Application of a Constrained ExternalFixator Frame for Treatment of a FixedEquinus Contracture
Robert W. Mendicino, DPM, FACFAS,1 Lara J. Murphy, DPM,2 Michael P. Maskill, DPM,3
Alan R. Catanzariti, DPM, FACFAS,4 and Harry Penny, DPM5
Ankle equinus can result from congenital, traumatic, neurological, and pathological etiologies. Correctivemethods have been described in the literature using a combination of soft tissue releases or osseousprocedures with reported complications. We present a case report of a patient with a post-traumaticfixed equinus deformity of 28° at maximum dorsiflexion, treated successfully through gradual correctionusing a modified constrained external fixator. The patient maintained a rectus foot and was able toperform all daily activities at the final follow-up. Fixed equinus deformities can be difficult to manage.Gradual correction with an external fixator is a reasonable treatment option. Level of Clinical Evidence:4 (The Journal of Foot & Ankle Surgery 47(5):468–475, 2008)
Equinus contractures develop from a number of differentetiologies including congenital, traumatic, neurological, andpathological (1–3). Acquired equinus contractures, whichevolve over a period of time, can advance into a fixeddeformity because of soft tissue contraction and bony ad-aptation. Scar contracture and neurological damage are of-ten seen in post-traumatic cases. Acquired equinus can beencountered as a single deformity, however it is often ac-companied with other forefoot and/or hindfoot misalign-ments including pes equinovarus (4).
Osteotomies and acute soft tissue releases have beendescribed for the treatment of complex foot and ankledeformities (5, 6). Complications relating to neurovascularstructures and skin may develop with acute reduction ofsevere deformities (7). The Ilizarov apparatus was designedand modified to correct deformities in all 3 orthogonal
Address correspondence to: Robert W. Mendicino, DPM, FACFAS,Vice Chair, Department of Surgery, Chief of Foot and Ankle Surgery, TheWestern Pennsylvania Hospital, 4800 Friendship Avenue North TowerFirst Floor, Pittsburgh, PA 15224. E-mail: [email protected].
1Attending Surgeon and Vice Chair of Department of Surgery, TheWestern Pennsylvania Hospital, Pittsburgh, PA.
2Second Year Resident, The Western Pennsylvania Hospital, Pitts-burgh, PA.
3Third Year Resident, The Western Pennsylvania Hospital, Pittsburgh,PA.
4Attending Surgeon and Director of Residency Training Program, TheWestern Pennsylvania Hospital, Pittsburgh, PA.
planes using gradual correction (1, 4, 6–8). Herzenberg andPaley (6) described the use of the Ilizarov application forsoft tissue deformity correction. Acquired cases of contrac-tion after skeletal maturity could be realigned without theneed for an osteotomy (6).
An external fixator can be used as a constrained or uncon-strained hinge system. A constrained hinge system uses thecenter of rotation of a joint as the location for the placement ofthe hinges. The external fixator is then manipulated or adjusteddaily to rotate around the joint axis in a calculated manner.This is usually used for large joints with identifiable centers ofrotation. Unconstrained systems use a distraction technique torotate around the center of the joint. This technique uses thenatural rotation of the joint and is usually used with smallerjoints or deformities with multiple joint axes.
Melvin and Dahners (5) described the use of a dynamictension system with an unconstrained Ilizarov frame for cor-rection of equinus with various etiologies. The constrainedhinged method has been described to have a high level oftechnical difficulty for the patient and physician and hasproven to be unreliable in obtaining accurate correction aroundthe ankle joint axis (5). This manuscript describes a patientwith a traumatically induced fixed equinus deformity withresidual peroneal motor and sensory neuropathy. A detaileddescription on the application and use of a modified con-strained rotating hinged frame is presented. Challenges in-cluded a retained prograded tibial rod from previous surgeryfor a tibial shaft fracture as well as postsurgical scar formation.The modification of the frame for creation of an appropriateankle joint axis and motor are discussed. The use of adjunctiveprocedures including peroneal and tarsal tunnel release along
A 35-year-old female patient was referred to the Foot and
FIGURE 1 (A, B, C) Pre-operative photographs of a post-traumplantarflexed position.
