he role of endoscopy in the management of intraventric-ular and skull base tumors is well established.1-8 Its role
n the management of intra-axial tumors is almost unknownn the literature and appears to be poorly defined.9,10 A pre-equisite for endoscopy is the presence of a cavity, either fluidr air filled, through which to view the target. Therefore, it isnsurprising that the use of endoscopic assistance for theesection of intra-axial tumors has thus far not been em-raced.The importance of radical resection for the optimal man-
gement of both low- and high-grade gliomas is incontest-ble.11-16 Indeed, the only contention appears to be how rad-cal a resection is needed. If the ability to look around cornersnd to improve visualization would improve the degree ofesection of gliomas, endoscopy may have a role in the man-gement of these tumors. This article examines the use of thendoscope for improving the degree of intra-axial tumor re-ection and concomitantly for decreasing the morbidity andength of surgery.
ndicationsndoscopy may be helpful whenever the ability to achieveomplete removal of an intrinsic tumor is questionable. Therade or histological subtype of the tumor is inconsequential.he endoscope enhances illumination and magnification,hich is sometimes enough to differentiate between normal
issue and residual tumor. However, the real benefit of en-
Center for Minimally Invasive Neurosurgery, Prince of Wales Private Hos-pital, Randwick NSW, Australia.
Division of Neurological Surgery, Barrow Neurological Institute, St. Jo-seph’s Hospital and Medical Center, Phoenix, AZ.
ddress reprint requests to Peter Nakaji, MD, c/o Neuroscience Publica-tions, Barrow Neurological Institute, 350 W. Thomas Road; Phoenix, AZ
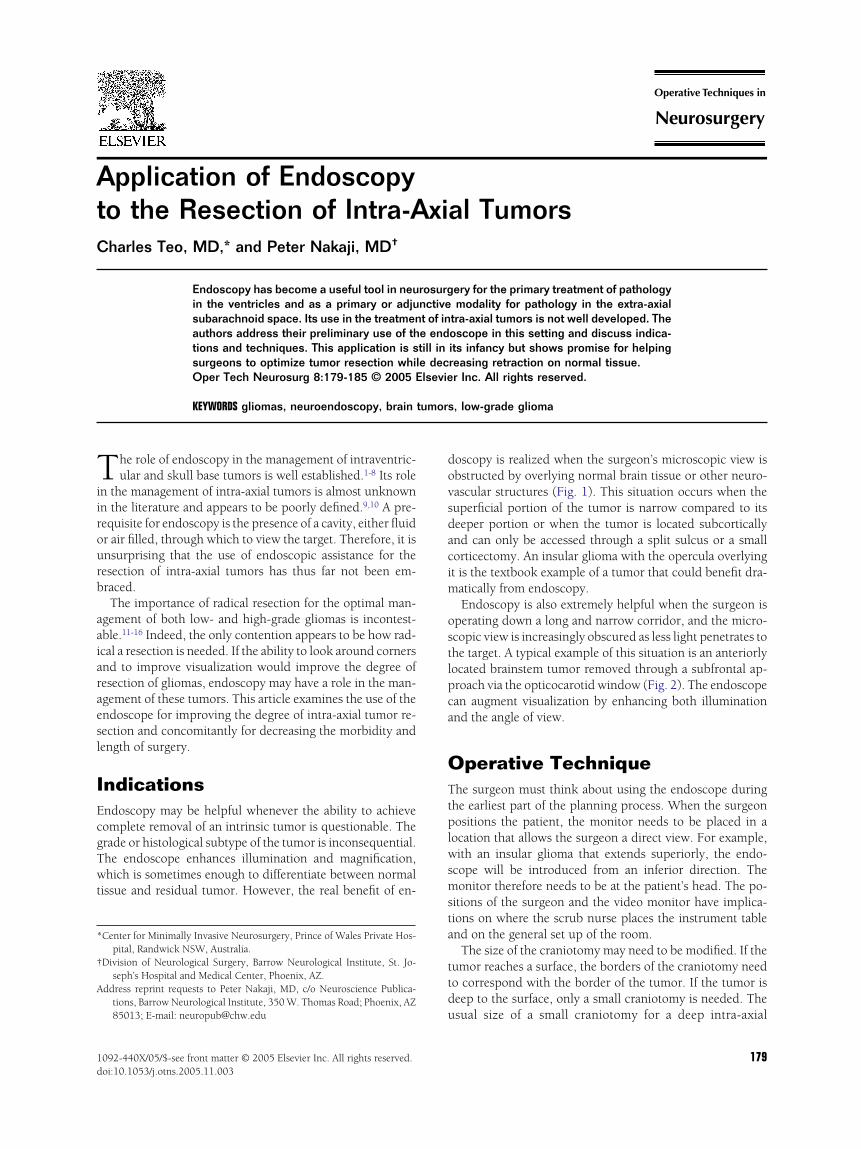
oscopy is realized when the surgeon’s microscopic view isbstructed by overlying normal brain tissue or other neuro-ascular structures (Fig. 1). This situation occurs when theuperficial portion of the tumor is narrow compared to itseeper portion or when the tumor is located subcorticallynd can only be accessed through a split sulcus or a smallorticectomy. An insular glioma with the opercula overlyingt is the textbook example of a tumor that could benefit dra-
atically from endoscopy.Endoscopy is also extremely helpful when the surgeon is
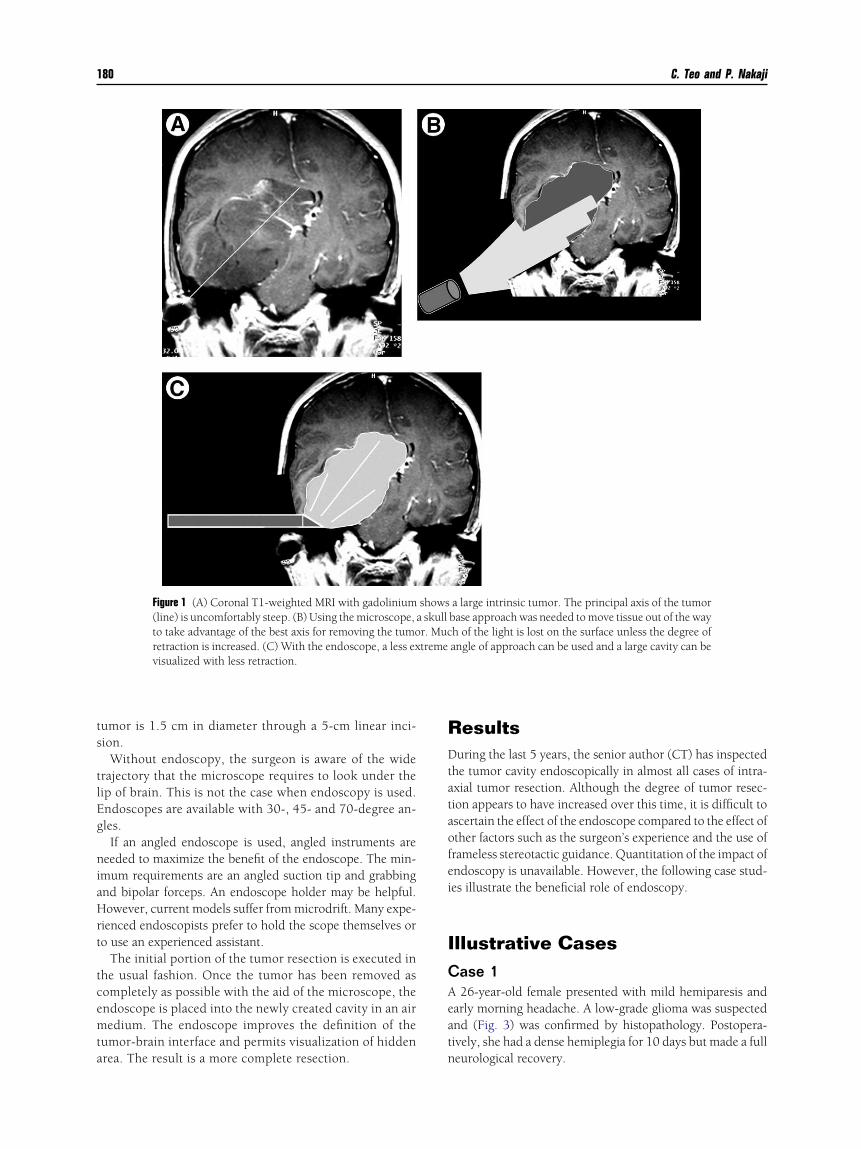
perating down a long and narrow corridor, and the micro-copic view is increasingly obscured as less light penetrates tohe target. A typical example of this situation is an anteriorlyocated brainstem tumor removed through a subfrontal ap-roach via the opticocarotid window (Fig. 2). The endoscopean augment visualization by enhancing both illuminationnd the angle of view.
