Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 1 of 40 It is your responsibility to check on the intranet that this printed copy is the latest version Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Lead Author: The Thrombosis Committee Additional author(s) Kathy Teale (Lead author and primary contact); Peter Woolfson, Rowena Thomas-Dewing, Debbie Morris-Connearn, Liz Lamerton, Jon Watt, Daniel Horner, Janet Hegarty Division/ Department: Pharmacy / Medicines Safety Committee / Thrombosis Committee Applies to: (Please delete) Salford Royal Care Organisation Approving Committee: Thombosis committee Date approved: 12/2/2021 Expiry date: February 2026 Contents Contents Section Page Click here for the document summary sheet: 1 What is the policy about? 2 2 Where will this document be used? 2 3 Why is this document important? 3 4 What is new in this version? 3 5 Guideline – Key Points 3 5.2 Preoperative decision making 4 PREOP FLOWCHART 4 5.3 Should elective surgery be delayed? 5 5.4 Should oral anticoagulation be stopped? 5 5.5 Can oral anticoagulation continue? 5 5.6 Specialist units may have their own policy detailing which procedures require an interruption to oral anticoagulation 5 5.7 When should anticoagulation be stopped? 5 TABLE Safe stopping interval 6 5.8 Bridging therapy for patients on VKA with high thrombosis risk 7 5.8. Which oral anticoagulants are VKA? 7 5.10 Which patients are high thrombosis risk? 7 5.11 Tinzaparin or Enoxaparin? 8 LMWH Choice FLOWCHART 8 5.12 Who will manage the bridging therapy? 9 5.13 What dose of LMWH does the patient need? (body weight nomograms) 9-10 NOMOGRAM Tinzaparin NOMOGRAM Enoxaparin 10 5.1 4 Day of surgery or procedure 11 5.15 Admission and testing 11 Group arrangements: Salford Royal NHS Foundation Trust (SRFT) Pennine Acute Hospitals NHS Trust (PAT)
Transcript
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 1 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Anticoagulation Guideline the Peri-Procedural
Perioperative Management of Patients Taking Oral Anticoagulants
Lead Author: The Thrombosis Committee
Additional author(s) Kathy Teale (Lead author and primary contact); Peter Woolfson,
1. Overview (What is this policy about?) This policy describes the management of patients who are taking oral anticoagulant medicines and who require surgery or invasive procedures. This policy does not cover anti-platelet medicines.
2. Scope (Where will this document be used?)
• Outpatient clinics and Preop
• Units carrying out invasive procedures
• Day Surgery Unit and Surgical Admissions Unit
• Theatres
• Wards Associated Documents “Emergency Reversal of anticoagulation in patients on unfractionated heparins” NCA policy http://intranet.srht.nhs.uk/policies-resources/trust-policy-documents/trust-wide-clinical/gen/twcg0120/?locale=en
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 3 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
“Anticoagulation of patients with prosthetic heart valves” NCA policy http://intranet.srht.nhs.uk/EasysiteWeb/getresource.axd?AssetID=162519&type=full&servicetype=Attachment
3. Background (Why is this document important?)
• When patients on anticoagulation require surgery or an invasive procedure, the risks and benefits of stopping or continuing anticoagulation must be considered.
• It may be necessary to stop oral anticoagulation.
• It may be necessary to replace oral anticoagulation with low molecular weight heparin (LMWH) perioperatively - bridging anticoagulation.
• Anticoagulation medicines always need to be restarted postoperatively. If bridging was required preoperatively, this must continue until oral anticoagulation has reached therapeutic effectiveness.
4. What is new in this version?
No significant changes
5. Guideline
5.1 Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants – Key points
• Patients who have recently (less than 3 months) had a stroke or TIA, VTE or PE will
normally have their surgery postponed.
• Some minor surgery (eg dental extraction, some cardiology interventions, some
endoscopic interventions) can be carried out without stopping anticoagulation.
• Other surgery will require interruption of oral anticoagulation.
• Bridging is not required for patients who have been taking a direct oral anticoagulant
(DOAC).
• Patients taking vitamin K antagonists only require bridging if they are at high risk of
thrombosis.
• Preoperative bridging is usually with low molecular weight heparin (LMWH) at home.
• Patients on long term anticoagulation requiring surgery are complex and high risk.
Cancellations increase the risk of thrombotic complication and/or development of heparin
induced thrombocytopaenia and should be avoided whenever possible.
• Restarting anticoagulation postoperatively balances the risk of haemorrhage with the risk
of thrombosis. The surgical team should review this daily.
• Discharge requires communication with anticoagulation clinic and provision of an
adequate supply of medicines.
• Patients who do not require bridging therapy should receive prophylactic LMWH eg
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 4 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
• Bridging anticoagulation therapy is not required for antiplatelet medicines (see separate
policy)
5.2 Preoperative decision making
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 5 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.3 Should elective surgery be delayed?
There is a group of patients with a very high thrombosis risk, in whom delaying elective surgery
will be beneficial.
• Any patient on anticoagulation therapy who has had a stroke, transient ischaemic attack or venous thromboembolism within the last 3 months should have their surgery delayed if possible.
Contact the surgeon to ask if surgery can be delayed.
