46
ANTICOAGULANTI ORALI DIRETTI: Caso clinico in Neurologia Silvia Ros SOC Neurologia Azienda Per i Servizi Sanitari N. 2 Bassa Friulana-Isontina
| Date post: | 13-Mar-2019 |
| Category: |
Documents |
| Upload: | truongkhuong |
| View: | 215 times |
| Download: | 0 times |

ANTICOAGULANTI ORALI
DIRETTI:
Caso clinico in Neurologia
Silvia Ros
SOC Neurologia
Azienda Per i Servizi Sanitari N. 2 Bassa Friulana-Isontina
‘Scoagulare’ ‘Riscoagulare’
‘Non scoagulare’
that is the question
…. E con quali farmaci
Aurelio E 77 anni
• FA permanente in Warfarin
• Ipertensione arteriosa
• 2015 Accesso in PS: Improvvisa comparsa afasia globale e deficit stenico arto superiore dx
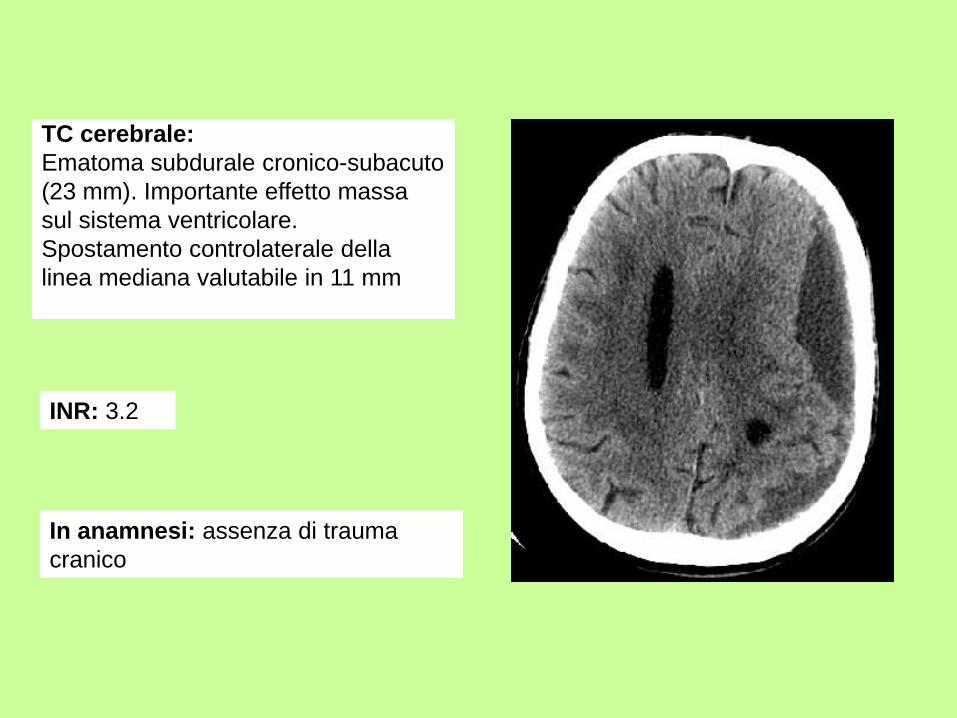
TC cerebrale:
Ematoma subdurale cronico-subacuto
(23 mm). Importante effetto massa
sul sistema ventricolare.
Spostamento controlaterale della
linea mediana valutabile in 11 mm
In anamnesi: assenza di trauma
cranico
INR: 3.2
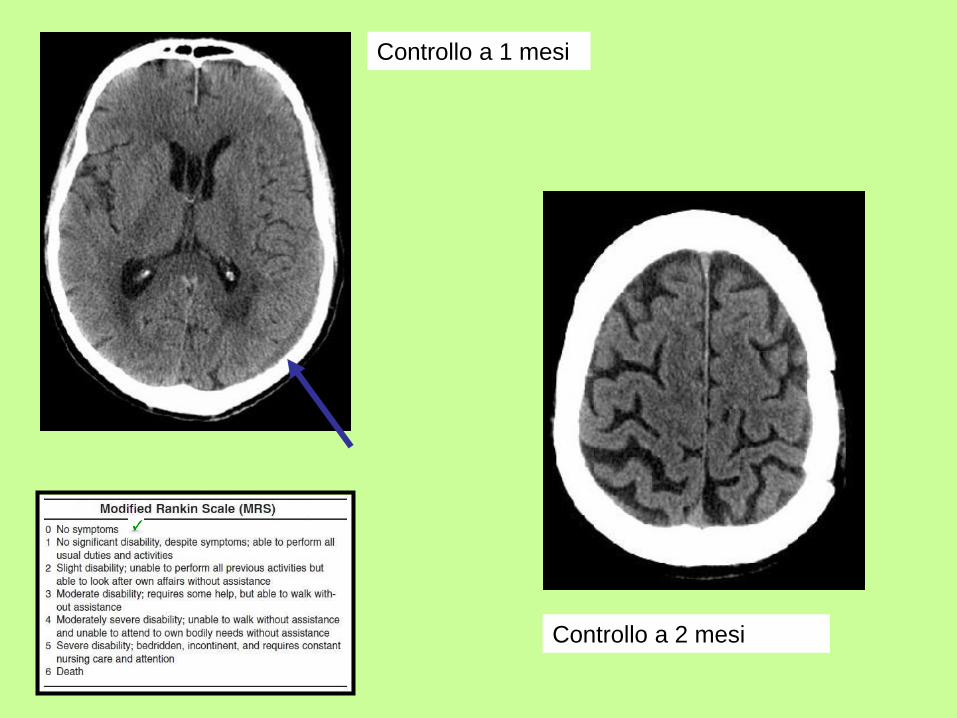
Controllo a 1 mesi
Controllo a 2 mesi
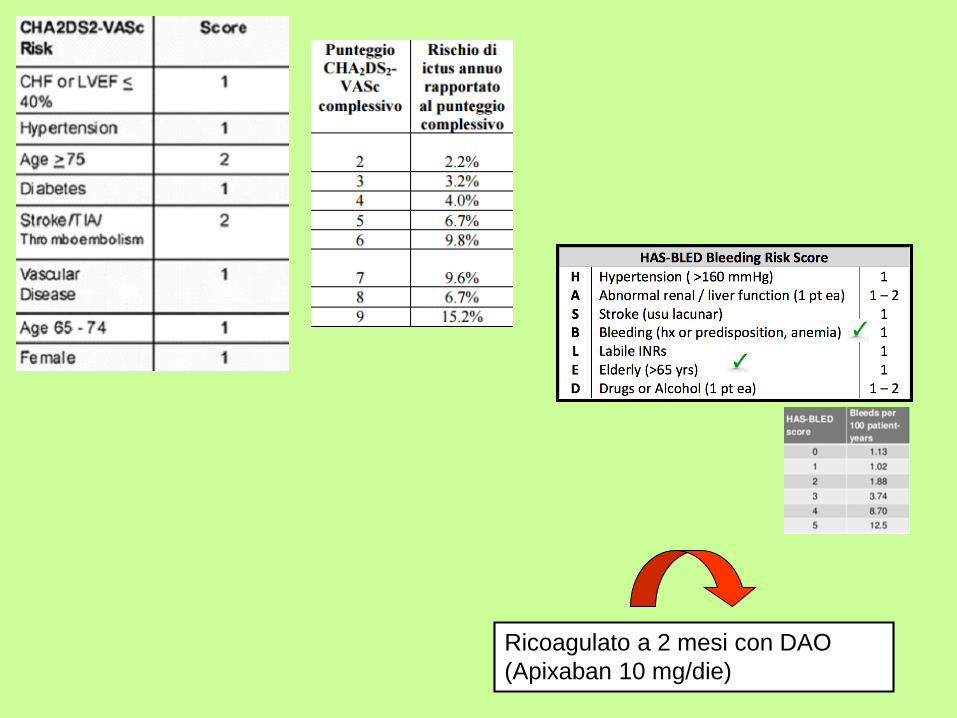
Ricoagulato a 2 mesi con DAO
(Apixaban 10 mg/die)
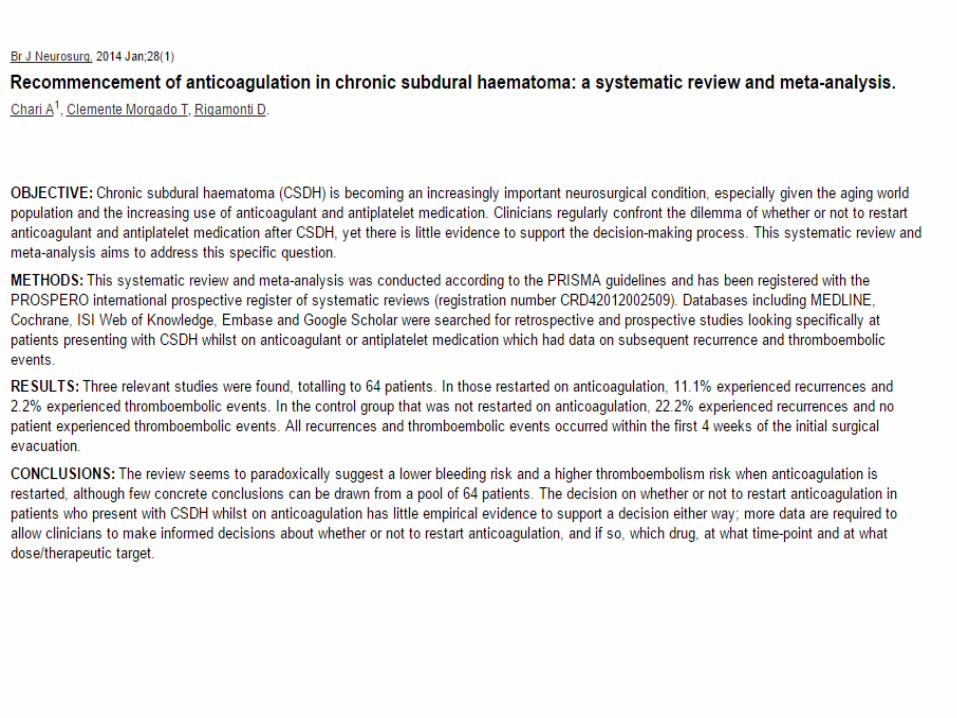

The safety and efficacy of resumption of oral anticoagulation versus long-term discontinuation has not been
fully clarified in patients who experienced SDH while under treatment with oral anticoagulation.
We investigated the outcome of 49 patients SDH while receiving oral anticoagulation.
Most bleeding occurred while patients were within the recommended therapeutic window for oral
anticoagulation.
Mortality was 15%. The event-free survival probability was higher in the group of patients with reinstitution of
phenprocoumon therapy than in the group without.
Over a median follow-up of 32 months, thromboembolic events occurred in 4 of 23 patients without oral
anticoagulation versus in none of 15 patients with phenprocoumon; hemorrhagic complications occurred in 1 in
23 versus 3 in 15 patients.