Ankle Institute of Western Pennsylvania in October 2005 with
VOLUME 4
complaints of a painful fixed equinus contracture of her leftlower extremity. The patient had been involved in a severemotor vehicle accident in February 2005 resulting in a lacer-
fixed equinus deformity with a maximum dorsiflexion of 28° in a
atic
ated spleen, liver, and kidney along with a left-sided pelvic
7, NUMBER 5, SEPTEMBER/OCTOBER 2008 469
the
fracture, tibial fracture, and peroneal and tibial nerve injury.The patient had a residual fixed equinus deformity with max-imum dorsiflexion of 28° in a plantarflexed position and aretained tibial intramedullary rod from her previous surgery(Figures 1 and 2). Pre-operative evaluation and work-up con-sisted of magnetic resonance imaging (MRI), noninvasive
FIGURE 2 (A, B, C) Pre-operative radiographs demonstrating
lower extremity studies, scintigraphy to rule out underlying
470 THE JOURNAL OF FOOT & ANKLE SURGERY
osteomyelitis, and electrodiagnostic studies to evaluate theextent of nerve damage. All of the pre-operative tests wereunremarkable except the electrodiagnostic studies, which dem-onstrated left common peroneal motor neuropathy and leftsuperficial peroneal and sural nerve sensory neuropathy. Therewas no evidence of acute denervation, myopathy, or myositis
fixed equinus deformity and retained tibial intramedullary rod.
of bilateral lower extremity musculature.
The patient underwent surgical intervention, which in-cluded application of a multiplanar circular external fixator,gastrocnemius recession, and common peroneal nerve andtarsal tunnel release. Significant fibrosis and scarring werenoted surrounding the common peroneal and posterior tibialnerves. Minimal improvement of the equinus contracturewas noted with the gastrocnemius lengthening.
An external fixator was then applied. Initially, 2 tibial ringswere placed circumferentially around the lower extremity withthe tibia located centrally. Because of the residual tibial in-tramedullary rod, the 2 proximal olive wires and the distal wirewere angulated to pass through the cortex of the tibia ratherthan centrally through the bone to avoid contacting the in-tramedullary rod. This was performed under fluoroscopy.These wires were placed within 45° of the frontal plane in astandard crossing fashion. The distal ring was stabilized with 1olive wire running medial to lateral and a 5-mm half pin.Because of the length of the retained tibial rod, an extensioncube was placed from the tibial ring distally to allow placementof the half pin in the tibia distal to the rod (Figure 3). The olivewires were then tensioned and alignment of all componentswas noted to be at right angles to the tibia. This was confirmedusing image intensification.
A footplate was then mounted parallel to the axis of thefoot. Counter-posted olive wires were placed throughthe metatarsal shafts and midfoot to maintain the integrity ofthe forefoot joints. An olive wire and smooth wire were thencrossed through the calcaneus. The ankle joint axis was then
FIGURE 3 Due to a retained tibial rod from previous surgery, 2tibial rings were mounted using a modified technique of wire place-ment and application of a half pin required placement distal to theretained hardware.
evaluated for placement of the universal hinges. The ankle
VOLUME 4
joint axis was determined by using Inman’s axis, which runsthrough the distal aspects of the medial and lateral malleoli.This axis runs from anterior-medial-dorsal to posterior-lateral-plantar. This axis can be verified with the use offluoroscopy and a Kirschner wire. A wire is run through thetalus, across the distal aspects of the malleoli, creating theankle joint axis. The ankle joint is then manipulated throughits range of motion under image intensification. The pinshould not rotate or translate. The connecting rods with thealigned hinges were then placed medial and lateral connect-ing the tibial component to the foot plate (Figure 4). Theankle joint was then distracted to prevent crushing of thetalus during the correction of the equinus. A cut olive wirewas placed percutaneously across the joint to prevent dis-location of the talonavicular joint.