5.4 Should oral anticoagulation be stopped?
Several types of surgery at SRFT require the INR to be normal – defined as 1.4 or less (note for the DOAC drugs there is no blood test available). The list can never be completely inclusive; but the broad groups are:
• Neurosurgery or Spinal surgery
• Head and neck surgery
• Abdominal or breast surgery
• TURBT, TURP, ureteroscopic surgery
• Percutaneous nephro-lithotripsy
• Orthopaedic joint replacement and revision surgery
• Laparoscopic surgery
• Endoscopic surgery (See BSG guideline – appendix 4)
• Other major surgery (> 60 min)
5.5 Can oral anticoagulation continue?
Minor surgery can often be performed without stopping the anticoagulant medicine and
there is some surgery for which anticoagulation is beneficial. Most minor surgery is performed under local anaesthetic; it is therefore unlikely that many of these patients will come for preop assessment.
If the planned surgery is minor and does not fit into the above operation groups, please
contact the surgeon to see if they are happy for anticoagulation to continue.
5.6 Specialist units may have their own policy detailing which procedures require an interruption to oral anticoagulation
Where there are policies specific to a specialist unit (eg endoscopy) these should be followed. However all units should follow the bridging therapy outlined in this policy.
5.7 When should anticoagulation be stopped?
Vitamin K antagonists (VKA) and direct oral anticoagulants (DOAC) have variable elimination half-lives. For some, that are renally excreted, the half-life will be dependent on the eGFR. The table below can be used to decide when to stop the anticoagulant.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 6 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
DOAC activity is prolonged by Cytochrome p450 inhibitors, P-glycoprotein inhibitors, NSAIDs, Antiplatelet and other anticoagulant medicines. (see Appendix 2). Discuss with Pharmacy if the patient is taking any of these medicines as well as their DOAC.
5.8 Bridging therapy for patients on VKA with high thrombosis risk
5.9 Which oral anticoagulant medicines may require bridging?
It is only the vitamin K antagonist (VKA) medicines that may require preoperative bridging. Note, abrupt cessation of warfarin can be prothrombotic. The direct oral anticoagulant (DOAC) medicines do not require bridging as they have a short duration of action when stopped and a rapid onset of action when restarted. The vitamin K antagonists are: The direct oral anticoagulants are:
• Warfarin Sodium
• Acenocoumarol (Nicoumalone/ Sinthrome®)
• Phenindione
• Apixaban (Elquis®)
• Rivaroxaban (Xarelto®)
• Edoxaban (Lixiana®)
• Dabigatran (Pradaxa®)
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 7 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.10 If VKA anticoagulation is stopped, who requires bridging therapy?
For some conditions there is a high risk of thrombosis if VKA anticoagulation is stopped. These patients require ‘bridging’ with a short acting anticoagulant, usually with a low molecular weight heparin (LMWH) such as tinzaparin or enoxaparin. PATIENTS WITH HIGH THROMBOSIS RISK ON VKA REQUIRE BRIDGING
• Venous thromboembolism (DVT or PE) less than 3 months ago
• Venous thromboembolism (DVT or PE) more than 3 months ago and very high risk of further VTE, i.e. patients with target INR of 3.5
• Atrial fibrillation with history of TIA, CVA less than 3 months ago
• Atrial fibrillation with history of TIA, CVA more than 3 months ago and 3 or more risk factors (Congestive cardiac failure, Hypertension, diabetes, aged >75 years)
• Other mechanical aortic valve replacement with one or more risk factors for stroke: Risk factors = AF, previous TIA or CVA, hypertension, diabetes, CCF, LV EF <30%, age >75 years
• Known intra-cardiac thrombus
• Known severe thrombophilia (protein C, Protein S, antithrombin deficiency, antiphospholipid antibodies)
Therefore the following conditions do not require bridging
• Atrial fibrillation with no past history of TIA, CVA
• VTE more than 3 months ago and target INR 2.5
• Any tissue valve replacement, any valve repair.
• Mechanical aortic valve replacement and no risk factors for stroke
ONLY patients taking VKA AND with HIGH RISK of further thrombosis require bridging
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 8 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.11 Choice of medicine for bridging therapy
Pre-procedure bridging therapy should start when INR is subtherapeutic. This will be 2 days after stopping warfarin and 1 day after stopping acenocoumarol (Sinthrome) or Phenindione. Bridging therapy with LMWH, last dose should be 24 hours before surgery, i.e. before 08:00 on the morning of the day before surgery. Patients with eGFR>30ml/min: Bridge with tinzaparin 175units/kg daily. Patients with eGFR<30ml/min: Bridge with enoxaparin 1mg/kg once daily. Pharmacy medicines information (65223 or oncall pharmacist via switchboard) can advise on alternative medicine for patients with heparin allergy, with ethical issues relating to use of pig products and patients weighing <40kg or >160kg. Patients with previous HIT will need to be discussed with haematology (Haematology SpRs via switchboard, Haematology secretaries extension 64983, 64982).
NOTE: Patients with heparin allergy, previous Heparin Induced Thrombocytopenia (HIT), ethical objection to the use of pig products and patients with body weight less than 40kg or greater than 160kg will need to be referred to haematology or pharmacy for individualised bridging plan.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 9 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.12 Who manages bridging therapy preoperatively?
