41
Anticoagulants Reducing the risk Sue Wooller & Amanda Powell May 2013
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | harold-ellis |
| View: | 218 times |
| Download: | 5 times |

AnticoagulantsReducing the risk
Sue Wooller & Amanda PowellMay 2013

Coroner highlights prescribing error after patient dies from warfarin overdose
BMJ 2002;325:922
Failure to prescribe appropriate prophylaxis against PUD contributes to the death of a patient from a GI bleed whilst anticoagulated
MPS - UK Casebook 2005
Fatal outcome of Azapropazone/Warfarin interaction - INR not checked despite early signs of bleeding.
Improving Medication Safety - DoH 2004

Delay in follow up after 20% increase in Warfarin dosage leads to fatal haemorrhage
Improving Medication Safety - DoH 2004
Suprachoroidal haemorrhage after Clarithromycin co-prescribed with Warfarin leaves patient with permanent visual damage
Journal of Royal Society of Medicine 2001
Patient dies of a subdural haematoma secondary to a grossly elevated INR having been recently discharged from hospital
MPS website
Patient, post DVT, had a constantly low INR due to mistaking 0.5mg for 5mg tablets
Local incident 2010
Patient, post DVT, given warfarin on only Saturdays and Sundays due to poor discharge communication
Local incident 2010
Patient admitted to ITU with life threatening haematoma after continuing on loading dose of warfarin post discharge
Local incident 2011

AnticoagulantsReducing the risk
Sue Wooller & Amanda PowellMay 2012

THE BLOODCLOTS……….NEVERMIND

The therapeutic "window" Hylek EM, et al. New Engl J Med 1993;120:897-902

Observational study of 18 820 patients aged > 16 years admitted over six months and assessed for cause of admission.
There were 1225 admissions related to an ADR, giving a prevalence of 6.5%, with the ADR directly leading to the admission in 80% of cases.
The median bed stay was eight days, accounting for 4% of the hospital bed capacity.
The projected annual cost of such admissions to the NHS is £466m The overall fatality was 0.15%. Most reactions were either definitely or possibly avoidable. Drugs most commonly implicated in causing these admissions
included low dose aspirin, diuretics, warfarin, and NSAIDs other than aspirin, the most common reaction being gastrointestinal bleeding.
Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients
BMJ 2004;329:15-19

National Patient Safety Agency

88

Coroner highlights prescribing error after patient dies from warfarin overdose
BMJ 2002;325:922
The coroner returned a verdict of accidental death on a 79 year old patient.
The man died of gastrointestinal haemorrhage three weeks after being told to take the wrong dose.
Doctors at the surgery in south east Sheffield used to write repeat prescriptions for the drug by hand, on the basis of the patient’s latest blood test results.
The card would then be handed to the receptionist, who would inform the patient of any required change in dose.
The patient in question was taking doses of 2 mg or 3 mg on alternate days. His doctor wrote the word "Same" on the patient’s card and passed it to the receptionist, who read his writing as "5mg."

Describing the incident as a "disastrous error," the doctor concerned said the surgery has since changed its protocol for repeat prescriptions of the drug.
Blood test results and recommended doses of warfarin are now entered into the computer system by the doctor, the doctor informs the patient by phone the same evening of the result, and confirmation of the dosage is sent in writing to the patient a few days later.
But he added that he had said in the court hearing that his own handwriting was often difficult to read. "I accept entirely in my own handwriting my ‘S’ and my ‘5’ are very similar and my ‘S’ can easily be mistaken for a ‘5’”
Coroner highlights prescribing error after patient dies from warfarin overdose
BMJ 2002;325:922

Reducing the risks: Oral anticoagulants Improving Medication Safety 2004, DoH
Staff at Basildon Hospital have developed an automatic voicemail system which calls patients at home with their INR result, dose and clinic appointment time.
The system has been in operation for more than 2 years, transmitting over 60,000 reports by telephone. There were no clinical incidents.

