SCCD: N.G. AFRICAN DEVELOPMENT FUND Language: English Original: French APPRAISAL REPORT HEALTH SYSYTEM DEVELOPMENT SUPPORT PROJECT (PADS) REPUBLIC OF BENIN DEPARTMENT OF SOCIAL DEVELOPMENT OCSD CENTRAL AND WEST REGIONS MARCH 2005
Transcript
SCCD: N.G.
AFRICAN DEVELOPMENT FUND Language: English
Original: French
APPRAISAL REPORT
HEALTH SYSYTEM DEVELOPMENT SUPPORT PROJECT (PADS)
REPUBLIC OF BENIN
DEPARTMENT OF SOCIAL DEVELOPMENT OCSD CENTRAL AND WEST REGIONS MARCH 2005
TABLE OF CONTENTS
PROJECT INFORMATION SHET, CURRENCY EQUIVALENTS, WEIGHTS AND MEAURES, LIST OF TABLES, LIST OF ANNEXES, LIST OF ACRONYMS AND ABBREVIATIONS, SOCIO-ECONOMIC INDICATORS, EXECUTIVE SUMMARY, LOGICAL FRAMEWORK OF PROJECT i-xi 1. ORIGIN AND HISTORY OF PROJECT.......................................................................1 2. THE SECTOR ................................................................................................................1 2.1. Health Situation...............................................................................................................1 2.2. Government Policy and Sector Action Program.............................................................2 2.3. Institutional Framework and Sector Organization ..........................................................4 2.4. Human Resources of the Sector ......................................................................................5 2.5. Financing of the Sector ...................................................................................................6 2.6. Interventions of Donors ..................................................................................................7 2.7. Health Sector Constraints................................................................................................8 3. PROJECT COMPONENTS............................................................................................9 3.1. Utilization of Health Services .........................................................................................9 3.2. Quality of Health Services in the Health Zone .............................................................11 3.3. Communicable Diseases ...............................................................................................13 3.4. Reproductive Health Services.......................................................................................14 4. THE PROJECT.............................................................................................................14 4.1. Design and Rationale of Project....................................................................................14 4.2. Project Areas and Beneficiaries ....................................................................................16 4.3. Strategic Context...........................................................................................................17 4.4. Project Objectives .........................................................................................................18 4.5. Project Description........................................................................................................18 4.6. Impact on the Environment...........................................................................................23 4.7. Project Costs… .............................................................................................................24 4.8. Financing Sources and Expenditure Schedule ..............................................................25 5. PROJECT IMPLEMENTATION.................................................................................26 5.1. Executing Agency.........................................................................................................26 5.2. Institutional Arrangements............................................................................................27 5.3. Implementation and Supervision Schedule...................................................................28 5.4. Procurement Arrangements...........................................................................................29 5.5. Disbursement Arrangements.........................................................................................33 5.6. Monitoring and Evaluation ...........................................................................................33 5.7. Financial and Audit Reports .........................................................................................34 5.8. Coordination of Assistance ...........................................................................................35
6. SUSTAINABILITY AND RISKS OF THE PROJECT...............................................35 6.1. Recurrent Expenditure ..................................................................................................35 6.2. Sustainability of Project ................................................................................................36 6.3. Main Risks and Mitigative Measures............................................................................37 7. PROJECT BENEFITS ..................................................................................................37 7.1. Economic Impact ..........................................................................................................38 7.2. Impact on Women.........................................................................................................38 7.3. Social Impact….............................................................................................................39 8. CONCLUSIONS AND RECOMMENDATIONS .......................................................39 8.1. Conclusions ...............................................................................................................40 8.2. Recommendations and Loan Conditions ......................................................................43 This report was written by Mr. I. Sanogo, Health Analyst (OCAR.2), Mrs. S. Foryt, Financial Analyst (OCAR.2) and Mrs. H. Mrabet, Architect (OCAR.2), following an appraisal mission to Benin from 10 to 23 December 2004. Questions on this project should be referred to Mr. N. SAFIR, Acting Director OCAR, Extension 2141 or Mr. J. E. PORGO, Division Manager, OCAR.2, Extension 2173.