Bridging therapy is best managed by the anticoagulation clinic that cares for the patient. All Salford patients should be referred to the Salford clinic. General Practitioners will not be involved with perioperative anticoagulation. For patients outside Salford, please contact the patient’s anticoagulation clinic – we are aware that some clinics (including Macclesfield and Bolton) have no prescribing practitioners. Possible alternative carers are Salford Anticoagulation Clinic and Salford Preop Clinic. The anticoagulation clinic will need to know: the operation, the date of the operation, whether the surgery is Day Case or Inpatient.
5.13 Nomograms for tinzaparin and enoxaparin (40kg to 160kg)
LMWH and renal function All LMWH heparins are renally excreted. Patients with significant renal impairment (eGFR<30ml/min) are at greater risk of accumulating LMWHs, treatment dose enoxaparin is reduced from 1.5mg/kg to 1.0mg/kg for these patients. Patients with CKD 5 (eGFR <15) have unpredictable excretion and anti-Xa assay will be required to assess residual activity before surgery Anti-factor Xa assay Refer to Quick Reference Guide for sample timing and target peak and trough values. LMWH and body weight Careful assessment of individual patient factors considering the risk of bleeding against the risk of thrombosis need to be carried out, especially for obese patients and patients with a low body weight. Patients less than 40kg or greater than 160kg should be discussed with pharmacy (09:00-17:00 medicines information 65223; out of hours oncall pharmacist via switchboard) Patients weighing >160kg have unpredictable absorption of subcutaneous LMWH, antiXa assay may be indicated during postoperative bridging to ensure effective anticoagulation. Nomograms are on the next page.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 10 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Tinzaparin (Innohep) Dosing Nomogram (175units/Kg) once daily for patients with eGFR>30ml/min (colour relates to current Innohep syringe colours)
Actual Body Weight (kg)
Total Daily Dose (175units/Kg)
Volume and Frequency of Tinzaparin pre-filled syringe 20000units/mL to administer subcutaneously (whole syringe)
Greater than 160 Absorption unpredictable. Discuss bridging with Pharmacy 65223
Enoxaparin (Clexane & Clexane Forte) Dosing Nomogram 1mg/Kg once daily for patients with eGFR<30ml/min (colour relates to current Clexane syringe colours)
Body Weight (Kg) Total Daily Dose (1mg/Kg)
Volume and frequency of Enoxaparin syringe to administer subcutaneously
111 – 140 120mg SC once daily 0.8ml 120mg (mauve) forte syringe SC daily
141 – 160 150mg SC once daily 1.0ml 150mg (blue) forte syringe SC daily
Greater than 160 Above 160 kg absorption is unreliable, discuss bridging with pharmacy 65223
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 11 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.14 Day of surgery or procedure
5.15 Admission and testing
Check the day and time of the last dose of oral anticoagulant Check the day and time if the last dose of subcutaneous LMW heparin INR: Patient taking vitamin K antagonists (warfarin, acenocoumarol, phenindione).
INR should be 1.4 or less. Anti-Xa assay: Only recommended for patients on treatment dose LMWH (enoxaparin) with
CKD5 (eGFR <15) as there may be a prolonged effect. Anti-Xa should be 0.1 IU/ml or less. See Quick Reference Guide.
If the patient was taking DOAC (apixaban, edoxaban, dabigatran, rivaroxiban) no blood tests are required, but it should be confirmed with the patient that they have omitted doses correctly in line with the table in section 2.
5.16 Management of INR greater than 1.4
This will depend on the urgency of surgery and the INR value Urgent surgery (no delay possible) Prothrombin complex concentrate (beriplex) List reschedule possible 1mg vit K IV wait 3 to 4 hours and repeat INR See policy emergency reversal of anticoagulation in patients taking oral coumarins for dose recommendations FFP is not used routinely to reverse warfarin anticoagulation. It is important that the patient’s anticoagulation clinic is informed that vitamin K has been given as bridging therapy will need to be extended
5.17 Management of anti-factor Xa > 0.1 IU/ml
ONLY indicated for patients with eGFR <15 who have used treatment dose enoxaparin. Discuss with the Surgeon, who may be happy to proceed with surgery in the presence of residual anticoagulant effect. NB prophylactic range 0.3 - 0.7 IU/ml, therapeutic range 0.5 - 1.2 IU/ml If reversal is required, discuss with haematology (Haematology SpRs via switchboard, Haematology secretaries extension 64983, 64982) or pharmacy (09:00-17:00 medicines information 65223; out of hours oncall pharmacist via switchboard) FFP is not used routinely to reverse heparin anticoagulation.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 12 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.18 Epidural / spinal anaesthesia
Spinal anaesthesia / one shot epidural anaesthesia
• Patients who have not received bridging therapy, can have spinal anaesthesia if the
INR is 1.4 or less or if DOAC was stopped more than 48 hours ago*.
• Patients who are bridging, spinal anaesthesia for surgery is considered to be safe,
provided the INR is 1.4 or less and the last dose of LMWH was more than 24 hours ago*.
