28
Aortic Valve Repair
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | jade-muriel-elliott |
| View: | 226 times |
| Download: | 2 times |

Aortic Valve Repair

Aortic Root
• Annulus
• Cusp
• Sinus
• ST junction
• Sub Commissure Triangle

TEE
• Cusp number• Diameter of annulus, S of Valsalva , STJ• Cusp thickness• Free margin• Coaptation line• Direction and size of Rergurgitation Jet• Mechanism: Dissection, Aneurysm of Aortic root, Leaflet
prolapse, Endocarditis, Degenerative

Repair For
• AI
or
• Aortic Root Aneurism

Repair:When?• limited to patients with (AR) without a component
of stenosis.
• Repair may not be justified in older patients with excellent proven longevity of bioprostheses.
• Bicuspid valves may be less amenable to reparative techniques than tricuspid valves, because the calcification in
the bicuspid valve is more diffuse from free margin to aortic wall
• Valve repair is an established part of the treatment armamentarium for aortic valvular disease but is a technique in evolution, requiring better definition of successful approaches.
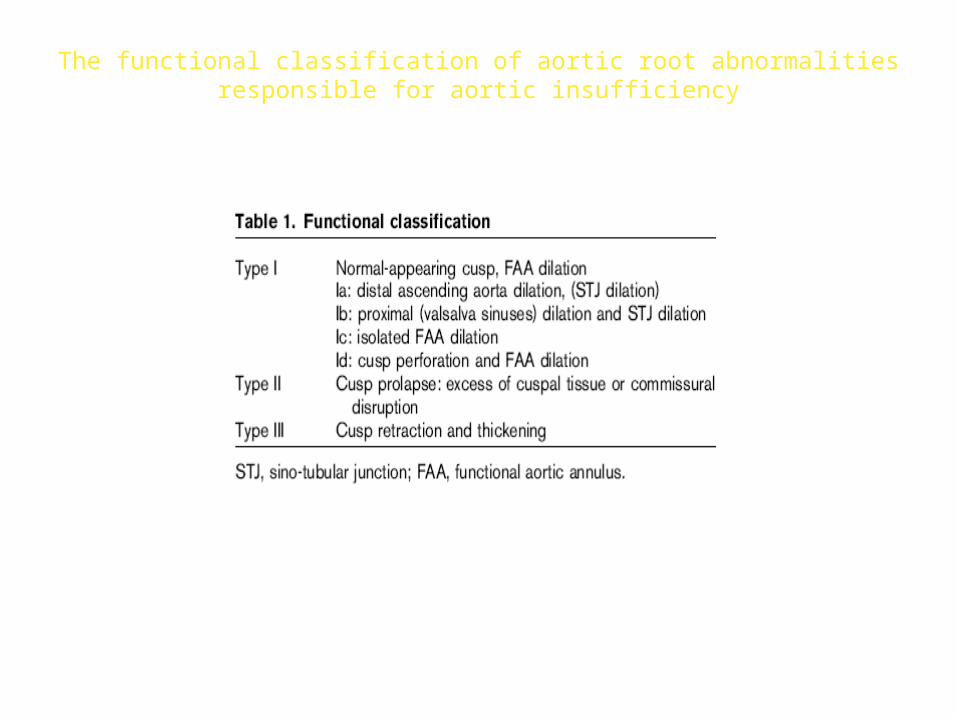
The functional classification of aortic root abnormalitiesresponsible for aortic insufficiency
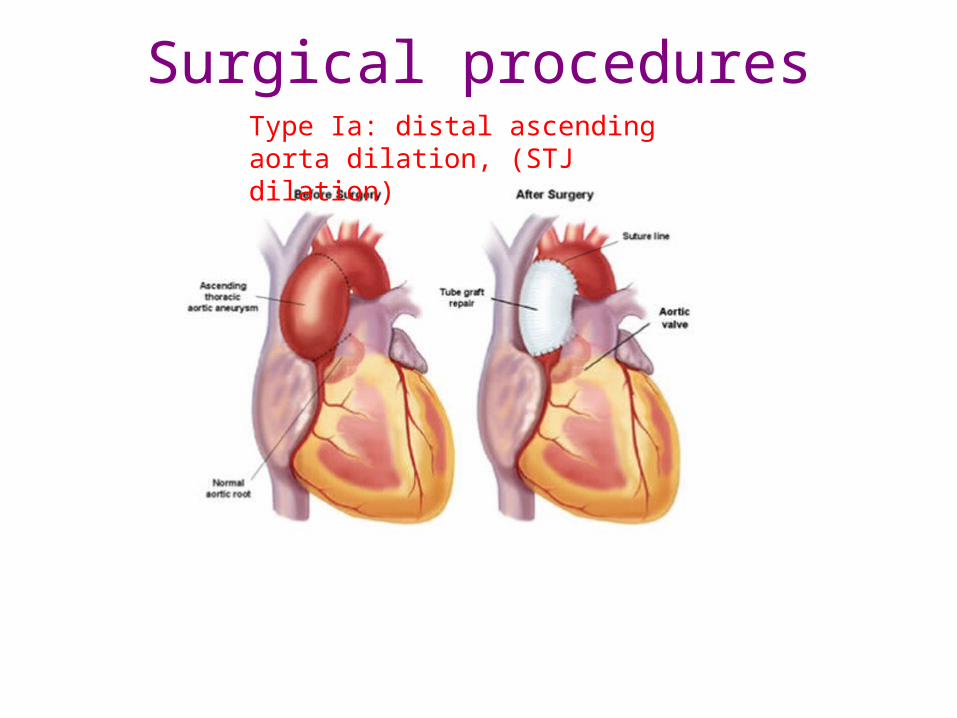
Surgical proceduresType Ia: distal ascending aorta dilation, (STJ dilation)