The information given hereunder is intended to provide guidance to prospective suppliers, contractors and all persons interested in the procurement of goods and services for the projects approved by the Boards of Directors of the Bank Group. More detailed information and guidance may be obtained from the Executing Agency of the Borrower.
1. COUNTRY : Republic of Benin
2. NAME OF PROJECT : Health System Development Support Project (Health III)
3. PROJECT AREA :
The project covers the entire national territory through assistance given to the Ministry of Public Health (MPH) at the central level. Its activities, however, focus on the departments of Donga and Zou to improve access to quality health services, promote maternal/child health and enhance disease control; and the department of Borgou to extend the facilities of the DGH in Parakou.
4. BORROWER : Republic of Benin
5. EXECUTING AGENCY : Project Management Unit (PMU) within the MPH
6. PROJECT DESCRIPTION :
The sector goal of the project is to contribute to the attainment of health-related Millennium Development Goals in Benin: reduction of infant mortality, improvement of maternal health, and control of STI/HIV/AIDs, malaria and other diseases. Its specific objectives are: (i) to improve the supply and quality of health services; and (ii) encourage greater use of health services. The three components of the project are: (i) improvement of access to quality health services; (ii) promotion of maternal and child health and disease control; and (iii) project management.
7. COST OF PROJECT
Foreign exchange : UA 18.64 million
Local currency : UA 05.83 million
Total : UA 24.47 million
8. PROPOSED FINANCING
ADF loan : UA 22.00 million
Government : UA 02.47 million
9. PROBABLE APPROVAL DATE : April 2005
10. PROBABLE START-UP DATE AND
DURATION OF PROJECT : January 2006 - 5 years
ii
11. PROCUREMENT OF GOODS AND SERVICES:
The procurement of works, goods and services shall be done in accordance with the relevant ADB Group rules of procedure as follows: Works: (UA 6 million) International competitive bidding through the delegated project owner for the construction of hospitals and zonal offices and extension work on DGH-Borgou in Parakou; Goods: (UA 10.91 million) International competitive bidding for the procurement of: (i) biomedical furniture and equipment, (ii) treated mosquito nets, (iii) Coartem and rapid diagnosis tests for malaria, (iv) ambulances, (v) aerial communication network systems, and (vi) instructional material for EONC and IMCI as well as kits for midwives; National competitive bidding for procurement of: (i) hospital furniture; (ii) office automation, IT and audiovisual equipment; (iii) sanitation equipment, and (iv) vehicles. The maximum amount per contract is UA 200 000. Direct negotiation with: (i) CAME for the procurement of drugs, consumables and reagents; and (ii) the Department of Pharmacy and Diagnostic Exploration in the Ministry of Public Health for medicinal plant gardens. Services (UA 5.16 million) Limited shopping for experts to provide the following services: (i) supervision as delegated project owner; (ii) conduct of architectural and technical studies, supervision and control of construction work on zonal hospitals and offices, and extension work on DGH-Borgou; (iii) training in mutual fund management; (iv) IEC activities; (v) studies and diagnosis through monitoring, evaluation and supervision (maintenance, health zone functionality and human resource development); (vi) training and guidance during retraining and training workshops organized by the MPH and MFSWS; (vii) technical assistance for the PMU; and (viii) project assessment. Direct negotiation with the IRSP, vocational training schools (INMES and ENIIAB) as well as medical and maintenance schools in the sub-region for medical, paramedical, administrative and maintenance training courses. The Department of Hygiene and Basic Sanitation (DHBS) in the Ministry of Public Health shall plan hygiene and sanitation activities. Meanwhile, the Disease Control Department (DCD) shall plan priority disease control activities and the Department of Pharmacy and Exploratory Diagnosis will train traditional healers. Direct agreements signed with these MPH departments shall be forwarded to the Bank for review. Operations (UA 1.71 million): Limited shopping to recruit staff for the project management unit. The shortlists are prepared after calls for bidders at the national level;
iii
Agreement with the MPH and MEHTP for monitoring and evaluation of project activities; The functioning of the project (office supplies, fuel, etc.) shall be ensured through: (i) shopping for suppliers for contracts below UA 200,000; and (ii) competitive bidding for contracts above UA 20,000. Miscellaneous (UA 0.69 million): Limited shopping for NGOs to set up mutual funds and manage contributions paid on behalf of poor members by the project.
12. CONSULTANCY SERVICES REQUIRED:
Consultancy services shall be needed to conduct studies, provide training and carry out annual audits of the project.
iv
CURRENCY EQUIVALENTS
(December 2004 )
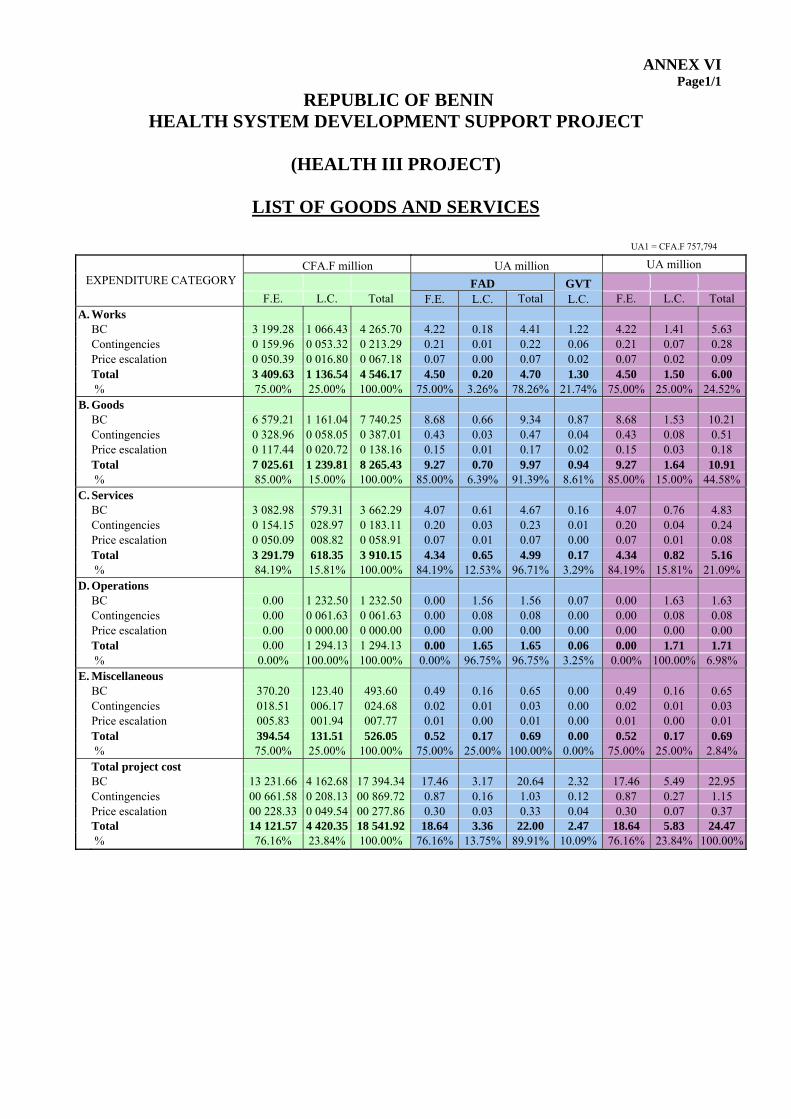
National currency = CFA Franc UA 1 = CFA.F 757.794 UA 1 = Є1.194 UA 1 = US$ 1.478
UNITS OF MEASURE
Metric system
FISCAL YEAR 1st January – 31st December
LIST OF TABLES Page
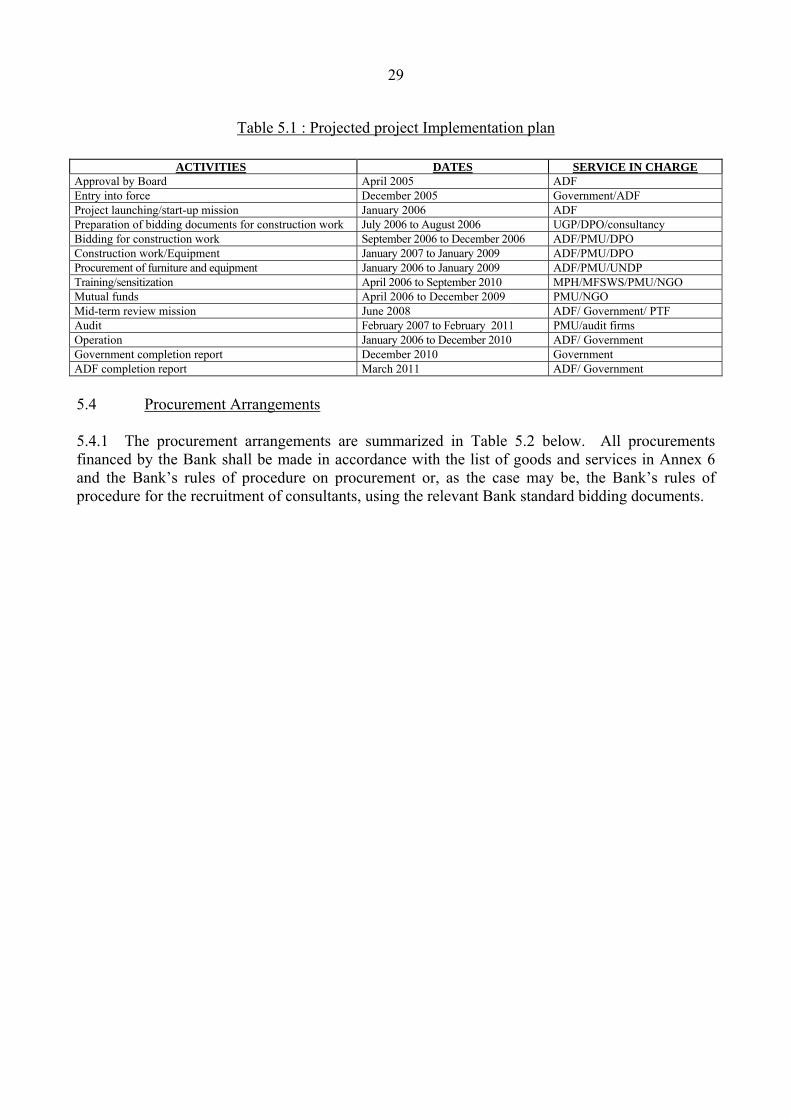
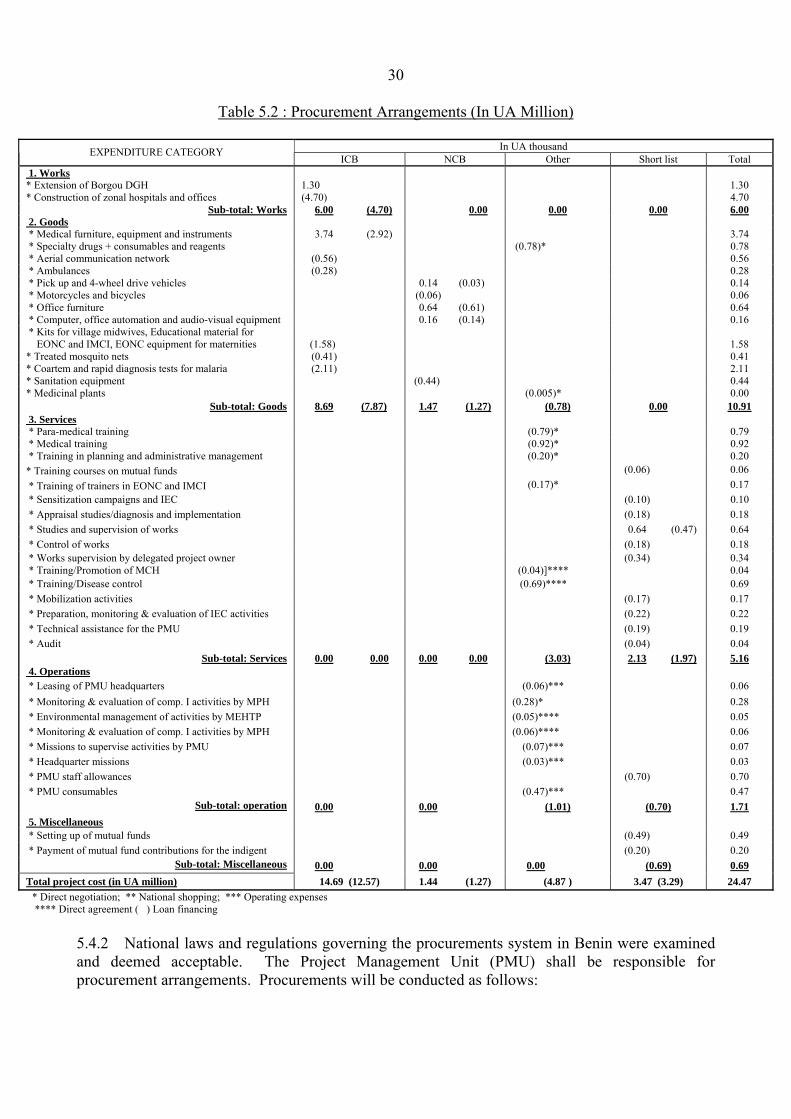
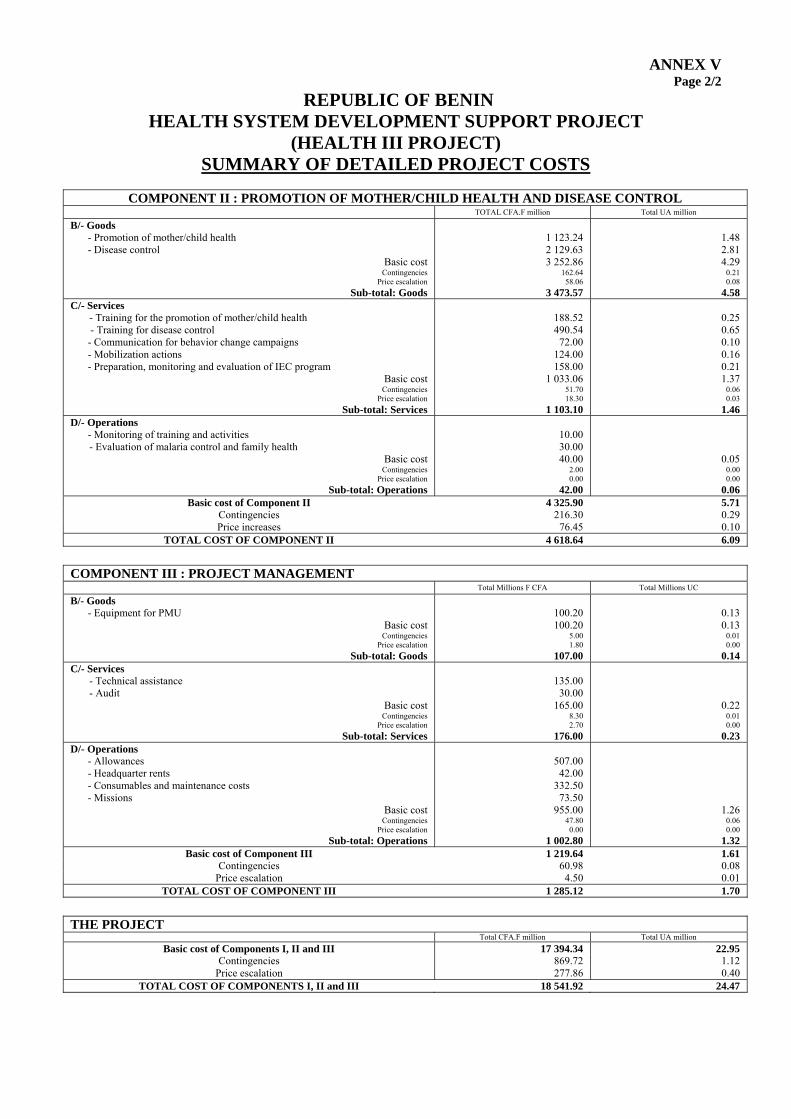
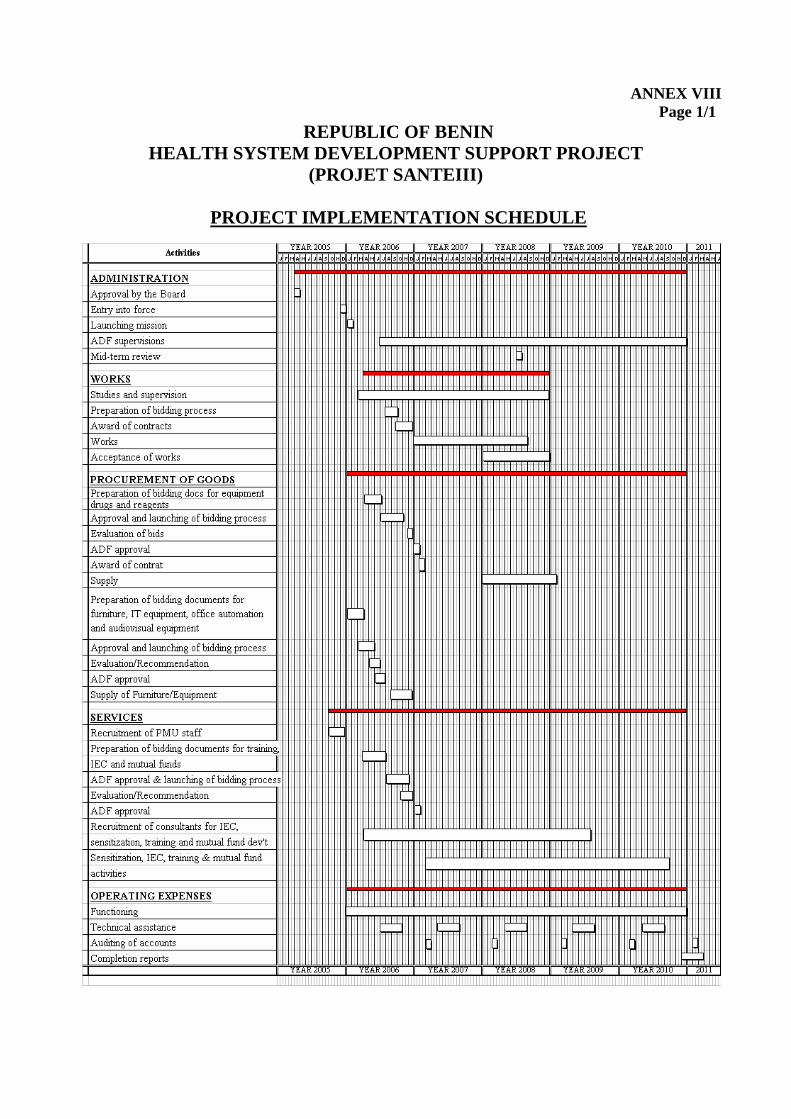
Table 2.1: Distribution of Private Health Care Institutions By Department 5 Table 2.2: Health Budget Trends in Relation to the State Budget 6 Table 4.1: Project Costs by Component 24 Table 4.2: Project Costs by Expenditure Category 24 Table 4.3: Project Costs by Financing Source 25 Table 4.4: Project Costs by Component and By Financing Source 25 Table 4.5: Project Costs by Expenditure Category and Financing Source 25 Table 4.6: Expenditure Schedule by Component 26 Table 4.7: Expenditure Schedule by Expenditure Category 26 Table 4.8: Expenditure Schedule by Financing Source 26 Table 5.1: Estimated Project Implementation Plan 29 Table 5.2: Procurement Arrangements 30
LIST OF ANNEXES Number of pages
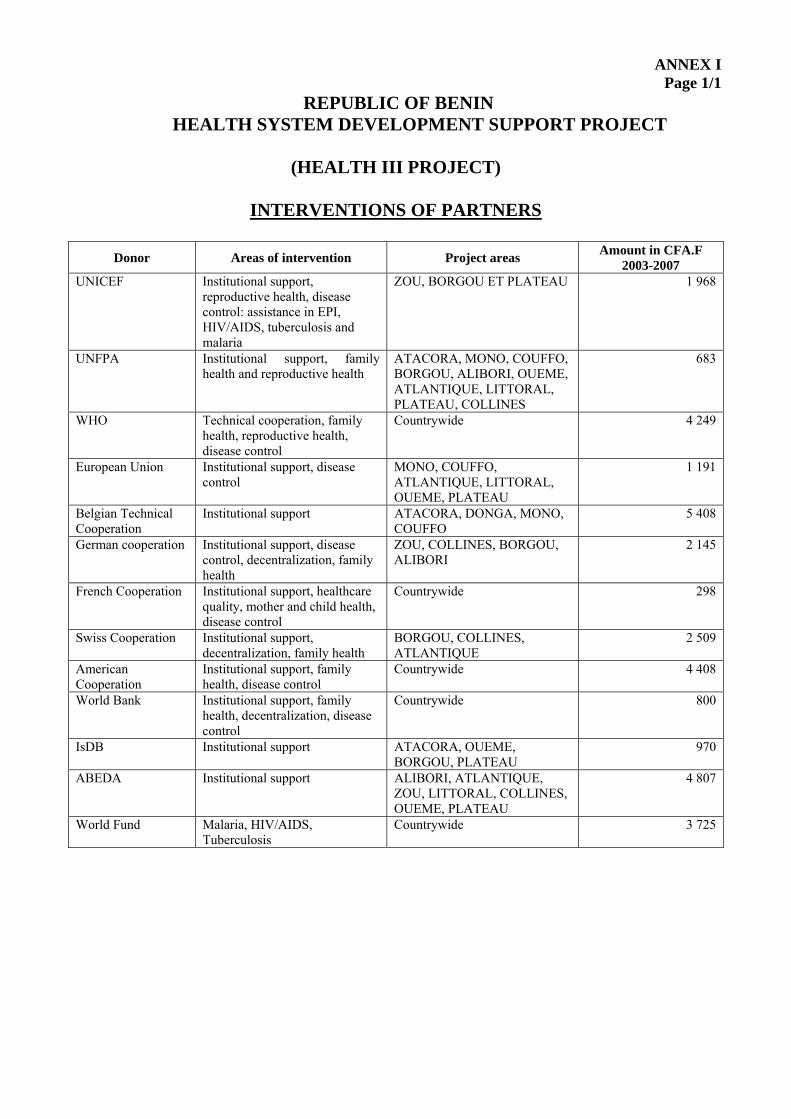
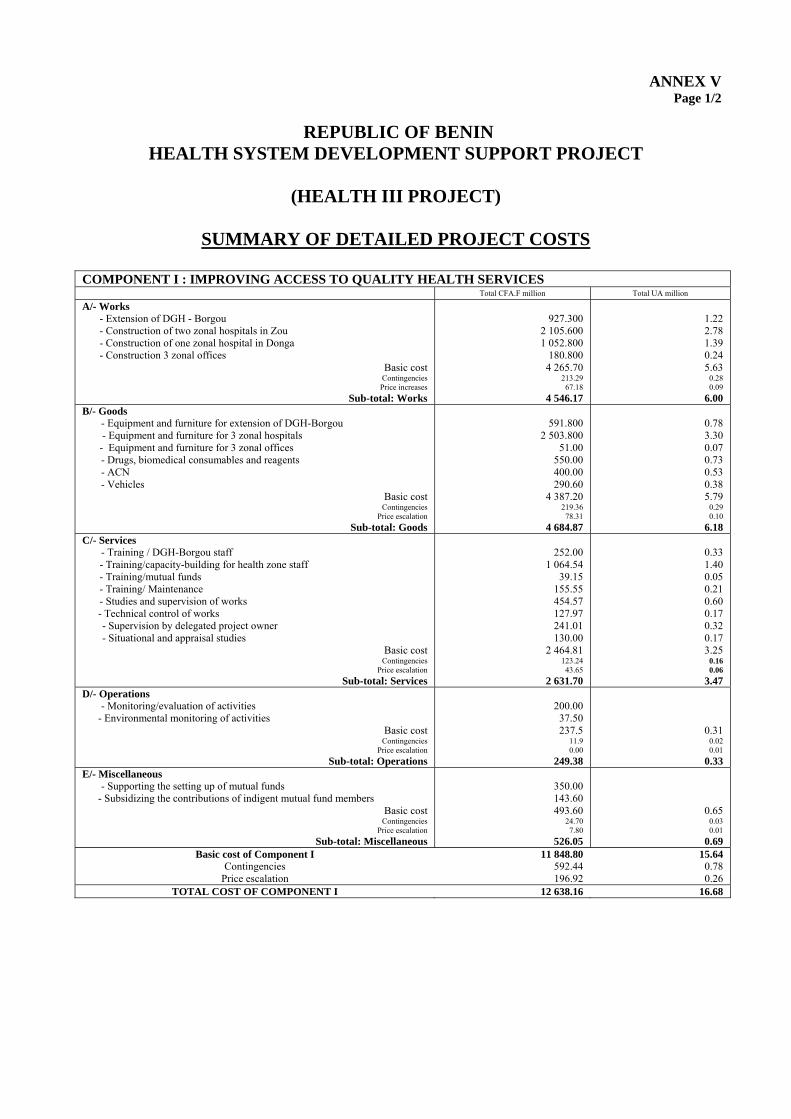