Epidural catheter for post op analgesia
• There is a risk of epidural haematoma both at insertion and at removal of epidural
catheters.
• Consider alternative methods of post-operative analgesia such as PCA with wound
catheter.
• If no other mode of anaesthesia/analgesia is suitable, discuss with pain team.
• Do not restart VKA or DOAC until epidural catheter is removed.
• Prophylactic dose LMWH can be given with epidurals in place.
• If Bridging is required while the epidural is in place, Consider unfractionated heparin
infusion. (See separate policy) as UFH can be fully reversed by protamine and
anticoagulant activity will cease within 4 hours of stopping the infusion.
See policy Pain Management Protocol for the management of Epidural Analgesia
* providing eGFR >30ml/min
5.19 Hospital acquired thrombosis prophylaxis
Prophylactic tinzaparin is indicated for patients who have stopped oral anticoagulation but are not receiving bridging with therapeutic dose LMWH. It is important that this is replaced by therapeutic dose LMWH bridging at the earliest opportunity in patients with high risk of thrombosis (who were bridging preoperatively). Antiembolism stockings and/or Intermittent Pneumatic Compression Devices (IPCD) should be used during surgery unless contraindicated. IPCDs may be prescribed for postoperative use. See Policy for the Prevention of Hospital Acquired Thrombosis
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 13 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.20 Management of major haemorrhage
Activate the major haemorrhage protocol. For patients on DOACs – follow the ‘Management of bleeding in patients on NOACs/DOACs’ For patients on VKA - consider vitamin K or Prothrombin complex concentrate – follow the Emergency reversal of anticoagulation in patients taking oral coumarins (eg.Warfarin)
5.21 Management of anticoagulation if surgery is cancelled
Occasionally it is not possible to proceed with surgery and the operation has to be cancelled. It is vitally important that a clear plan is set out for the patient before they are discharged.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 14 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Service teams should be aware of all patients who have interrupted anticoagulation therapy, and consider this when deciding priority. Service team must provide new date for surgery within 2 weeks. A new date must be agreed so that anticoagulation advice can be given. If the delay is more than 2 weeks discuss with haematology / anticoagulation. Standard oral anticoagulation will be restarted. Medication advice (new date < 2 weeks) Patients treated with direct oral anticoagulant (DOAC)
• Restart DOAC. Instruct the patient to stop the DOAC 48 hours (for dabigatran check
eGFR and adjust instruction as necessary – see section 6.2) before the revised date for
surgery
Patients treated with vitamin K antagonist who do not require bridging
• Do not restart vitamin K antagonist
• Do not prescribe LMWH Patients treated with vitamin K antagonist who require bridging
• Do not restart vitamin K antagonist
• Continue treatment dose LMWH – will need new outpatient prescription for supply of treatment dose LMWH to last until revised date of surgery
• Provide new diary sheet with date of operation, date of last LMWH Medication advice (new date >2 weeks) Restart usual oral anticoagulation regime. New plan to be arranged when new admission date is agreed. Adverse incident report
• All cancellations are adverse incidents; however cancellation of patients who have
stopped anticoagulation increases the risk of serious thrombosis and thromboembolism.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 15 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.20 Post-operative management of anticoagulation
5.21 Day surgery patient management
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 16 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
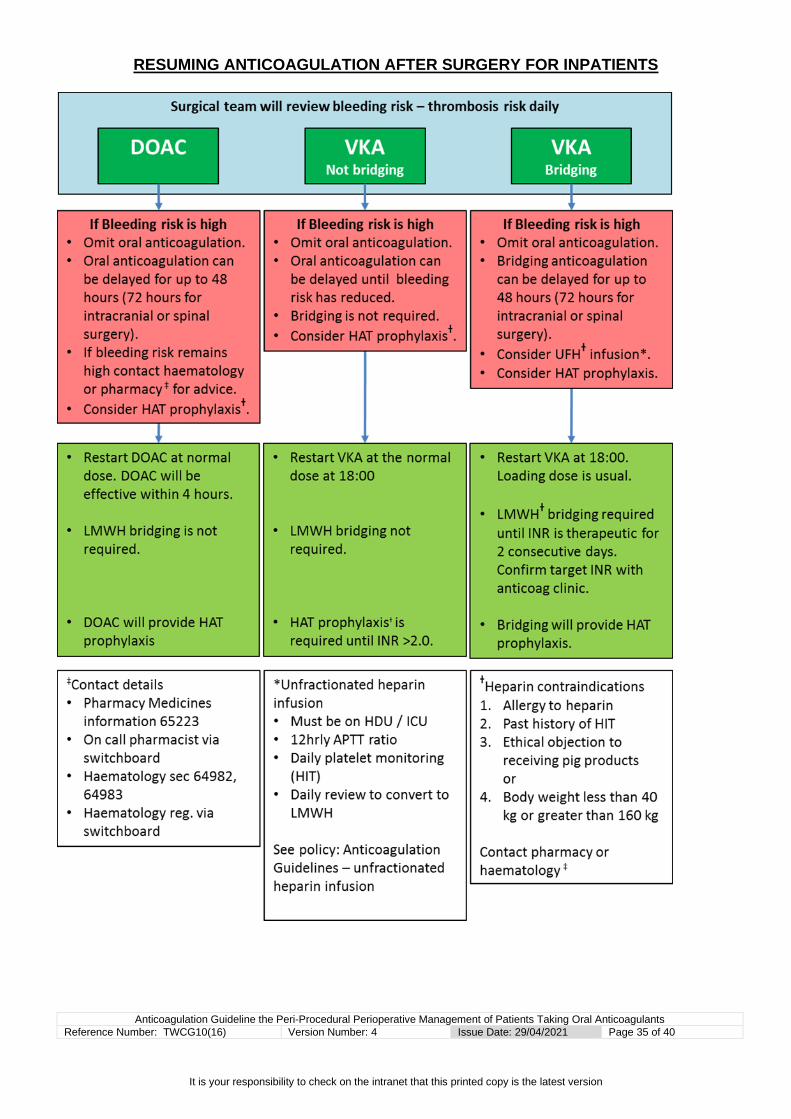
1. Patients treated with direct oral anticoagulant. The surgeon will decide whether the patient should restart their DOAC on the day of surgery or on the following day. No loading dose is needed, the patient should restart at their normal dose. If HAT prophylaxis is indicated, the DOAC will be effective. LMWH is not required.
