APIXABAN NELLA SPAF 21 maggio 2015 ROMA Dott. Sergio Agosti Cardiologo, Ospedale Novi Ligure (AL) www.docvadis.it/agostisergi o [email protected]http://www.arcaliguria.it/ SPAF: quale ruolo ha ancora l’ASA?
Transcript
APIXABAN NELLA SPAF21 maggio 2015
ROMA
Dott. Sergio AgostiCardiologo, Ospedale Novi Ligure (AL)www.docvadis.it/[email protected]://www.arcaliguria.it/
Introduction to ASA • One of the most widely used drugs of the 20th century1
• Taken by millions of patients worldwide for the treatment and prevention of CVD, and is the most widely tested antiplatelet drug1
• Has been (and is still) used for stroke prevention in AF1,2
ASA = acetylsalicylic acid; CVD = cardiovascular disease; VKA = vitamin K antagonist 1. Dai Y, Ge J. Thrombosis 2012;2012:245037; 2. Camm AJ et al. Eur Heart J 2012;33:2719–47 2
Traditionally considered a safe, but less effective, alternative to VKAs when anticoagulation is contraindicated, or for use in patients at low risk
of stroke1,2
However, this is not consistent with the latest treatment guidelines2
ASA for stroke prevention in AFAIAC and AHA/ACC Guidelines
ASA for stroke prevention in AFESC Guidelines
ASA??
Camm AJ et al. Eur Heart J
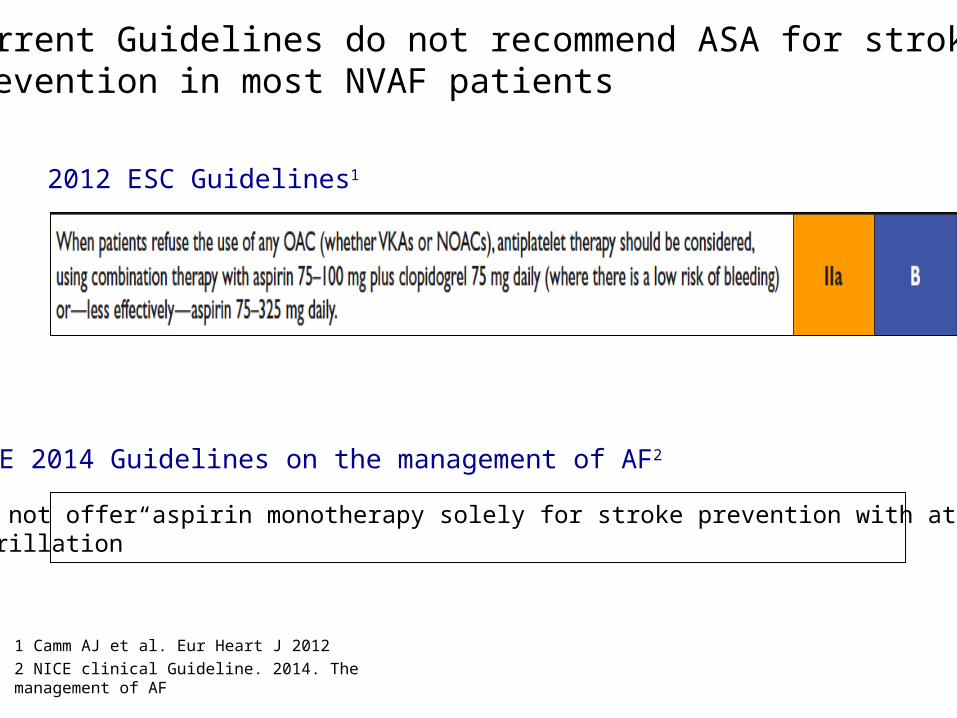
NICE 2014 Guidelines on the management of AF2
“Do not offer aspirin monotherapy solely for stroke prevention with atrial fibrillation”
2012 ESC Guidelines1
Current Guidelines do not recommend ASA for stroke prevention in most NVAF patients
1 Camm AJ et al. Eur Heart J 20122 NICE clinical Guideline. 2014. The management of AF
Limited efficacy of ASA in reducing stroke risk in patients with AF
Random effects model; error bars = 95% CI; *P>0.2 for homogeneity; †Relative risk reduction (RRR) for all strokes (ischaemic and haemorrhagic); for ischaemic stroke only, RRR was 21% (95% CI: −1 to 38%)ASA = acetylsalicylic acid; QOD = every other dayHart RG et al. Ann Intern Med 2007;146:857–67