Conclusions Reinstitution of oral anticoagulation with phenprocoumon after previous SDH appears to have an
acceptable risk for hemorrhagic complications.
Decision making might consider case-by-case differences.
To establish specific guidelines, prospective large cohort studies are needed.
J Neurol Surg A Cent Eur Neurosurg 2015, Aug 20
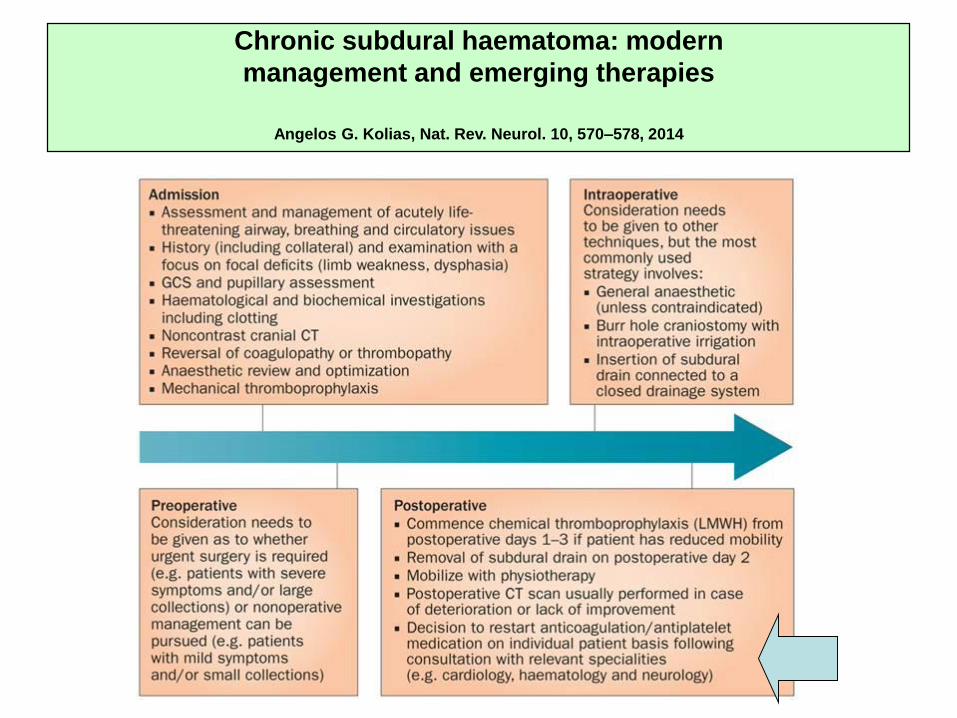
Chronic subdural haematoma: modern
management and emerging therapies
Angelos G. Kolias, Nat. Rev. Neurol. 10, 570–578, 2014
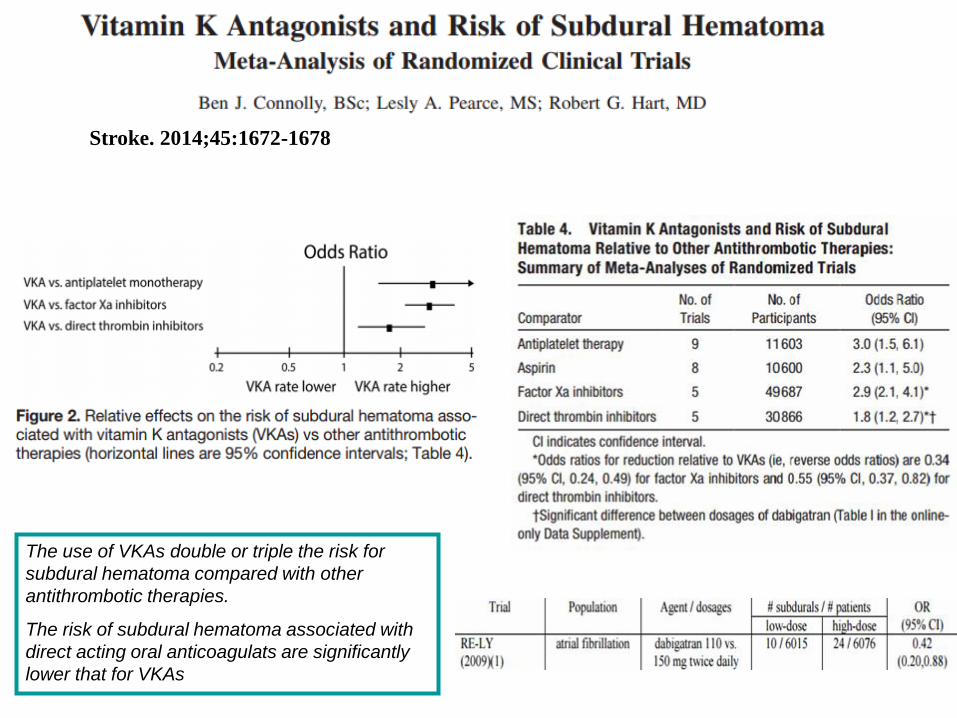
Stroke. 2014;45:1672-1678
The use of VKAs double or triple the risk for
subdural hematoma compared with other
antithrombotic therapies.
The risk of subdural hematoma associated with
direct acting oral anticoagulats are significantly
lower that for VKAs
• Ipertensione arteriosa
• Cardiopatia ischemico ipertensiva
• Dislipidemia
• Fibrillazione atriale permanente.
• TAO (Warfarin) fino al 2013 poi DAO (Rivaroxaban 20 mg).
Danilo.G., 76 anni
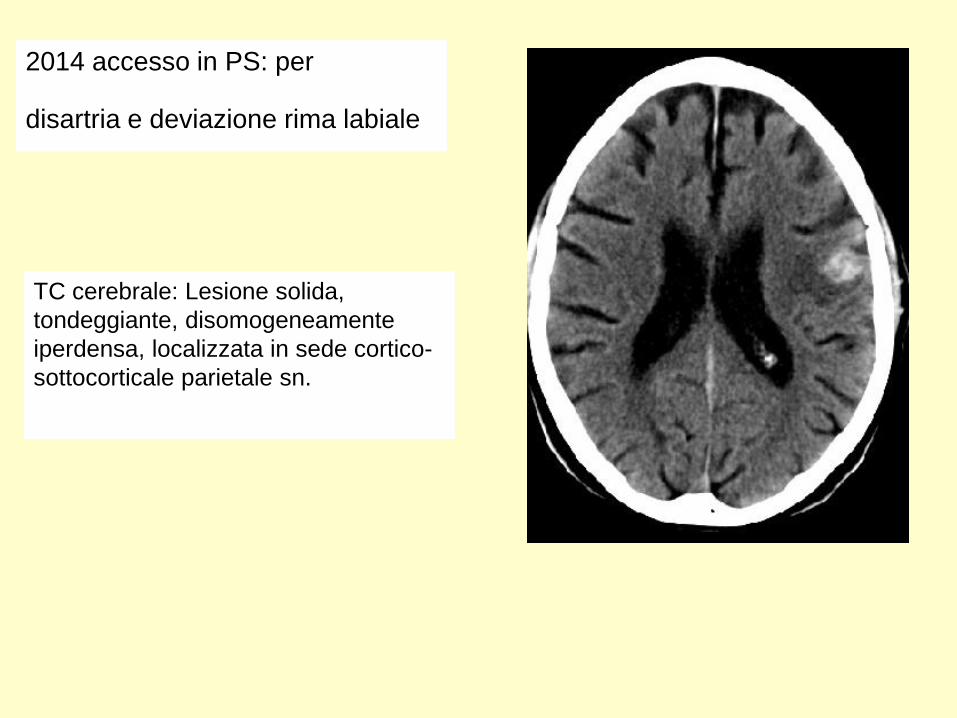
TC cerebrale: Lesione solida,
tondeggiante, disomogeneamente
iperdensa, localizzata in sede cortico-
sottocorticale parietale sn.
2014 accesso in PS: per
disartria e deviazione rima labiale
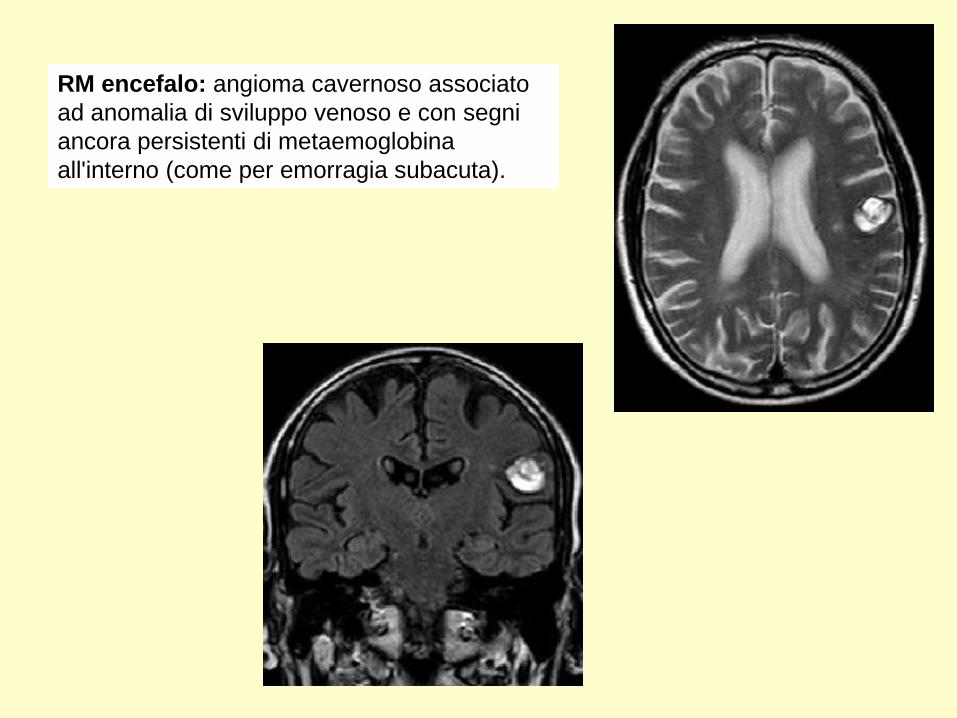
RM encefalo: angioma cavernoso associato
ad anomalia di sviluppo venoso e con segni
ancora persistenti di metaemoglobina
all'interno (come per emorragia subacuta).
