanism of action• Calcium channel blockers bind to the voltage-gated Ca++
channel of L-type from the inner side of the membrane. • Verapamil and diltiazem block Ca++ channels both in the
heart and in the vessels.• Dihydropyridines block Ca++ channels in the vessels
only.• Blockade can be reversed (at least partially) by drugs
that increase transmembrane flux of Ca++, such as beta-1 agonists.
27
Cardiac and Vascular ActionsCardiac actions(Only verapamil and diltiazem can cause these effects)• Decreased conduction (in "slow fibers").• Increased refractoriness (markedly, but only in "slow fibers" or in fibers that fire
frequently and are incompletely polarized at rest).• Decreased automaticity (mainly in ischemic zones, by preventing Ca++ overload).• Dose-dependent decrease of cardiac contractility.
Vascular actions(All Ca++ channel blockers can cause these effects)• Vasodilation (mainly in arterioles, where the calcium-dependent tone of the
smooth muscle is more pronounced).• Some dihydropyridines have a relative vascular selectivity (nicardipine for
cerebral and coronary vessels)

28
Other Actions
Other actions• Relaxation of bronchiolar, gastrointestinal and
uterine smooth muscle (modest).• Inhibition of insulin release (verapamil,
nifedipine, after very high doses)• Inhibition of platelet aggregation (in vitro)• Blockade of P-glycoprotein which is a multidrug
transporter associated with the development of drug resistance in cancer cells (verapamil).
29
Pharmacokinetics
ABSORPTIONOral bioavailability: variable (verapamil: 30% ) (amlodipine: 80%)Oral Tmax: 30-60 min.
DISTRIBUTIONIn all tissues including brain.
BIOTRANSFORMATION> 99% in liver and other organs. Some metabolites are active.
EXCRETION< 1 % excreted by the kidney.
Half-life: very variable(Diltiazem: . 3 hours; amlodipine . 40 hours)
30
Adverse EffectsCentral Nervous System• Headache (up to 20%)• Dizziness, lightheadedness (up to 20%), weakness (up to 10%).Cardiovascular System• Flushing (nifedipine up to 25%).• Peripheral edema (nifedipine, up to 50%)• Profound hypotension (mainly with immediate-release nifedipine)• Tachycardia, palpitations (nifedipine, . 5%).• A-V block, bradycardia, arrhythmias (verapamil, diltiazem, .2%).• Ventricular fibrillation (verapamil, diltiazem, in patients with accessory AV
pathways)• Aggravation of myocardial ischemia (nifedipine .10%).Other systems• Constipation (verapamil, up to 40%), gingival hyperplasia (verapamil up to 19%)