RRR (%)†100 –10050 0 –50
AFASAK (1989)
SPAF (1991)
EAFT (1993)
ESPS II (1997)
ASA better Placebo better
LASAF (1997)125 mg/d
125 mg QOD
UK-TIA (1999)300 mg/d
1200 mg/d
JAS (2006)T
All trialsRRR: 19%*
(95% CI: –1 to 35%)
Only the SPAF trial showed a benefit of ASA over placebo for reducing stroke risk
ASA was less effective than VKA in historical trials in AF
Random effects model; error bars = 95% CI; *P>0.2 for homogeneity; †Relative risk reduction (RRR) for all strokes (ischaemic and haemorrhagic); ASA = acetylsalicylic acidHart RG et al. Ann Intern Med 2007;146:857–67 9
RRR (%)†
100 –10050 0 –50
AFASAK I (1990)
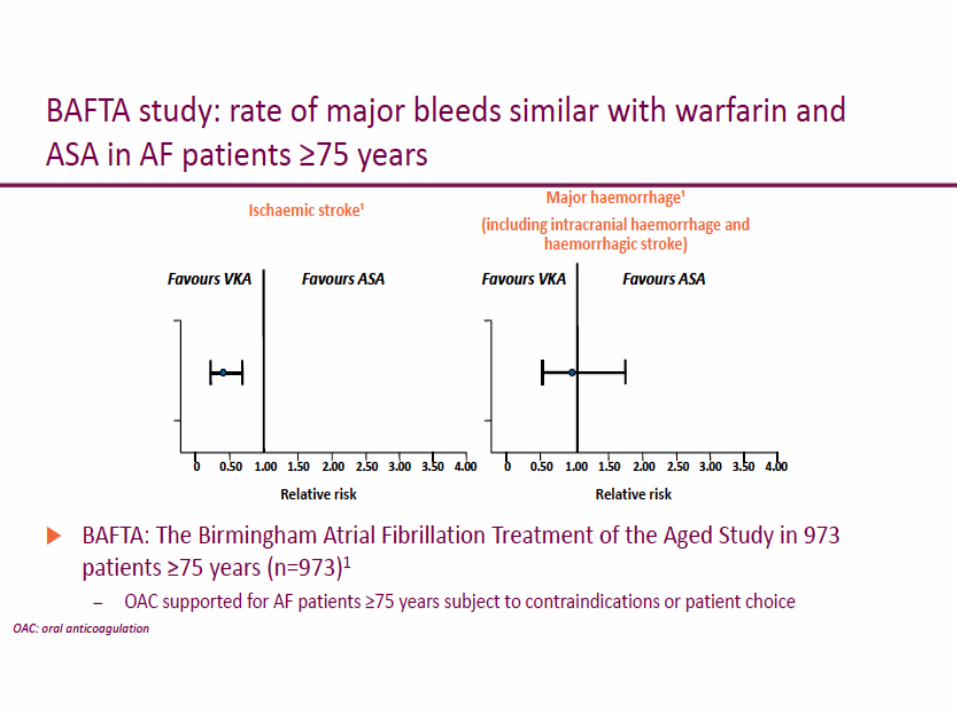
BAFTA (2007)
EAFT (1993)
PATAF (1999)
Warfarin better ASA better
Chinese ATAFS (2006)
SPAF II (1994)Age 75 yrsAge >75 yrs
All trials (4620 pt) RRR: 38%*(95% CI: 18-52%)
Risk of major and intracranial bleeding not significantly different between ASA and OAC