Nursing home administered 1mg tablets instead of 3mg tablets to a patient resulting in an INR of 1.4
Nursing home administered 2.5mg Warfarin daily instead of 21/2 tablets of 3mg (7.5mg) daily
Patient discharged from CCU with Warfarin dose written in a booklet about medicines for the heart. Took 3 x 5mg daily instead of 3.5mg daily
National Patient Safety Agency

From the MPS website
Dr L, a GP, had received notice of her requested attendance at a coroner’s inquest into the death of one of her patients.
Mr G had been an inpatient at the local hospital, where he had been anticoagulated with warfarin. After discharge, he had become unwell and been re-admitted to the hospital. Unfortunately, he had died from a subdural haematoma, secondary to a grossly elevated INR.
There had been no opportunity to check his INR during the short period in which he had been out of hospital…

Local examplesResidential home called for advice:
Patient had been discharged home from hospital a month previously, had a DVT during admission and had been started on warfarin.
Patient had been discharged home on a Saturday and the discharging team advised for the patient to have 3mg of warfarin on the Saturday and Sunday.
For the month since being discharged from hospital the nursing home had been giving the patient 3mg of warfarin every Saturday and Sunday, no warfarin during the week and no INR monitoring.

Local examples
There was a patient taking 0.5mg instead of 5mg as the GP had issued 0.5mg and we didn't know he had them - we kept increasing his dose and nothing was happening.
Many patients still fail to let us know when they are given new meds/antibiotic courses.
Anticoagulant Clinic Pharmacist, UHW

Local examples Patient was slow loaded for AF on 3mg daily for 7
days then re-check INR. Given 3mg & 1mg tablets. Took both despite yellow book clearly stating
3mg (1 blue tablet) daily. INR on Day 8 >15
Patient given 5mg tablets instead of his usual 3mg. Just thought the colour had changed despite
being on warfarin for several years. INR >8.0 after 1 week.
Cwm Taf Anticoagulation Service

Local examples
Patient given 2 x 10mg loading doses on the ward Discharged at a weekend with 1mg, 3mg &
5mg tablets Continued with 10mg daily until next INR check
as thought this was correct Admitted to ITU with life threatening
haematoma after 5 days
Cwm Taf Anticoagulation Service
Use of 0.5mg Warfarin tablets is not widespread yet many patient and carers need to break 1mg tablets to produce correct dose
Local policy of only using 3mg tablets and then prescribing 2mg daily dose causes very real problems for patients
Alternate day dosing regimes are difficult especially for those with poor memories
National Patient Safety AgencyPatient workshop

Problems with information not communicated to GPs
Poor communication with carers No planning for coping during first 4 weeks post-
discharge Lack of information about effect of foods and
alcohol on anticoagulant control Overall, discharge is the weakest yet critical
stage
National Patient Safety AgencyPatient workshop

National Patient Safety AgencySafer Use of Anticoagulants, 2006Patient workshop
“They’re given a bag of tablets and a letter to take to their GP and that’s where it stops”
“People who are discharged from hospital are given so much information in such a short time that half of it goes over their head. They’re not worried about what pill they’re going to take - they’re worried about how they’re going to manage at all”

A 66-year-old man with ischaemic heart disease was treated with warfarin for AF.
He developed acute arthritis, diagnosed as gout by his general practitioner, and was prescribed the anti-inflammatory drug azapropazone.
The dose was subsequently increased in response to an exacerbation of his arthritis.
The patient then developed signs of bleeding. The general practitioner arranged for a full blood count, but did not
check the INR. Before the results were available, the patient suffered a massive
intracranial haemorrhage, was admitted to hospital, and died. On admission his INR was greater than 10.
Reducing the risks: Oral anticoagulantsImproving Medication Safety 2004, DoH

Suprachoroidal haemorrhage after addition of ClarithromycinJournal of the Royal Society of Medicine 2001; 94: 583-584
62 year old lady with AVR/MVR anticoagulated with Warfarin target INR 3.0
Attended casualty with sudden deterioration of vision after coughing
A week before presentation she had begun a course of Clarithromycin for a chest infection
INR 3 days before start of course: 2.3 INR 3 days into the course: 2.9 INR on presentation: 8.2

Co-ingestion of herbal medicines and warfarinBJGP 2004; 54 : 439-441 Postal questionnaire Thirty-five general practices in Devon and Somerset identified
2600 patients taking warfarin and sent postal questionnaires to them.
Response rate = 54.2% One or more of the specified herbal remedies thought to interact
with warfarin were taken by 8.8% of all patients. Complementary or homeopathic treatments not specified in the
survey questionnaire were taken by 14.3% of responders. Overall, 19.2% of responders were taking one or more such
medicines. The use of herbal medicines had not been discussed with a
conventional healthcare professional by 92.2% of patients.