perative Techniquehe surgeon must think about using the endoscope during
he earliest part of the planning process. When the surgeonositions the patient, the monitor needs to be placed in a
ocation that allows the surgeon a direct view. For example,ith an insular glioma that extends superiorly, the endo-
cope will be introduced from an inferior direction. Theonitor therefore needs to be at the patient’s head. The po-
itions of the surgeon and the video monitor have implica-ions on where the scrub nurse places the instrument tablend on the general set up of the room.
The size of the craniotomy may need to be modified. If theumor reaches a surface, the borders of the craniotomy needo correspond with the border of the tumor. If the tumor iseep to the surface, only a small craniotomy is needed. The
sual size of a small craniotomy for a deep intra-axial
179
ts
tlEg
niaHrt
tcemta
RDtataofei
ICAeatn
180 C. Teo and P. Nakaji
umor is 1.5 cm in diameter through a 5-cm linear inci-ion.
Without endoscopy, the surgeon is aware of the widerajectory that the microscope requires to look under theip of brain. This is not the case when endoscopy is used.ndoscopes are available with 30-, 45- and 70-degree an-les.If an angled endoscope is used, angled instruments are
eeded to maximize the benefit of the endoscope. The min-mum requirements are an angled suction tip and grabbingnd bipolar forceps. An endoscope holder may be helpful.owever, current models suffer from microdrift. Many expe-
ienced endoscopists prefer to hold the scope themselves oro use an experienced assistant.
The initial portion of the tumor resection is executed inhe usual fashion. Once the tumor has been removed asompletely as possible with the aid of the microscope, thendoscope is placed into the newly created cavity in an airedium. The endoscope improves the definition of the
umor-brain interface and permits visualization of hiddenrea. The result is a more complete resection.
Figure 1 (A) Coronal T1-weighted MRI with gadolinium(line) is uncomfortably steep. (B) Using the microscope,to take advantage of the best axis for removing the tumoretraction is increased. (C) With the endoscope, a less exvisualized with less retraction.
esultsuring the last 5 years, the senior author (CT) has inspected
he tumor cavity endoscopically in almost all cases of intra-xial tumor resection. Although the degree of tumor resec-ion appears to have increased over this time, it is difficult toscertain the effect of the endoscope compared to the effect ofther factors such as the surgeon’s experience and the use oframeless stereotactic guidance. Quantitation of the impact ofndoscopy is unavailable. However, the following case stud-es illustrate the beneficial role of endoscopy.
llustrative Casesase 126-year-old female presented with mild hemiparesis and
arly morning headache. A low-grade glioma was suspectednd (Fig. 3) was confirmed by histopathology. Postopera-ively, she had a dense hemiplegia for 10 days but made a fulleurological recovery.
a large intrinsic tumor. The principal axis of the tumorbase approach was needed to move tissue out of the wayh of the light is lost on the surface unless the degree ofangle of approach can be used and a large cavity can be
showsa skullr. Muctreme
Endoscopy to the resection of intra-axial tumors 181
Figure 2 (A) Axial T1-weighted MRI with gadolinium shows a tumor extending off the lateral upper midbrain. (B) Aview from the microscope down to the tumor is long and progressively darker as the depth increases. (C) Under theendoscope, additional tumor is visible on the wall of the cavity of the tumor (arrow). (D) With an angled suction tip,
the residual tumor is removed. (Continued on next page) (Color version of figure is available online.)
182 C. Teo and P. Nakaji
Figure 2 (Cont’d) (E) A postoperative axial T1-weighted MRI with gadolinium shows asatisfactory resection.