Two long rods were connected from the proximal tibialring to the anterior foot plate to be used as the motor for theequinus correction. Two 3-hole posts were stacked ob-liquely to allow for a flat surface area with complete appo-sition of screw components on the proximal ring (Figure 5,A). This also provided proper alignment of the anterior rodsand prevented improper angulation and therefore residualangular deformities following correction. Kirschner wireswere placed across all the digits and the metatarsophalan-geal joints to prevent digital contractures and maintainstabilization of the forefoot. The patient was admitted for 24hours for pain management. Physical therapy was consultedfor gait training. The patient was discharged home on 14
FIGURE 4 The footplate was mounted parallel to the foot andattached to the distal tibial ring via a constrained hinge system thatused Inman’s axis for accurate placement.
days of low molecular weight heparin for deep vein throm-
7, NUMBER 5, SEPTEMBER/OCTOBER 2008 471
bophlebitis prophylaxis and instructed to remain completelynon–weight bearing on the affected extremity over thecourse of the treatment.
FIGURE 5 (A) Two long rods connected at the footplate andproximal tibial ring were used as the motor for gradual correction.Two 3-hole posts were placed in an oblique manner on the tibial ringto provide a flat surface area for connection of the rods and properangulation for the correction. (B) A focused view shows the conicalwashers used to maintain the angulated position of the nuts toprevent the bending of the rods when locking after corrections arecompleted.
Shortening of 4 mm of the anterior rods was performed in
472 THE JOURNAL OF FOOT & ANKLE SURGERY
the office, providing the initial correction of the equinus de-formity 1 week status post-surgery. Gradual correction wasinitiated 2 weeks status post-surgery. The gradual correctionrate was determined by the patient’s pain tolerance, the pres-ence of posterior tibial nerve compression symptoms, andtissue elasticity. The patient was instructed to shorten theanterior rods by turning the nuts one-half turn 4 times per day.The use of conical washers aided in maintaining the angulatedposition of the nuts to prevent bending of the rods whenlocking after corrections are completed (Figure 5, B). Radio-graphs were taken showing 8° of plantarflexion remaining at 3weeks status post-surgery. All joints were evaluated andshowed proper alignment without any signs of dislocation. Thedecision was made to increase the rate of correction by amultiple of 8 (double the correction). The patient was advisedto continue with this rate of correction until she was unable totolerate the pain or until her next visit. This was continued untilher seventh post-operative week at which time radiographsdemonstrated a measured overcorrection of 18° dorsiflexion(Figure 6). This equaled a total correction of 46°. Overcorrec-tion was maintained for an additional 7 weeks. Generally, forcontracture deformities, the external fixator is maintained for atotal of twice the amount of time it takes to correct the defor-mity or at least a minimum of 6 additional weeks (7, 9).