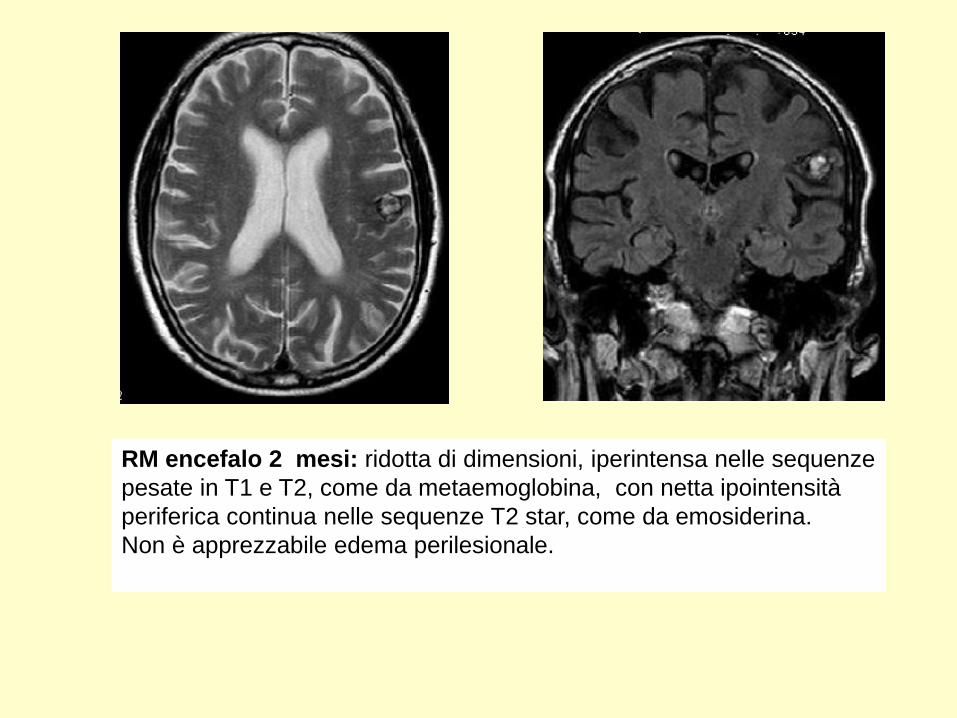
RM encefalo 2 mesi: ridotta di dimensioni, iperintensa nelle sequenze
pesate in T1 e T2, come da metaemoglobina, con netta ipointensità
periferica continua nelle sequenze T2 star, come da emosiderina.
Non è apprezzabile edema perilesionale.
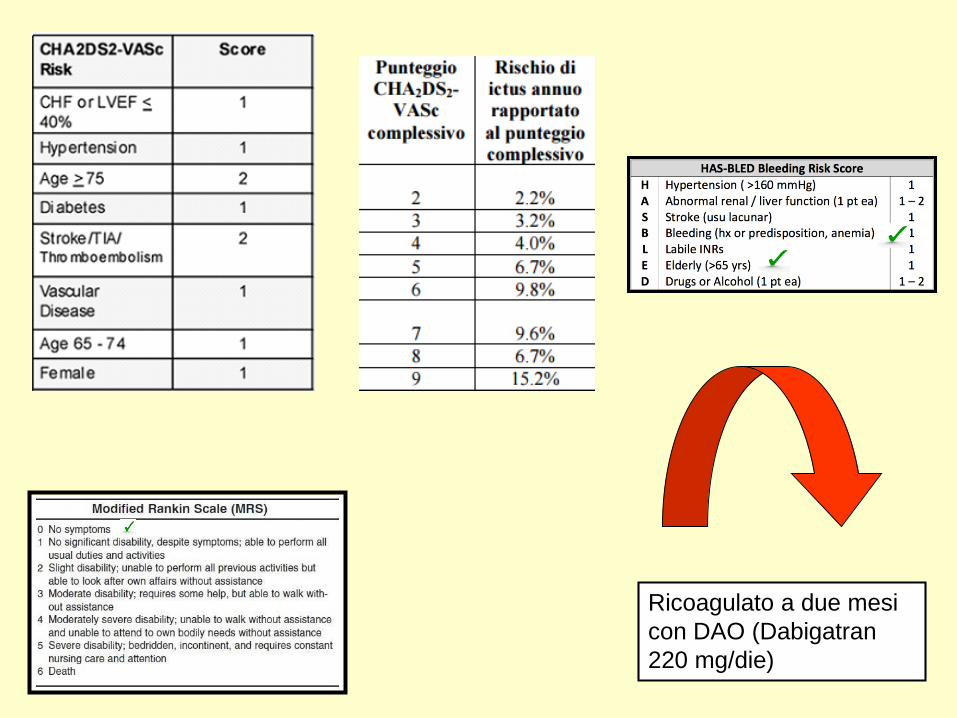
Ricoagulato a due mesi
con DAO (Dabigatran
220 mg/die)
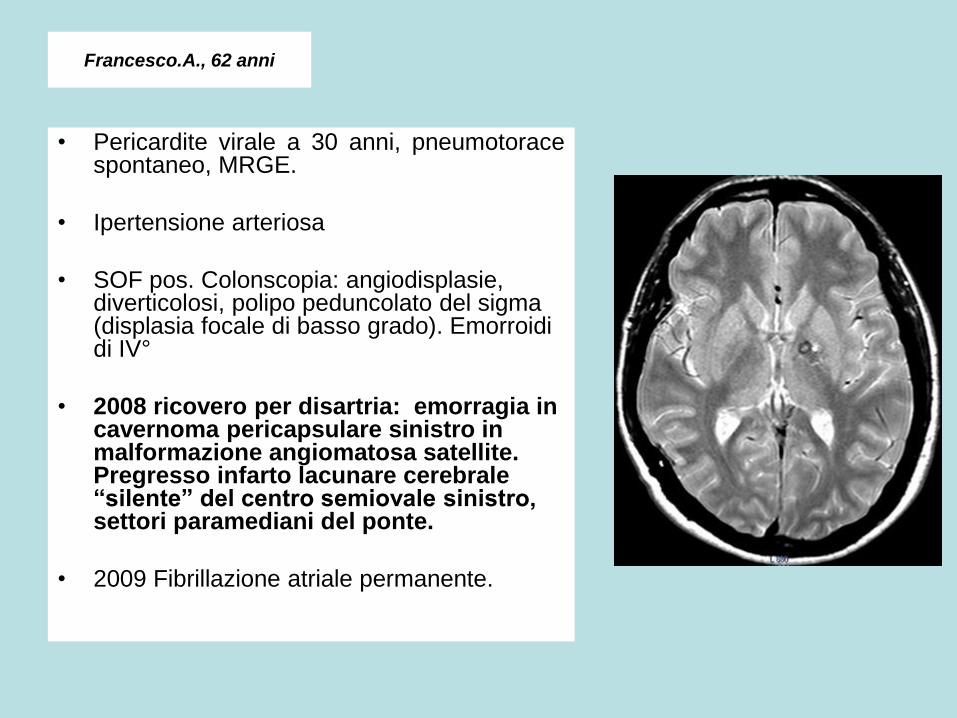
Francesco.A., 62 anni
• Pericardite virale a 30 anni, pneumotoracespontaneo, MRGE.
• Ipertensione arteriosa
• SOF pos. Colonscopia: angiodisplasie, diverticolosi, polipo peduncolato del sigma (displasia focale di basso grado). Emorroidi di IV°
• 2008 ricovero per disartria: emorragia in cavernoma pericapsulare sinistro in malformazione angiomatosa satellite. Pregresso infarto lacunare cerebrale “silente” del centro semiovale sinistro, settori paramediani del ponte.
• 2009 Fibrillazione atriale permanente.
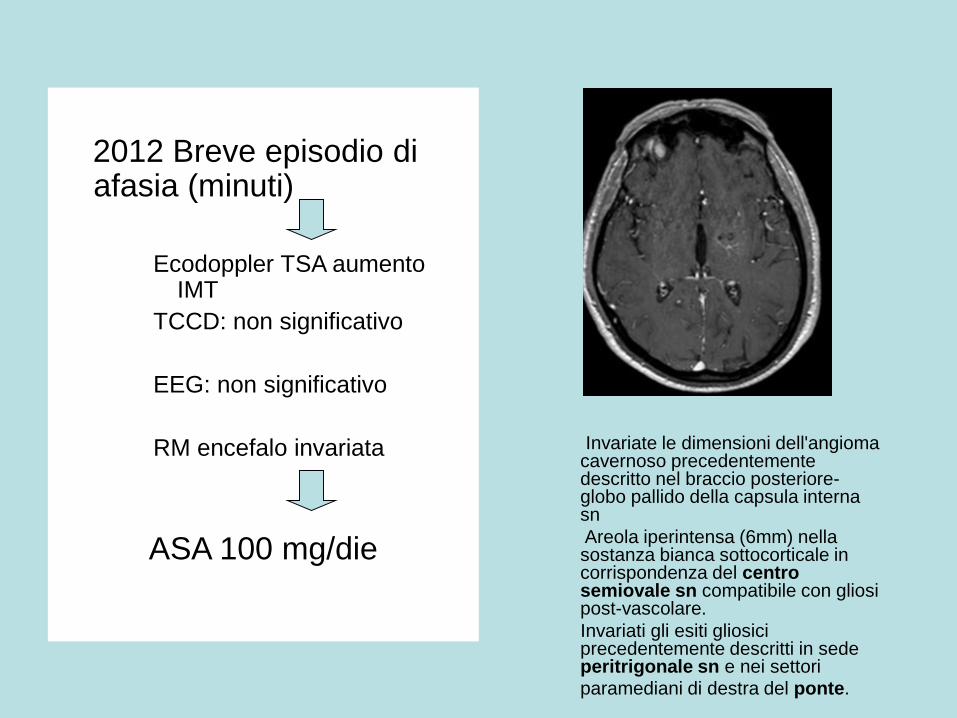
2012 Breve episodio di afasia (minuti)
Ecodoppler TSA aumento IMT
TCCD: non significativo
EEG: non significativo
RM encefalo invariata
ASA 100 mg/die
Invariate le dimensioni dell'angioma cavernoso precedentemente descritto nel braccio posteriore-globo pallido della capsula interna sn
Areola iperintensa (6mm) nella sostanza bianca sottocorticale in corrispondenza del centro semiovale sn compatibile con gliosi post-vascolare.
Invariati gli esiti gliosici precedentemente descritti in sede peritrigonale sn e nei settori paramediani di destra del ponte.