*Modified HAS-BLED score used in this study: 1 point each for systolic blood pressure >160 mmHg, renal dysfunction, liver dysfunction, stroke, bleeding, age >65 years, drugs affecting bleeding or alcohol abuse (maximum score = 7); score 0 –2 indicates low bleeding risk, ≥3 indicates high bleeding risk; ASA = acetylsalicylic acidFriberg L et al. Eur Hear J 2012:33:1500-10; Pisters R et al. Chest 2010;138:1093–100
ASA for stroke prevention in AFAIAC and AHA/ACC Guidelines
2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation
JACC - DOI: 10.1016/j.jacc.2014.03.022
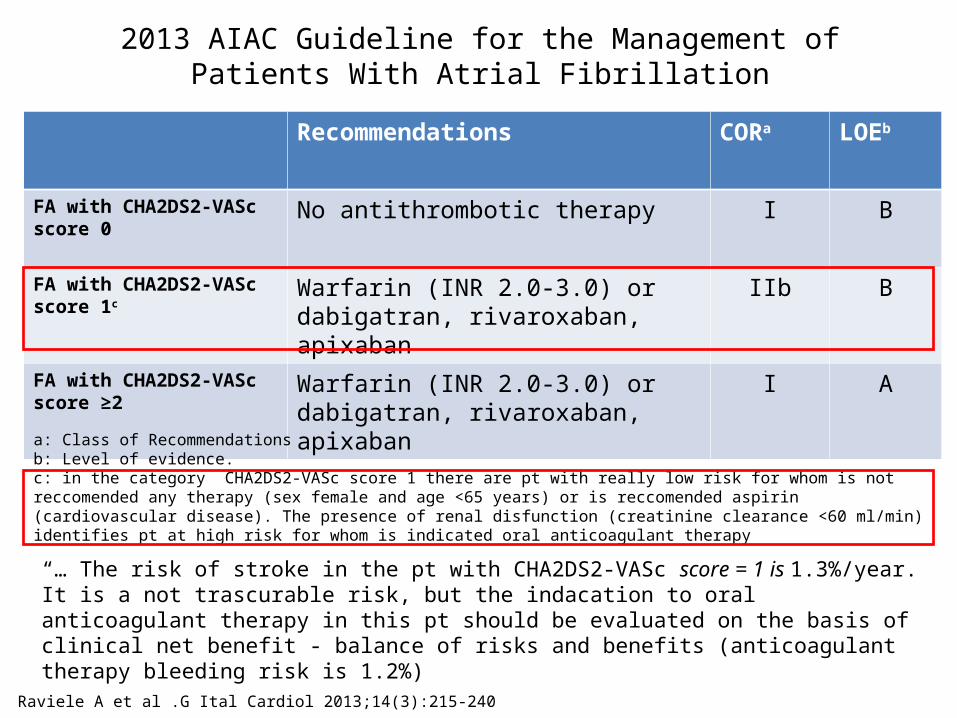
Raviele A et al .G Ital Cardiol 2013;14(3):215-240
Recommendations CORa LOEb
FA with CHA2DS2-VASc score 0 No antithrombotic therapy I B
FA with CHA2DS2-VASc score 1c Warfarin (INR 2.0-3.0) or dabigatran, rivaroxaban, apixaban
IIb B
FA with CHA2DS2-VASc score ≥2
Warfarin (INR 2.0-3.0) or dabigatran, rivaroxaban, apixaban