nausea, heart burn, abdominal pain (up to 10%).
31
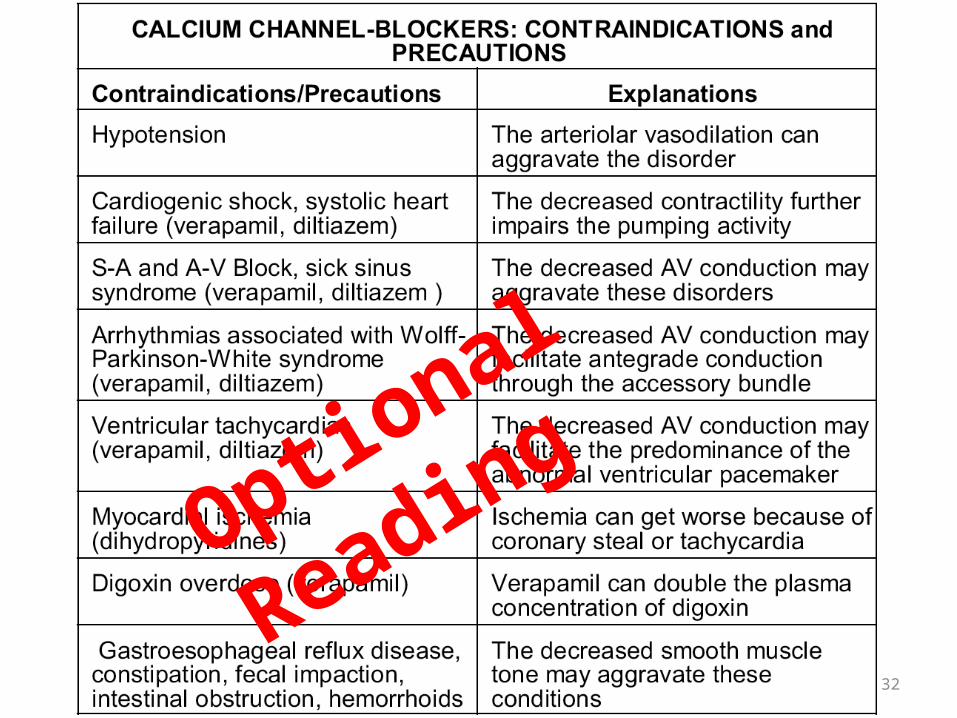
Contraindications and Precautions
• Hypotension• Cardiogenic shock, systolic heart failure (verapamil, diltiazem)• SA and AV block, sick sinus syndrome (verapamil, diltiazem)• Arrhythmias associated with Wolff-Parkinson-White
syndrome (verapamil, diltiazem)• Ventricular tachycardia (verapamil, diltiazem)• Myocardial ischemia (dihydropyridines)• Digoxin overdose • GERD, constipation, fecal impaction, intestinal obstruction,
hemorrhoids
(you must remember the ones in blue)
32
Optional Reading
33
Therapeutic Uses
Angina pectoris
a) Exertional angina mainly because they decrease myocardial O2demand (due to decreased afterload, heart rate and contractility)
Verapamil and diltiazem are the preferred drugs.High doses may cause undesirable effects due to:
increased end diastolic volumethe increased ejection time
b) Variant angina mainly because they increase myocardial O2 supply (due to coronary vasodilation)
All calcium channel blockers are considered drugs of choice:High doses of dihydropyridines may cause undesirable effects due to:
reflex tachycardiareflex increase in cardiac contractility
34
Therapeutic Uses
Unstable angina and myocardial infarction• During myocardial ischemia, an increase in Ca++ influx (due
to membrane depolarization) can trigger a secondary cellular damage.
• A cytoprotective effect, due to a decrease in the amount of necrosis in the heart tissue, has not been consistently supported by clinical studies, but these drugs can reduce the rate of reinfarction and death in patients without heart failure.
Cardiac arrhythmiasHypertension
35
Therapeutic UsesHypertrophic cardiomyopathy and diastolic heart failure• Diltiazem (alone or in combination with beta-blockers) improves diastolic compliance
by reducing myocardial contractility.
Subarachnoid hemorrhage• Dihydropyridines (especially nicardipine) dilate cerebral vessels at doses that have
little effects in the periphery. Therefore they inhibit delayed reactive vasospasm arising from hemorrhage.
Raynaud's phenomenon• They are drugs of choice for relieving peripheral vasospasm.
Migraine• They are sometimes used for migraine prophylaxis (mechanism not established).
Neuropsychiatric disorders• Various neuropsychiatric disorders (rapid-cycling bipolar disorder, Tourette’s disease,
Huntington’s disease). Long term-efficacy in these disorders remains to be established.