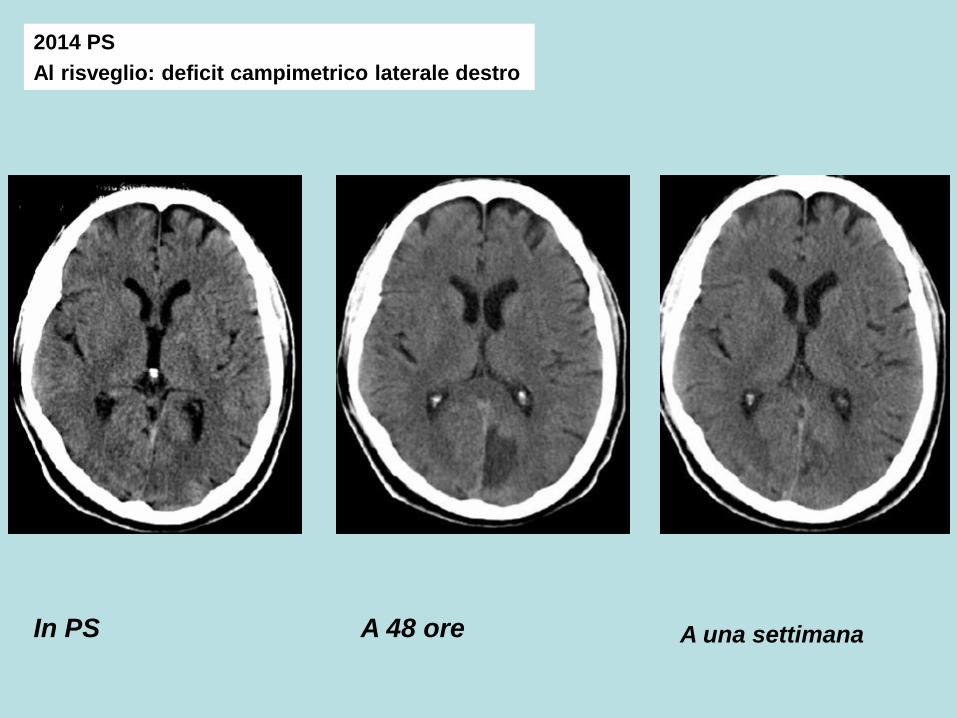
A 48 oreIn PS
2014 PS
Al risveglio: deficit campimetrico laterale destro
A una settimana
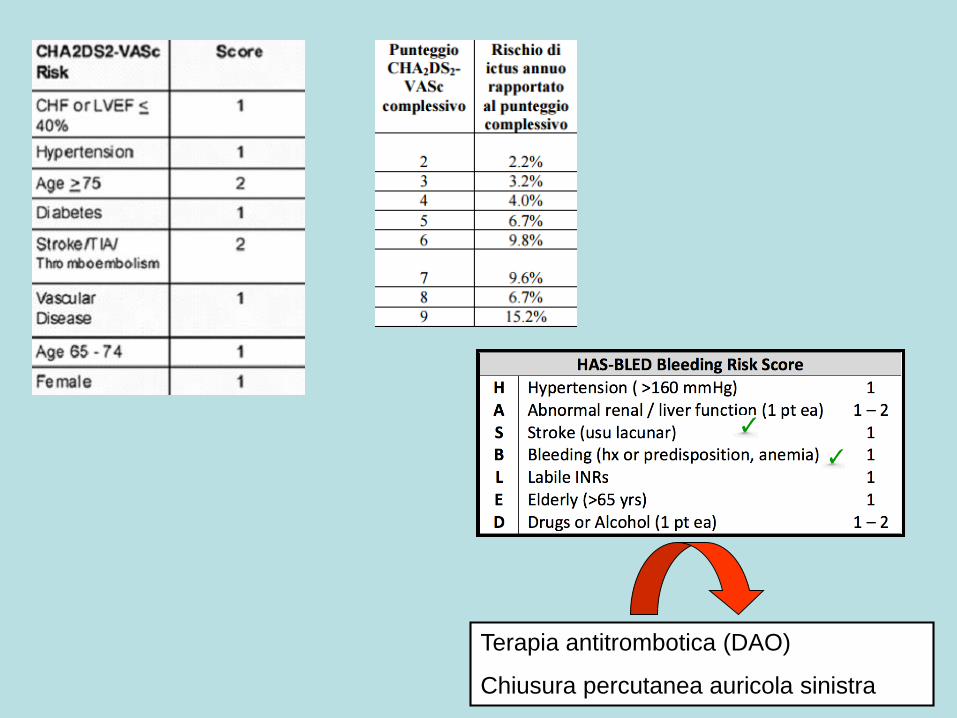
Terapia antitrombotica (DAO)
Chiusura percutanea auricola sinistra
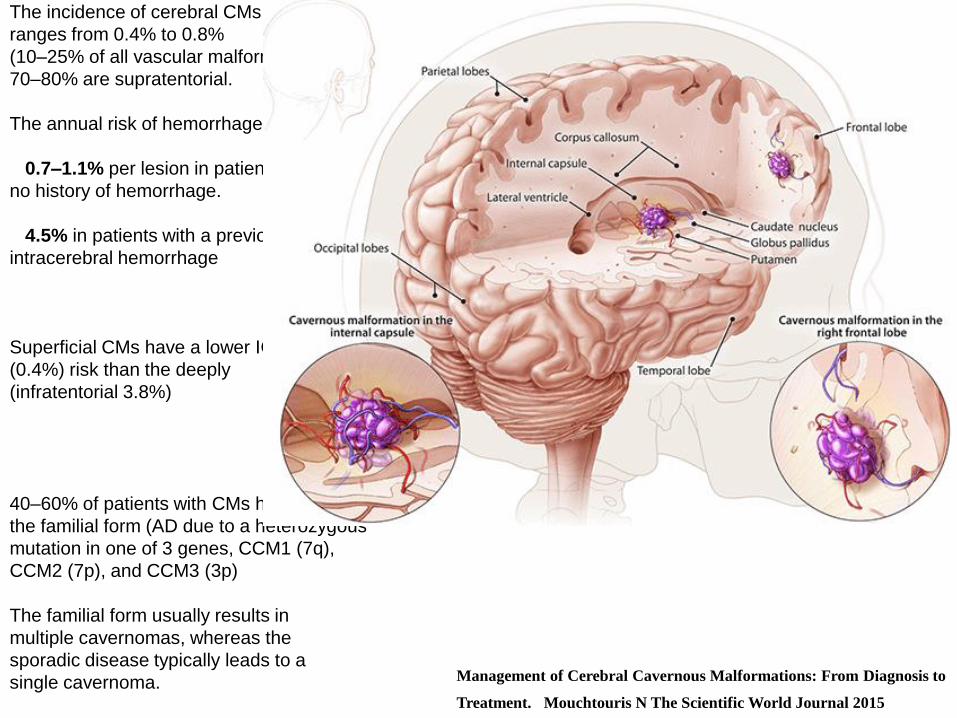
The incidence of cerebral CMs
ranges from 0.4% to 0.8%
(10–25% of all vascular malformations).
70–80% are supratentorial.
The annual risk of hemorrhage is:
0.7–1.1% per lesion in patients with
no history of hemorrhage.
4.5% in patients with a previous
intracerebral hemorrhage
Superficial CMs have a lower ICH
(0.4%) risk than the deeply
(infratentorial 3.8%)
40–60% of patients with CMs have
the familial form (AD due to a heterozygous
mutation in one of 3 genes, CCM1 (7q),
CCM2 (7p), and CCM3 (3p)
The familial form usually results in
multiple cavernomas, whereas the
sporadic disease typically leads to a
single cavernoma. Management of Cerebral Cavernous Malformations: From Diagnosis to
Treatment. Mouchtouris N The Scientific World Journal 2015
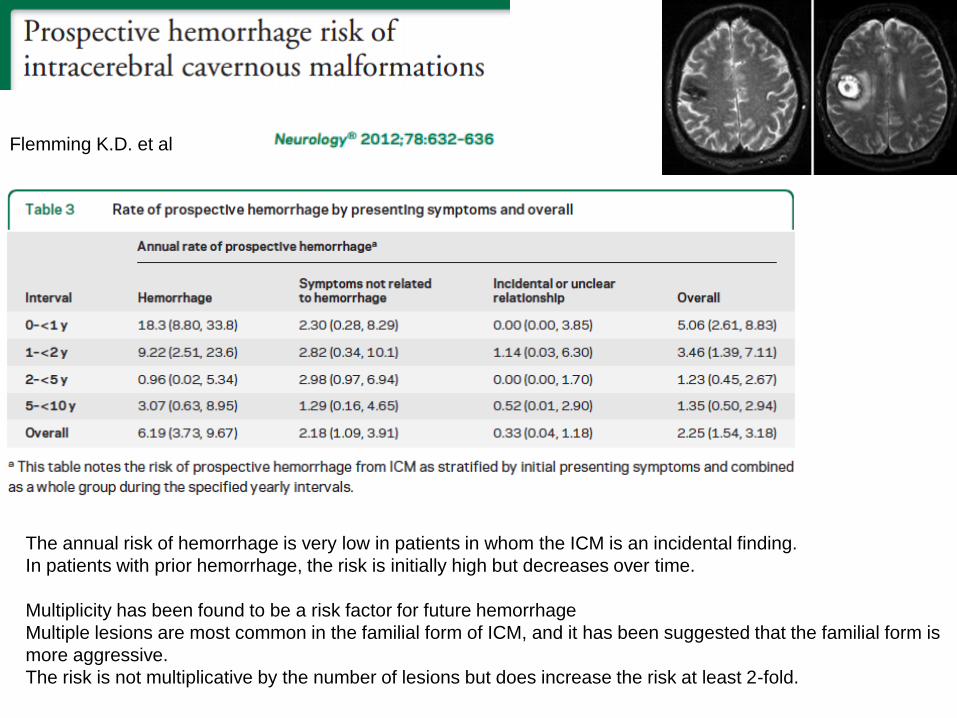
Flemming K.D. et al
The annual risk of hemorrhage is very low in patients in whom the ICM is an incidental finding.
In patients with prior hemorrhage, the risk is initially high but decreases over time.
Multiplicity has been found to be a risk factor for future hemorrhage
Multiple lesions are most common in the familial form of ICM, and it has been suggested that the familial form is
more aggressive.
The risk is not multiplicative by the number of lesions but does increase the risk at least 2-fold.
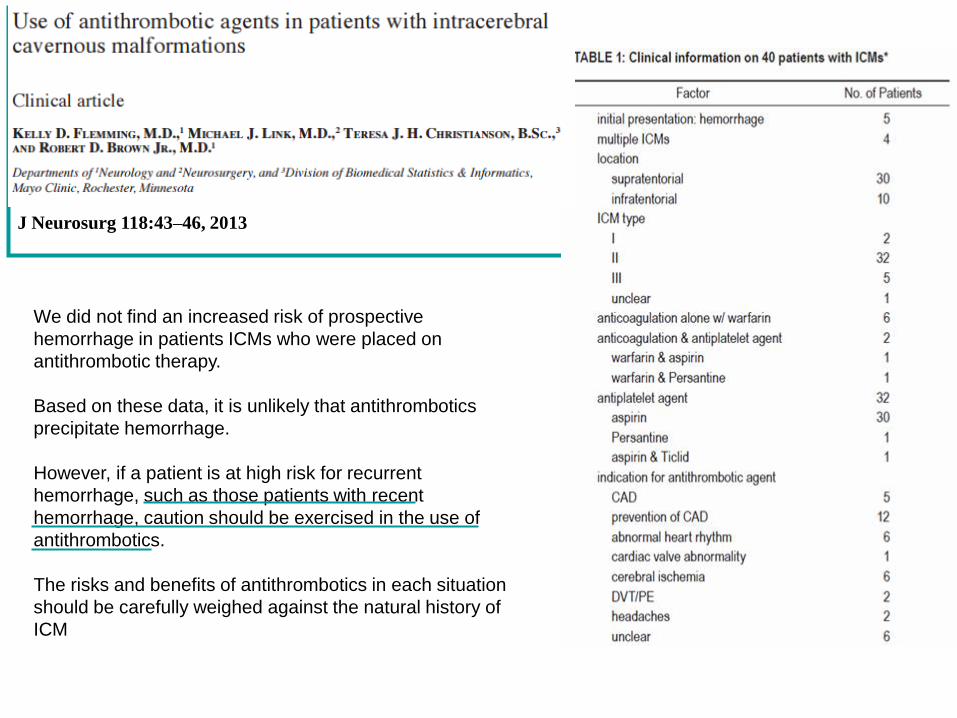
J Neurosurg 118:43–46, 2013
We did not find an increased risk of prospective
hemorrhage in patients ICMs who were placed on
antithrombotic therapy.