Reducing the risks: Oral anticoagulants Improving Medication Safety 2004, DoH
All patients taking anticoagulants should be monitored carefully
Responsibilities of health care team should be clearly defined There should be regular service audits Report stresses the critical importance of effective
communications when patients move from one care setting to another
On discharge, drug regimen /treatment plan need to be communicated in a timely and reliable way to ensure safe and seamless transfer
Staff should ensure that patients understand their discharge medicines

National Patient Safety AgencyPatient Safety Alert 18 (March 2007)
Ensure all staff caring for patients anticoagulant therapy have the necessary work competences
Review and update procedures and clinical protocols for anticoagulant services to ensure they reflect safe practices
Audit anticoagulant services using BSH/NPSA safety indicators as part of the annual medicines management audit programme
Ensure that patients prescribed anticoagulants receive appropriate verbal and written information
Promote safe practice with prescribers and pharmacists to check that patients’ INR is being monitored regularly and that the INR level is safe before issuing or dispensing repeat prescriptions for oral anticoagulants
Promote safe practice for prescribers co-prescribing one or more clinically significant interacting medicines for patients already on oral anticoagulants - make arrangements for INR tests and inform monitoring clinic. Pharmacists to ensure precautions have been taken.
Ensure that dental practitioners manage patients on anticoagulants according to evidence based therapeutic guidelines.
Amend local policies to standardise the range of anticoagulant products used incorporating characteristics identified by patients as promoting safer use.
Promote the use of written safe practice procedures for the administration of anticoagulants in social care settings. Minimise and risk assess the use of MDS.
National Patient Safety AgencyPatient Safety Alert 18 (March 2007)

Safety Indicators NPSA/BCSHBritish Journal of Haematology (2007)
136 (1); 26-29
Proportion of patient-time in range
Percentage of INRs > 5·0
Percentage of INRs > 8·0
Percentage of INRs > 1·0 INR unit below target (e.g. percentage of INRs < 1·5 for patients with target INR of 2·5)
Percentage of patients suffering adverse outcomes, categorised by type, e.g. major bleed
Percentage of patients lost to follow up (and risk assessment of process for identifying patients lost to follow up).

Safety Indicators NPSA/BCSHBritish Journal of Haematology (2007)
136 (1); 26-29
Percentage of patients with unknown diagnosis, target INR or stop date
Percentage of patients with inappropriate target INR for diagnosis, high and low
Percentage of patients without written patient educational information.
Percentage of patients without appropriate written clinical information, e.g. diagnosis, target INR, last dosing record.
Who is at risk?BMJ 2002; 325: 828-831Questions to ask when considering oral anticoagulation
Is there a definite indication? Is there a high risk of bleeding? Will current medication/disease interfere
with control? Is compliance/attendance at clinic a
problem? Will there be regular review of
risks/benefits of anticoagulation?

Who is at risk?BMJ 2002; 325: 828-831NICE CG36Patients at high risk of bleeding with Warfarin Age >75 years Uncontrolled hypertension Alcohol excess Poor compliance/clinic attendance Bleeding lesions/ history of bleeds Bleeding tendency (e.g. thrombocytopenia) or concomitant
NSAIDs and antibiotics Instability of INR and INR above 3 Have a history of poorly controlled anticoagulation
therapy. Are on multiple other drug treatments (polypharmacy) Are taking antiplatelet drugs
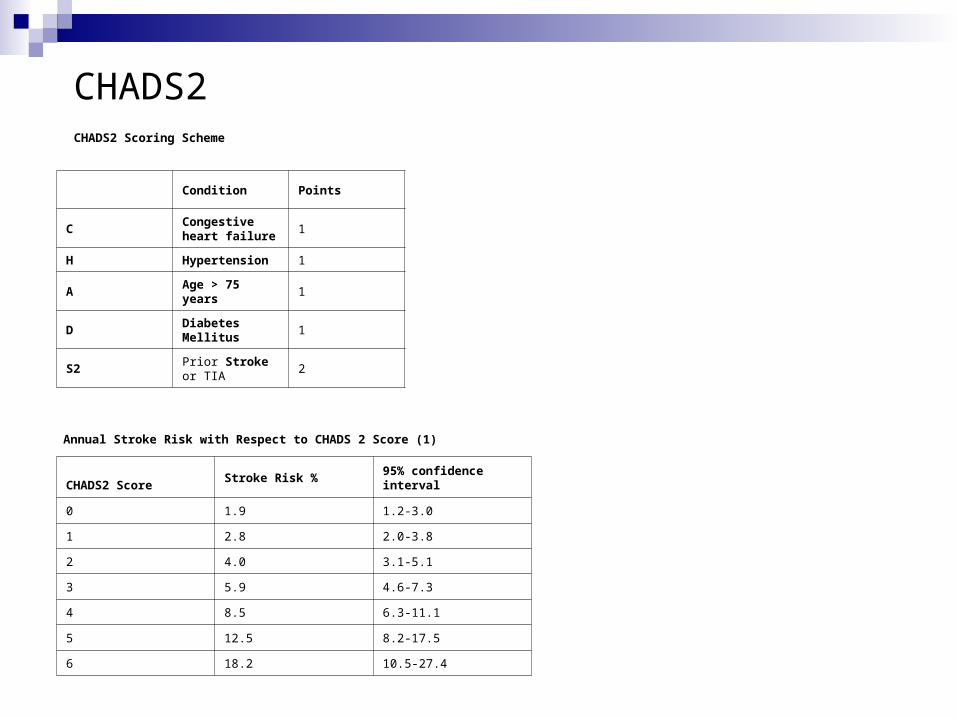
CHADS2 Scoring Scheme
Condition Points
CCongestive heart failure
1
H Hypertension 1
AAge > 75 years
1
DDiabetes Mellitus
1
S2Prior Stroke or TIA
2
Annual Stroke Risk with Respect to CHADS 2 Score (1)
CHADS2 ScoreStroke Risk %
95% confidence interval
0 1.9 1.2-3.0
1 2.8 2.0-3.8
2 4.0 3.1-5.1
3 5.9 4.6-7.3
4 8.5 6.3-11.1
5 12.5 8.2-17.5
6 18.2 10.5-27.4
CHADS2