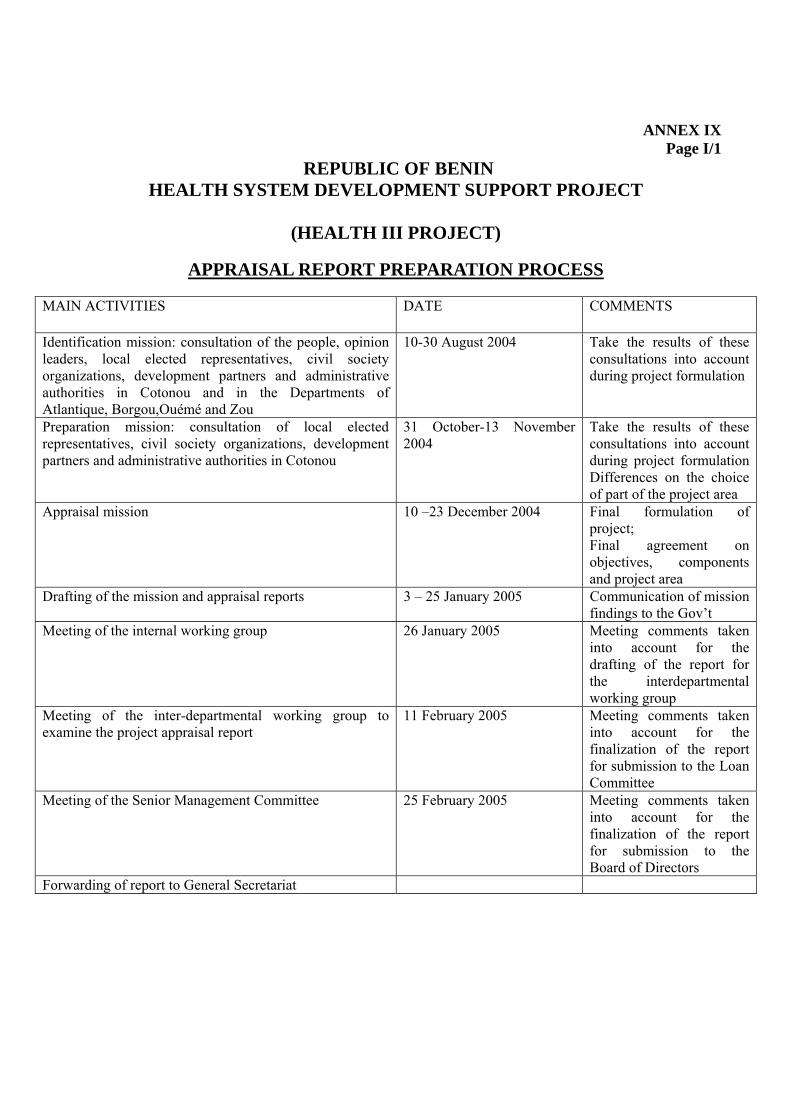
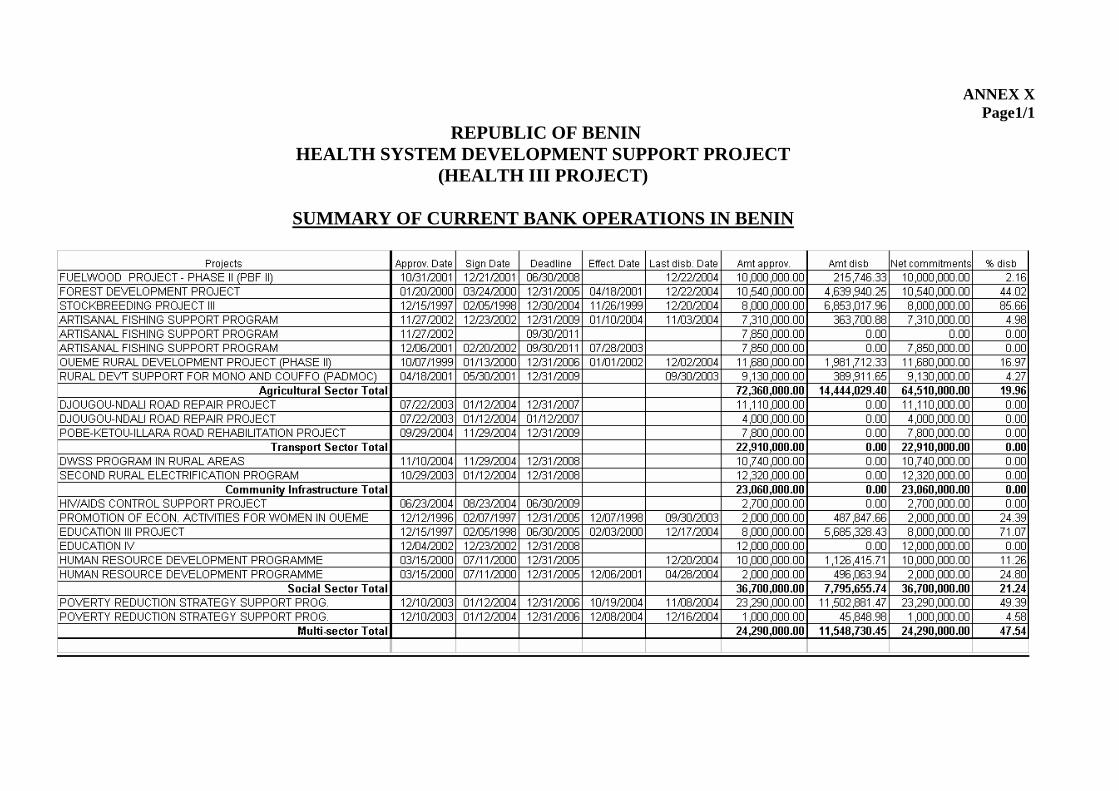
Annex 1 Interventions of Partners 1 Annex 2 Administrative Map of Benin and Project Areas 1 Annex 3 Summary of Coordinator’s Terms of Reference 1 Annex 4 Summary of Socio-Environmental Arrangements 1 Annex 5 Summary of Detailed Project Costs 2 Annex 6 List Of Goods and Services 1 Annex 7 Organization Chart of The PMU 1 Annex 8 Project Implementation Plan 1 Annex 9 Appraisal Report Preparation Process 1 Annex 10 Summary of Ongoing Bank Operations in Benin 1
v
LIST OF ACRONYMS AND ABBREVIATIONS ABEDA Arab Bank for Economic Development in Africa ADB African Development Bank ADMAB AAggeennccee ppoouurr llee DDéévveellooppppeemmeenntt ddeess MMuuttuueelllleess AAggrriiccoolleess aauu BBéénniinn ((AAggrriiccuullttuurraall MMuuttuuaall FFuunndd
DDeevveellooppmmeenntt AAggeennccyy iinn BBeenniinn)) AFD FFrreenncchh DDeevveellooppmmeenntt AAggeennccyy CAME Centrale d’Achat de Médicaments Essentiels (Essential Drugs Procurement Agency) CBC Communication for Behavior Change CBO Community-based Organization CIDA Canadian International Development Agency CCOOGGEESS CCoommiittéé ddee GGeessttiioonn ((MMaannaaggeemmeenntt ccoommmmiitttteeee)) CSP Country Strategy Paper DDDDPPHH DDeeppaarrttmmeennttaall DDiirreeccttoorraattee ooff PPuubblliicc HHeeaalltthh DGH Departmental General Hospital DHS Demographic and Health Survey DCA Delegated Contracting Authority EENNIIIIAABB EEccoollee NNaattiioonnaallee dd’’IInnffiirrmmiieerrss eett dd’’IInnffiirrmmiièèrreess AAddjjooiinnttss dduu BBéénniinn ((BBeenniinn NNaattiioonnaall SScchhooooll ooff
NNuurrsseess aanndd NNuurrssiinngg AAssssiissttaannttss)) EONC Emergency Obstetrical and Neo-natal Care EEUU EEuurrooppeeaann UUnniioonn GGDDPP GGrroossss DDoommeessttiicc PPrroodduucctt GTZ German Cooperation for Development HHBBSSDD HHyyggiieennee aanndd BBaassiicc SSaanniittaattiioonn DDeeppaarrttmmeenntt HIV Human Immuno-deficiency Virus HZ Health Zone ICDR International Center for Development and Research IEC Information, Education, Communication IMCI Integrated Management of Childhood Illnesses IMF International Monetary Fund IINNMMEESS IInnssttiittuutt NNaattiioonnaall MMééddiiccoo--ssoocciiaall ((NNaattiioonnaall SSoocciiaall WWeellffaarree IInnssttiittuuttee)) MCH Mother and Child Health MCPFD Ministry in Charge of the Plan, Forecasts and Development MMDDGGss MMiilllleennnniiuumm DDeevveellooppmmeenntt GGooaallss MEHTP Ministry of the Environment, Housing and Town Planning MFE Ministry of Finance and the Economy MFSWS Ministry of the Family, Social Welfare and Solidarity MPH Ministry of Public Health MMPPSSLL Ministry of Public Service and Labor NGO Non-governmental Organization OPEC Organization of Petroleum Exporting Countries PHR Partners for Health Reform PLWHA Person Living with HIV/AIDS PMU Project Management Unit PPNNCC PPrreennaattaall CCoonnssuullttaattiioonn PRSP Poverty Reduction Strategy Paper ROBS Network of Health NGOs in Benin STIs Sexually Transmitted Infections UA Unit of Account UNDP United Nations Development Program UNESCO United Nations Educational, Scientific and Cultural Organization UNFPA United Nations Population Fund UNICEF United Nations Children Fund USAID US Agency for International Development WB World Bank WHO World Health Organization ZMT Zonal Management Team ZO Zonal Office
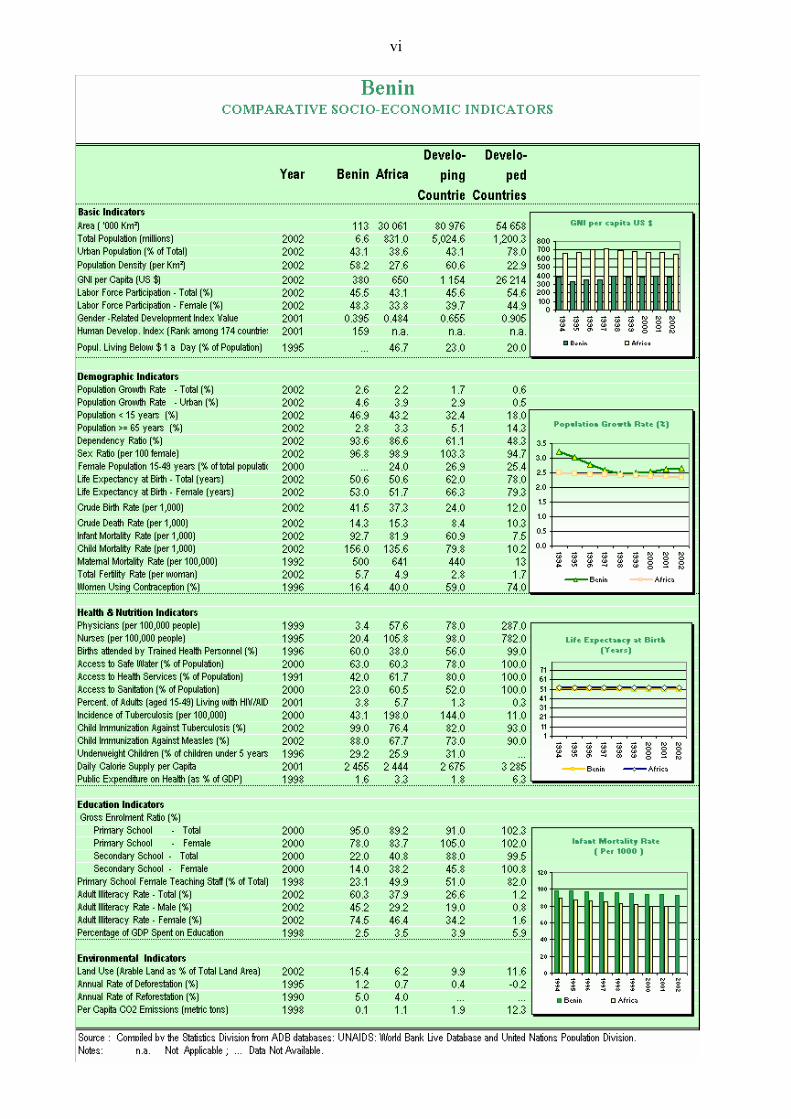
vi
vii
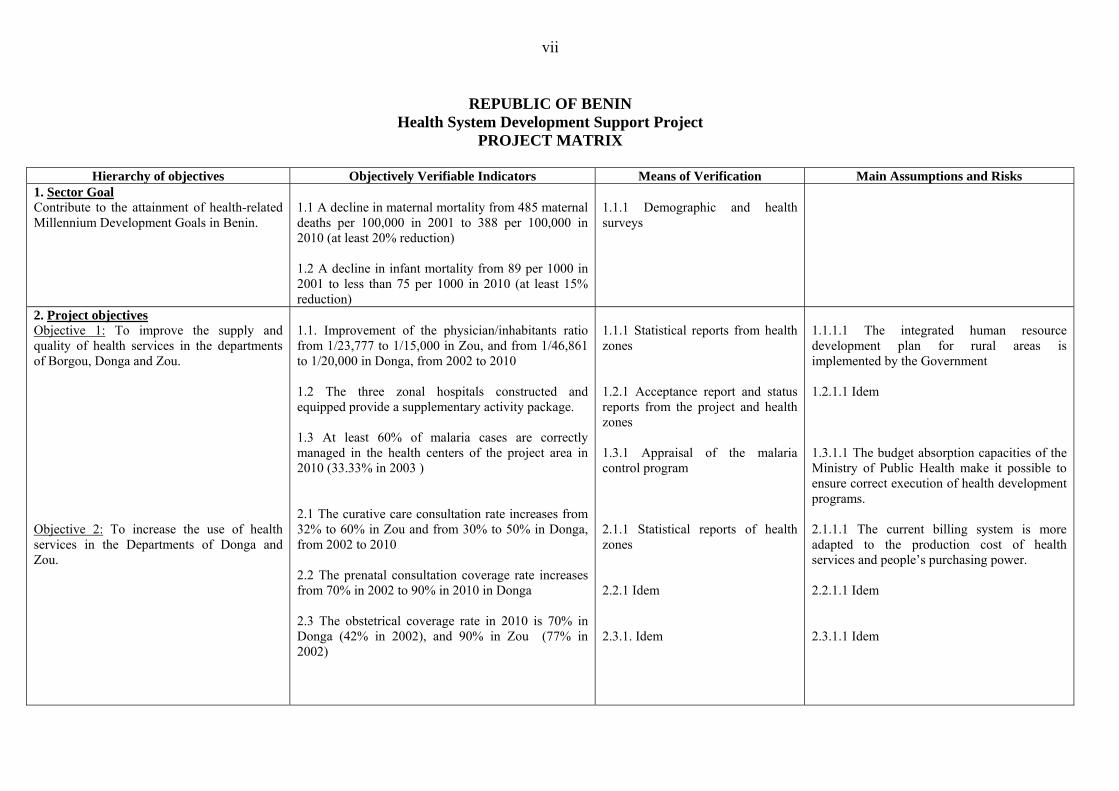
REPUBLIC OF BENIN
Health System Development Support Project PROJECT MATRIX
Hierarchy of objectives Objectively Verifiable Indicators Means of Verification Main Assumptions and Risks
1. Sector Goal Contribute to the attainment of health-related Millennium Development Goals in Benin.
1.1 A decline in maternal mortality from 485 maternal deaths per 100,000 in 2001 to 388 per 100,000 in 2010 (at least 20% reduction) 1.2 A decline in infant mortality from 89 per 1000 in 2001 to less than 75 per 1000 in 2010 (at least 15% reduction)
1.1.1 Demographic and health surveys
2. Project objectives Objective 1: To improve the supply and quality of health services in the departments of Borgou, Donga and Zou. Objective 2: To increase the use of health services in the Departments of Donga and Zou.
1.1. Improvement of the physician/inhabitants ratio from 1/23,777 to 1/15,000 in Zou, and from 1/46,861 to 1/20,000 in Donga, from 2002 to 2010 1.2 The three zonal hospitals constructed and equipped provide a supplementary activity package. 1.3 At least 60% of malaria cases are correctly managed in the health centers of the project area in 2010 (33.33% in 2003 ) 2.1 The curative care consultation rate increases from 32% to 60% in Zou and from 30% to 50% in Donga, from 2002 to 2010 2.2 The prenatal consultation coverage rate increases from 70% in 2002 to 90% in 2010 in Donga 2.3 The obstetrical coverage rate in 2010 is 70% in Donga (42% in 2002), and 90% in Zou (77% in 2002)
1.1.1 Statistical reports from health zones 1.2.1 Acceptance report and status reports from the project and health zones 1.3.1 Appraisal of the malaria control program 2.1.1 Statistical reports of health zones 2.2.1 Idem 2.3.1. Idem
1.1.1.1 The integrated human resource development plan for rural areas is implemented by the Government 1.2.1.1 Idem 1.3.1.1 The budget absorption capacities of the Ministry of Public Health make it possible to ensure correct execution of health development programs. 2.1.1.1 The current billing system is more adapted to the production cost of health services and people’s purchasing power. 2.2.1.1 Idem 2.3.1.1 Idem
viii
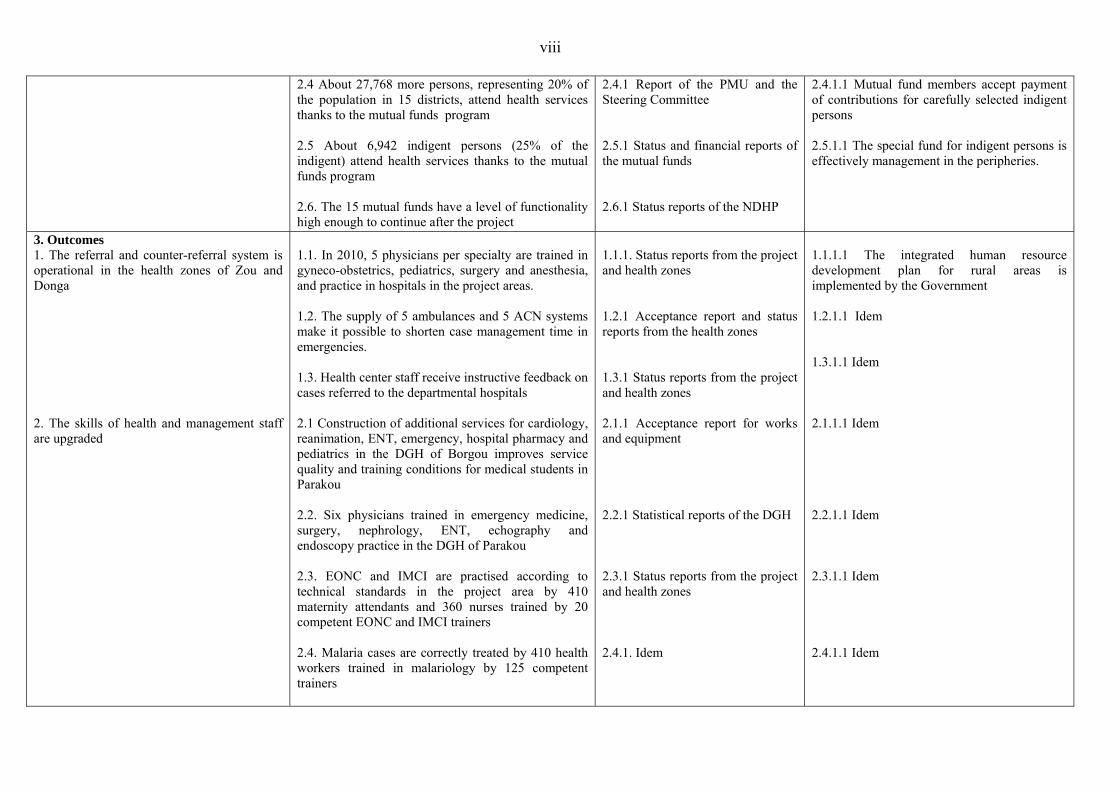
2.4 About 27,768 more persons, representing 20% of the population in 15 districts, attend health services thanks to the mutual funds program 2.5 About 6,942 indigent persons (25% of the indigent) attend health services thanks to the mutual funds program 2.6. The 15 mutual funds have a level of functionality high enough to continue after the project
2.4.1 Report of the PMU and the Steering Committee 2.5.1 Status and financial reports of the mutual funds 2.6.1 Status reports of the NDHP
2.4.1.1 Mutual fund members accept payment of contributions for carefully selected indigent persons 2.5.1.1 The special fund for indigent persons is effectively management in the peripheries.