Surgical procedures
Type Ia lesions are treated by reduction of the circumference of the Sino-tubular junction and is usually achieved by replacing the ascending aorta with an appropriately sized Dacron graft.
Ideally, its diameter should be approximately the size of the native aortic annulus
Type Ia: distal ascending aorta dilation, (STJ dilation)

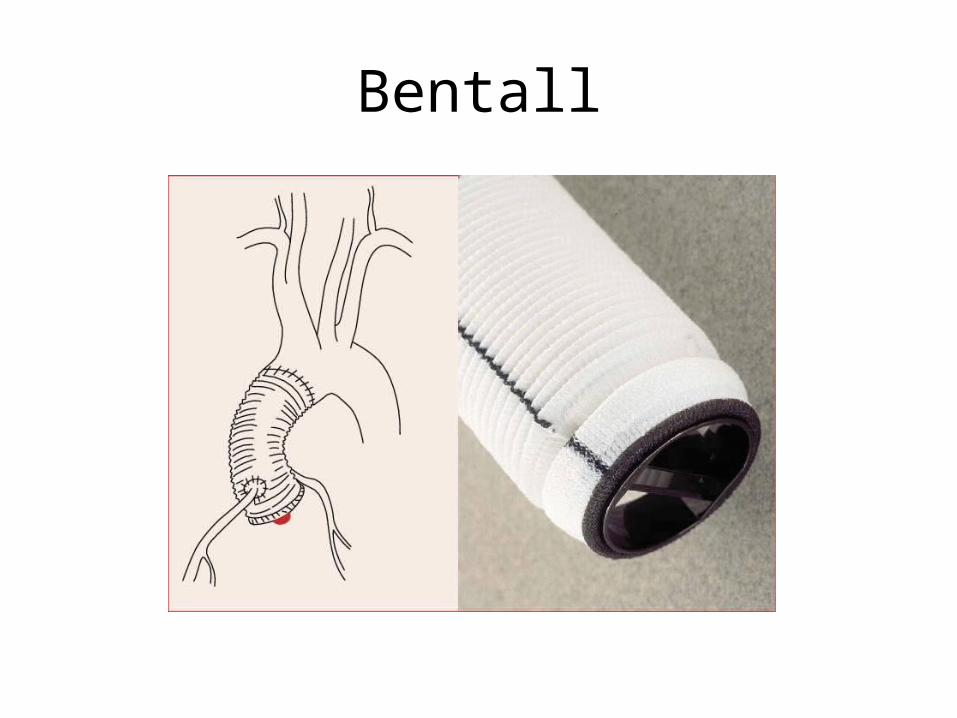
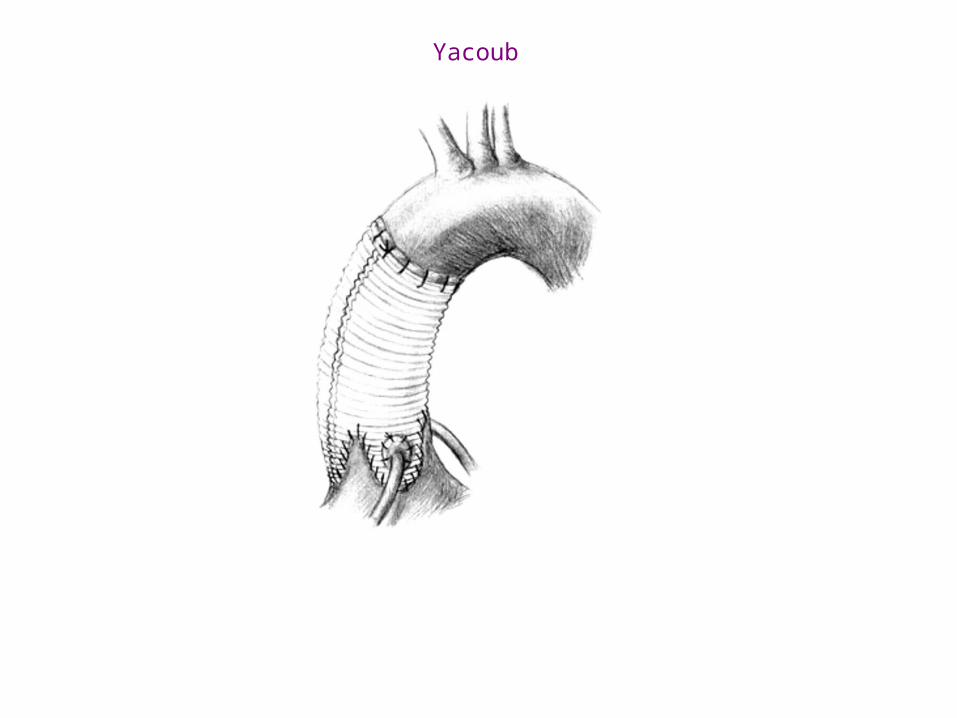
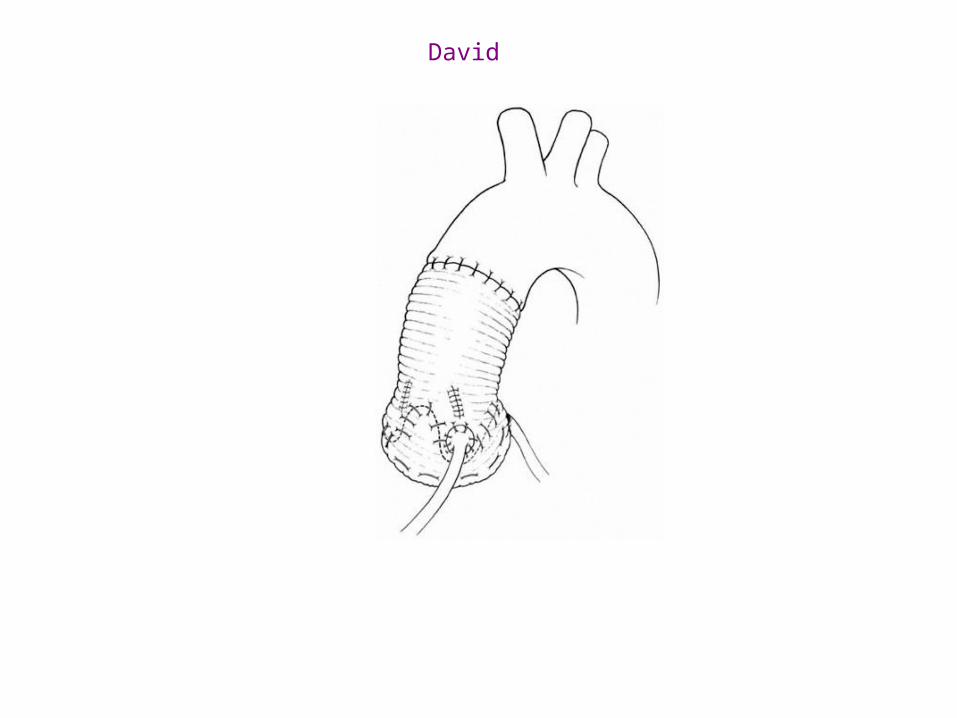
Type Ib: proximal (valsalva sinuses) dilation and STJ dilation