CHADS2VASCCHA2DS2-VASc score for stroke risk in atrial fibrillation
FeatureScore
Congestive Heart Failure 1
Hypertension 1
Age >75 years 2
Age between 65 and 74 years 1
Stroke/TIA/TE 2
Vascular disease (previous MI, peripheral arterial disease or aortic plaque)
1
Diabetes mellitus 1
Female 1

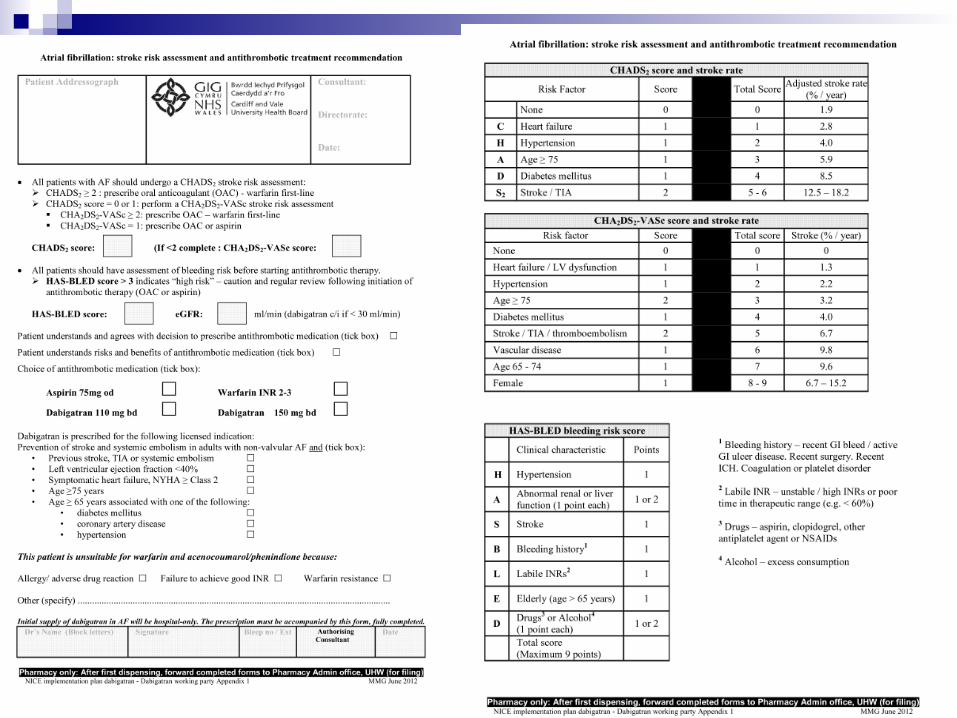
Who is at risk?Circulation 2012; 126: 860-865HAS-BLED score for bleeding risk on oral anticoagulation in atrial fibrillation
FeatureScore if present
Hypertension (Systolic >= 160mmHg)
1
Abnormal renal function
1
Abnormal liver function
1
Age >= 65 years
1
Stroke in past 1
Bleeding 1
Labile INRs 1
Taking other drugs as well
1
Alcohol intake at same time
1
•score of 3 or more indicates increased one year bleed risk on anticoagulation sufficient to justify caution or more regular review
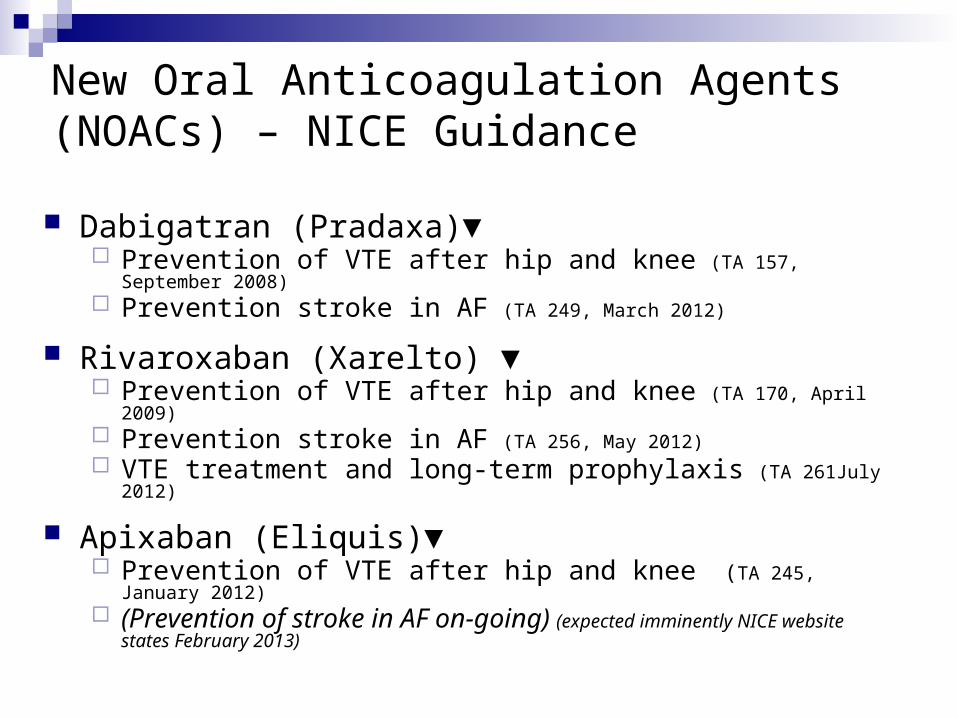
New Oral Anticoagulation Agents (NOACs) – NICE Guidance
Dabigatran (Pradaxa)▼ Prevention of VTE after hip and knee (TA 157, September 2008) Prevention stroke in AF (TA 249, March 2012)
Rivaroxaban (Xarelto) ▼ Prevention of VTE after hip and knee (TA 170, April 2009) Prevention stroke in AF (TA 256, May 2012) VTE treatment and long-term prophylaxis (TA 261July 2012)
Apixaban (Eliquis)▼ Prevention of VTE after hip and knee (TA 245, January 2012) (Prevention of stroke in AF on-going) (expected imminently NICE website