Based on these data, it is unlikely that antithrombotics
precipitate hemorrhage.
However, if a patient is at high risk for recurrent
hemorrhage, such as those patients with recent
hemorrhage, caution should be exercised in the use of
antithrombotics.
The risks and benefits of antithrombotics in each situation
should be carefully weighed against the natural history of
ICM
The question of whether and when to prescribe antithrombotic
agents to ICH survivors is one of the major contemporary
dilemmas for stroke physicians.
The increasing proportion of both prior-to-ICH anticoagulant
treatment and AF among ICH survivors further adds to the
importance of this question.
Stroke 2015;46:2094-2099.
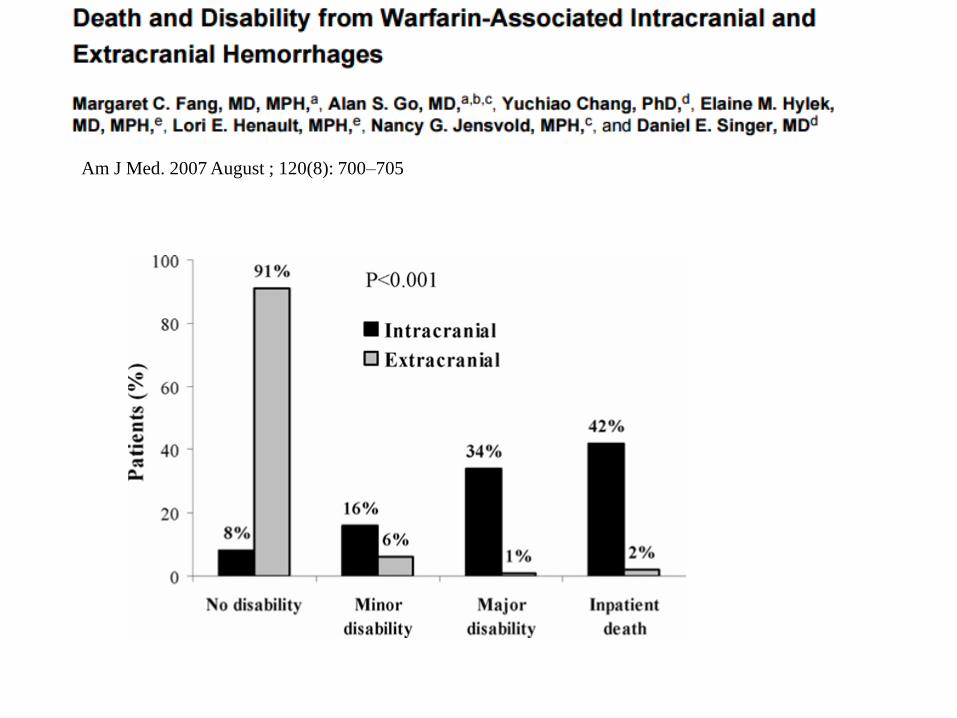
Am J Med. 2007 August ; 120(8): 700–705
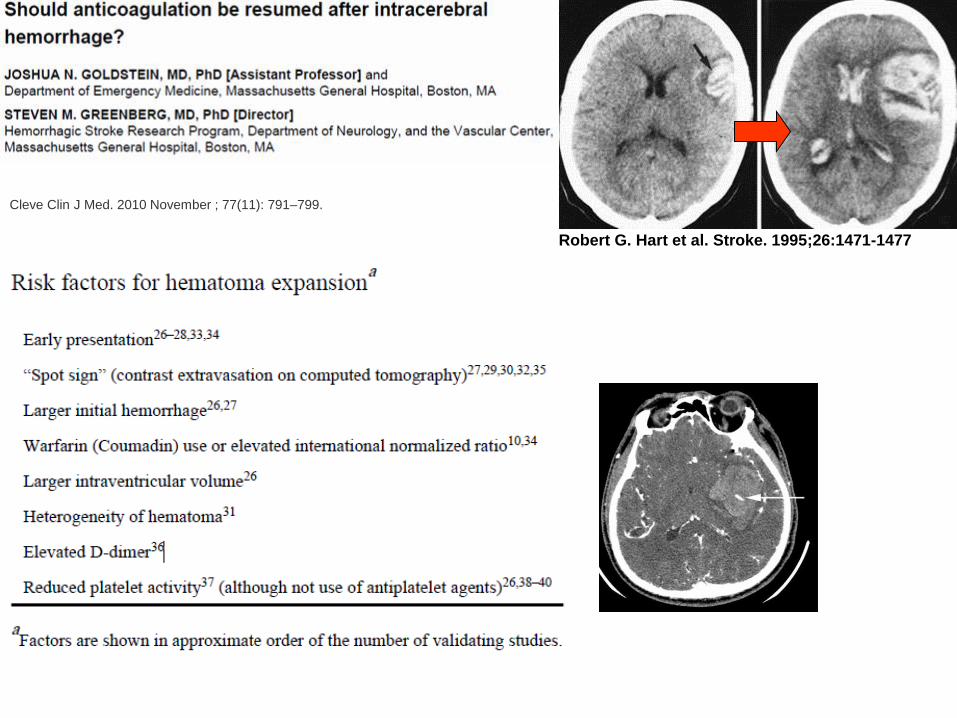
Cleve Clin J Med. 2010 November ; 77(11): 791–799.
Robert G. Hart et al. Stroke. 1995;26:1471-1477
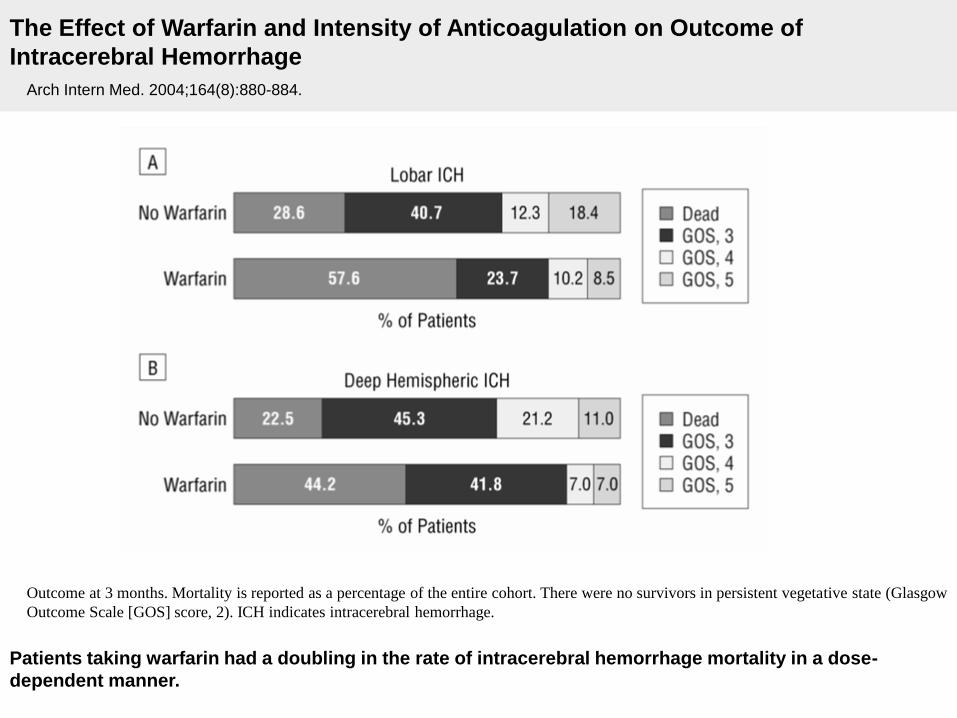
The Effect of Warfarin and Intensity of Anticoagulation on Outcome of
Intracerebral Hemorrhage
Arch Intern Med. 2004;164(8):880-884.
Outcome at 3 months. Mortality is reported as a percentage of the entire cohort. There were no survivors in persistent vegetative state (Glasgow
Outcome Scale [GOS] score, 2). ICH indicates intracerebral hemorrhage.
Patients taking warfarin had a doubling in the rate of intracerebral hemorrhage mortality in a dose-
dependent manner.
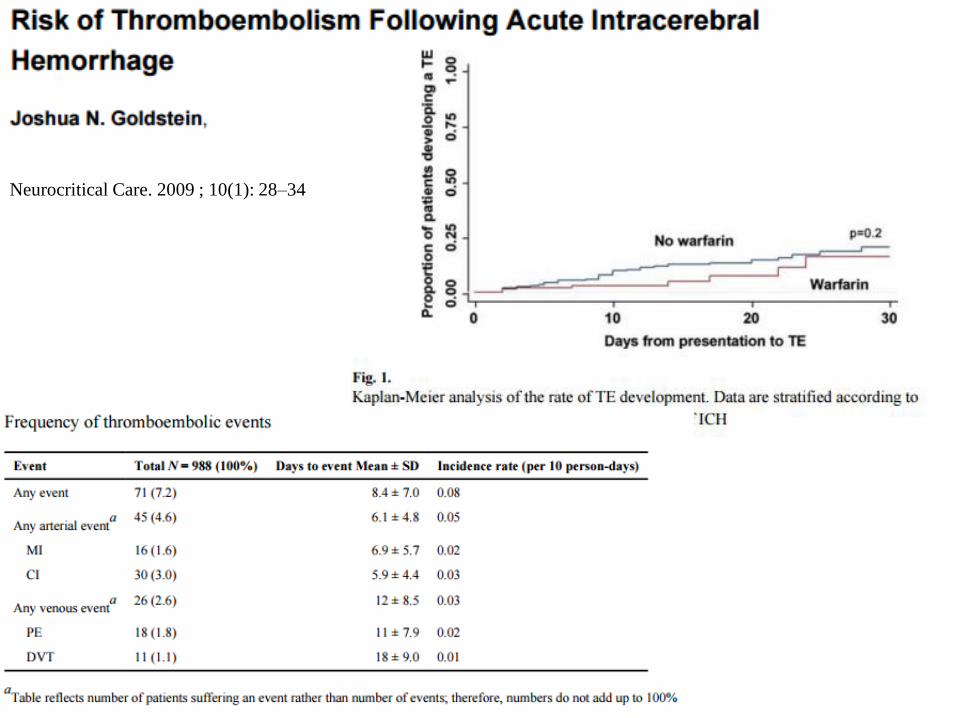
Neurocritical Care. 2009 ; 10(1): 28–34
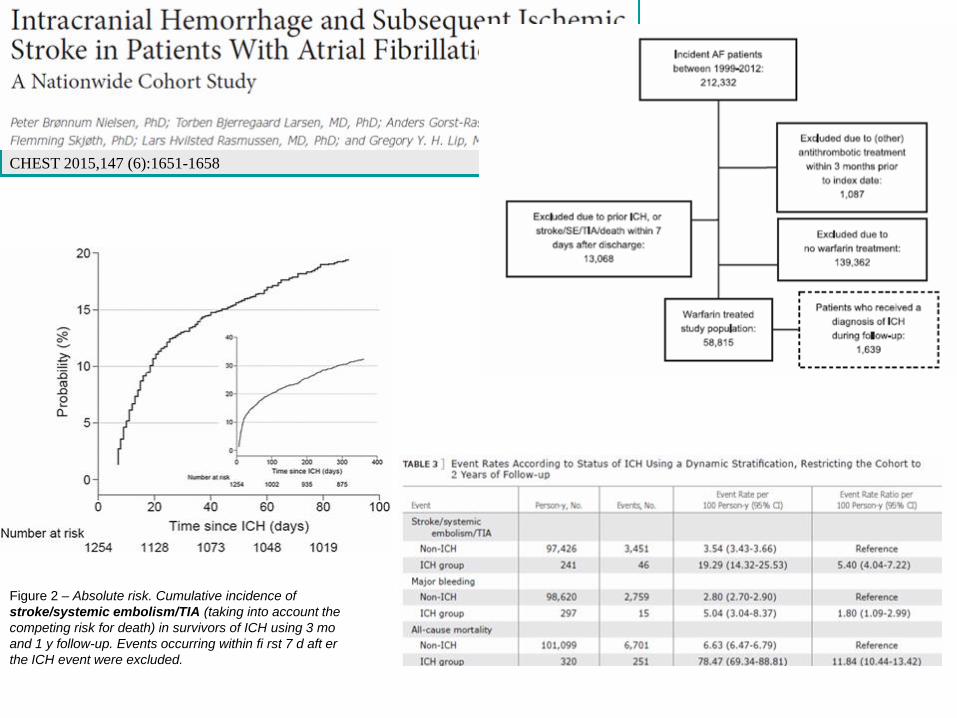
Figure 2 – Absolute risk. Cumulative incidence of
stroke/systemic embolism/TIA (taking into account the
competing risk for death) in survivors of ICH using 3 mo
and 1 y follow-up. Events occurring within fi rst 7 d aft er
the ICH event were excluded.