3. Outcomes 1. The referral and counter-referral system is operational in the health zones of Zou and Donga 2. The skills of health and management staff are upgraded
1.1. In 2010, 5 physicians per specialty are trained in gyneco-obstetrics, pediatrics, surgery and anesthesia, and practice in hospitals in the project areas. 1.2. The supply of 5 ambulances and 5 ACN systems make it possible to shorten case management time in emergencies. 1.3. Health center staff receive instructive feedback on cases referred to the departmental hospitals 2.1 Construction of additional services for cardiology, reanimation, ENT, emergency, hospital pharmacy and pediatrics in the DGH of Borgou improves service quality and training conditions for medical students in Parakou 2.2. Six physicians trained in emergency medicine, surgery, nephrology, ENT, echography and endoscopy practice in the DGH of Parakou 2.3. EONC and IMCI are practised according to technical standards in the project area by 410 maternity attendants and 360 nurses trained by 20 competent EONC and IMCI trainers 2.4. Malaria cases are correctly treated by 410 health workers trained in malariology by 125 competent trainers
1.1.1. Status reports from the project and health zones 1.2.1 Acceptance report and status reports from the health zones 1.3.1 Status reports from the project and health zones 2.1.1 Acceptance report for works and equipment 2.2.1 Statistical reports of the DGH 2.3.1 Status reports from the project and health zones 2.4.1. Idem
1.1.1.1 The integrated human resource development plan for rural areas is implemented by the Government 1.2.1.1 Idem 1.3.1.1 Idem 2.1.1.1 Idem 2.2.1.1 Idem 2.3.1.1 Idem 2.4.1.1 Idem
ix
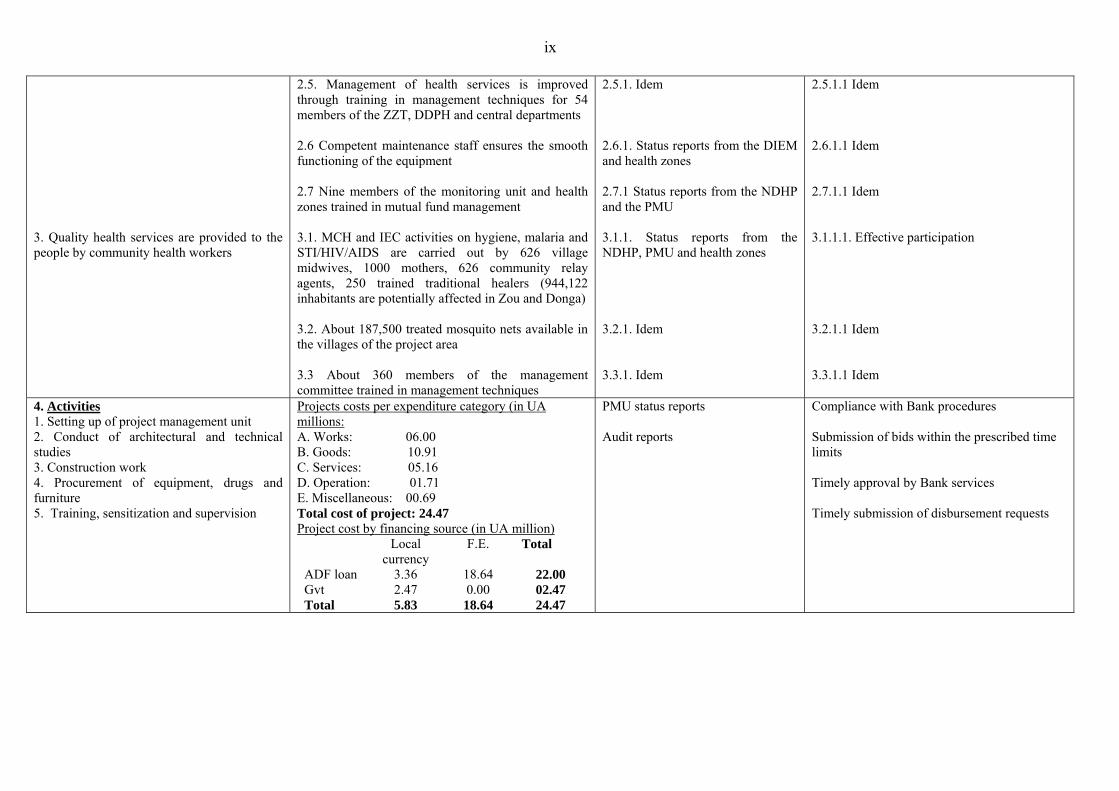
3. Quality health services are provided to the people by community health workers
2.5. Management of health services is improved through training in management techniques for 54 members of the ZZT, DDPH and central departments 2.6 Competent maintenance staff ensures the smooth functioning of the equipment 2.7 Nine members of the monitoring unit and health zones trained in mutual fund management 3.1. MCH and IEC activities on hygiene, malaria and STI/HIV/AIDS are carried out by 626 village midwives, 1000 mothers, 626 community relay agents, 250 trained traditional healers (944,122 inhabitants are potentially affected in Zou and Donga) 3.2. About 187,500 treated mosquito nets available in the villages of the project area 3.3 About 360 members of the management committee trained in management techniques
2.5.1. Idem 2.6.1. Status reports from the DIEM and health zones 2.7.1 Status reports from the NDHP and the PMU 3.1.1. Status reports from the NDHP, PMU and health zones 3.2.1. Idem 3.3.1. Idem
2.5.1.1 Idem 2.6.1.1 Idem 2.7.1.1 Idem 3.1.1.1. Effective participation 3.2.1.1 Idem 3.3.1.1 Idem
4. Activities 1. Setting up of project management unit 2. Conduct of architectural and technical studies 3. Construction work 4. Procurement of equipment, drugs and furniture 5. Training, sensitization and supervision
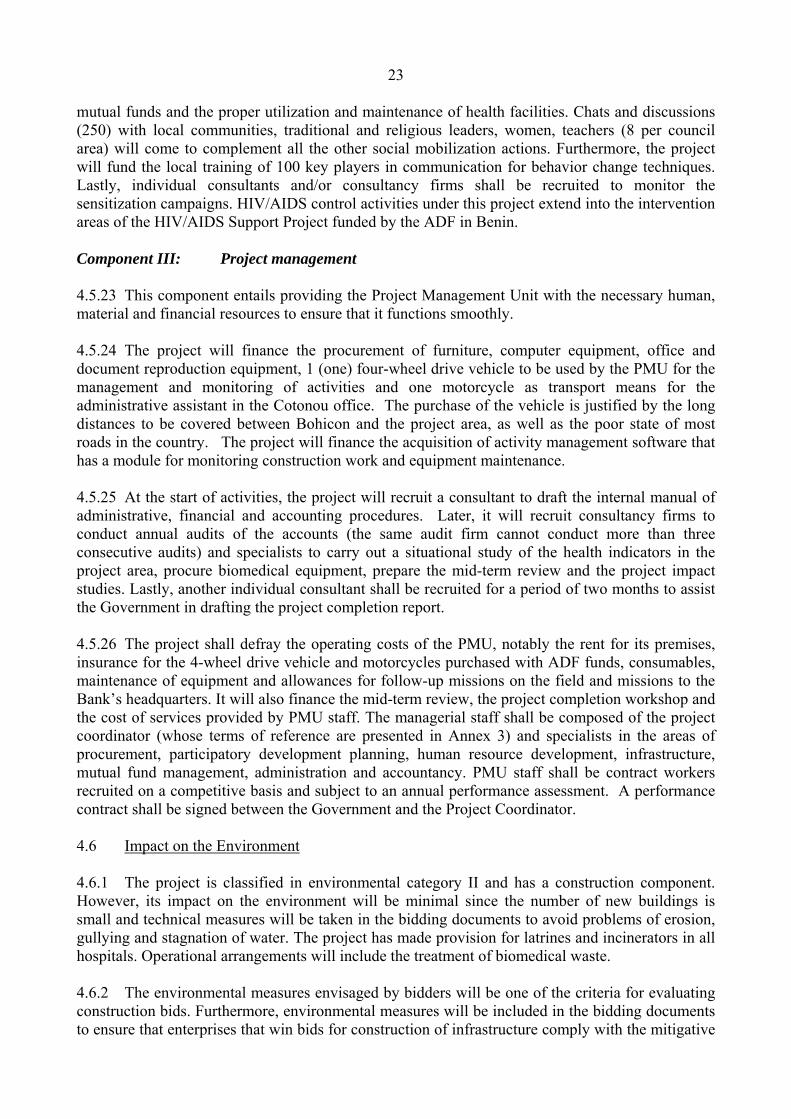
Projects costs per expenditure category (in UA millions: A. Works: 06.00 B. Goods: 10.91 C. Services: 05.16 D. Operation: 01.71 E. Miscellaneous: 00.69 Total cost of project: 24.47 Project cost by financing source (in UA million)
Compliance with Bank procedures Submission of bids within the prescribed time limits Timely approval by Bank services Timely submission of disbursement requests
x
EXECUTIVE SUMMARY 1. Project History
In a bid to tackle the health problems faced by its citizens, the Government of Benin designed a health sector development policy for 2002 – 2006 that tallies with the objectives of the Poverty Reduction Strategy Paper. To implement this policy, Benin submitted a request for financing to the Bank in July 2004. The Bank responded by proposing to assist Benin through the present project that was identified in August 2004, prepared in November 2004 and appraised in December 2004. The project takes into account the Millennium Development Goals, the global strategy and the commitments of other donors. It is also in line with the Bank Group’s operations strategy for Benin for 2002-2004 and its update, which is essentially to ensure a sustainable improvement of the country’s productive capacities, improve basic social services and reforms, and promote good governance. 2. Purpose of Loan
The project shall be co-financed by the ADF with a loan of UA 22 million and the Government
of Benin (UA 2.47 million). 3. Project Objectives
The sector goal of the project is to contribute to the attainment of the health-related
Millennium Development Goals in Benin: reduction of infant mortality, improvement of maternal and child health, control of STI/HIV/AIDS, malaria and other diseases. Its specific objectives are: (i) to improve on the supply and quality of health services; and (ii) to encourage greater use of health services. To that end, the project will reinforce the district health system and increase the supply of health services in the Departments of Borgou, Zou and Donga, in order to increase access to quality health services for the greatest number of Benin’s citizens. 4. Project Description
The project has three components: (i) increasing access to quality health services; (ii) promoting maternal and child health and disease control; and (iii) project management. Component I of the project comprises the development of health mutual funds; institution of a system to provide financial coverage to indigent patients; staff training; improvement of the referral system; conduct of studies; construction, equipment and maintenance of health infrastructure. In Component II, the project will help to improve coordination and implementation of hygiene promotion activities, control of malaria and STI/HIV/AIDS, promotion of mother and child health with special emphasis on emergency obstetrical and neo-natal care and the integrated management of childhood illnesses. Preference will be given to the community approach in project implementation through village midwives, community liaison officers, traditional healers, women’s associations and management committees. 5. Project Cost
The total project cost, net of taxes and customs duties, is estimated at UA 24.47 million, of
which UA 18.64 million is in foreign exchange and UA 5.83 million in local currency. Provision is made for an average allocation of 5% for contingencies, an annual inflation rate of 2% for foreign exchange and 5% for local currency.
xi
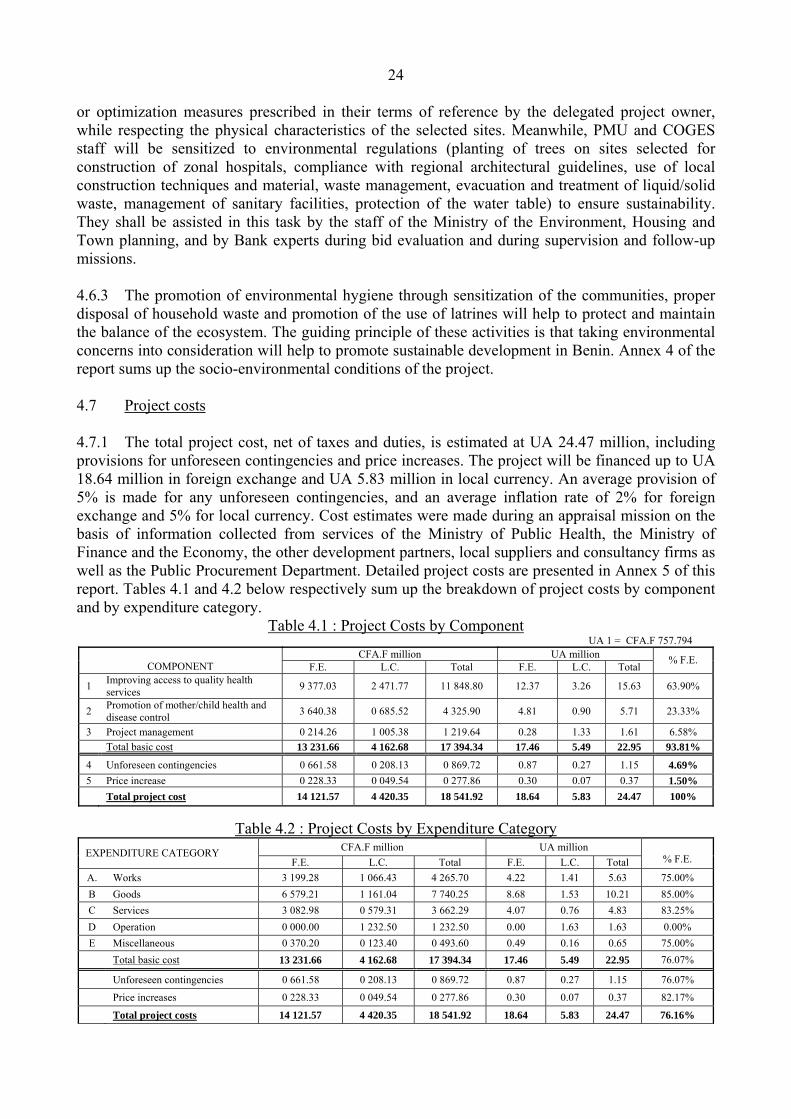
6. Financing Sources The project will be co-financed with an ADF loan and counterpart funds from the
Government of Benin. The ADF loan, amounting to UA 22 million, represents 89.91% of total project costs and covers 100% of expenses in foreign exchange (UA 18.64 million). The Government’s contribution (UA 2.47 million) represents 10.09% of total project costs and covers 42.32% of project costs in local currency. It will be used to finance expenses relating to the extension and equipment DGH-Borgou, the purchase of 5 (five) vehicles for the zonal offices, studies and supervision of extension work in DGH-Borgou as well as monitoring and evaluation of activities in the two components. 7. Project Implementation
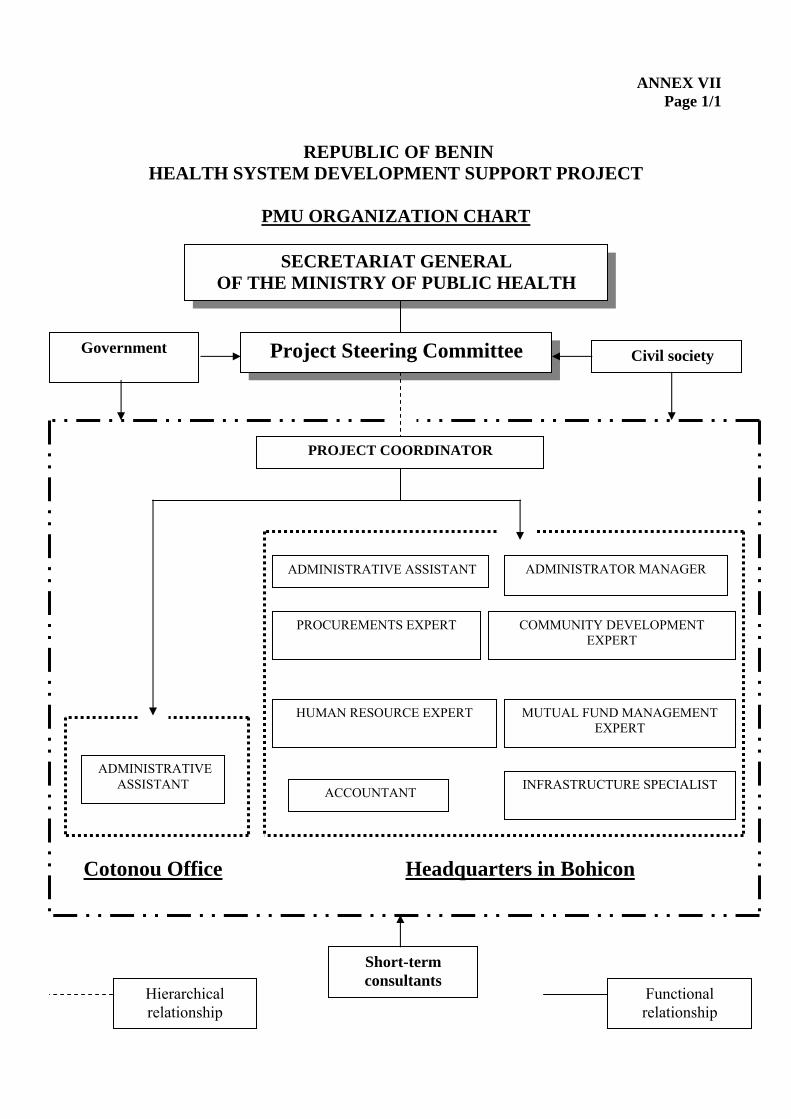
A Project Management Unit shall be set up under the authority of the Secretary-General of the Ministry of Public Health to implement this project. The members of the PMU shall be contract employees recruited through a competitive procedure and subject to continuous performance evaluation. The activities of the PMU shall be supervised by a Project Steering Committee composed of several ministries, representatives of development partners, the private denominational health sector and civil society. The duration of project implementation shall be 5 years. 8. Conclusions and Recommendations
The project constitutes a major step in the implementation of Benin’s health policy. It will
improve the health status of the people in general, and of women and children in particular. Hence, it is recommended that an ADF loan, not exceeding UA 22 million, be awarded to the Government of Benin for implementation of the project described in this report.
1. ORIGIN AND HISTORY OF PROJECT 1.1 The General Population and Housing Census of 2002 revealed that Benin, with an annual population growth rate of 3.25%, had 6,700,000 inhabitants, of whom 51.1% were women. Most of the population, which is essentially rural (61%) and young (47% below the age of 15), lives in the southern part of the country. There is widespread poverty with a national incidence of 37%, which mainly affects women and people in rural areas. This situation of generalized poverty, coupled with limited access to potable water (63%) and overcrowding under unsanitary conditions takes a heavy toll on the health of the people. 1.2 Indeed, the country’s health situation is dominated by endemic infectious and parasitic diseases, especially malaria. It is also prone to occasional outbreaks of cholera and meningitis. The border regions are particularly exposed to epidemics due to intense migratory movements, while life expectancy at birth is 59. Benin’s health system cannot cope with this situation because it is plagued with numerous problems that include inequitable distribution of human resources to the detriment of the northern regions of the country, the low functionality of the district health system, especially the referral and counter-referral system, and low attendance in health facilities (34%). 1.3 Faced with this situation, the Government of Benin designed a health sector development policy for 2002-2006 that tallies with the objectives of the 2003-2005 Poverty Reduction Strategy Paper and its updated version of 2004. Indeed, this policy focuses on improving the quality of and access to care and health services, especially for the poor and needy, and increasing community participation and encouraging greater use of health services. To support implementation of this policy, the Government of Benin submitted a request to the Bank in July 2004. 1.4 The present project was identified, prepared and appraised by the corresponding missions to Benin in August, November and December 2004, respectively. It is in line with the Government’s Action Program and the Bank Group’s Country Strategy Paper for Benin for 2002-2004 (extended to June 2005) and its updated version to reduce poverty. This strategy focuses on rural and social development, notably in the area of health: HIV/AIDS and malaria control, protection of women’s and children’s health, human resource development in deficient areas and introduction of financing alternatives that enable the majority of the people to have access to healthcare. The project also draws on the experience gained in the implementation of previous projects, notably the Health II Project, in the areas of infrastructure and equipment maintenance, staff training and improving access to health services for the underprivileged. Lastly, the project is in conformity with the health-related Millennium Development Goals, which include: reduction of infant mortality, improvement of maternal health and control of HIV/AIDS, malaria and other diseases. 2. THE SECTOR 2.1 Health Situation 2.1.1 The health situation of the people in Benin remains precarious, despite the efforts made by the Government and its partners, including the Bank. As is the case in neighboring countries (Togo, Nigeria, Burkina Faso, Niger) the epidemiological profile of Benin is dominated by infectious and parasitic diseases. According to the 2002 statistical report of the Ministry of Health, malaria topped the list, cited as chief complaint by 37% of patients (856,059 consultations), followed by acute respiratory infections (377,075), gastro-intestinal ailments (182,206), injuries (137,263) and diarrhea (127 060). The observed HIV/AIDS prevalence in 2002 was 1.9% with high predominance in the 15 to 49 age group (85.3% of cases). Tuberculosis, the primary opportunistic infection that accompanies AIDS, is on the rise and remains a major public health problem.