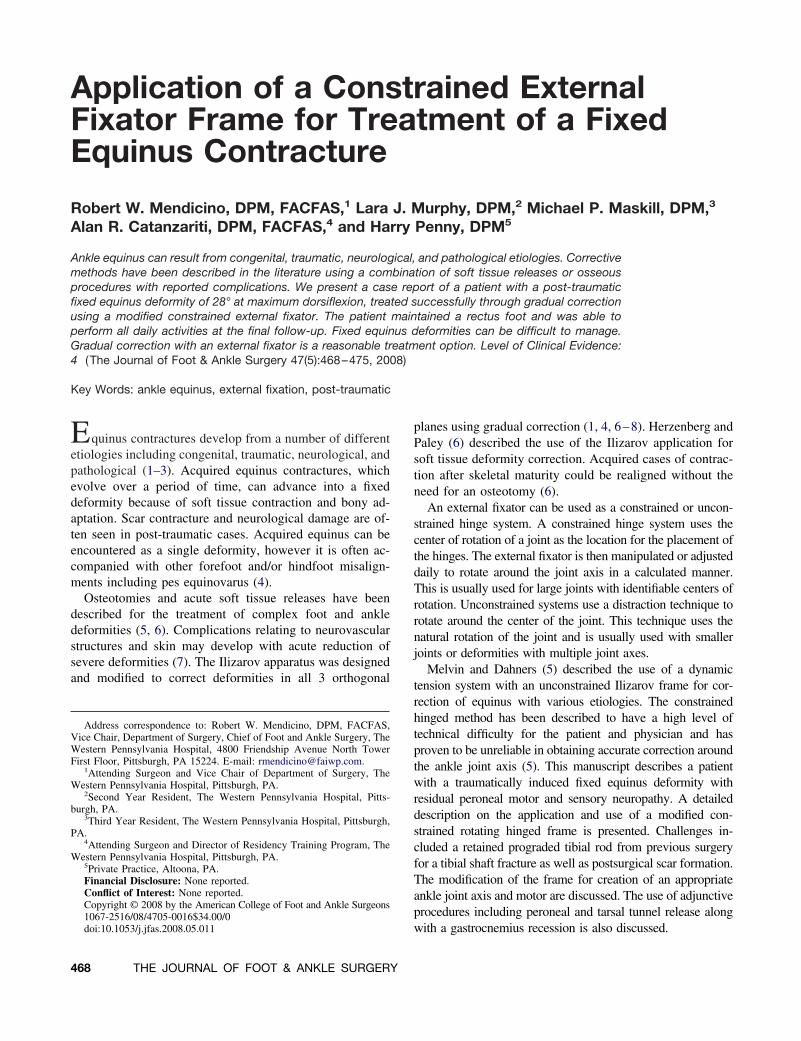
The patient had the fixator removed 4 months status postapplication. The patient was placed in a removable cast andinstructed to be partial weight bearing with crutches. Thepatient was then placed in a molded anterior clamshellankle-foot orthoses with a plantarflexory stop. The patientexperienced minimal pain and on physical exam demon-strated passive dorsiflexion of 10°. The patient was thenprescribed aggressive physical therapy including range ofmotion exercises for the left lower extremity as well asposterior muscle group stretching and strengthening. Thepatient had a rectus foot and demonstrated return of functionof the anterior muscle group at the 1-year follow-up exam-ination (Figure 7). The patient was released to participate innormal daily activities and advised to remain in the anklefoot orthoses at night for the next 6 months.
Discussion
Post-traumatic lower extremity deformities are challeng-ing cases. The hinged constrained fixator method has beendescribed as a surgical tool for correction of complex de-formities in gradual settings. However, there has been nospecific recommendation for its use in treating traumaticuniplanar ankle deformities. Tsuchiya et al (7) in 2003evaluated the difference in correction between 2 differenthinged groups for equinus contracture correction. Theyfound little clinical difference between these 2 groups withmean correction of 32.9 � 12.9° in the natural hinge group
and 36.1 � 10.5° in the rotating hinge group. Tsuchiya et al
FIGURE 6 (A and B) Photographs of the patient 7 weeks post-operative demonstrates a measured 18° of dorsiflexion. (C and D)Radiographic evaluation 7 weeks post-operatively demonstrates correction of the deformity with proper alignment of all lower extremity
joints.
VOLUME 47, NUMBER 5, SEPTEMBER/OCTOBER 2008 473
FIGURE 7 (A, B, C) Photographs of the patient at final follow-up shows the foot in a rectus position with no residual equinus.
474 THE JOURNAL OF FOOT & ANKLE SURGERY
(7) did note differences however in complications includingdigital flexor contractures with the rotating hinged groupand anterior subluxation of the talus in the natural hingedgroup. These complications were avoided in this case byfixating the talonavicular, metatarsophalangeal, and digitaljoints.
Other reported complications include tarsal tunnel syn-drome, valgus drift, pin site infections, and recurrence ofdeformity (1, 4, 5, 8, 9). Lamm et al (10) in 2007 found thatacute corrections of greater than 10° may benefit fromprophylactic tarsal tunnel release. They also felt that gradualcorrection is much less likely to cause nerve entrapment andrecommended prophylactic decompression of the posteriortibial nerve. Initiation of a secondary surgical decompres-sion or a decrease or cessation in the rate of correctionshould be considered if posterior tibial nerve compressivesymptoms were to occur (10).