CHEST 2015,147 (6):1651-1658
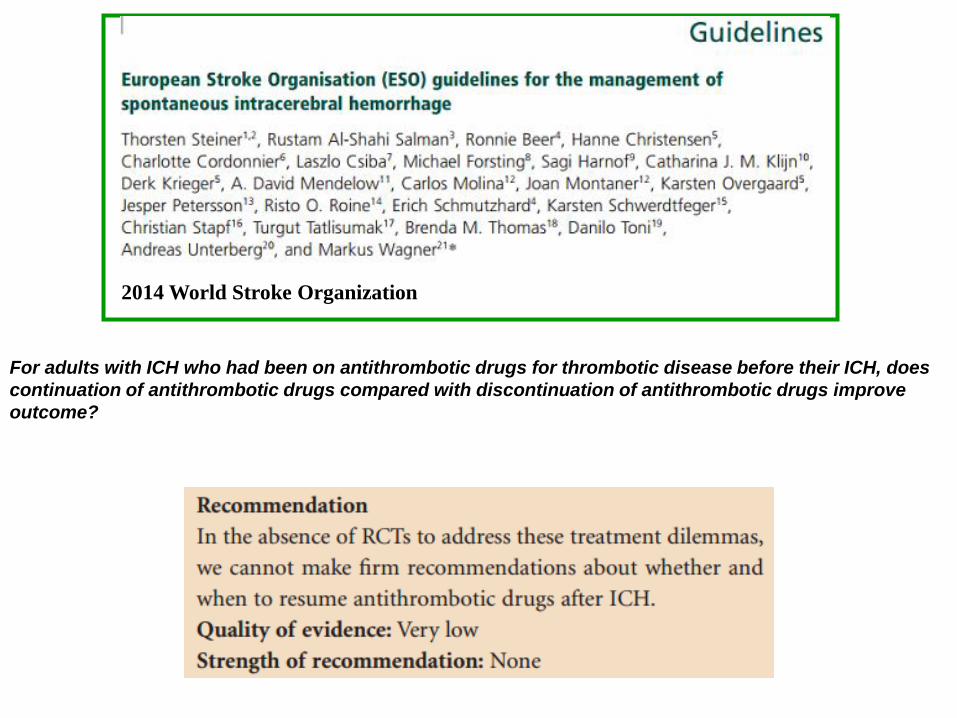
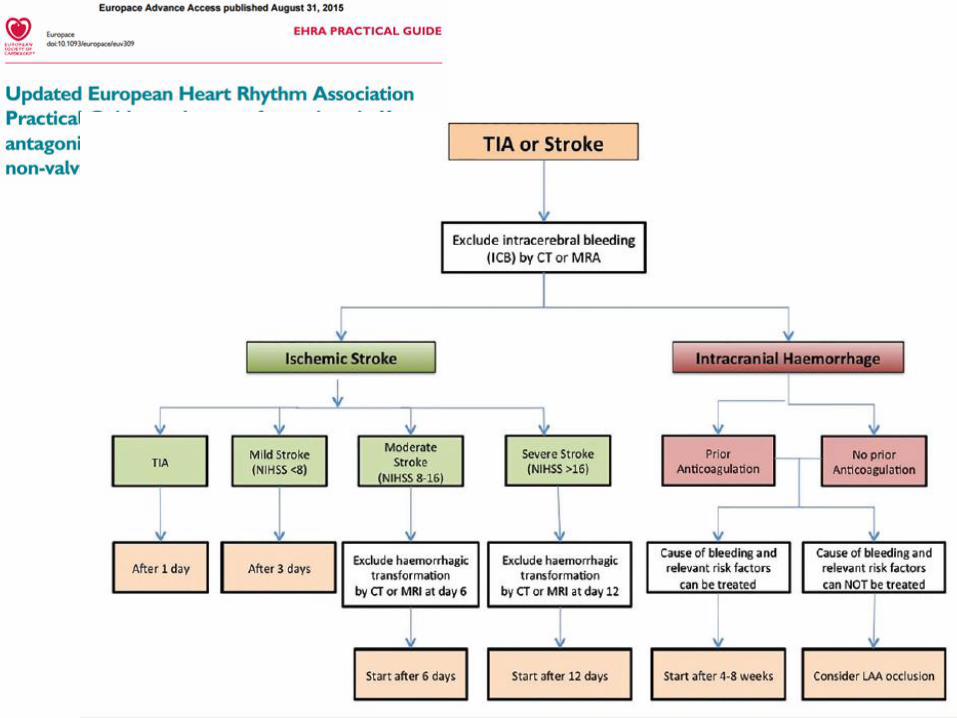
2014 World Stroke Organization
For adults with ICH who had been on antithrombotic drugs for thrombotic disease before their ICH, does
continuation of antithrombotic drugs compared with discontinuation of antithrombotic drugs improve
outcome?
Additional information:
• Small observational case series and literature reviews have not found a relevant effect on the risk of recurrent ICH from restarting antiplatelet drugs in survivors of ICH.
• Similarly, only observational studies address whether, when, and in whom to restart oral anticoagulation after ICH.
• Suggested timings for restarting these drugs range from not earlier than 14 days up to 10 to 30 weeks.
• A RCT to address the dilemma about whether to restart
or stop antiplatelet drugs after ICH is underway
(www.RESTARTtrial.org).
• Alternatives to restarting antithrombotic drugs, such as left atrial appendage occlusion, could be an alternative for managing patients in atrial fibrillation with a
high risk of cardioembolic stroke after acute ICH.
2014 World Stroke Organization
When stratifying a patient’s risk for recurrent ICH may affect management decisions, it
is reasonable to consider the following risk factors for ICH recurrence:
• Lobar location of the initial ICH;
• Older age
• Presence and number of microbleeds on gradient echo MRI
• Ongoing anticoagulation
• Presence of apolipoprotein E ε2 or ε4 alleles (ClassIIa; Level of Evidence B).
BP should be controlled in all ICH patients (ClassI; Level of Evidence A). Measures to
control BP should begin immediately after ICH onset (Class I; Level of Evidence A). A
long-term goal of BP <130 mm Hg systolic and 80 mm Hg diastolic is reasonable
(Class IIa; Level of Evidence B).
Stroke. 2015; 46:2032-2060
• Lifestyle modifications, including avoidance of alcohol use greater than 2 drinks per
day, tobacco use, and illicit drug use, as well as treatment of obstructive sleep apnea,
are probably beneficial (Class IIa;Level of Evidence B).
• Avoidance of long-term anticoagulation with warfarin as a treatment for nonvalvular
atrial fibrillation is probably recommended after warfarin-associated spontaneous
lobar ICH because of the relatively high risk of recurrence (Class IIa; Level of
Evidence B).
• Anticoagulation after non lobar ICH and antiplatelet monotherapy after any ICH
might be considered, particularly when there are strong indications for these agents
(Class IIb; Level of Evidence B).
Stroke. 2015;46:2032-2060
Stroke. 2015; 46: 2032-2060
•The optimal timing to resume oral anticoagulationafter anticoagulant-related ICH is uncertain.
Avoidance of oral anticoagulation for at least 4 weeks, in patients without mechanical heart
valves, might decrease the risk of ICH recurrence (ClassIIb; Level of Evidence B). If indicated,
aspirin monotherapy can probably be restarted in the days after ICH, although the optimal timing
is uncertain (Class IIa; Level of Evidence B).
•The usefulness of dabigatran, rivaroxaban, or apixaban in patients with atrial fibrillation
and past ICH to decrease the risk of recurrence is uncertain (ClassIIb; Level of Evidence C).
(New recommendation)
•There are insufficient data to recommend restrictions on the use of statins in ICH patients (Class
IIb;Level of Evidence C).