2
2.1.2 The morbidity rate is particularly high among women and children. Indeed, the incidence of simple and severe malaria among children under 5 is 6,921 cases per 10,000 and 898 cases per 10,000 respectively, with an average case-fatality rate of 7 deaths per 1000 (statistical report of the MPH). Malnutrition also features prominently among maternal and child health problems. Exclusive breastfeeding is practiced only for 38% of babies under 6 months and children under 5 suffer from retarded growth, with 11% of them being severely retarded. The proportion of women suffering from anemia is 64%, with 2% of them suffering from severe anemia (a hemoglobin rate of less than 7g/dl). The obstetrical cover varies from one region to another; for a national average of 63.1%, the lowest rate is observed in Atacora (34.6%) while the departments of Alibori, Borgou, Atlantique, Collines, Couffo and Donga have rates that range from 40% to 60%. The result is high maternal and infant mortality rates of 485 maternal deaths per 100,000 live births and 89.1 per 1000 (DHS 2001). 2.2 Government Policy and the Sector Action Program 2.2.1 The health sector development strategies and policy paper for 2002-2006, inspired from the Government’s Poverty Reduction Strategy Paper, defined three global objectives as follows: (i) improving the quality and access of care and health services; (ii) increasing community participation and the use of health services; and (iii) improving care for the poor and needy. The attainment of these objectives, which include those of the health-related Millennium Development Goals, will depend on the following five main actions: (i) reorganizing the base of the health pyramid and reinforcing health cover; (ii) financing the sector and improving resource management; (iii) improving the quality of care; (iv) preventing and controlling priority diseases such as AIDS, malaria and tuberculosis; and (v) promoting family health. 2.2.2 With regard to the first action, the Government and its partners, including the Bank, have made substantial efforts in recent years to provide the country with health infrastructure, attaining a geographical coverage of 80%. The recently completed Health II Project funded by the ADF, significantly helped to improve the geographical access rate through the construction and rehabilitation of health infrastructure in the department of Borgou/Alibori. Despite such relatively wide coverage of the national territory with health infrastructure, attendance in health facilities is low (34%) because of high prices and the poor quality of care. 2.2.3 For the second action, mechanisms to mobilize additional financial resources to supplement the State budget and donor contributions have been put in place to diversify sector financing sources. It is within this context that experiments to support mutual fund systems are underway as a means of solving the problem of financial inaccessibility to healthcare. Indeed, the Government has designed a health mutual fund development strategy under the coordination of a unit created in the community health service of the National Directorate of Health Protection (NDHP). On the field, implementation efforts are made essentially by NGOs and cooperation institutions, thus transforming Benin into “a vast experimental ground for health mutual funds”. 2.2.4 The Government is also developing a strategy to provide care to indigent persons. According to Decree No. 97/321 of 17 July 1997 relating to the assistance managed by the Ministry in charge of social welfare, an indigent person is “anyone who is in a situation of extreme poverty, unemployed, lacking adequate resources for survival, a victim of a natural disaster and placed in a particularly difficult situation, deprived of vital resources, experiencing social and economic difficulties and needing assistance from the State, local councils and the society to survive, as a result of his or her age, physical, mental or social state”. Over the last four fiscal years, an endowment of CFA.F 1 billion is allocated each year by the Government of Benin to the Ministry of Public Health and the Ministry of Family Affairs for the provision of care to indigent persons.
3
The aim of such an endowment, or indeed redistribution of public resources, is to ensure equity and equal opportunity, which constitute a key objective of the social welfare policy, and to provide support to persons living in abject poverty. The Government is looking for an appropriate mechanism, the best model for enhancing transparency in the management of funds and the means for ensuring optimum use of financial resources. The posting of a delegated financial controller to each ministry and the decentralization of budget management to departmental directorates of health and the various health zones are in line with this concern. 2.2.5 In an attempt to solve the problem of poor healthcare quality, Benin implemented strategies to enhance the management of human and material resources. Indeed, efforts have been deployed at all levels of the health system to promote the operational management of human resources through capacity-building and decentralized management. However, much inequality persists in the geographical distribution of trained staff to the detriment of rural areas and the northern part of the country. An infrastructure and equipment maintenance policy focusing on management procedures and the enhancement of user responsibility was designed and implemented in 2002. 2.2.6 With regard to disease control, HIV/AIDS, malaria and tuberculosis have been rated as priority diseases in Benin’s health policy, in accordance with the Abuja Declaration of African Union Heads of State and of Government. A National AIDS Control Committee and its branch offices have been set up to coordinate activities for promoting multisectoriality, communication, awareness-raising and behavior change in the population as a whole and in target groups in particular, prevention of mother-to-child transmission through blood, syndromic treatment of STIs, management of persons living with HIV and AIDS orphans, development of epidemiological surveillance and research. The Bank just approved an HIV/AIDS support project in July 2004 to back the efforts of Benin and its partners in this endeavor which still requires a lot of investments. 2.2.7 As concerns malaria, the focus is on reducing morbidity and mortality through improved access to healthcare for malaria patients, the use of treated mosquito nets for children under 5 and pregnant women and the improvement of malaria prevention among pregnant women. The “treatment and prophylaxis” component has become particularly complicated in recent years with the emergence of plasmodium strains that are resistant to Chloroquine, the main drug for treating simple malaria. Benin therefore revised its malaria control program by replacing Chloroquine with COARTEM – a combination of two molecules, Artemether and Lumefantrine – for treatment and Sulfadoxine-Pyrimethamine for intermittent preventive treatment for pregnant women. This situation requires new interventions such as the training of staff on case management, supplying the country with COARTEM and rapid diagnosis tests. To ensure quality management of malaria cases, the program plans to organize training in May-June 2005 to test the new modules prepared to that end. The training will be given to 25 health workers at the Regional Public Health Institute. 2.2.8 The national family health policy in four components covering women’s health, infant health, youth health and men’s health, is aimed at reducing maternal and infant mortality, encouraging responsible sexual behavior among the youth and getting men interested in reproductive health. Norms and standards were defined for each of the four components and the Department of Family Health, which is responsible for design and coordination of this component, is encountering difficulties in field implementation, notably with regard to emergency obstetrical and neonatal care (EONC) and integrated management of childhood illnesses. 2.2.9 Apart from the official health services, the people of Benin massively resort to traditional medicine and herbs to treat their ailments. Hence, much focus has been given to this branch of medicine in the national health policy through: (i) the setting up of a unit to that end in the Ministry of Public Health; (ii) the listing of traditional healers per department; (iii) the training of a certain number of them in malaria and STI/HIV/AIDS case management; and (iv) the creation of medicinal
4
plant gardens. However, a lot still remains to be done in this area before traditional medicine can fully play its role in improving the health. 2.3 Institutional Framework and Sector Organization 2.3.1 The organization of the public and private health sector is based on the administrative demarcation of the country into 12 Departments and 77 local councils. It comprises three additional levels, namely: the peripheral, intermediate and central levels. Each of these levels has management organs and healthcare infrastructure. 2.3.2 The peripheral level of the health system is the health zone, the local appellation for a health district. It is therefore the level at which national health development programs and projects are implemented and the basic level for healthcare provision to the people. There are 34 health zones in the country, each covering an average population of 100,000 to 200,000 inhabitants. Each health zone has a network of first contact health services and a referral hospital. The first contact services comprise village health units (VHUs), district health centers (DHCs), municipal health centers (MHCs) and private health units. The first level management organs are the village committee for VHUs, the district management committee (DMC) for DHCs and the municipal health constituency management committee (MHCMC) for MHCs. Furthermore, there are development associations in the various council areas which pursue the larger objective ensuring the wellbeing of the people. With regard to referrals, the zonal hospital management board, the health committee and the zonal management team respectively manage the hospital and the health zone. The doctor coordinating the health zone shall head the zonal management team composed of several other health, administrative, financial and technical officials of the health zone. 2.3.3 The health zones have different levels of functionality due to organizational shortcomings or shortage of staff, equipment or infrastructure. Only 25 out of 34 zonal hospitals fully play their role as referral structures and 50% of the zonal management teams do not have all the necessary skills to manage the zonal health system efficiently. Most of the management committees need renewal and training of members in social mobilization and health center management techniques. 2.3.4 The intermediate level administratively corresponds to the departmental level. It is worth noting that after the administrative redemarcation of 1999 which created 12 departments (by splitting each of the country’s 6 departments into two), the health system did not increase the number of departmental directorates of health and departmental general hospitals. Hence, there is currently one departmental directorate of health and one departmental general hospital for every two administrative departments. The health infrastructure at the intermediate level is the departmental general hospital (DGH), which is the referral structure for zonal hospitals within the department. The DGH is managed by a Director who reports to a Board of Directors. Placed under the coordination of the Departmental Director of Health (DDH) and the Management Board (CODIR) the intermediate level is the point at which national strategic guidelines are adapted to regional specificities; it is also the level for controlling standards and providing technical assistance to zonal health management teams. It also plagued by organizational shortcomings and a shortage of staff, equipment and infrastructure. 2.3.5 The central or national level defines strategic guidelines; it is also the level at which policies are designed and decisions taken on health sector development. The Minister’s Cabinet, the Secretariat General and the central departments coordinate all activities. At the central level, the National University Teaching Hospital is the apex of the healthcare pyramid. With regard to access
5
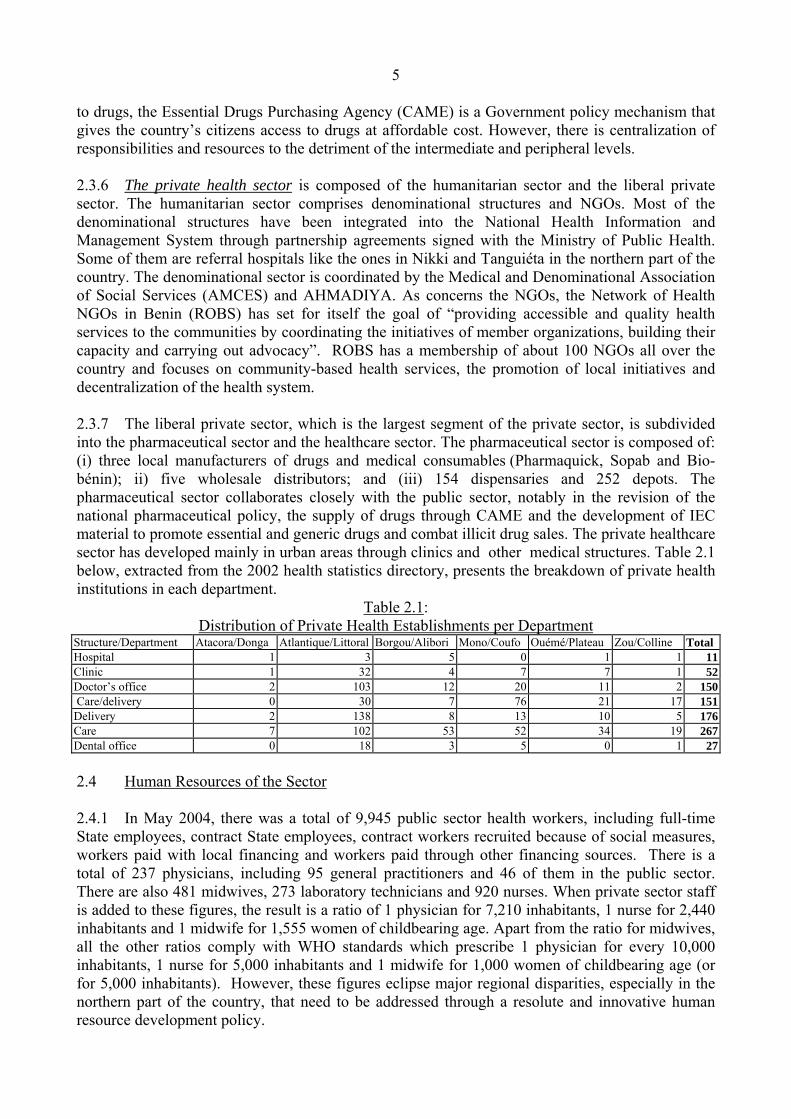
to drugs, the Essential Drugs Purchasing Agency (CAME) is a Government policy mechanism that gives the country’s citizens access to drugs at affordable cost. However, there is centralization of responsibilities and resources to the detriment of the intermediate and peripheral levels. 2.3.6 The private health sector is composed of the humanitarian sector and the liberal private sector. The humanitarian sector comprises denominational structures and NGOs. Most of the denominational structures have been integrated into the National Health Information and Management System through partnership agreements signed with the Ministry of Public Health. Some of them are referral hospitals like the ones in Nikki and Tanguiéta in the northern part of the country. The denominational sector is coordinated by the Medical and Denominational Association of Social Services (AMCES) and AHMADIYA. As concerns the NGOs, the Network of Health NGOs in Benin (ROBS) has set for itself the goal of “providing accessible and quality health services to the communities by coordinating the initiatives of member organizations, building their capacity and carrying out advocacy”. ROBS has a membership of about 100 NGOs all over the country and focuses on community-based health services, the promotion of local initiatives and decentralization of the health system. 2.3.7 The liberal private sector, which is the largest segment of the private sector, is subdivided into the pharmaceutical sector and the healthcare sector. The pharmaceutical sector is composed of: (i) three local manufacturers of drugs and medical consumables (Pharmaquick, Sopab and Bio-bénin); ii) five wholesale distributors; and (iii) 154 dispensaries and 252 depots. The pharmaceutical sector collaborates closely with the public sector, notably in the revision of the national pharmaceutical policy, the supply of drugs through CAME and the development of IEC material to promote essential and generic drugs and combat illicit drug sales. The private healthcare sector has developed mainly in urban areas through clinics and other medical structures. Table 2.1 below, extracted from the 2002 health statistics directory, presents the breakdown of private health institutions in each department.
Table 2.1: Distribution of Private Health Establishments per Department
Structure/Department Atacora/Donga Atlantique/Littoral Borgou/Alibori Mono/Coufo Ouémé/Plateau Zou/Colline Total Hospital 1 3 5 0 1 1 11Clinic 1 32 4 7 7 1 52Doctor’s office 2 103 12 20 11 2 150 Care/delivery 0 30 7 76 21 17 151Delivery 2 138 8 13 10 5 176Care 7 102 53 52 34 19 267Dental office 0 18 3 5 0 1 27 2.4 Human Resources of the Sector 2.4.1 In May 2004, there was a total of 9,945 public sector health workers, including full-time State employees, contract State employees, contract workers recruited because of social measures, workers paid with local financing and workers paid through other financing sources. There is a total of 237 physicians, including 95 general practitioners and 46 of them in the public sector. There are also 481 midwives, 273 laboratory technicians and 920 nurses. When private sector staff is added to these figures, the result is a ratio of 1 physician for 7,210 inhabitants, 1 nurse for 2,440 inhabitants and 1 midwife for 1,555 women of childbearing age. Apart from the ratio for midwives, all the other ratios comply with WHO standards which prescribe 1 physician for every 10,000 inhabitants, 1 nurse for 5,000 inhabitants and 1 midwife for 1,000 women of childbearing age (or for 5,000 inhabitants). However, these figures eclipse major regional disparities, especially in the northern part of the country, that need to be addressed through a resolute and innovative human resource development policy.
6
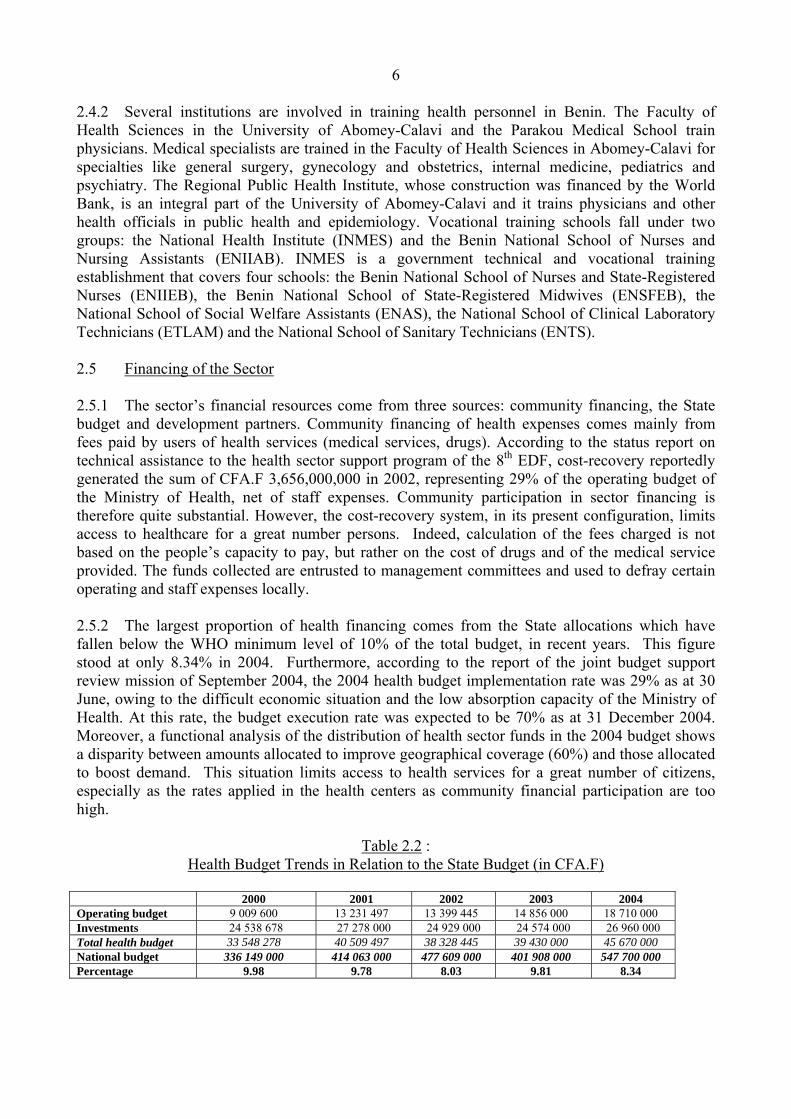
2.4.2 Several institutions are involved in training health personnel in Benin. The Faculty of Health Sciences in the University of Abomey-Calavi and the Parakou Medical School train physicians. Medical specialists are trained in the Faculty of Health Sciences in Abomey-Calavi for specialties like general surgery, gynecology and obstetrics, internal medicine, pediatrics and psychiatry. The Regional Public Health Institute, whose construction was financed by the World Bank, is an integral part of the University of Abomey-Calavi and it trains physicians and other health officials in public health and epidemiology. Vocational training schools fall under two groups: the National Health Institute (INMES) and the Benin National School of Nurses and Nursing Assistants (ENIIAB). INMES is a government technical and vocational training establishment that covers four schools: the Benin National School of Nurses and State-Registered Nurses (ENIIEB), the Benin National School of State-Registered Midwives (ENSFEB), the National School of Social Welfare Assistants (ENAS), the National School of Clinical Laboratory Technicians (ETLAM) and the National School of Sanitary Technicians (ENTS). 2.5 Financing of the Sector 2.5.1 The sector’s financial resources come from three sources: community financing, the State budget and development partners. Community financing of health expenses comes mainly from fees paid by users of health services (medical services, drugs). According to the status report on technical assistance to the health sector support program of the 8th EDF, cost-recovery reportedly generated the sum of CFA.F 3,656,000,000 in 2002, representing 29% of the operating budget of the Ministry of Health, net of staff expenses. Community participation in sector financing is therefore quite substantial. However, the cost-recovery system, in its present configuration, limits access to healthcare for a great number persons. Indeed, calculation of the fees charged is not based on the people’s capacity to pay, but rather on the cost of drugs and of the medical service provided. The funds collected are entrusted to management committees and used to defray certain operating and staff expenses locally. 2.5.2 The largest proportion of health financing comes from the State allocations which have fallen below the WHO minimum level of 10% of the total budget, in recent years. This figure stood at only 8.34% in 2004. Furthermore, according to the report of the joint budget support review mission of September 2004, the 2004 health budget implementation rate was 29% as at 30 June, owing to the difficult economic situation and the low absorption capacity of the Ministry of Health. At this rate, the budget execution rate was expected to be 70% as at 31 December 2004. Moreover, a functional analysis of the distribution of health sector funds in the 2004 budget shows a disparity between amounts allocated to improve geographical coverage (60%) and those allocated to boost demand. This situation limits access to health services for a great number of citizens, especially as the rates applied in the health centers as community financial participation are too high.