2. Patients treated with vitamin K antagonists, who are not bridging The surgeon will decide whether the patient should restart their VKA on the day of surgery or on the following day. Loading is not recommended. Restart the oral VKA at the patients normal dose. If HAT prophylaxis is indicated, prophylactic dose LMWH must also be prescribed until the INR is considered therapeutic. 3. Patients treated with vitamin K antagonists who are bridging The surgeon will decide whether the patient should restart their VKA on the day of surgery or on the following day. The patient will restart their bridging LMWH injection on the same day. It is very likely that the anticoagulation clinic will have instructed the patient on what doses of VKA they should take. Loading is recommended. First dose 2 x normal dose, second dose 1.5 x normal dose, third dose and subsequent doses are normal dose. Sub-cutaneous injections of treatment dose LMWH must continue until the INR is therapeutic, supervised by the patients anticoagulation clinic. 4. Discharge requirements for patients on VKA who are bridging
• Check that the patient has adequate LMWH syringes
• Check that the patient has a post-operative anticoagulation clinic appointment
• Check that the patient has verbal and written instructions regarding the start date and start dose of their oral anticoagulant
Inform the surgical team if requirements are not met.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 17 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.22 Inpatient management
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 18 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.23 Managing patients with a high bleeding risk
Patients on DOAC Anticoagulation can be delayed for 48 hours (72 hours if intracranial or spinal surgery). If the bleeding risk is still high, discuss with Haematology or Pharmacy whether delay can continue or whether alternative anticoagulation is indicated. HAT prophylaxis should be prescribed if indicated: Prophylactic dose LMWH* and/or intermittent pneumatic compression device
Oral anticoagulation should start as soon as possible. Review daily. Patients on VKA who are not bridging Anticoagulation can be delayed until the risk of postoperative bleeding has reduced. HAT prophylaxis should be prescribed if indicated: Prophylactic dose LMWH* and/or intermittent pneumatic compression device Patients on VKA who are bridging Anticoagulation should not be postponed longer than 48 hours (72 hours for intracranial and spinal surgery) post op. Do not restart oral anticoagulation while bleeding risk is high. Consider: Low molecular weight heparin* at treatment dose (see 6.6.5 nomograms)
Therapeutic LMWH will remain active for 24 hours after injection Protamine may partially reverse LMWH The risk of HIT is low Does not require HDU
Unfractionated heparin* infusion (see separate policy) Heparin will be active for 4 hours after stopping infusion Heparin can be fully reversed with protamine Will require 12 hourly APTT ratio monitoring Will require daily FBC to monitor for heparin induced thrombocytopaenia (HIT) Will require HDU/ICU care Review daily and convert to LMWH
* Check heparin allergy, previous HIT, ethical issues with pig products, body weight <40kg or >160kg. Discuss alternative with Pharmacy or Haematology.
Review daily. Restart oral anticoagulation when bleeding risk has reduced.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 19 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5.24 Managing patients who do not have a high bleeding risk
1. Patients treated with direct oral anticoagulants The surgeon will decide when to restart the DOAC. Usually 24 – 48 hours for general surgery; 48 – 72 hours for neuro surgery and spinal surgery. As DOAC have a rapid onset of action, bridging is not required. Prophylaxis against hospital acquired thrombosis is provided by the DOAC. 2. Patients treated with vitamin K antagonists who are not bridging The surgeon will decide when the patient should restart their VKA. Usually 24 – 48 hours for general surgery; 48 – 72 hours for neuro surgery and spinal surgery. Start the VKA at the patients usual dose. Bridging is not required. If Thromboprophylaxis for HAT is indicated LMWH* at prophylactic dose should be prescribed until the INR is > 2.0. 3. Patients treated with vitamin K antagonists who are bridging The surgeon will decide whether the patient should restart their oral anticoagulation. Usually 24 – 48 hours for general surgery; 48 – 72 hours for neuro surgery and spinal surgery. Check INR daily. Loading is recommended. First dose 2 x normal dose, second dose 1.5 x normal dose third dose and subsequent doses are normal dose. Bridging with sub-cutaneous injections of LMWH* at treatment dose must continue until the INR is therapeutic on 2 consecutive days. Target INR 2.5 to 4.0 depending on indication and patient factors should be checked with anticoagulation clinic or yellow anticoagulation record book. The bridging dose of LMWH will provide HAT prophylaxis. * Check heparin allergy, previous HIT, ethical issues with pig products, body weight <40kg or >160kg. Discuss alternative with Pharmacy or Haematology.