states February 2013)

Dabigatran (Pradaxa) ▼ Used in Cardiff and Vale is for prevention of stroke in AF
Formulary status – Specialist Initiated
Dose is: 150mg twice a day or 110mg twice for patients > 80 years
First prescription from secondary care
Complete documentation prior to the first dispensing from hospital pharmacy
Continued prescribing by GP practices

Rivaroxaban (Xarelto) ▼ Used in Cardiff and Vale is treating deep vein thrombosis
and preventing recurrent deep vein thrombosis and pulmonary embolism after a diagnosis of acute deep vein thrombosis in adults
Formulary status – Hospital Only Dose is 15mg twice a day for 3 weeks then 20mg daily
Patients intolerant of warfarin on LMWH IVDU / alcoholics Patients with precipitated DVT (e.g. following surgery)
Apixaban (Eliquis)▼ Used in Cardiff and Vale for prevention of VTE after hip
and knee replacements (rivaroxaban used previously for this indication by some Cardiff and Vale orthopaedic surgeons)
2.5mg twice a day for 10 to 14 days post knee surgery
2.5mg twice a day for 32 – 38 days post hip surgery
Formulary status – Hospital Only
Full supply from secondary care on discharge
Not to be continued by the GP practice.










![Anticoagulants 2[1]](https://static.documents.pub/doc/80x56/577d22541a28ab4e1e9715d3/anticoagulants-21.jpg)