Figure 3 This intra-axial tumor presented to the surface and had a superficial component that was as wide as the deeperpart. In this situation endoscopy was unnecessary. (B) Postoperative MRI confirmed that excellent resection was
achieved without the endoscope.
Endoscopy to the resection of intra-axial tumors 183
Figure 4 Preoperative coronal T1-weighted MRI shows a large hy-pointense tumor involving the frontal and temporal lobes. The mid-dle cerebral artery and its branches were intimately involved withthe tumor. (B) Postoperative MRI shows incomplete resection. Theendoscope was not used in this case. In retrospect, using the endo-scope to look higher would likely have led to a more completeresection. (C) After surgery, the patient did well and had no neuro-logical deficits.
184 C. Teo and P. Nakaji
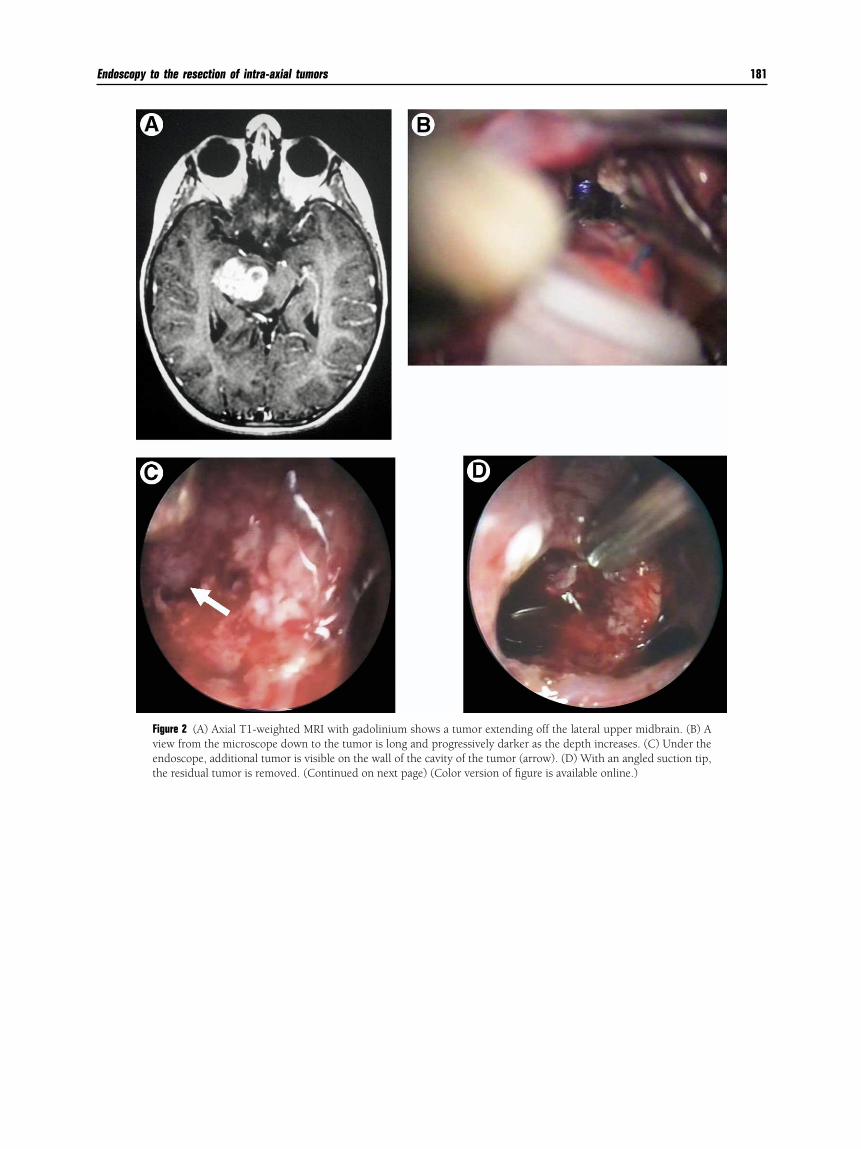
Figure 5 (A) T2-weighted MRIs show an insular glioma that extends to the temporal pole and involves the right frontallobe. (B) Postoperative MRIs show a radical but incomplete resection. The operation was performed through a keyholecraniotomy and a limited opening in the Sylvian fissure. The endoscope was instrumental in achieving this degree ofresection. (C) The patient had an uncomplicated postoperative course without neurological deficit. The pathology,
however, recurred as an anaplastic astrocytoma.