Table 2.2 : Health Budget Trends in Relation to the State Budget (in CFA.F)
2.6 Interventions of Donors 2.6.1 Several external, bilateral and multilateral partners support the implementation of the various strategies retained by the Ministry of Public Health (see Annex 1: Interventions of partners). Bilateral partners like Germany, Belgium, Canada, China, Egypt, France, the Netherlands, Switzerland and the USA generally intervene to give grants. The multilateral partners are the UN agencies, the European Union and the development banks, notably the World Bank, the Islamic Development Bank and the African Development Bank. These institutions generally provide assistance in the form of concessional loans, although part or all this assistance may be given as grants. Non-governmental organizations also participate in health sector development. Prominent among them are international NGOs like the Raoul Follereau Foundation, the Order of Malta and some national NGOs. According to a report published in December 2004 after a study commissioned by the Ministry of Public Health on the intervention map of health development partners in Benin from 1996 to2006, the investment areas most preferred by health partners are: institutional support, family health and priority diseases, especially STI/HIV/AIDS. Malaria control in particular did not seem to attract much attention even though malaria is the chief complaint of patients who come for consultation. In terms of geographical coverage, the same document indicates that the departments of Zou and Donga are least covered by the interventions of partners. 2.6.2 The Ministry of the Economy and Finance coordinates all donor interventions in the country. The World Bank, other bilateral partners and the ADF are financing a budget support program within the framework of poverty reduction (Poverty Reduction Support Credit for the IDA or Poverty Reduction Strategy Support Program (PRSSP) for the ADF, whose contribution for 2004 stood at CFA.F 11.46 billion). The measures retained in the health sector by the PRSSP include: i) posting newly recruited staff mainly to rural areas and instituting job incentive mechanisms for rural health units; (ii) consolidating the advanced strategy of initiating priority interventions for landlocked areas in all departments by the end of 2005; (iii) implementing and evaluating mechanisms to finance care for the indigent; and (iv) publishing and applying the reform of health center management committees (COGES), in order to enhance community management through training and increase the participation of the poor and needy. Regular updates are made (PRSC 1, PRSC 2) after evaluation of the implementation status of planned interventions and a medium-term expenditure framework for 2005-2007 has been drawn up that includes all the partners listed above. 2.6.3 The current health sector financing method in Benin is undergoing a transition phase that is still dominated by the “project approach”, although there is a very recent trend towards budget support. Hence, several partners, including the World Bank and Swiss Cooperation, assist the Government in conducting specific health development projects all over the country. The main achievements in the current process are essentially the holding of regular meetings to coordinate and harmonize interventions and the designation of a leader responsible for overall coordination and dialogue with the Government. In the design of all the projects it finances in Benin, including health projects, the Bank participates in this process, systematically insisting that there should be complementarity and relevant synergies with policies defined by the Government and those implemented by other donors. 2.6.4 Bank interventions in Benin’s health sector focus on two projects, namely: the HIV/AIDS control support project and the health component of the Human Resource Development Program (HRDP). The HIV/AIDS support project, financed with an ADF grant of UA 2.7 million is in the start-up phase, since the Government has not yet fulfilled all the conditions precedent to first disbursement. The health component of the HRDP, financed by OPEC for the sum of UA 4.16 million and administered by the ADF, has two components, namely: institutional development and
8
improvement of access to basic social services for the people. The activities of the current project are complementary with the HIV/AIDS control support project and the health component of the HRDP. 2.7 Health Sector Constraints 2.7.1 Despite the efforts made by the Government and its partners, several constraints hamper the development of the health sector in Benin. Such constraints include: (i) the low utilization of health services by the people; (ii) centralized resource management, especially human resources; and (iii) the poor quality of maintenance for existing facilities and equipment. Health Service Utilization Constraints 2.7.2 The utilization rate of health services is low (34%). This rate is all the more disturbing when considered side by side with the relatively satisfactory geographical coverage rate for top level health facilities, which stands at 80%. The low utilization of health services is due to financial difficulties, the poor quality of care, poor reception in health structures and cultural reasons. 2.7.3 From 1988, Benin adopted the cost recovery system to implement the Bamako Initiative and ensure health sector financing. Although there are texts governing billing mechanisms, it is difficult to talk of a real policy in this area. Indeed, there is no statutory justification for the rates charged for medical services in public and private establishments or for drug prices in Government health institutions (Status Report, European Union, April 2004). Wide disparities in drug prices have been noted between the various healthcare levels, between and even within the various departments, and between the various council areas. Moreover, there are no drug price control mechanisms. Hence, the average cost per case in 2002 was CFA.F 913, which is a major financial impediment to most people in Benin whose gross GDP per capita is CFA.F 280,782 (2002 Directory of Health Statistics). The Government plans to initiate a study that will make a profound analysis of the billing problem and make proposals that strike a balance between the real cost of medical services and the capacity and willingness of the people to pay for such services. 2.7.4 Moreover, 20% of Benin’s population lives in extreme poverty. For this fraction of the population, inaccessibility to health services stems, not from high rates, but from total marginalization from the system as a result of poverty. In addition to the proposals expected from the study on billing, other special interventions are needed to increase access to healthcare for such indigent people. This entails looking for health financing alternatives such as mutual funds and other systems for providing healthcare to poor patients. 2.7.5 With regard to cultural obstacles to the use of health services, conventional sensitization methods have shown their limits, hardly affecting the utilization rate of health services. Indeed, most of the people practice self-medication at home or prefer traditional medicine. The introduction of communication for behavior change through peer counseling is a potential avenue that could produce positive results. Moreover, the satisfactory figures registered for immunization activities carried out through an advanced strategy in the villages, justify extension of the other health services right down to the community/family level through community relay structures, associations and NGOs. Indeed, the vaccination coverage for children under 1 in 2002 reached very high rates of 119% for BCG, 102% for DCTCP3 and 97% for the anti-measles vaccine. The rates exceeding 100% could stem from the poor evaluation of children’s ages and underestimation of the target population (denominator).
9
Human resource management constraints 2.7.6 The human resource situation in Benin’s health sector is characterized more by inequitable geographical distribution than by insufficiency in quality and quantity. For instance, although there is a national average ratio of 1 physician per 7,210 inhabitants (for both private and public sectors), only the departments of Atlantique and Littoral have a ratio that is below 1 physician per 10,000 inhabitants (WHO standards). In Atacora/Donga and Borgou/Alibori in the North, the figures are respectively 46,861 and 17,532 inhabitants per physician. Apart from such staff concentration in the South to the detriment of the North, other aspects include a higher staff concentration in urban areas than in rural areas, staff reticence to working in rural areas, the inability of intermediate and peripheral structures to influence staff deployment and a shortage of specialized clinical staff. Indeed, the country lacks specialists especially in gynecology and obstetrics, surgery, pediatrics and anesthesia/resuscitation to ensure the optimum functioning of the health zones. Consequently, there is need for training in these priority domains and the findings of the imminent national study should make it possible to design an integrated human resource development plan for rural areas. The implementation of such a plan will require the assistance of all partners. Constraints relating to health infrastructure and equipment 2.7.7 There are wide disparities between the departments in Benin with regard to infrastructure coverage. The coverage rate in Zou, for example, is only 56% while the national average is 80%. Another constraint is the large number of health structures that do not comply with equipment and architectural norms and standards; this is the case with many isolated dispensaries and maternities all over the country. To address this problem, several stakeholders such as the Arab Bank for Economic Development in Africa, the Health Component of the Human Resource Development Project funded by OPEC and administered by the ADF, the World Bank and Swiss Cooperation, have undertaken to rehabilitate and construct more health centers in the years ahead. This will make it possible to provide a minimum activity package at the first level of healthcare. However, ensuring continuity in healthcare requires that zonal hospitals be constructed to provide the supplementary package at the second level. 2.7.8 Furthermore, the quality of infrastructure and equipment maintenance is poor. This limits the functionality of health structures since the poorly maintained equipment frequently breaks down and is repaired after long delays and at very high cost. Actions to enhance the management of maintenance activities by involving the management committees and collaborating with the private sector will help to improve the situation. 3. PROJECT COMPONENTS Considering the above constraints, the project’s main areas of intervention are: (i) improvement of healthcare quality through human resource development, consolidation of the referral system, construction of zonal hospitals and maintenance of infrastructure and equipment; (ii) improvement of the health services utilization rate by initiating a program to develop mutual funds and provide care to indigent patients, developing community-based health services, controlling communicable diseases and providing emergency obstetrical and neonatal care to the population. 3.1 Utilization of health services 3.1.1 This depends on several factors which include healthcare financing alternatives such as mutual funds, care for the indigent, community-based health services and traditional medicine.
10
Health mutual funds 3.1.2 Given the low attendance rate in health facilities, the Government has included the development of health mutual funds as a priority in health policy documents and is planning to set up an autonomous unit in charge of this component in the MPH. Health mutual funds are community-managed health insurance systems that enable members to have financial access to healthcare all the year round. The members of the mutual fund pay a premium, especially after the harvest when they are financially solvent. In this way, they are covered for a certain number of medical services determined beforehand, regardless of the amount of contribution paid. In other words, it is a risk-sharing system. In Africa, the experience of countries like Rwanda has shown that mutual fund members use health services five times more than non-members. In Benin, the oldest and most developed experiment in this domain is a project by the International Center for Development and Research (ICDR) to promote health mutual funds in the rural areas of Borgou and Collines. This project was started in 1994 in partnership with Swiss Cooperation and 24 council mutual funds were set up that involved more than 100 villages and covered a population of about 17,000 beneficiaries. It covers deliveries, hospitalizations and emergency surgery in more than 30 health centers and 3 denominational hospitals. 3.1.3 There are other experiments in the country with PHR Plus that are financed by the USAID (in Alibori) and the Danish, German and Belgian cooperations. In Donga, Borne Fonden covers the councils of Ouake, Copargo and 2 districts in the Bassila council area. In Zou, UNICEF is working with the councils of Abomey, Djidja and Agbangnizoun; the Association for the Development of Agricultural Mutual Funds in Benin (ADMAB) operates in Agboka district in the Abomey council area; Borne Fonden operates within the Zakpota and Agbagnizoun councils. These experiments have shown that it takes time to convince the people to join mutual funds since they do not always understand the concept of risk-sharing. A coverage rate of 9% to 20% may be reasonably attained after 2 or 3 years of operation. 3.1.4 These interventions notwithstanding, there is still no legal framework governing mutual funds and for reasons of equity several councils and districts in the country still have to be covered to enable the people living in such areas, especially the poor and needy, to have access to healthcare. In 2005, the Government will draft legislation governing mutual funds in Benin with World Bank support and so make it possible to undertake other interventions within a better organized framework. The political context is therefore favorable and the many current experiments in the country will serve as a catalyst and provide inspiration for the project as it strives to promote greater utilization of health services. Care for the indigent 3.1.5 Access to basic healthcare for the majority of poor people remains a big problem in Benin, whereas the country has a global poverty incidence rate of 37%. Denominational structures which traditionally providing care to the indigent do not follow standard modalities. Each structure has its own procedures for managing the indigent, its own criteria for identifying indigent persons and its own modalities for providing care to the poor and needy. Such modalities range from the application of flat rates and the provision of healthcare on credit to free medical treatment. In the public sector, efforts to provide care to the poor are recent and the practice has neither been formalized nor codified in the health units providing such care. For the past four years, the Government has allocated an annual sum of CFA.F 1 billion to the Ministry of Public Health and the Ministry of Family Affairs for provision of care to the indigent. However, the centralized management of this fund does not make it possible to reap maximum benefits in terms of greater access to healthcare for the indigent. Moreover, given the sheer scope of poverty, this allocation is
11
not enough to solve the problem even when it is managed in a decentralized manner. Additional financing as well as interventions that involve mutual funds, development associations and management committees will make it possible to secure more resources, propose alternatives to the current indigence fund management model and lay the foundation for sustainable approaches that facilitate access to care for the indigent. Such additional financing should guarantee that indigent patients have access to basic health services relating to reproductive health, vaccination and disease control, especially malaria and STI/HIV/AIDS. Community-based health services and traditional medicine 3.1.6 The low attendance recorded in health structures contrasts with the performance of preventive activities. Indeed, while health center attendance has stagnated at 34% for some years now, in spite of the improvement in geographical coverage for health infrastructure, the vaccination coverage figures for children under 1 have reached very high levels. For instance, 60% of pregnant women have received at least two doses of the anti-tetanus vaccine. The disparity between these figures and those for health center attendance may be explained by the adoption of an advanced strategy in the execution of vaccination activities in the villages of the community as a complement to the fixed strategy adopted in the health centers. This situation underscores the importance of bringing health services closer to users to ensure optimum utilization. Consequently, the development of community-based health services through community relay structures, associations and local NGOs will be one of the project’s areas of intervention to improve the health of the people. This activity shall be coordinated and technically supervised by employees from the social welfare centers of the Ministry of Family Affairs, Social Welfare and Solidarity. 3.1.7 Furthermore, the vast majority of the people in Benin prefer traditional medicine for cultural reasons or as an alternative to highly expensive “modern” medicine. That is why the Government initiated a promotional program from September 2004, with WHO support. The unit set up to that end within the Department of Pharmacy and Diagnostic Exploration of the Ministry of Public Health has already undertaken several actions which include: (i) the establishment of a list of 7,500 traditional healers all over the country; (ii) the organization of consultations at the council, departmental and national levels; (iii) the development of medicinal plant gardens managed by teams of traditional healers; (iv) preparation of two training modules on malaria and STI/HIV/AIDS; and (v) the training of 2,000 traditional healers on the diagnosis and treatment of simple malaria, the diagnosis and referral of severe malaria as well as malaria prevention. The above interventions notwithstanding, there is need to build the technical capacity of traditional healers so that they can efficiently play their role in satisfying demand for healthcare and improving the health status of the people. 3.2 Quality of Health Services in the Health Zones 3.2.1 The quality of health services in a given health zone depends on the presence of competent and motivated staff, the existence of a referral system and the existence of an efficient infrastructure and equipment maintenance system, all under the coordination and management of a competent zonal management team. Human resources 3.2.2 The health system in Benin is plagued with staffing problems, in terms of quantity and quality, and inequitable distribution of human resources on the national territory. This problem is more acute in the marginalized regions of the North and in rural areas. The joint Government/Partners Mission that reviewed budget support from 7 to 23 September 2004 identified
12
priority needs in general and for 2005 in particular, as follows: 100 State-registered midwives, 100 State-registered nurses, 50 junior nurses, 58 physicians including 50 general practitioners, 4 pediatricians, 6 gynecologists, 7 surgeons, 8 laboratory technicians and 8 senior x-ray technicians. The same mission recommended the recruitment of more contract staff for positions in landlocked, poor and isolated regions. Training qualified staff for deployment to marginalized regions and to the North of the country is a priority for the health system in Benin. In the Zou department, there is one physician per 23,777 inhabitants (standard requirement 1/10,000) and one midwife per 2,634 women of childbearing age (standard requirement 1/1000). In Donga, the ratios are one physician per 46,861 inhabitants and one midwife per 19,172 inhabitants (standard requirement 1/1000 inhabitants). 3.2.3 In a bid to provide a sustainable solution to this problem, the Government and its partners intend to conduct a nation-wide study whose conclusions and recommendations will be used to draft an integrated human resource development plan for rural areas. Meanwhile, pending the conclusions of this study, the Ministry of Health, with the support of several partners, is reflecting on the adoption of viable approaches that will not only help to staff rural areas with sufficient human resources in terms of quality and quantity and but also encourage staff to stay in these regions. The project will support implementation of the integrated human resource development plan as well as the adoption of viable problem-solving approaches, notably the signing of notarial agreements by scholarship applicants requiring them to serve for a certain number of years in regions identified as deficient in human resources. Referral hospitals 3.2.4 Although Benin has a relatively sufficient amount of basic health infrastructure, such infrastructure is often substandard, unevenly distributed, under-equipped and understaffed. The departments of Zou and Donga are examples of such inequitable distribution. Indeed the health coverage in Zou is only 56% compared to the national level of 80% and the two departments have an average of one health center for every 13,000 inhabitants compared to the annual average of 1/10,000. The Arab Bank for Economic Development in Africa has pledged to construct 6 health centers in Zou while the Human Resource Development Project will build two in Donga. Meanwhile, there is only one substandard zonal hospital in the three health zones of Zou, and another in the two health zones of Donga for which financing is not yet available. Building, equipping and staffing zonal hospitals with competent personnel to enhance functionality is crucial to the improvement of the referral and counter-reference system and fundamental to the functioning of the district health system. 3.2.5 The referral and counter-referral system is based on the principle of a clear apportionment of services and organization of working relations between the two levels of the health district, all geared towards handling more than 90% of the health problems faced by the population in the district (zone). The health center, which is the first level, provides the minimum package of activities and the zonal hospital, which is the second level, provides the supplementary package. If there is a case that is beyond the technical capacity of the health center, the staff will resort to the district hospital in two possible ways (referral): either through communication to get additional information that will enable them to manage the case, or by simply transferring the patient to the district hospital for more adequate care. After treating the patient, the hospital, in turn, sends the patient back to his area of origin for follow-up at the health center. This is what is referred to as counter referral. This therefore requires: (i) first level infrastructure that can provide the minimum package (trained staff, equipment); (ii) zonal hospitals that are capable handling referred cases (trained staff, equipment); and (iii) a communication system between the two levels (radio communication, ambulance). Not all health zones in the country have these three fundamental