5.24 Discharge after inpatient stay
Patients taking vitamin K antagonists require a follow up appointment with their anticoagulation clinic, usually within 3 days of discharge. Patients who are still on treatment dose LMWH because their INR is not therapeutic will need to continue the LMWH until their anticoagulation clinic appointment. An outpatient prescription will be required. Note: some out of area anticoagulation clinics cannot manage bridging, if this is the case alternative care must be arranged.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 20 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
6. Roles and responsibilities
All clinical staff involved in the prescribing and administration of anticoagulant drugs must adhere to this policy including full documentation in electronic patient records as detailed. This policy should be read in conjunction with the relevant clinical anticoagulation treatment guidelines. The Trust Board has overall responsibility for developing, implementing and monitoring the effectiveness of this policy. The Chief Executive is accountable to the Trust Board for ensuring that :
• Policy is developed and implemented across the Trust
• Implementation is monitored and that any deficiencies are brought to the attention of the Trust Board
The Executive Nurse Director has delegated responsibility for:
• Ensuring that the Trust has a comprehensive policy for the prevention of harm from anticoagulation.
• Developing an effective implementation strategy
• Ensuring monitoring arrangements are in place for the effectiveness of the Policy
The Divisional Managing Directors and Divisional Directors of Nursing are responsible for:
• Keep under review current risk assessment, control measures, procedures and training within their areas to ensure where deficiencies are identified, recommendations and actions plans are developed.
• Ensure adequate provision of training and support to staff in relation to the requirements of the policy and the administration of anticoagulant therapy.
• Ensure all deviations from policy are identified via the adverse incident system.
The Executive Medical Director, Clinical Directors, Clinical Leads and Consultants will be responsible for:
• Ensure systems are in place on admission to identify those patients who are at risk of developing thrombosis or complications from anticoagulation drug therapy.
• Ensure all staff develop and maintain basic professional competence in prevention of harm from anticoagulation therapy and are aware of their responsibilities in preventing its occurrence,
• Ensuring all prescriptions for anti-coagulant drugs are in accordance with this policy.
• Ensure all confirmed episodes of bleeding or thrombosis are documented as complications on EPR within Health Issues
Lead Nurses, Matrons and Ward Managers, will within their areas of control:
• Ensure systems are in place on admission to identify those patients who are taking anticoagulant drug therapy.
• Ensure all staff develop and maintain basic professional competence in administration of anticoagulant drug therapy and are aware of their responsibilities in preventing harm from anticoagulation.
• Ensure all staff develop and maintain an appropriate level of knowledge in the use and administration of anticoagulation drug therapy. .
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 21 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
• Ensure reporting systems are in place to inform medical staff of any suspected DVT or PE or episodes of bleeding or INR>7 and that all confirmed episodes
• are documented as complications on EPR within Health Issues.
• Ensure that any deviations from policy are reported via the adverse incident system
All staff will:
• Ensure anticoagulation drugs are administered in accordance with the prescription, which is in line with the policy.
• Inform medical staff of any suspected occurrences of thrombosis or bleeding Ensure all episodes of thrombosis or bleeding are documented as complications on EPR within Health Issues.
• Ensure all deviations from policy are reported via the adverse incident system.
• Ensure that inadequacies in stock level of anticoagulation drugs are reported immediately to the ward/unit manager.
Pharmacy is responsible for:
• Ensuring that all prescriptions clinically checked for anticoagulation drug therapy comply with the guidelines or have documented reasons for variation.
• Ensure ward stock levels of anticoagulation drugs are maintained. The Thrombosis committee
• Revise and update the policy every 2 years
• Receive and seek answers to queries relating to the policy
• Identify all instances of hospital acquired thrombosis
• Identify all instances of anticoagulant associated bleeding
• Identify all adverse incidents relating to anticoagulation
7. Monitoring document effectiveness
• Key standards: o 100% anticoagulated patients will be identified at preop o 100% anticoagulated patients will be highlighted on the theatre templates o INR will be checked for all patients on VKA anticoagulants o Surgeons will write post op anticoagulation plan on EPR o 100% anticoagulated patients restart their anticoagulation
• Method(s)*: o AIR system o Automated data to thrombosis committee o Annual audit
• Team responsible for monitoring: o Thrombosis committee
• Frequency of monitoring: o Annually
• Process for reviewing results and ensuring improvements in performance: o Through thrombosis committee o Pharmacy updates o Clinical governance meetings
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 22 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
*If clinical audit is an appropriate method of monitoring inclusion of an audit tool in the appendix is encouraged. Clinical audits must be registered with the Clinical Audit Department. Where evidence of non-compliance with the policy is to be monitored through submission of adverse incident reports (DATIX) a description of how this data will be collected, collated and reported should be provided in this section.