CAt(h
CAw5fsaa
eap
CAMTnm
CNeiagtcpm
R
1
1
1
1
1
1
1
FasaSdt
Endoscopy to the resection of intra-axial tumors 185
ase 232-year-old male with seizures and headache was thought
o have a low-grade glioma on magnetic resonance imagingMRI) (Fig. 4). His postoperative course was uneventful, andistopathology confirmed a grade 2 astrocytoma.
ase 338-year-old female who initially presented with seizures
as diagnosed as having a probable low-grade glioma (Fig.). She had been told the tumor was inoperable. She wasollowed for 18 months before her seizures worsened, anderial MRI showed clear progression. She was right-handednd had no speech or motor deficits. The patient underwent
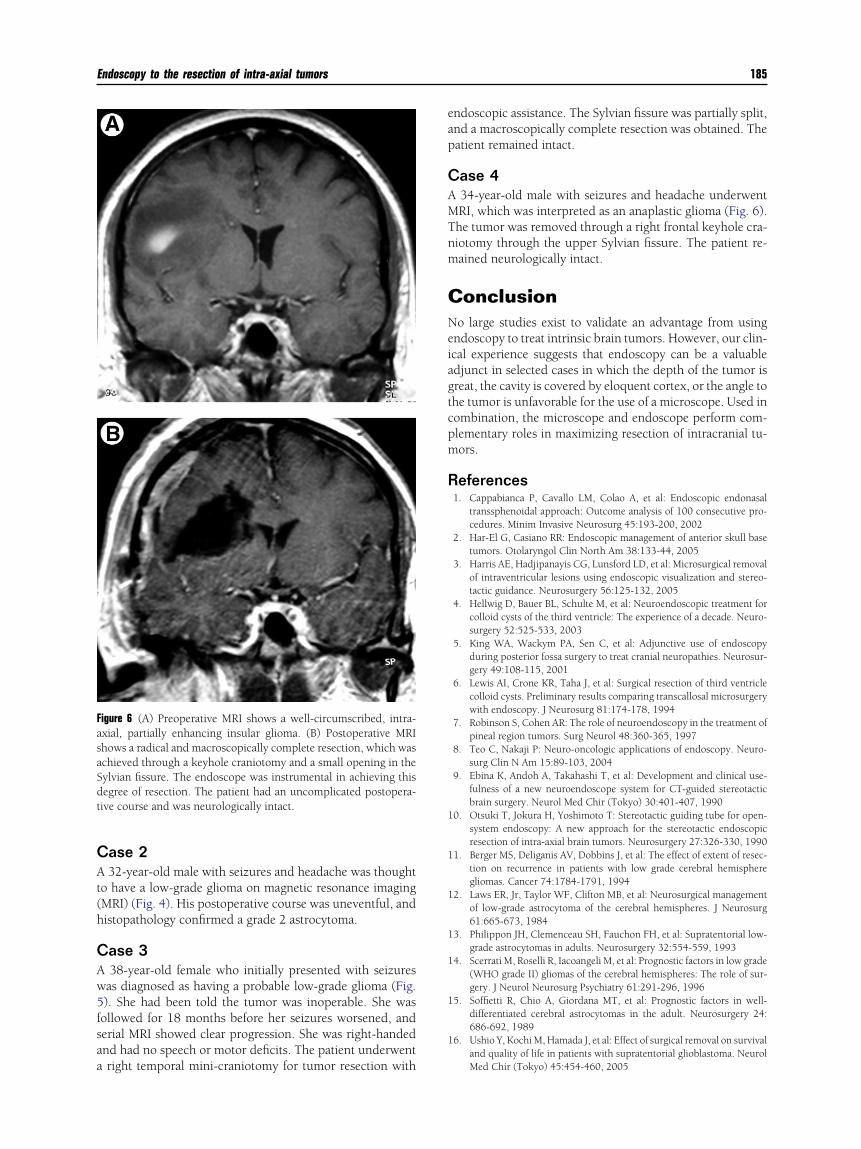
igure 6 (A) Preoperative MRI shows a well-circumscribed, intra-xial, partially enhancing insular glioma. (B) Postoperative MRIhows a radical and macroscopically complete resection, which waschieved through a keyhole craniotomy and a small opening in theylvian fissure. The endoscope was instrumental in achieving thisegree of resection. The patient had an uncomplicated postopera-ive course and was neurologically intact.