13
elements of the referral and counter-referral system; for instance, there is a burning need to construct zonal hospitals in the project area. Maintenance of infrastructure and equipment 3.2.6 With regard to maintenance, there is an acute shortage of qualified staff at all levels of the health system. Furthermore, the allocations made by the Government as maintenance credits are spent mainly on vehicles and not on buildings or medical equipment. Preventive maintenance is not developed and since the system is neither supervised nor audited, missing equipment and spare parts cannot be accounted for. The Government drew on the experience of the Benin-German primary healthcare project and the ADF II Health Project to draft a policy in 2002 governing the maintenance of infrastructure, medico-technical equipment and vehicles. This policy provides for a maintenance system that is modeled on the three-tier pyramidal health system: the peripheral level of the maintenance system is based in the zonal hospitals and shall be managed by a maintenance engineer; departmental maintenance units are being set up in DGHs and departmental directorates of public health. The Department of Infrastructure, Equipment and Maintenance in the Ministry of Health coordinates overall implementation of the maintenance policy. The project will support the implementation of this policy by training staff and reorganizing the maintenance system at the grassroots through greater involvement of management committees and the consolidation of partnerships between the public and private sectors. Overall management system for the health zones 3.2.7 The health zones in Benin are plagued with numerous operational difficulties that stem from organizational shortcomings or the shortage of staff, equipment and infrastructure. Only zonal hospitals in 25 out of the 34 zones fully play their role as referral structures. The affirmed political will to decentralize management has not been fully translated into reality on the field, and this has given rise to operational difficulties and the need to renew most of the management organs. Since the health zone is the level at which health services are provided to the people, there is a close relationship between its functionality status and the quality of care, the attendance rate in health structures and by extension, the health status of the people. That is why the Health Zone Development Support Unit defined criteria for the evaluation of health zone functionality as follows: (i) the existence and functionality of management organs; (ii) a management process notably with health development plans; (iii) local resource management including preventive maintenance; (iv) health training activities, notably including the availability of the minimum package of activities at the level of the zonal hospital; (v) the referral and counter-referral system. An evaluation of the 34 health zones in the country using this criteria will lead to the drafting of a health zone development plan that takes into account the technical management of health activities, human resource management as well as financial, administrative and material management. 3.3 Communicable Diseases (Malaria, Diarrhea and STI/HIV/AIDS) 3.3.1 The endemicity of infectious and parasitic infections such as malaria, diarrhea and STI/HIV/AIDS in Benin stems mainly from behavioral causes that remain resistant to the sensitization strategies hitherto developed by health services. With regard to malaria in particular, poor case management is also another cause. Indeed, surveys conducted by the malaria control program and WHO (mid-term review of Abuja objectives, May 2004) have shown that in 2003, only 33.33% of malaria cases were correctly treated in health centers upon appearance of the very first symptoms. This figure is far below the target of 60% set by the Abuja Declaration which raised malaria, tuberculosis and HIV/AIDS to the status of priority diseases against which vigorous action had to be taken. Furthermore, the Government made adjustments to its malaria control
14
program, notably by replacing Chloroquine with Coartem because of the high level of resistance manifested by some strains of plasmodium. 3.3.2 Several types of interventions are therefore necessary to reduce the burden of these diseases, especially on children, within the framework of integrated management of childhood illnesses, such as malaria, malnutrition, acute respiratory infections, and diarrhea. Training qualified staff to coordinate malaria control, procuring a new drug for treatment and prevention and initiating awareness-raising activities will help to efficiently tackle malaria which is the leading pathology in Benin. As concerns STI/HIV/AIDS, the interventions that have been planned will complement those of the ADF-sponsored HIV/AIDS Project being implemented in the other departments. Communication for behavior change through peer counseling will be developed under this project. 3.4 Reproductive Health Activities Access to reproductive health services in Benin is also as limited as for all the other health services. Proof of this is the high annual population growth rate of 3.25% revealed by the Demographic and Health Survey of 2001. Childbearing starts early for women in Benin, with the fertility rate reaching 109 per 1000 from the age of 15 to 19 years; the total fertility rate is 5.6 per woman. Limited access to reproductive health services equally accounts for the high maternal mortality rate (485 maternal deaths per 100,000 live births). Indeed, given the shortage and/or poor quality of staff as well as the low functionality of health infrastructure and facilities due to poor maintenance, Benin has few health structures that really provide emergency obstetrical and neonatal care (EONC), which is the key to reducing infant and maternal deaths. There are only 1.4 (instead of 4) health units per 500,000 that provide basic EONC, resulting in a 22.9% coverage in EONC services instead of 100%. To improve on these indicators, there is need to train staff, encourage workers to remain in understaffed areas, equip health centers and ensure maintenance. 4. PROJECT 4.1 Design and Rationale of Project 4.1.1 The project was designed to contribute to the implementation of health sector development policies and strategies in Benin. Indeed, by developing human resources, consolidating the referral and counter-referral system, improving the maintenance system and enhancing the functionality of health zones, the project will contribute to the realization of the primary objective of the national health policy, which is to improve the quality of health services and increase access to healthcare and health services. It will also contribute to the attainment of the second objective of increasing community participation and encouraging greater use of health services, through the development of health mutual funds, the development of community-based health services and reinforcement of the role of traditional medicine. Lastly, the project will help to improve the healthcare management of the poor and needy (third objective) by paying the contributions of indigent members in mutual fund programs, while proposing measures to enhance the use of Government funds allocated to that end. 4.1.2 The project was designed and formulated after a needs analysis of the 12 departments that make up the country, based on the health and poverty level indicators of the population as well as the presence, or otherwise, of partners. The main health indicators taken into account are the attendance rate in health structures, the obstetrical coverage rate which partly determines the maternal mortality rate, the infant mortality rate, and the ratio of health personnel, especially physicians and midwives, to the population. The functionality status of first level hospitals was also taken into account, since Benin has relatively good geographical coverage for first-level
15
infrastructure (80%). Certain activities of the project will focus on improving these specific indicators in the project area while other activities will have a national impact. 4.1.3 The project was also designed and formulated taking gender equity into consideration. In Benin society, women experience the greatest financial obstacles to healthcare since they are the hardest-hit by poverty. This will be taken into account in the payment of the contributions of indigent members of mutual fund programs by ensuring that there is a greater proportion of women among the beneficiaries. Furthermore, the development of community-based health services will facilitate access to such services for women since their numerous household chores prevent them from visiting health services, especially when such services are located far away. Reducing infant morbidity will also give more free time to women. Sensitization activities, notably on STI/HIV/AIDS, will be of double benefit to women because they are more vulnerable from the biological and social standpoints. 4.1.4 The participatory approach was adopted during project design. Indeed, decentralized Government structures, local elected officials and the main development partners participated in the discussions. The World Bank, the European Union, USAID, Belgian and Swiss Technical Cooperations, GTZ, the Network of Health NGOs in Benin (ROBS), potential beneficiary groups, community-based organizations (CBOs), management committees, private operators, women’s and youth associations were all involved in the design of this project. In particular, the project took into account the quasi-unanimous position of partners that priority be given to activities that raise attendance in health services and those that improve geographical coverage. 4.1.5 The Bank already has some experience in this area in Benin through the financing of several projects that focus on health or have a health component: construction of the Regional Public Health Institute in Ouidah, the Health System Reinforcement Project (Health II), the Human Resource Development Project (HRDP) and the HIV/AIDS Control Support Project. The current project supplements and reinforces the activities of the STI/HIV/AIDS Control Support Project by extending them to the Departments of Donga and Zou. IEC activities, in particular, supplement activities to prevent mother-to-child transmission in maternities found in the HIV/AIDS project area. In fact, women will more readily undergo screening tests during pregnancy if they are aware that their babies can be protected against HIV through the efficient methods practiced in the maternity. 4.1.6 According to the completion report of the Health II Project, the main lessons learnt include: (i) frequent changing of the coordinator and low motivation of the other members of the coordination unit, which results in blockage of activities and prolongs the project implementation period; (ii) the underutilization of constructed health infrastructure; and (iii) irregularity of project audits. The following measures will be taken to address these difficulties and improve implementation of the current project: (i) the PMU staff will be recruited through a competitive process to avoid frequent staff redeployment by the State, which is prejudicial to project implementation; (ii) the mandates of the various project officials shall include evaluations by objective based on predetermined assessment criteria, in order to increase accountability and ensure that implementation deadlines are respected; (iii) a performance contract shall be signed between the Government and the Project Coordinator; (iv) to reduce the risk of low returns on investment due to under-utilization of the facilities, actions that increase demand for healthcare will be preferred over buildings or included in project activities in cases where buildings are absolutely necessary; (v) central and decentralized Government structures as well as community-based associations have to be involved in project implementation to ensure sustainability of the actions implemented; (vi) a steering committee will ensure that audits, status reports and mid-term reviews are prepared regularly and forwarded to the Bank and the Government.
16
4.1.7 The current project will also draw on the positive experience of Health Project II and even consolidate it. Such is the case with the procurement of generic essential drugs under the Health Project II, which facilitated the renewal of stocks by including a wider range of drugs on the drug list. This made it possible, not only to treat a greater number of diseases but also to reduce stock outages, thereby improving the quality of healthcare. Furthermore, training under the Health II Project improved the technical quality of treatment although the trained staff did not stay in place for long. The present project will address that problem by developing measures that will encourage trained staff to remain in the project area. Similarly, construction and rehabilitation activities have improved geographical coverage, staff working conditions and the comfort of health service users for both outpatient care and hospitalization. However, this had no notable impact on the attendance rate in health structures, thus confirming the general observation made after sector analysis during design of the present project. Consequently, the current health system development support project will lay emphasis on activities that raise attendance in existing in structures. However, buildings will be constructed only when it is absolutely necessary, bearing in mind that there is need to include activities that will encourage more patients to use the facilities. 4.2 Project Areas and Beneficiaries 4.2.1 The project covers 3 of the 12 departments in the country, namely Borgou, Zou and Donga (Annex 2: Administrative map of Benin and project areas). The department of Borgou was selected because the Parakou Departmental General Hospital serves as a training facility for the School of Medicine opened in Parakou in response to the need to maintain medical staff within the northern part of the country. Furthermore, this hospital, in its current configuration, does not fulfill the minimum technical criteria required for a medical training facility since it lacks services such as cardiology, reanimation and ENT, while certain existing services, such as pediatrics, need to be expanded. Since the project has a component for training qualified staff and in the absence of a real university teaching hospital for which the Government is still seeking financing, the realization of the additional construction and extension works will enable the DGH to contribute to human resource development in the medical sector and to fully play its role as a hospital offering highest level specialized care in the department of Borgou/Alibori and the entire Northern region; all the more so since Cotonou, the capital, is very far from Parakou. The intervention of the current project, which supplements the rehabilitation work carried out in this hospital under the ADF Health II Project, will be limited to these construction activities, equipment and staff training activities. 4.2.2 The low level of health indicators, which fall below the national average, and the relatively limited presence of other donors justify the choice of Donga. The economic status of the people depends very much on cotton whose prices are falling, thereby aggravating the already high poverty levels. GTZ carried out some activities in the department to organize NGOs within the framework of decentralization, which constitutes a solid base for partnership and a guarantee of success for the project’s activities. Donga department has 26 districts and 202 villages. The ratios are 1 physician to 46,861 inhabitants (the standard being 1 physician to 10,000 inhabitants) and one midwife to 19,172 inhabitants (the standard being 1 midwife to 5000 inhabitants). The attendance rate in health structures is 30% compared to the national average of 34%. Prenatal consultation activities cover 70% of pregnant women and 42% of them benefit from assisted delivery. There are 25 health centers in Donga including two whose construction has been planned within the framework of PDRH. The department has two health zones with no zonal hospitals that are up to standard. Belgian Cooperation intends to bring the Bassila zonal hospital up to standard and the denominational hospital of the Order of Malta in Djougou requires standardization work on condition that it is upgraded into a zonal hospital.
17
4.2.3 The department of Zou was also selected because of its low health indicators. It has 9 council areas subdivided into 76 districts and 424 villages. It has 1 physician for every 23,777 inhabitants (the standard being 1/10,000) and 1 midwife to 2,634 women of childbearing age (the standard being 1/1,000). The attendance rate in heath structures is 32%. The coverage is 95% for prenatal consultations and 77% for obstetrical consultations. The infant mortality rate is 106 per 1000, compared to a national average of 89.1 per 1000. The department is subdivided into 3 health zones: the Djidja-Abomey-Agbangnizoun health zone whose zonal hospital is below standard and the Covè-Zagnanado-Ouinhi and Bohicon-Zogbodomè-Zakpota health zones which have no zonal hospitals. Overall, they have 47 health centers, including 5 that are still to be constructed by ABEDA. 4.2.4 The beneficiaries of the project are the people from the three departments of Borgou (724,171 inhabitants), Zou (618,192 inhabitants) and Donga (325,930 inhabitants), or 1,668,293 inhabitants representing more than a quarter (26%) of the country’s total population. Indeed, in Donga and Zou, the development of mutual funds and the management of indigent patients, community activities to promote maternal and child health, the promotion of hygiene and disease control, will be most beneficial to the indigent population and those living in rural areas who make up the greatest majority. The people of Borgou, and by extension those living in the entire Northern part of the country, will benefit from the interventions of the Parakou DGH since this hospital will play its role as regional hospital of last resort after the planned expansion. All citizens of Benin will also benefit from the effects of the project through the specialized training of several physicians which will provide the country with a pool of experts in the various priority specialties. In particular, the training of health officials in malariology will improve coordination of the control and treatment of malaria which is the leading cause of morbidity and mortality in the country. The project’s contribution to the development of the maintenance system will benefit the entire population of Benin by enhancing the durability and functionality of biomedical infrastructure and equipment. By financing the functionality assessment of 34 health zones and serving as an accompaniment to the measures that will be proposed in the integrated human resource development plan for rural areas, the project will help to improve health system management, which is the foundation needed for provision quality and efficient services to the people. 4.3 Strategic Context 4.3.1 The project is in line with the health-related millennium development goals, namely: reducing infant mortality, improving maternal health, controlling STI/HIV/AIDS, malaria and other diseases. The project also falls in line with the strategic objectives of Benin’s PRSP for 2003-2005 and its update of July 2004, especially the second strategic aspect which aims at: (i) improving the overall management of the system; (ii) increasing access, quality and use of health services thereby contributing to the attainment of national objectives of reducing infant and maternal mortality and managing epidemics; and (iii) improving the people’s financial access to quality health services. Indeed, activities to reinforce the district health system, notably the study on the functionality of health zones created under the project, will help to improve the overall management of the system within the framework of decentralization. Implementation of the mutual fund program which includes a system for managing indigent patients will help to enhance the people’s financial access to quality health services. 4.3.2 The project reflects the priorities of the 2005-2007 Medium Term Expenditure Framework of the PRSP which, in particular, makes provision for substantial allocations to the decentralized level to facilitate financial access to health services for the poorest patients. The 2005-2007 MTEF equally provides for a greater allocation for operational expenses to cover investments, notably human resource development through training and staff deployment to disadvantaged areas.