Horizontal mattress sutures without pledges are placed in one lane underneath the sinuses for later fixation of the graft to the aortic root.
Kallenbach K et al. MMCTS 2007;2007:mmcts.2006.001917
© 2007 European Association for Cardio-thoracic Surgery


David Yacoub

Surgical procedures
For the Type Ic the most appropriate surgical procedure may be a partial sub-commissural annuloplasty or circular annuloplasty
Circular Annuloplasty
Type Ic: isolated FAA dilation
Commissural Annuloplasty

Reduction annuloplasty
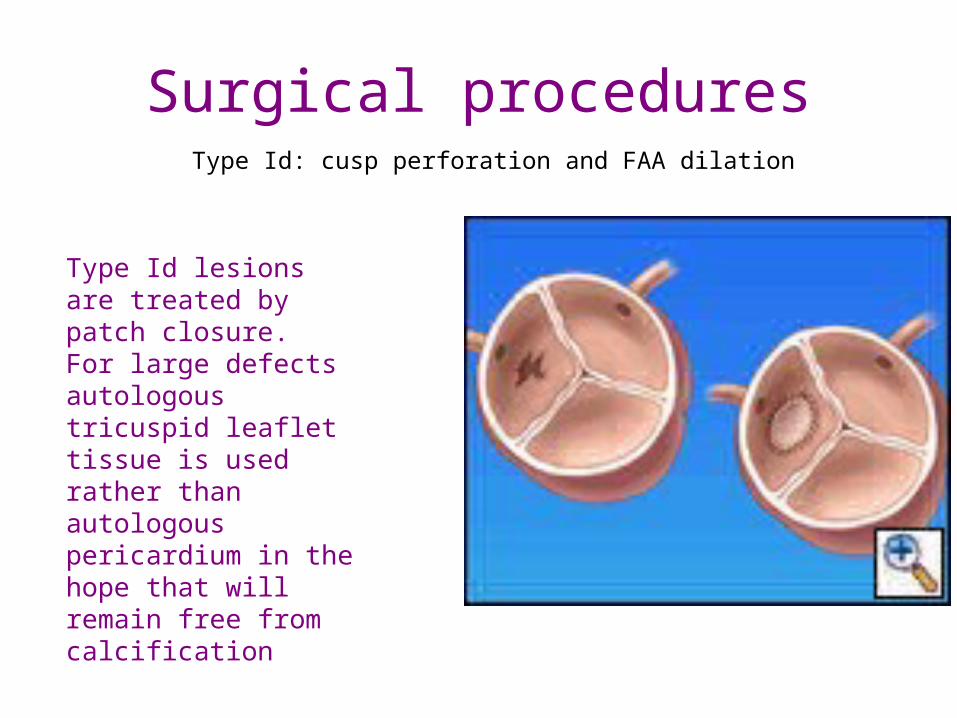
Surgical proceduresType Id: cusp perforation and FAA dilation