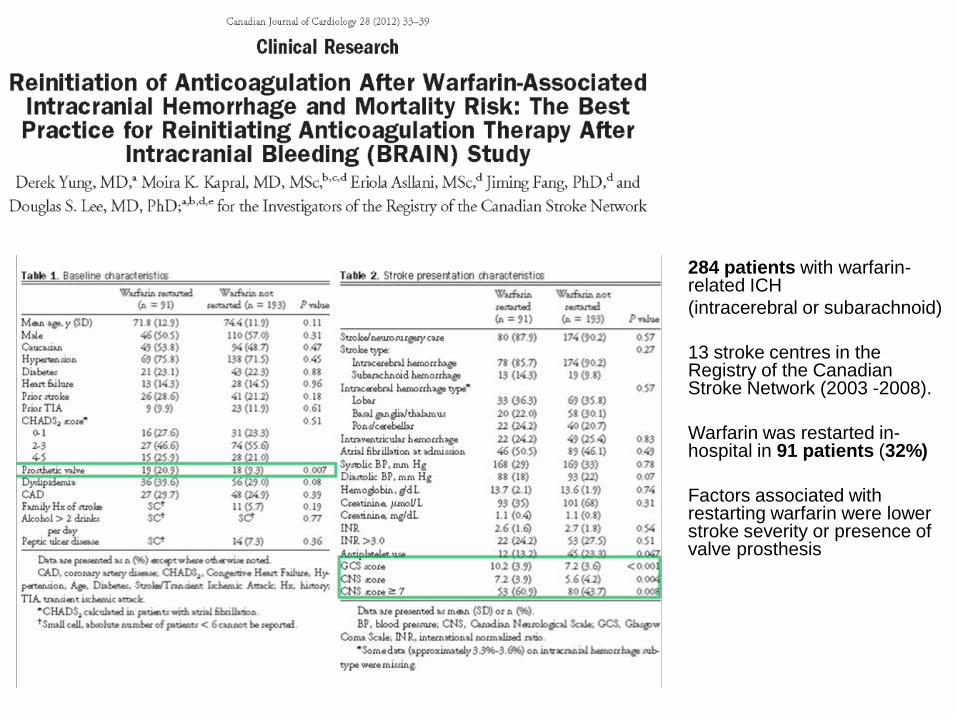
284 patients with warfarin-related ICH
(intracerebral or subarachnoid)
13 stroke centres in the Registry of the Canadian Stroke Network (2003 -2008).
Warfarin was restarted in-hospital in 91 patients (32%)
Factors associated with restarting warfarin were lower stroke severity or presence of valve prosthesis
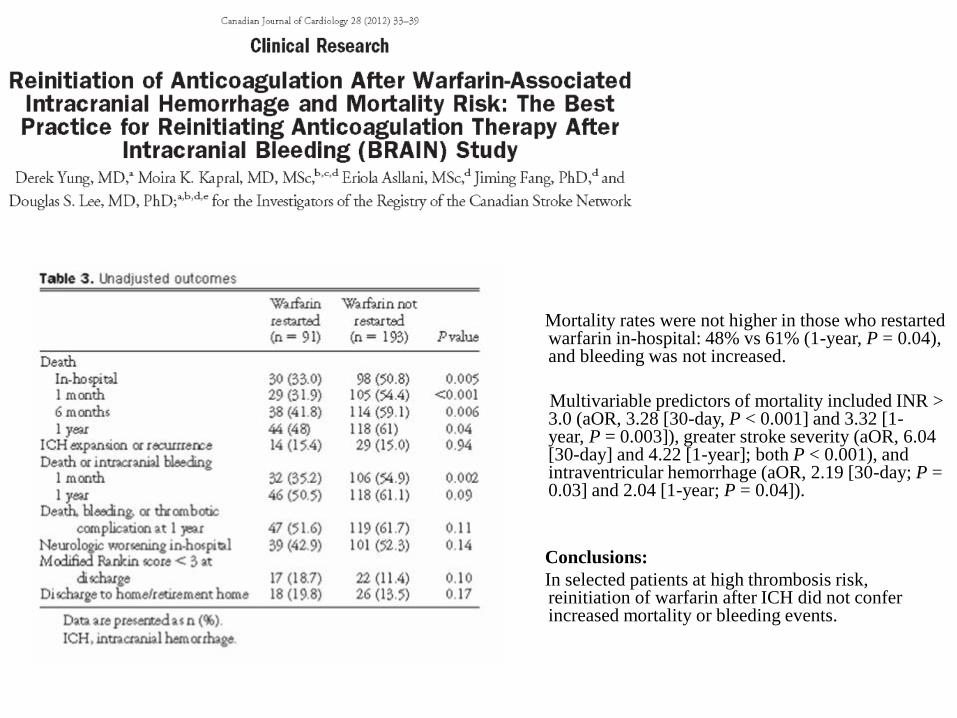
Mortality rates were not higher in those who restarted warfarin in-hospital: 48% vs 61% (1-year, P = 0.04), and bleeding was not increased.
Multivariable predictors of mortality included INR > 3.0 (aOR, 3.28 [30-day, P < 0.001] and 3.32 [1-year, P = 0.003]), greater stroke severity (aOR, 6.04 [30-day] and 4.22 [1-year]; both P < 0.001), and intraventricular hemorrhage (aOR, 2.19 [30-day; P = 0.03] and 2.04 [1-year; P = 0.04]).
Conclusions:
In selected patients at high thrombosis risk, reinitiation of warfarin after ICH did not confer increased mortality or bleeding events.
Arch Neurol. 2008;65(10):1313-1318
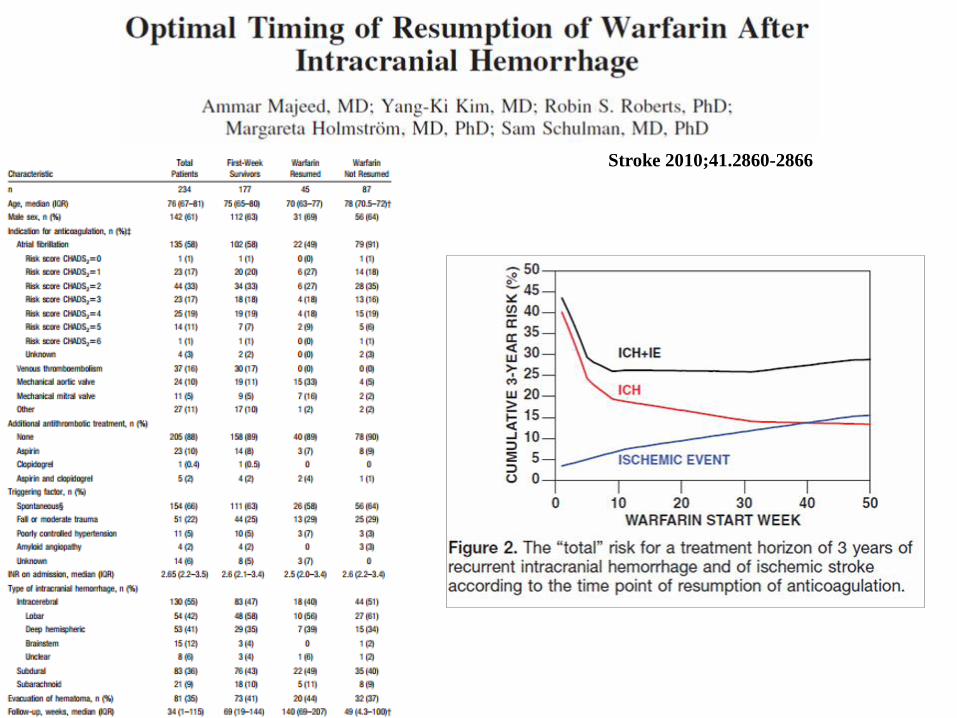
Stroke 2010;41.2860-2866
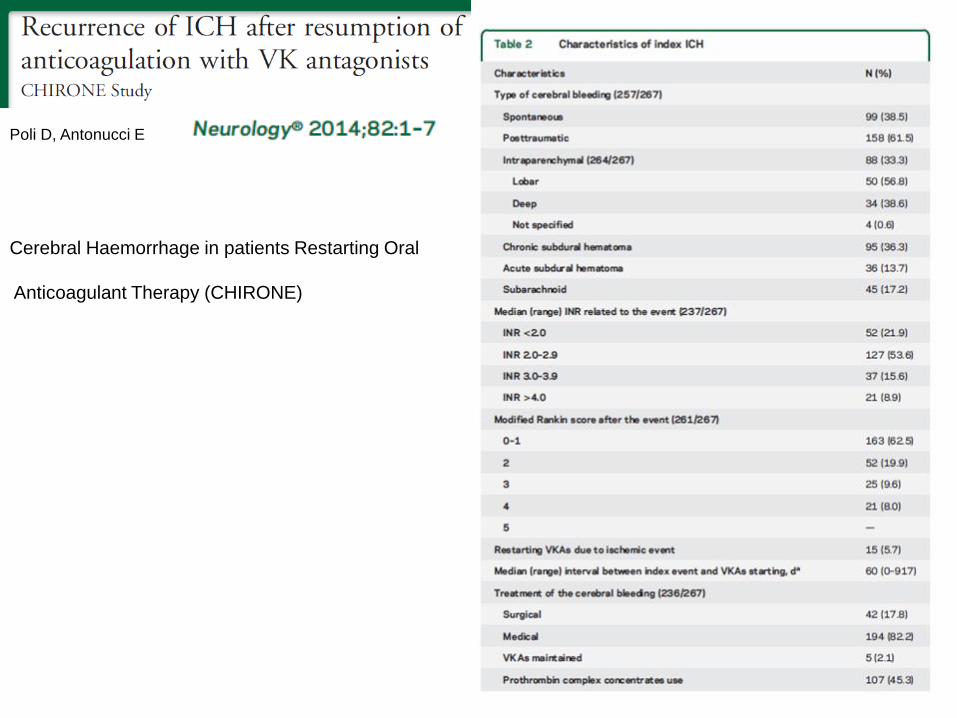
Poli D, Antonucci E
Cerebral Haemorrhage in patients Restarting Oral
Anticoagulant Therapy (CHIRONE)
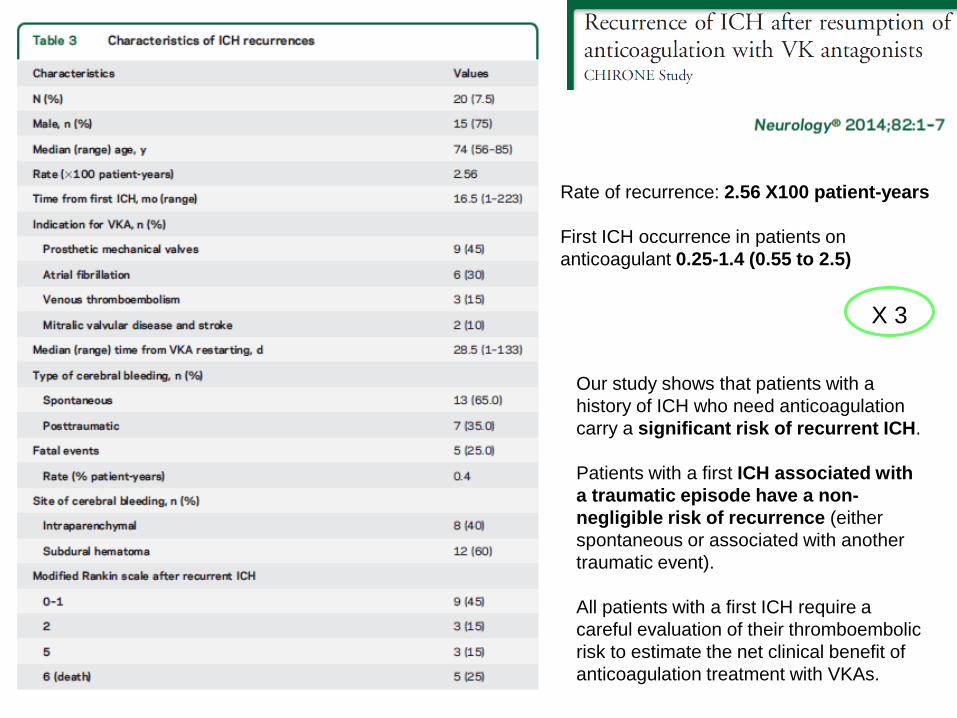
Our study shows that patients with a
history of ICH who need anticoagulation
carry a significant risk of recurrent ICH.