I A
a: Class of Recommendationsb: Level of evidence.c: in the category CHA2DS2-VASc score 1 there are pt with really low risk for whom is not reccomended any therapy (sex female and age <65 years) or is reccomended aspirin (cardiovascular disease). The presence of renal disfunction (creatinine clearance <60 ml/min) identifies pt at high risk for whom is indicated oral anticoagulant therapy
“… The risk of stroke in the pt with CHA2DS2-VASc score = 1 is 1.3%/year. It is a not trascurable risk, but the indacation to oral anticoagulant therapy in this pt should be evaluated on the basis of clinical net benefit - balance of risks and benefits (anticoagulant therapy bleeding risk is 1.2%)
2013 AIAC Guideline for the Management of Patients With Atrial Fibrillation
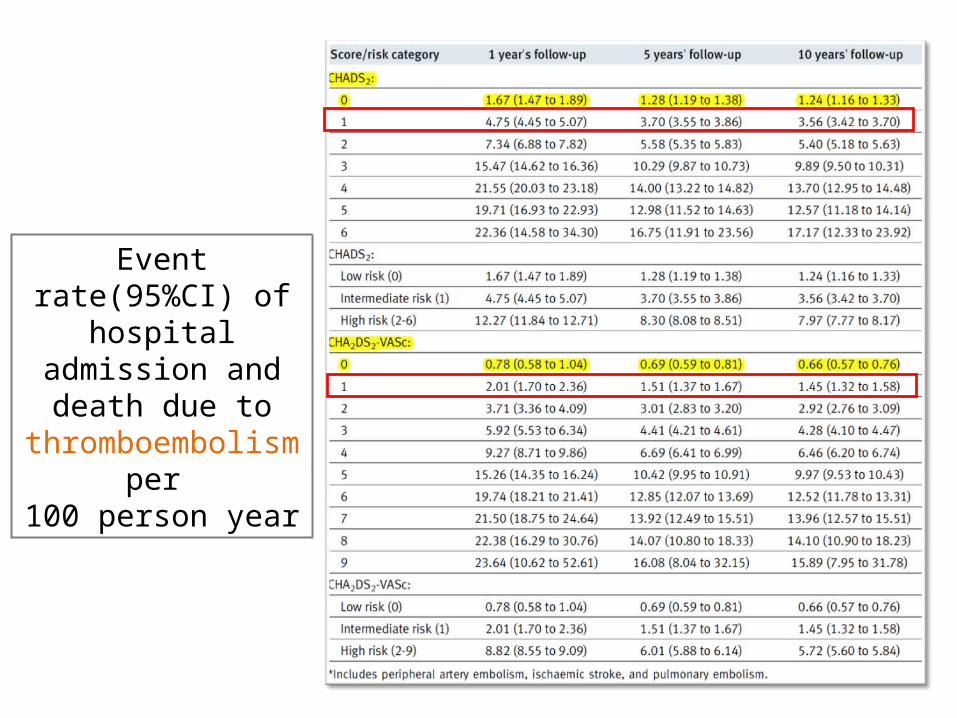
Event rate(95%CI) of hospital
admission and death due to
thromboembolism per
100 person year
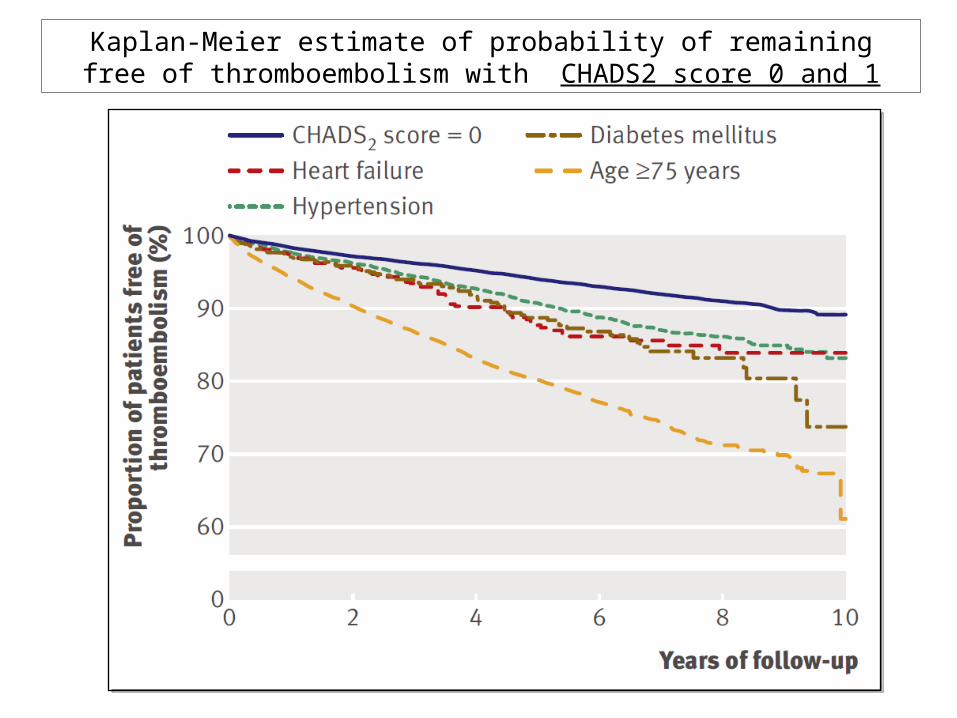