Type Id lesions are treated by patch closure.For large defects autologous tricuspid leaflet tissue is used rather than autologous pericardium in the hope that will remain free from calcification
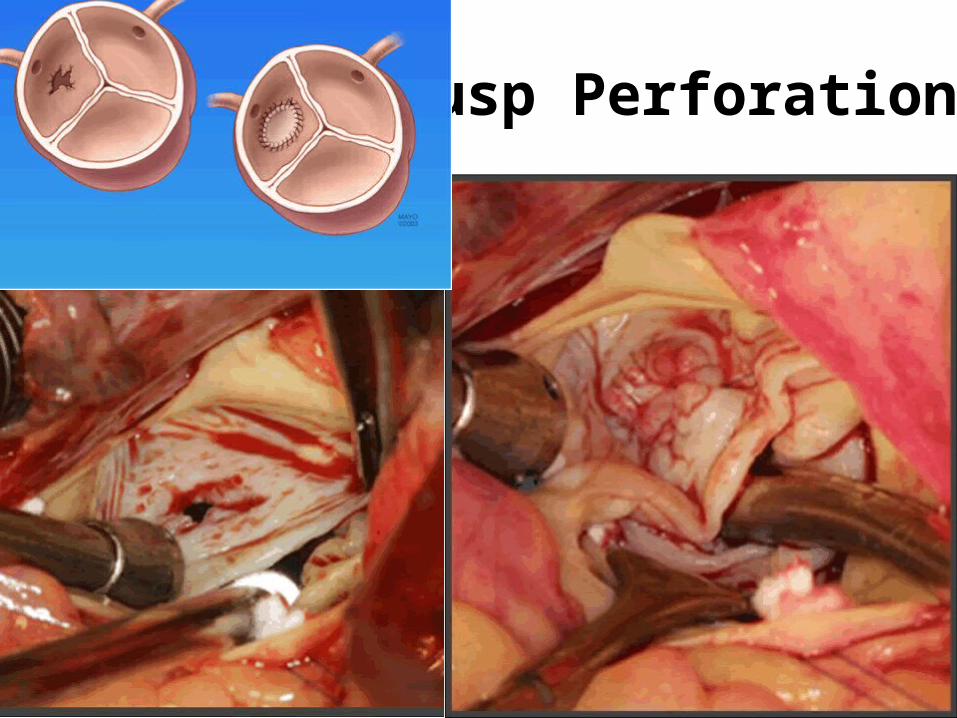
Cusp Perforation
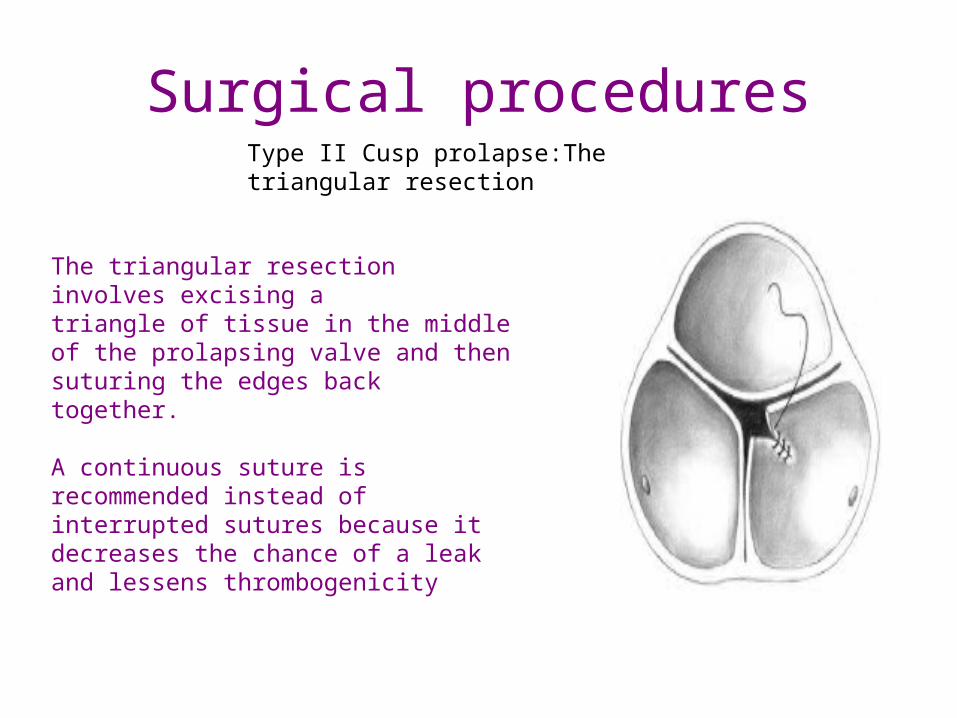
Surgical proceduresType II Cusp prolapse:The triangular resection
The triangular resection involves excising atriangle of tissue in the middle of the prolapsing valve and then suturing the edges back together.
A continuous suture is recommended instead of interrupted sutures because it decreases the chance of a leak and lessens thrombogenicity