Patients with a first ICH associated with
a traumatic episode have a non-
negligible risk of recurrence (either
spontaneous or associated with another
traumatic event).
All patients with a first ICH require a
careful evaluation of their thromboembolic
risk to estimate the net clinical benefit of
anticoagulation treatment with VKAs.
Rate of recurrence: 2.56 X100 patient-years
First ICH occurrence in patients on
anticoagulant 0.25-1.4 (0.55 to 2.5)
X 3
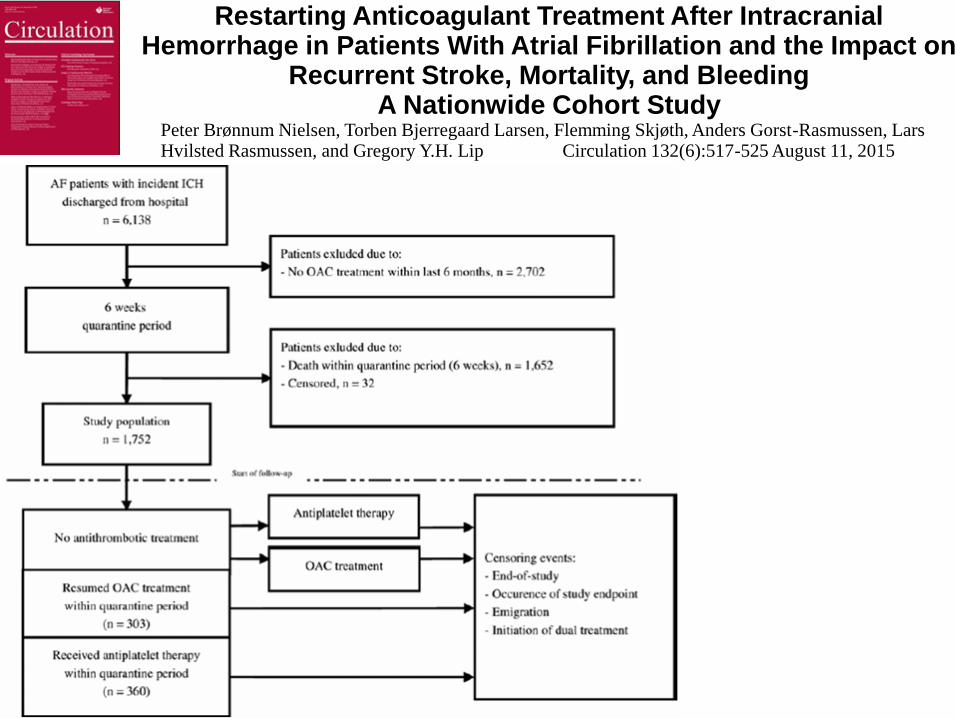
Restarting Anticoagulant Treatment After Intracranial Hemorrhage in Patients With Atrial Fibrillation and the Impact on
Recurrent Stroke, Mortality, and BleedingA Nationwide Cohort Study
Peter Brønnum Nielsen, Torben Bjerregaard Larsen, Flemming Skjøth, Anders Gorst-Rasmussen, Lars Hvilsted Rasmussen, and Gregory Y.H. Lip Circulation 132(6):517-525 August 11, 2015
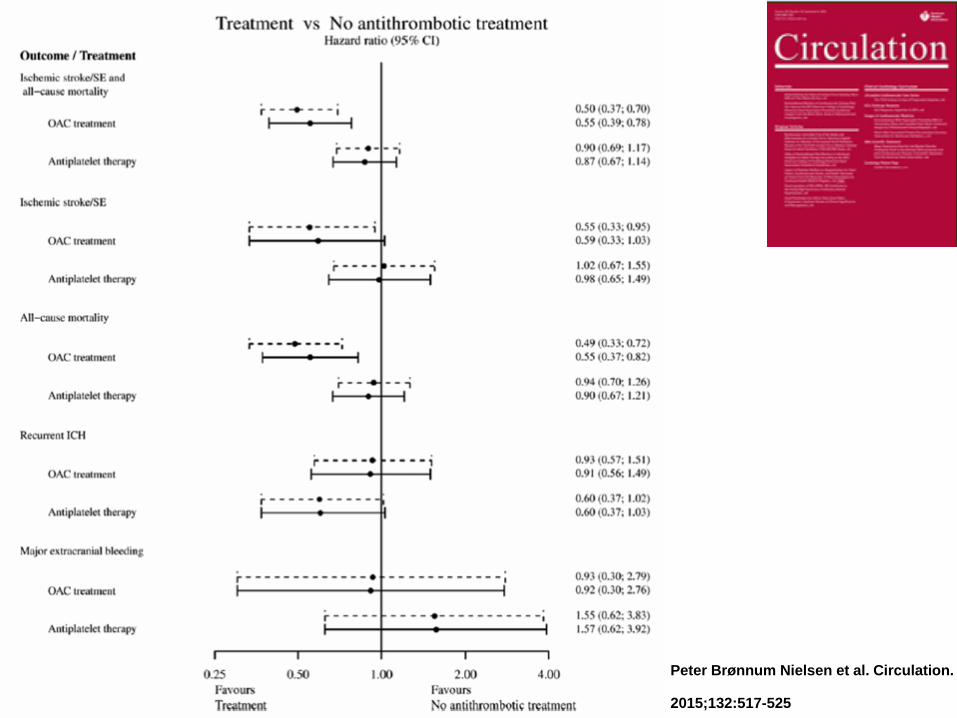
Peter Brønnum Nielsen et al. Circulation.
2015;132:517-525
Thromb Haemost 2014; 111: 14–18
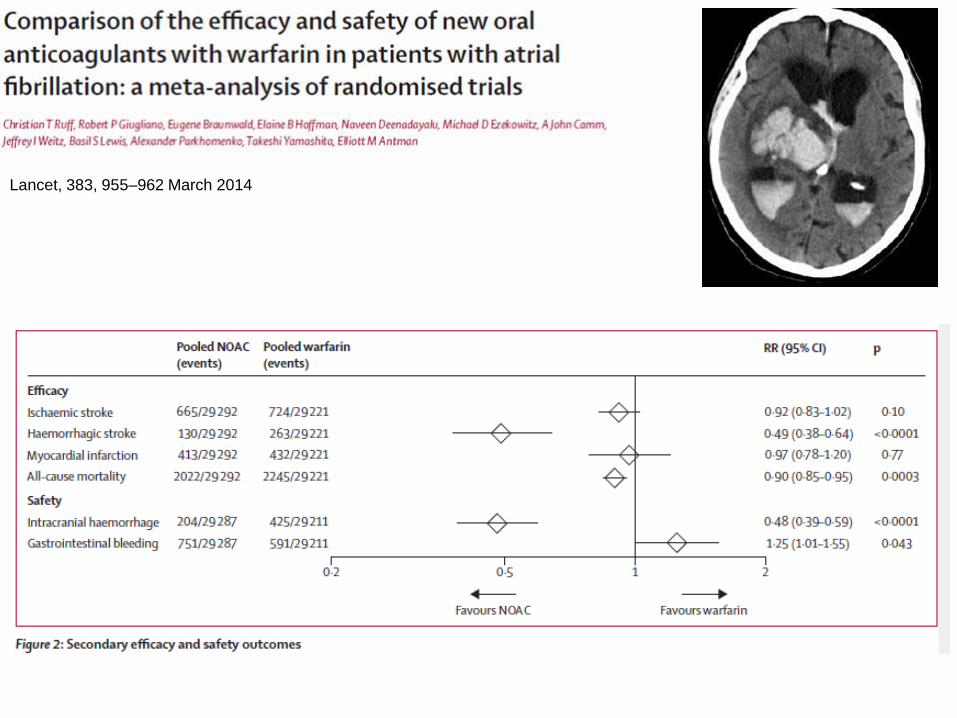
Lancet, 383, 955–962 March 2014
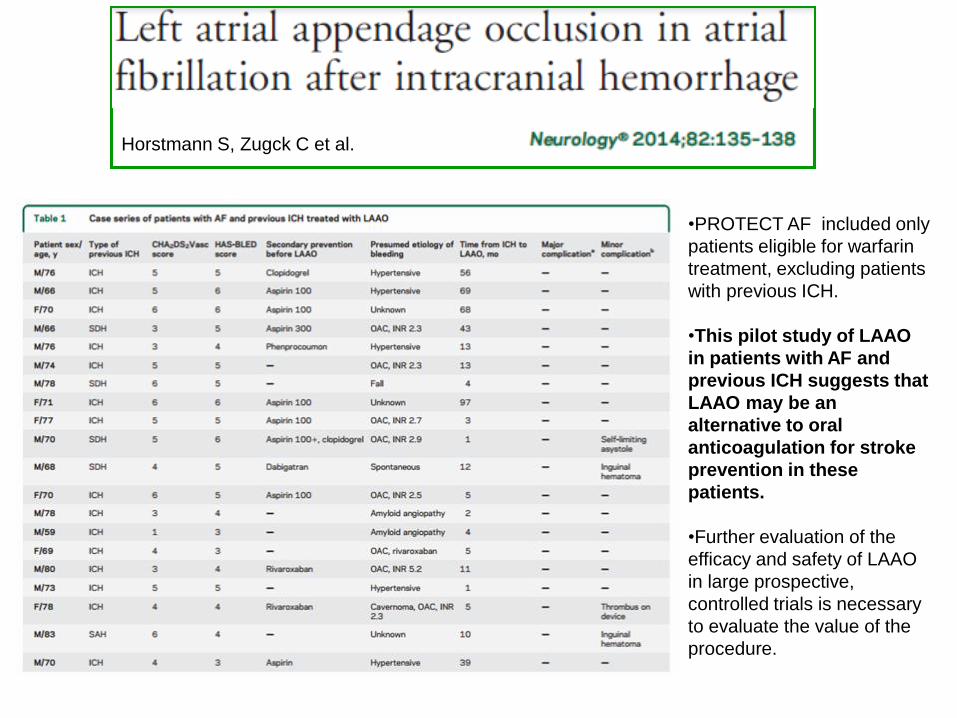
Horstmann S, Zugck C et al.
•PROTECT AF included only
patients eligible for warfarin
treatment, excluding patients
with previous ICH.
•This pilot study of LAAO
in patients with AF and
previous ICH suggests that
LAAO may be an
alternative to oral
anticoagulation for stroke
prevention in these
patients.
•Further evaluation of the
efficacy and safety of LAAO
in large prospective,
controlled trials is necessary
to evaluate the value of the
procedure.

