right temporal mini-craniotomy for tumor resection with
ndoscopic assistance. The Sylvian fissure was partially split,nd a macroscopically complete resection was obtained. Theatient remained intact.
ase 434-year-old male with seizures and headache underwentRI, which was interpreted as an anaplastic glioma (Fig. 6).he tumor was removed through a right frontal keyhole cra-iotomy through the upper Sylvian fissure. The patient re-ained neurologically intact.
onclusiono large studies exist to validate an advantage from using
ndoscopy to treat intrinsic brain tumors. However, our clin-cal experience suggests that endoscopy can be a valuabledjunct in selected cases in which the depth of the tumor isreat, the cavity is covered by eloquent cortex, or the angle tohe tumor is unfavorable for the use of a microscope. Used inombination, the microscope and endoscope perform com-lementary roles in maximizing resection of intracranial tu-ors.
eferences1. Cappabianca P, Cavallo LM, Colao A, et al: Endoscopic endonasal
2. Har-El G, Casiano RR: Endoscopic management of anterior skull basetumors. Otolaryngol Clin North Am 38:133-44, 2005
3. Harris AE, Hadjipanayis CG, Lunsford LD, et al: Microsurgical removalof intraventricular lesions using endoscopic visualization and stereo-tactic guidance. Neurosurgery 56:125-132, 2005
4. Hellwig D, Bauer BL, Schulte M, et al: Neuroendoscopic treatment forcolloid cysts of the third ventricle: The experience of a decade. Neuro-surgery 52:525-533, 2003
5. King WA, Wackym PA, Sen C, et al: Adjunctive use of endoscopyduring posterior fossa surgery to treat cranial neuropathies. Neurosur-gery 49:108-115, 2001
6. Lewis AI, Crone KR, Taha J, et al: Surgical resection of third ventriclecolloid cysts. Preliminary results comparing transcallosal microsurgerywith endoscopy. J Neurosurg 81:174-178, 1994
7. Robinson S, Cohen AR: The role of neuroendoscopy in the treatment ofpineal region tumors. Surg Neurol 48:360-365, 1997
8. Teo C, Nakaji P: Neuro-oncologic applications of endoscopy. Neuro-surg Clin N Am 15:89-103, 2004
9. Ebina K, Andoh A, Takahashi T, et al: Development and clinical use-fulness of a new neuroendoscope system for CT-guided stereotacticbrain surgery. Neurol Med Chir (Tokyo) 30:401-407, 1990
0. Otsuki T, Jokura H, Yoshimoto T: Stereotactic guiding tube for open-system endoscopy: A new approach for the stereotactic endoscopicresection of intra-axial brain tumors. Neurosurgery 27:326-330, 1990
1. Berger MS, Deliganis AV, Dobbins J, et al: The effect of extent of resec-tion on recurrence in patients with low grade cerebral hemispheregliomas. Cancer 74:1784-1791, 1994
2. Laws ER, Jr, Taylor WF, Clifton MB, et al: Neurosurgical managementof low-grade astrocytoma of the cerebral hemispheres. J Neurosurg61:665-673, 1984
3. Philippon JH, Clemenceau SH, Fauchon FH, et al: Supratentorial low-grade astrocytomas in adults. Neurosurgery 32:554-559, 1993
4. Scerrati M, Roselli R, Iacoangeli M, et al: Prognostic factors in low grade(WHO grade II) gliomas of the cerebral hemispheres: The role of sur-gery. J Neurol Neurosurg Psychiatry 61:291-296, 1996
5. Soffietti R, Chio A, Giordana MT, et al: Prognostic factors in well-differentiated cerebral astrocytomas in the adult. Neurosurgery 24:686-692, 1989
6. Ushio Y, Kochi M, Hamada J, et al: Effect of surgical removal on survivaland quality of life in patients with supratentorial glioblastoma. Neurol