Cusp Prolapse in Tricuspid Valve
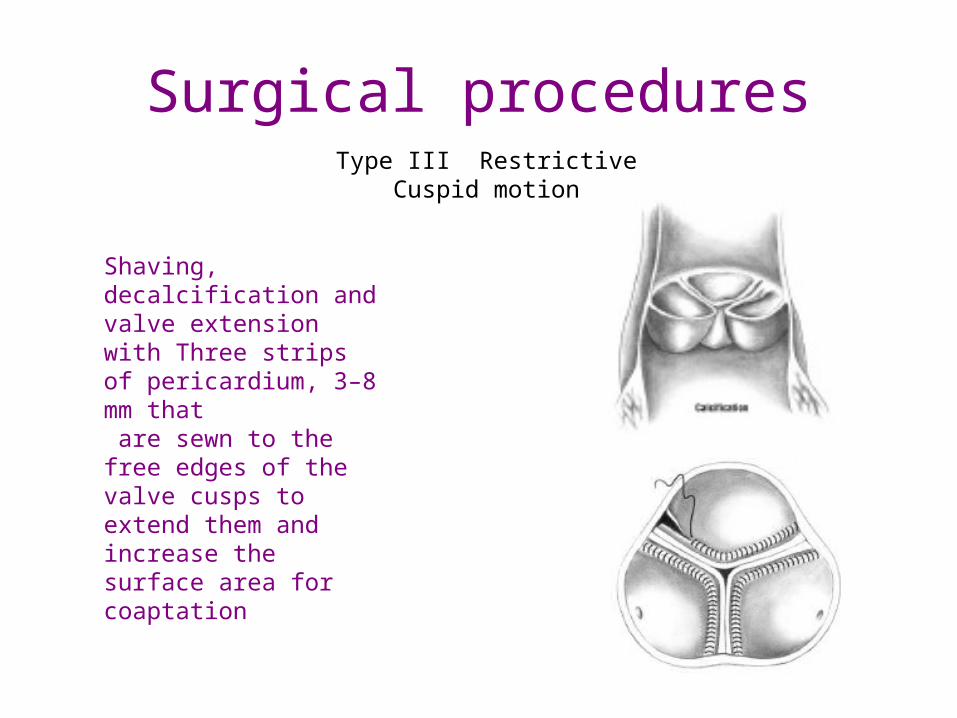
Surgical proceduresType III Restrictive Cuspid motion
Shaving, decalcification and valve extension with Three strips of pericardium, 3–8 mm that are sewn to the free edges of the valve cusps to extend them and increase the surface area for coaptation


Bicuspid Aortic Valve

Reoperation• The Toronto group reported a 26% reoperation rate at 5 years in
theirs series of 54 adults
• Surgeons at the Cleveland Clinic reported a 13% reoperation rate in a series of BAV patients
• We reported our experience at Mayo Clinic in 160 consecutive patients with indications for valve repair including a dilated annulus, BAV and trileaflet valve cusp prolapse [1]. At 5 years, the reoperation rate was 11% overall and 10%, 9% and 16% for dilated annulus, BAV and trileaflet valve cusp prolapse respectively.