Kaplan-Meier estimate of probability of remaining free of thromboembolism with CHADS2 score 0 and 1
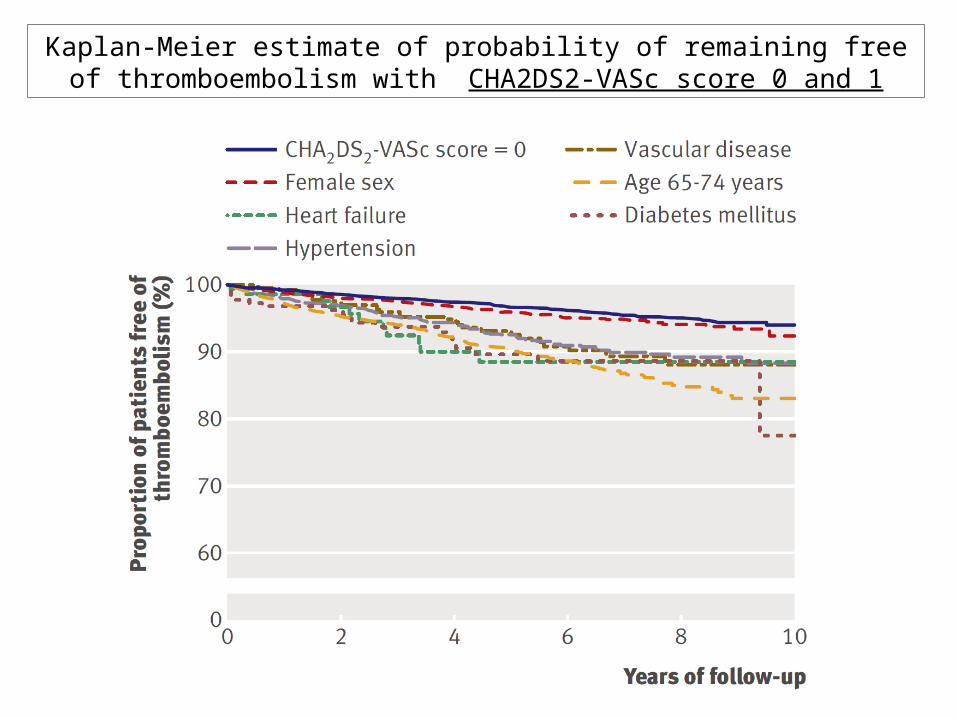
Kaplan-Meier estimate of probability of remaining free of thromboembolism with CHA2DS2-VASc score 0 and 1
ASA Conclusions
➢Antiplatelet therapy should be considered only when patients refuse any OAC, or cannot tolerate OAC for reasons unrelated to bleeding, or in a specific subgroups of pt with CHADVASC 1
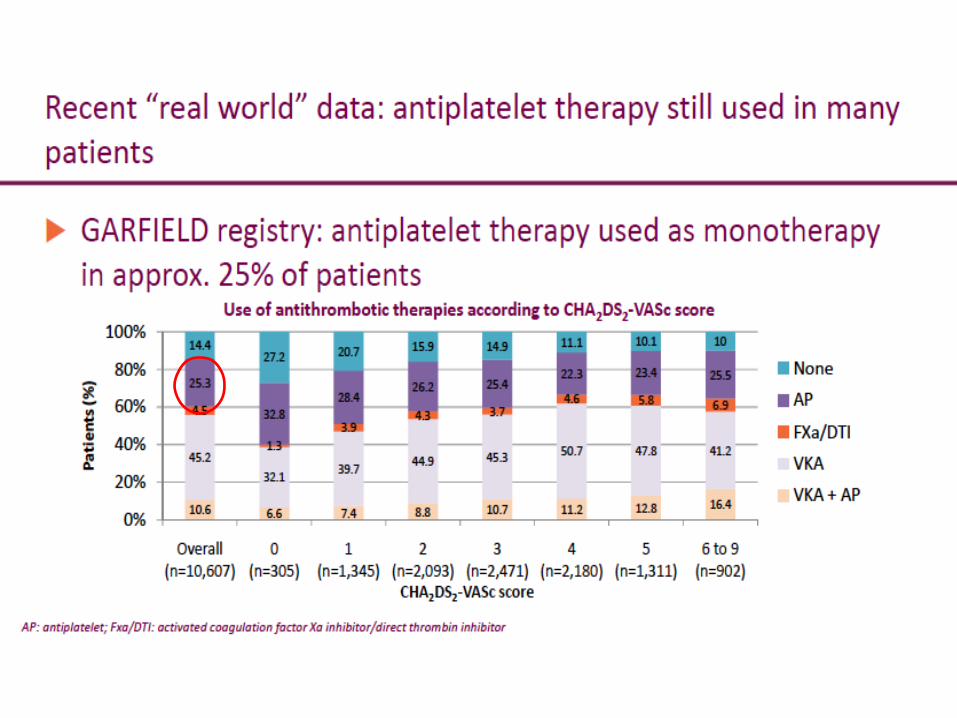
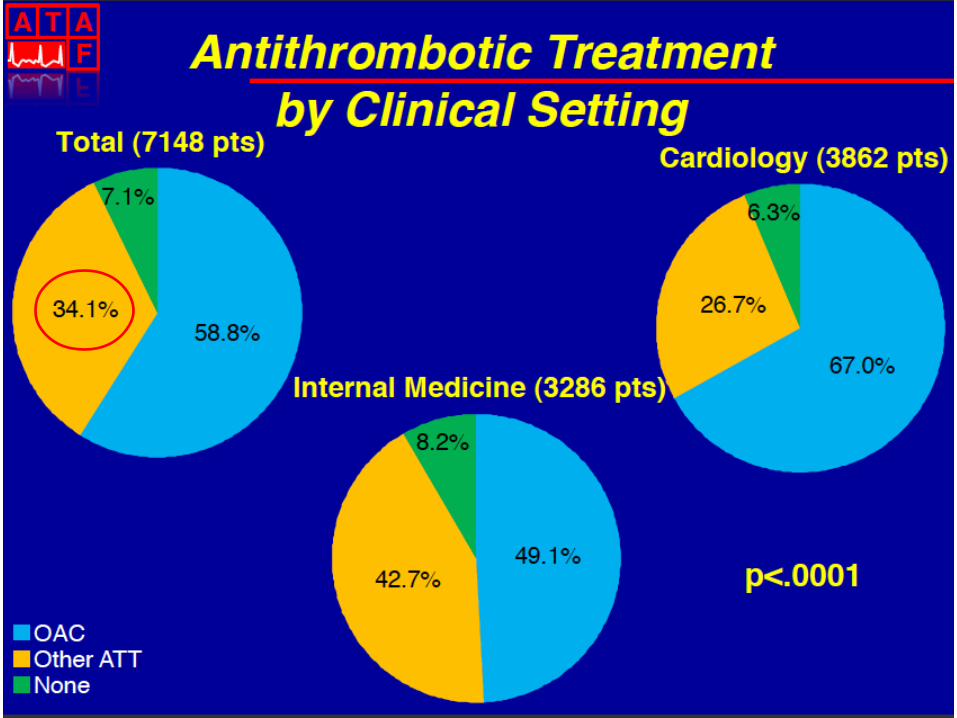
➢In the real world, antiplatelet therapy is still commonly prescribed for stroke prevention in AF
➢Compared with ASA, NOAs (apixaban) significantly reduced the relative risk of stroke or systemic embolism by 55% while the risk of major bleeding was not significantly increased
➢The evidence demonstrated that oral anticoagulation should be the preferred option in NVAF patients at risk of stroke