Complications also arising from improper placement orinadequate support of the external fixator can occur. Huang(11) noted the importance of distraction and proper hingeplacement of the external fixator to prevent crushing of thearticular surfaces. We used intraoperative pinning and con-sistent radiographic follow-up to monitor and prevent crush-ing of the talus and dislocation of the tarsal joints. Kocaogluet al (4) in 2002 recommended prevention of toe contrac-tures through rubber slings or Kirschner wire fixation ofthe distal and proximal interphalangeal joints as well as themetatarsophalangeal joints. Paley (12) in 1993 described theuse of a Kirschner wire across the phalangeal bases withoutincorporating the metatarsals for prevention of contractureswith the use of the Ilizarov device. We found operativepinning of all 5 digits across the metatarsophalangeal jointssatisfactory in maintaining appropriate alignment of theforefoot without residual contractures or complicationswithin the metatarsophalangeal joints.
Recurrence of any soft tissue deformity is a concern anda well-documented complication. Huang (11) in 1996 de-scribed the use of the Ilizarov frame for correction of kneeand ankle joint contractures with a recurrence rate of 11 outof 26 contractures within 3 years. Gradual correction was
used to obtain an overcorrected position of 18° dorsiflexion
VOLUME 4
in our case study. This correction was maintained for acalculated additional amount of time to decrease the chanceof recurrence. Long-term bracing of 6 to 12 months andphysical therapy are also helpful after removal of fixation tomaintain soft tissue correction.
Treatment of post-traumatic fixed equinus can be difficultwith some potential complications including recurrence. Wehave provided a description of the use of a constrainedhinged external fixator in conjunction with a comprehensivetreatment plan in order to obtain a successful outcome.
References
1. Carmichael K, Maxwell S, Calhoun J. Recurrence rates of burn con-tracture ankle equinus and other foot deformities in children treatedwith Ilizarov fixation. J Pediatr Orthop 254:523–528, 2005.
2. Hahn S, Park H, Park H, Kang H, Cho J. Treatment of severe equinusdeformity associated with extensive scarring of the leg. Clin OrthopRelat Res 393:250–257, 2001.
3. Hsu K, Kuo K, Hsu R. Correction of foot deformity by the Ilizarovmethod in a patient with segawa disease. Clin Orthop Relat Res314:199–202, 1995.
4. Kocaoglu M, Eralp L, Atalar A, Bilen F. Correction of complex footdeformities using the Ilizarov external fixator. J Foot Ankle Surg411:30–39, 2002.
5. Melvin J, Dahners L. A technique for correction of equinus contractureusing a wire fixator and elastic tension. J Orthop Trauma 202:138–142, 2006.
6. Herzenberg J, Paley D. Ilizarov applications in foot and ankle surgery.Advances in Orthopaedic Surgery 163:162–174, 1992.
7. Tsuchiya H, Sakurakichi K, Uehara K, Yamashiro T, Tomita K.Gradual closed correction of equinus contracture using the ilizarovapparatus. J Orthop Sci 8:802–806, 2003.
8. Elomrani N, Kasis A, Tis J, Saleh M. Outcome after foot and ankledeformity correction using circular external fixation. Foot Ankle Int2612:1027–1032, 2005.
9. Calhoun JH, Evans EB, Herndon DN. Techniques for the managementof burn contractures with the ilizarov fixator. Clin Orthop Rel Res280:117–124, 1992.
10. Lamm B, Paley D, Testani M, Herzenberg J. Tarsal tunnel decom-pression in leg lengthening and deformity correction of the foot andankle. J Foot Ankle Surg 463:201–206, 2007.
11. Huang S. Soft tissue contractures of the knee or ankle treated by theilizarov technique. Acta Orthop Scand 675:443–449, 1996.
12. Paley D. The correction of complex foot deformities using Ilizarov’s