.
8. Abbreviations and definitions
Terms are explained in the document
9. References and Supporting Documents
1. Daniels PR. Peri-procedural management of patients taking oral anticoagulants BMJ 2015; 351 doi: http://dx.doi.org/10.1136/bmj.h2391
2. James D. Douketis JD, Spyropoulos AC, Kaatz S et al, for the BRIDGE Investigators. Perioperative Bridging Anticoagulation in Patients with Atrial Fibrillation N Engl J Med 2015; 373:823-833
3. Healey JS, Eikelboom J, Douketis J, et al. Periprocedural bleeding and thromboembolic events with dabigatran compared with warfarin: results from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) randomized trial. Circulation 2012;126:343-8
4. Sherwood MW, Douketis JD, Patel MR, et al. Outcomes of temporary interruption of rivaroxaban compared with warfarin in patients with nonvalvular atrial fibrillation: results from the rivaroxaban once daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and embolism trial in atrial fibrillation (ROCKET AF). Circulation 2014;129:1850-9
5. Garcia D, Alexander JH, Wallentin L, et al. Management and clinical outcomes in patients treated with apixaban vs warfarin undergoing procedures. Blood 2014;124:3692-8
6. Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2013;369:2093-104
7. Priori SG et al. Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology. European Heart Journal 2007; 28: 253 – 258
8. Bonow RO et al. 2008 Focused Update Incorporated Into the ACC/AHA 2006 Guidelines for the Management of Patients With Valvular Heart Disease. Journal of the American College of Cardiology 2008; 52 (13): e104 – 108
Review will occur by the author, or a nominated person, within five years or earlier
should a change in legislation, best practice or other change in circumstance
dictate.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 24 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
11. Equality Impact Assessment (EqIA) tool
• The below tool must be completed at the start of any new or existing policy, procedure, or guideline development or review. N.B. For ease, all documents will be referred to as ‘Policy*’. The EqIA should be used to inform the design of the new policy and reviewed right up until the policy is approved and not completed simply as an audit of the final Policy itself.
• All sections of the tool will expand as required.
• EqIAs must be sent for review prior to the policy* being sent to committee for approval. Any changes made at committee after an EqIA has been sign off must result in the EqIA being updated to reflect these changes. Policies will not be published without a completed and quality reviewed EqIA.
Help and guidance available:
• Click here for the Policy*EqIA Tips for Completion QRG
• Email the Group EDI Team: [email protected] for advice or training information.
• Submission of policy* documents requiring EqIA sign off to: [email protected]. Allowing an initial four week turnaround.
• Where there is a statutory or significant risk, requests to expedite the review process can be made by exception to the Group Equality & Inclusion Programme Manager [email protected]
1. Possible Negative Impacts
Protected Characteristic Possible Impact Action/Mitigation
Age no
Disability no If patient has a carer, carers would also be informed of plan for anticoagulation management by preop team
Ethnicity no If there is a language barrier, patients would be informed of anticoagulation plan using the existing interpreter service
Gender no
Marriage/Civil Partnership no
Pregnancy/Maternity no
Religion & Belief no
Sexual Orientation no
Trans no
Other Under Served Communities (Including Carers, Low Income, Veterans)
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 25 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
5. EqIA Update Log (Detail any changes made to EqIA as policy has developed and any additional impacts included)
Date of Update Author of Update Change Made
2. Possible Opportunity for Positive Impacts
Protected Characteristic Possible Impact Action/Mitigation
Age no
Disability no
Ethnicity no
Gender no
Marriage/Civil Partnership no
Pregnancy/Maternity no
Religion & Belief no
Sexual Orientation no
Trans no
Other Under Served Communities (Including Carers, Low Income, Veterans) no
no
3. Combined Action Plan
Action (List all actions & mitigation below)
Due Date Lead
(Name & Job Role)
From Negative or Positive Impact?
4. Information Consulted and Evidence Base (Including any consultation)
Protected Characteristic Name of Source
Summary of Areas Covered
Web link/contact info
Age n/a
Disability n/a
Ethnicity n/a
Gender n/a
Marriage/Civil Partnership n/a
Pregnancy/Maternity n/a
Religion & Belief n/a
Sexual Orientation n/a
Trans n/a
Other Under Served Communities (Including Carers, Low Income, Veterans)
n/a
6. Have all of the negative impacts you have considered been fully mitigated or resolved? (If the answer is no please explain how these don’t constitute a breach of the Equality Act 2010 or the Human Rights Act 1998) this is a policy for medical management of medication in theperioperative period, based entirely on the patient’s indication for anticoagulation and medical history. – there are no equality and diversity issues as decisions are not based on any of the above characteristics. The outcome of the decision making process about anticoagulation medication would be communicated to the patient
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 26 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
or carer by the preop team in the same way as any other part of their admission process. If the patient has a learning or physical disability meaning they require help from carer, the carer would also be informed of the decision. IF language is a barrier, the interpreter service would be used to aid communication of the medicines management decisions.