36
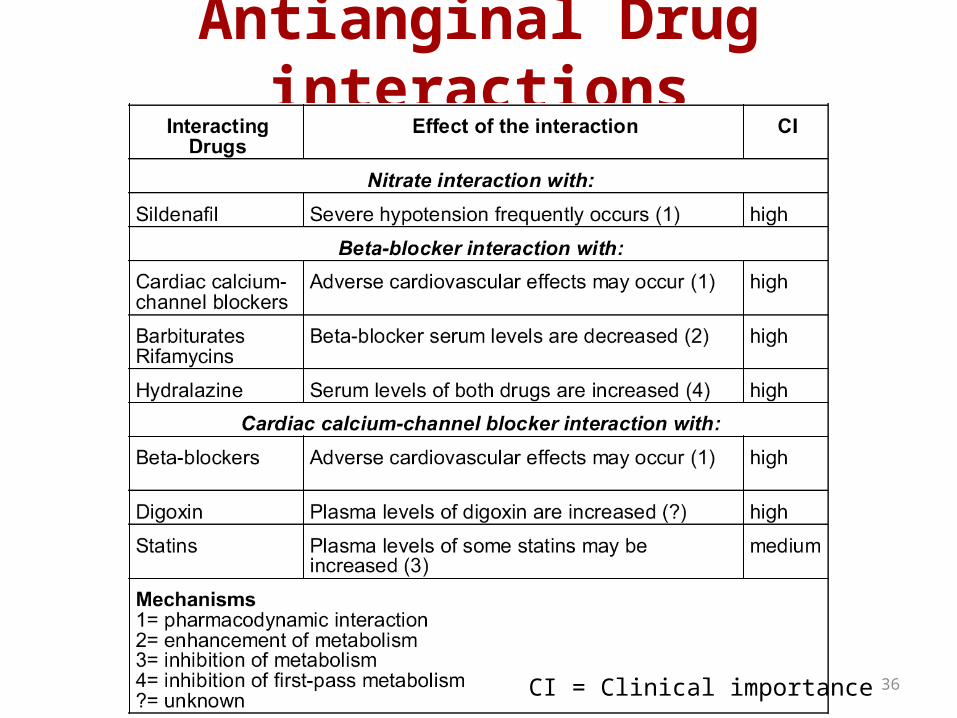
Antianginal Drug interactions
CI = Clinical importance
37
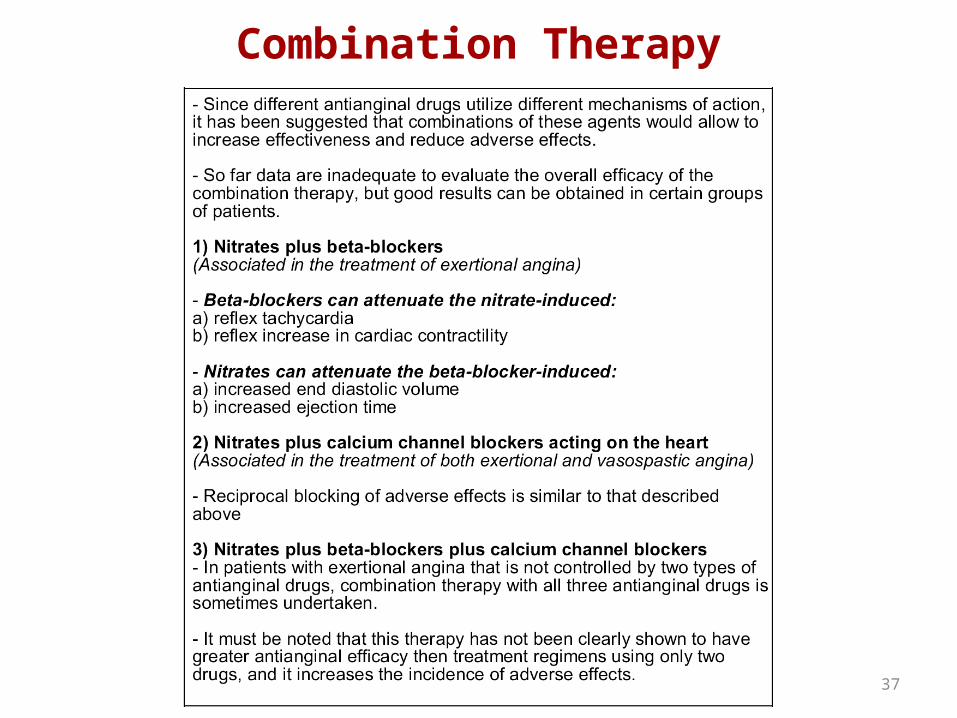
Combination Therapy

