7. Please explain how you have considered the duties under the accessible information standard if your document relates to patients? All patients are able to ask about and be involved with these decisions. which would be fully explained to them at preop assessment since they will be involved in their own medication management. Interpreter services would be used where necessary.
8. Equality Impact Assessment completed and signed off? (Insert named lead from EDI Team below). Please also add this information within Section 11. Name: Joe McMahon Date: February 2021
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 27 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
12. Appendices
Appendix 1 Oral Anticoagulants
Vitamin K antagonists (VKA’s) Warfarin Warfarin is a highly bioavailable VKA that is readily absorbed from the gastrointestinal tract and oxidatively metabolised primarily through the cytochrome P450 system. Half-life = 36-42 hours, therefore it usually takes several days for effect to develop when started and to abate when it is stopped. Acenocoumarol (Sinthrome) Bioavailability and metabolism are similar to that of warfarin, although has a shorter half-life of 8 - 12 hours Direct Oral Anticoagulants (DOACs) Four drugs are currently available: dabigatran, rivaroxaban, apixaban, and edoxaban. These drugs are given at fixed doses and coagulation are not routinely monitored. They are categorised on the basis of where in the coagulation cascade they exert their inhibitory effect. The two categories currently available are direct thrombin inhibitors and Factor Xa inhibitors. Direct thrombin inhibitors / direct oral anticoagulants (DOACs) Dabigatran is a direct thrombin inhibitor administered as the prodrug dabigatran etexilate. Once absorbed it is converted to its active form and promotes anticoagulation by directly binding to the active site of thrombin, competitively inhibiting the conversion of fibrinogen to fibrin. Peak plasma concentrations are reached in about 1.5 hours and the half-life ranges from 8 - 14 hours, with about 80% of the drug being eliminated renally. Factor Xa inhibitors / direct oral anticoagulants (DOACs) Factor Xa inhibitors target the prothrombin binding site on Factor Xa, which converts prothrombin to thrombin. Rivaroxaban reaches peak plasma concentrations in 2 - 4 hours; half-life is 7 - 11 hours, about 33% of the active drug is renally excreted. Apixaban reaches peak plasma concentration in approx. 3 hours, half-life of 8 - 15 hours. About 25% of the drug is eliminated renally, with most being eliminated through hepatic metabolism and the faeces. Edoxaban reaches peak plasma concentration in 1 – 2 hours, half-life is 9-10 hours; about 35% of the drug is renally excreted.
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 28 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Appendix 2 Drug interactions
DOAC medicine activity is prolonged / increased by
Cytochrome P450 3A4 inhibitors
P-glycoprotein inhibitors Others
HIV protease inhibitors • ritonavir • indinavir • nelfinavir • saquinavir some macrolide antibiotics • clarithromycin • telithromycin • erythromycin chloramphenicol (antibiotic) some azole antifungals • ketoconazole • itraconazole • fluconazole nefazodone (antidepressant) cobicistat aprepitant (antiemetic) some calcium channel blockers • verapamil • diltiazem bergamottin (constituent of grapefruit juice) Valerian
111 – 140 120mg SC once daily 0.8ml 120mg (mauve) forte syringe SC daily
141 – 160 150mg SC once daily 1.0ml 150mg (blue) forte syringe SC daily
Greater than 160 Above 160 kg absorption is unreliable, discuss bridging with pharmacy
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 32 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 33 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
MANAGEMENT OF PATIENTS CANCELLED ON THE DAY OF SURGERY
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 34 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
RESUMING ANTICOAGULATION AFTER DAY SURGERY
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 35 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
RESUMING ANTICOAGULATION AFTER SURGERY FOR INPATIENTS
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 36 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Appendix 4 Endoscopy anticoagulant policy (BSG)
App endix 3 Flowcharts
and tables
dix 4 Endoscopy anticoagulant policy (BSG)
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 37 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Appendix 5 Pre-printed diary sheet
PREOPERATIVE INSTRUCTION
Last dose of warfarin day -6 (No warfarin from day -5), LMWH starts in the morning on day -3 (If surgery day is Monday, last warfarin dose is Tuesday before, LMWH starts on Friday morning) Last dose of acenocoumarol or phenindione is day -4, LMWH starts day -2
Last dose of LMWH is morning of day before surgery day -1 POSTOPERATIVE DAY CASE INSTRUCTION
Vit K antagonist starts on evening of day of surgery (day 0 dose x2, day 1 dose x 1.5, then normal dose) LMWH starts at surgeons instruction. Usually 6 hours post op. and continues PM daily until INR therapeutic. POST OPERATIVE INPATIENT INSTRUCTION
Surgeon will decide after daily review. Usually 24 – 48 hour after general surgery, 48 – 72 hours after neuro or spinal surgery
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 38 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Appendix 6 Community nurse referral
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 39 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Anticoagulation Guideline the Peri-Procedural Perioperative Management of Patients Taking Oral Anticoagulants Reference Number: TWCG10(16) Version Number: 4 Issue Date: 29/04/2021 Page 40 of 40
It is your responsibility to check on the intranet that this printed copy is the latest version
Appendix 7 HIP FRACTURE Management HIP FRACTURE; Management of patients on anticoagulant and antiplatelet medicines LINK