18
4.3.3 By combating high mortality diseases (malaria, HIV/AIDS), giving priority to the vulnerable classes and improving maternal health through the development of emergency obstetrical and neonatal care, the project also tallies with the Bank’s policies on health and the control of communicable diseases. Indeed, in increasing access to quality healthcare, it lays emphasis on equity by including an important component on community-based activities and setting up mutual funds that will enable poor patients to be covered by the system. Through these interventions that focus on community-based health services and financial coverage of indigent patients, the project is in line with the Bank’s policy on cost recovery for health services; this policy considers basic health services as public property and as such, cost recovery systems have to ensure that the poorest patients have access to them. 4.3.4 Lastly, the project is keeping with the Bank’s Country Strategy Paper for Benin for 2002-2004 (running up to June 2005) and its updated version which lay emphasis on the rural and social sectors with consolidation of basic social services, notably health. The consolidation of basic social services entails providing and ensuring the use of quality basic social services that are financially and culturally accessible to the majority of the population: basic community health services, healthcare financing alternatives, rehabilitation/construction and equipment of health centers and zonal hospitals, improvement of the maintenance system and human resource development. 4.4 Project Objectives The general objective of the project is to contribute to the achievement of the health-related Millennium Development Goals in Benin: reducing infant mortality, improving maternal health and combating STI/HIV/AIDS, malaria and other diseases. Its specific objectives are to: (i) improve the supply and quality of health services; and (ii) encourage greater use of health services. 4.5 Project Description 4.5.1 To attain these objectives, the project focuses on the following three main components: (i) improving access to quality health services; (ii) promoting mother and child health and combating disease; and (iii) project management. The duration of project implementation shall be 5 years. Component I: Improving access to quality health services 4.5.2 The objective of this component is to reinforce the district health system in order to open access to quality healthcare for the greatest number of people in Benin. The interventions include the construction and equipment of health facilities, staff training, development of health mutual funds and the conduct of studies. Improvement of the referral and counter-referral system 4.5.3 To improve on the quality of healthcare, provide the best training conditions to the students in the Parakou Faculty of Medicine and help to maintain physicians in the northern part of the country, the project will finance the extension of the Parakou Departmental General Hospital through construction and equipment of additional services for cardiology, reanimation, ENT, emergency, hospital pharmacy and the extension of the pediatric service. 4.5.4 The project will also finance the construction of three zonal hospitals, two for the Djidja and Covè health zones in Zou department, and one in Djougou health zone in Donga department. Three zonal offices will be constructed to improve on the working conditions of the zonal management teams. The land on which the new facilities will be constructed is available in areas with electricity
19
and water supply and the Government will take the necessary administrative decisions to transfer it to the project. For the Borgou DGH, the problem of land does not arise given that the extension work will be done on an existing site. 4.5.5 To facilitate the execution and monitoring of construction work, a delegated project owner (DPO), recruited through a competitive process among the structures available in Benin, shall coordinate all construction and extension of the health facilities concerned. Indeed, there are 3 (three) structures that have agreements with the Government and act on its behalf as delegated project owner for the construction of infrastructure in rural and urban areas. They have procurement procedures that are deemed correct and acceptable by the multilateral institutions. They recruit engineering firms, assessment consultants and enterprises through consultations and competitive bidding. Following a competitive bidding process organized through the recruited DPO, the project will pay an engineering consultancy firm to conduct architectural and technical studies and supervise the construction of zonal hospitals, zonal offices and the extension of the DGH in Borgou. The project will also pay a technical control firm, recruited through a competitive process, to control the studies, works and material used for construction. 4.5.6 Furthermore, drugs and medical consumables, biomedical equipment, furniture and computer equipment will be procured for the additional newly constructed services in the Borgou DGH, the three hospitals and the zonal offices. Five ambulances and aerial communication network (ACN) systems will also be procured for the 5 health zones in Zou and Donga departments. The ACN will facilitate communication between the health centers and the referral hospital and the ambulances will help to curb delays in case management, especially for surgical and obstetrical emergencies. Five pick-up trucks will be procured for the zonal management teams to improve on the supervision of health centers and the supply of drugs and medical consumables to these centers. 4.5.7 With regard to the general improvement of staff management and the functioning of health zones, the project will participate in implementing the recommendations of the study planned by the Ministry of Public Health to prepare the drafting of the integrated human resource development plan for rural areas. The project will also pay consultants to conduct a national study on the evaluation of the functional capacity of the country’s 34 health zones. This study will make a diagnosis of the situation in the various zones and make proposals for improving the functioning of the health zone management organs, the management process, local resource management, the activities of health structures and the referral and counter-referral system. Implementation of the conclusions of this study will help to improve the functionality of the health zones, thereby increasing access to quality healthcare for the greatest number of people. With regard to the complete reorganization of the current maintenance system, the project will finance a study on diagnosis of the system and the possibility of contracting out all maintenance activities. 4.5.8 Lastly, the project will finance expenditure relating to the supervision of staff in health centers and members of the management committee by the zonal management teams, the supervision of the zonal management teams by other teams from the departmental directorates of health and supervision of the latter by officials from the central departments in the Ministry who are involved in project implementation. Development of mutual funds and a health coverage system for indigent patients 4.5.9 To improve financial access to healthcare, the project will follow a competitive process to recruit and finance an NGO specialized in health mutual fund development and management to implement a program for 15 mutual funds in 15 districts in Zou and Donga departments. By 31 December 2008 latest, the Government will forward a copy of the law governing health mutual funds in Benin to the Bank. The selected NGO shall choose the districts concerned following
20
criteria that guarantee the best chances of success; each of the 5 health zones is supposed to have 3 mutual funds. The goal is to cover at least 5% of the population in the 15 districts in the first year, 12% in the second year and 20% in the third year of the mutual fund program, making a total of 27,768 members by the end of the project. 4.5.10 To facilitate access to healthcare for part of the indigent population, the project will finance their contribution to the mutual fund program for a total of CFA.F 143.6 million. The beneficiaries shall be identified by the health center management committees with the assistance of social welfare centers, with due regard for gender equity in the selection of indigent beneficiaries. To prevent reticence from voluntary contributors, such financial contributions from the project shall not cover more than 25% of the total membership, representing 6,942 persons. However, the NGO responsible for setting up the mutual funds shall have the latitude to determine the number of indigent members to be covered, depending on the number of persons willing to join. Overall, the mutual fund program will cover 34,710 persons, representing 25% of the population in each district. The project will finance the procurement of 13 motorcycles to facilitate movement for administrative staff engaged in sensitization work. A unit in charge of mutual funds set up in the Ministry of Health shall coordinate and disseminate this experiment within the entire health system. The project will finance the training of 4 persons from this unit in mutual fund management techniques. Building staff capacity 4.5.11 The project will finance the training of 6 physicians in emergency medicine, surgery, nephrology, ENT, echography and endoscopy in order to build training capacity for students on internship in the Parakou DGH and improve service quality. Other health officials from the Parakou DGH will receive advanced courses in human resource management, health management, anesthesia, etc. The project will also finance the training of 20 specialists for the 5 health zones in Zou and Donga departments, representing a total of 5 doctors per specialty for pediatrics, gynecology/obstetrics, surgery and anesthesia/reanimation. To improve the maintenance of infrastructure and equipment, which are important in healthcare, the project will finance the training of two biomedical engineers, two engineers and 5 infrastructure maintenance technicians. The award of scholarships for these long training courses will be subject to the signature of a notarial agreement by beneficiaries pledging to serve for at least five years in a duty station within the project area. These training courses, once conducted, will make it possible to cover the needs of the project area in identified domains. 4.5.12 In a bid to improve the management of the entire system, the project will build the managerial capacity of the zonal management teams by training 3 members per project health zone, making a total of 15 in each of the following areas: human resource management, financial and material management including maintenance, and supervision and monitoring of activities. The officials in charge of supervision and monitoring in the 2 (two) departmental directorates of health (2 persons) and in the Health Zone Development Support Unit zones will also be trained in monitoring and supervision of activities. The officials in charge of financial and material management in the two departmental directorates of health and the official responsible for monitoring health zones in the Department of Financial Affairs will also be trained in financial and material management. The officials in charge of human resource management in the two departmental directorates of health and the official in charge of monitoring health zone human resources within the Department of Human Resources shall be trained in planning and decentralized management of human resources. Training courses will be organized in each department under the coordination of the health zone development support unit. Members of development associations and project area management committees (360 persons) shall also be
21
trained in budget planning techniques including maintenance, and techniques for managing contractual relations with mutual funds and the private sector in the area of maintenance. 4.5.13 In a bid to promote preventive maintenance and curb any delays in repairs, 25 local private service providers (5 per project health zone) shall be identified by the management committees and technicians from the departmental maintenance services of Zou and Donga. These local service providers shall then receive training from the technicians on a series of preventive and reparatory maintenance activities that have to be performed periodically or in case of damage in the various health structures: plumbing, electricity, masonry, electro-mechanics and computer technology. The practical modalities of this public sector-private sector partnership will be outlined in contracts signed with the management committee. 4.5.14 As part of its initiative to develop the mutual fund system, the project will finance the training of 4 members of the mutual fund unit in the Ministry of Health and 1 member per zonal office (9 persons in all) in mutual fund management techniques. Furthermore, 5 members per management committee, making a total of 360 beneficiaries, shall be trained in techniques to manage contractual relations with mutual funds. Component II: Promotion of mother/child health and disease control 4.5.15 This component is aimed at increasing the supply of health services. It entails improving the coordination and implementation of hygiene, disease control and family health activities. Project activities in this area will include technical assistance, training and equipment. Promotion of mother and child health 4.5.16 The project will lend assistance to the Ministry of Public Health by financing the training of 20 national trainers to implement emergency obstetric and neonatal care (EONC) and 20 national trainers for integrated management of childhood illness (IMCI), notably malaria, malnutrition, acute respiratory infections and diarrheal infections. It will also finance the training of 10 trainers, (1 per HZ, 1 per DDH and 3 at the DFH) to reinforce family planning services in particular and reproductive health (RH) in general. These trainers, who will be at the disposal of the Ministry to support the other zones of the country, shall later train 5 healthcare workers in each maternity in the project area on RH and EONC. Moreover, 5 health workers per health center and 10 health workers per zonal hospital, representing a total of 770 persons, will also be trained in IMCI techniques. In all, 60% of the trainers and health workers will be women. At the community level, the project will finance the training of 626 village midwives in sensitization techniques and different family health promotion activities: prenatal consultations, assisted delivery, integrated management of childhood illnesses, exclusive breastfeeding, diarrheal diseases, STI/HIV/AIDS, female genital mutilation, etc. All the above trained staff, who shall be selected on the basis of gender equity, will cover national needs (with regard to the trainers) and those of the project area to ensure smooth implementation of EONC and IMCI. 4.5.17 The project will finance the procurement of: (i) training material; (ii) midwifery kits; (iii) EONC material for zonal maternities (equipment for intra-uterine suction, suction cups, obstetrical forceps, aspirators for newborns, reanimation tables for newborns). Disease control 4.5.18 Under the new control policy for malaria, which remains the leading cause of morbidity and mortality, the project will finance the organization of 5 national courses on malariology in the
22
Regional Institute of Public Health. Each 3-week session of these courses shall be attended by 25 health workers, making a total of 125 malariologists who will coordinate the malaria control program in the whole country. The project will also finance the training of staff from health centers and zonal hospitals in the project area on the new treatment schedule. Malaria control will also be reinforced at the community level by financing the training of 20 members of women’s organizations at the zonal level in the management of mosquito net tontines. Promoting the role of treated mosquito nets in malaria control for pregnant women and children under 5 is a priority of the program and the experience of mosquito net tontines, which are already successfully operational in some health zones of the country, has to be extended to the project area. Moreover, health workers will train 1000 mothers in home management of fever caused by malaria. The project will provide the first stock of treated mosquito nets to women’s associations and NGOs (national needs stand at 1,200,000 units) to support the launching of the mosquito net tontine in the 5 health zones of the project. It will also finance the procurement of COARTEM and rapid diagnosis malaria tests. 4.5.19 As part of the program to promote traditional medicine, the project will also finance the training of 250 traditional healers, representing 50 per health zone, on sensitization techniques, psycho-social management of STI/HIV/AIDS, diagnosis and treatment of simple malaria, diagnosis and referral of serious malaria and malaria prevention. Such training shall be provided by the traditional medicine promotion unit in the Department of Pharmacy and Laboratories which has already established a list of traditional healers to be included in the program. These initiatives will extend the activities of the ADF-financed HIV/AIDS control project to the current project area. The project will finance the development of 20 medicinal plant gardens that shall be jointly operated by the traditional healers. Bicycles will also be given to the traditional healers who shall use them for sensitization activities. 4.5.20 In the area of disease control through promotion of environmental hygiene, the project will join the Department of Basic Hygiene and Sanitation in the Ministry of Public Health, within the framework of the hygiene and sanitation program, to finance the training of 360 community relay agents and NGO leaders in communication for behavior change techniques: body hygiene, washing hands before meals and after visiting the toilet, promotion and management of latrines, management of household garbage, cesspools, manure pits, etc. To promote the construction and use of latrines, masons residing in the villages will be trained, 15 per health zone, in latrine construction techniques. These masons shall be selected from a list established by the Department of Basic Hygiene and Sanitation within the framework of its program of action. The project will finance the procurement of sanitation material (carts, wheelbarrows, shovels) for women’s associations and NGOs involved in the promotion of hygiene. 4.5.21 The project will finance the cost of monitoring training and execution of activities by the Department of Basic Hygiene and Sanitation of the Ministry of Public Health and expenses related to the evaluation of malaria control and mother/child health promotion activities. Communication for behavior change 4.5.22 In a bid to encourage behavior change in the project area, a series of four annual sensitization and prevention campaigns shall be conducted for women, the youth, vulnerable children and orphans. To that end, the project shall follow a competitive procedure to secure the expertise of specialists from social welfare centers, specialized NGOs and the private sector to vet the content of messages and draft and implement sensitization and prevention messages. Sensitization and information radio programs (360) shall be broadcast to the general public on issues such as HIV/AIDS, reproductive health, priority diseases, body and environmental hygiene,
23
mutual funds and the proper utilization and maintenance of health facilities. Chats and discussions (250) with local communities, traditional and religious leaders, women, teachers (8 per council area) will come to complement all the other social mobilization actions. Furthermore, the project will fund the local training of 100 key players in communication for behavior change techniques. Lastly, individual consultants and/or consultancy firms shall be recruited to monitor the sensitization campaigns. HIV/AIDS control activities under this project extend into the intervention areas of the HIV/AIDS Support Project funded by the ADF in Benin. Component III: Project management 4.5.23 This component entails providing the Project Management Unit with the necessary human, material and financial resources to ensure that it functions smoothly. 4.5.24 The project will finance the procurement of furniture, computer equipment, office and document reproduction equipment, 1 (one) four-wheel drive vehicle to be used by the PMU for the management and monitoring of activities and one motorcycle as transport means for the administrative assistant in the Cotonou office. The purchase of the vehicle is justified by the long distances to be covered between Bohicon and the project area, as well as the poor state of most roads in the country. The project will finance the acquisition of activity management software that has a module for monitoring construction work and equipment maintenance. 4.5.25 At the start of activities, the project will recruit a consultant to draft the internal manual of administrative, financial and accounting procedures. Later, it will recruit consultancy firms to conduct annual audits of the accounts (the same audit firm cannot conduct more than three consecutive audits) and specialists to carry out a situational study of the health indicators in the project area, procure biomedical equipment, prepare the mid-term review and the project impact studies. Lastly, another individual consultant shall be recruited for a period of two months to assist the Government in drafting the project completion report. 4.5.26 The project shall defray the operating costs of the PMU, notably the rent for its premises, insurance for the 4-wheel drive vehicle and motorcycles purchased with ADF funds, consumables, maintenance of equipment and allowances for follow-up missions on the field and missions to the Bank’s headquarters. It will also finance the mid-term review, the project completion workshop and the cost of services provided by PMU staff. The managerial staff shall be composed of the project coordinator (whose terms of reference are presented in Annex 3) and specialists in the areas of procurement, participatory development planning, human resource development, infrastructure, mutual fund management, administration and accountancy. PMU staff shall be contract workers recruited on a competitive basis and subject to an annual performance assessment. A performance contract shall be signed between the Government and the Project Coordinator. 4.6 Impact on the Environment 4.6.1 The project is classified in environmental category II and has a construction component. However, its impact on the environment will be minimal since the number of new buildings is small and technical measures will be taken in the bidding documents to avoid problems of erosion, gullying and stagnation of water. The project has made provision for latrines and incinerators in all hospitals. Operational arrangements will include the treatment of biomedical waste. 4.6.2 The environmental measures envisaged by bidders will be one of the criteria for evaluating construction bids. Furthermore, environmental measures will be included in the bidding documents to ensure that enterprises that win bids for construction of infrastructure comply with the mitigative
24
or optimization measures prescribed in their terms of reference by the delegated project owner, while respecting the physical characteristics of the selected sites. Meanwhile, PMU and COGES staff will be sensitized to environmental regulations (planting of trees on sites selected for construction of zonal hospitals, compliance with regional architectural guidelines, use of local construction techniques and material, waste management, evacuation and treatment of liquid/solid waste, management of sanitary facilities, protection of the water table) to ensure sustainability. They shall be assisted in this task by the staff of the Ministry of the Environment, Housing and Town planning, and by Bank experts during bid evaluation and during supervision and follow-up missions. 4.6.3 The promotion of environmental hygiene through sensitization of the communities, proper disposal of household waste and promotion of the use of latrines will help to protect and maintain the balance of the ecosystem. The guiding principle of these activities is that taking environmental concerns into consideration will help to promote sustainable development in Benin. Annex 4 of the report sums up the socio-environmental conditions of the project. 4.7 Project costs 4.7.1 The total project cost, net of taxes and duties, is estimated at UA 24.47 million, including provisions for unforeseen contingencies and price increases. The project will be financed up to UA 18.64 million in foreign exchange and UA 5.83 million in local currency. An average provision of 5% is made for any unforeseen contingencies, and an average inflation rate of 2% for foreign exchange and 5% for local currency. Cost estimates were made during an appraisal mission on the basis of information collected from services of the Ministry of Public Health, the Ministry of Finance and the Economy, the other development partners, local suppliers and consultancy firms as well as the Public Procurement Department. Detailed project costs are presented in Annex 5 of this report. Tables 4.1 and 4.2 below respectively sum up the breakdown of project costs by component and by expenditure category.
Table 4.1 : Project Costs by Component UA 1 = CFA.F 757.794
CFA.F million UA million COMPONENT F.E. L.C. Total F.E. L.C. Total
% F.E.
1 Improving access to quality health services 9 377.03 2 471.77 11 848.80 12.37 3.26 15.63 63.90%
2 Promotion of mother/child health and disease control 3 640.38 0 685.52 4 325.90 4.81 0.90 5.71 23.33%
4.7.2 The project shall be jointly financed by an ADF loan of UA 22 million, which represents 89.91% of the total project cost and covers 100% of costs in foreign exchange (UA 18.64 million). The Government’s contribution (UA 2.47 million) represents 10.09% of total project costs and covers 42.32% of costs in local currency. It shall be used to finance expenses relating to the extension and equipment of DGH-Borgou as well as the monitoring and evaluation of the activities of the two components. The various financing sources are presented in Table 4.3.
Table 4.3 : Project Costs by Financing Source (in UA million)
4.8 Financing Sources and Expenditure Schedule 4.8.1 Project implementation shall cover a period of five years, in accordance with the list of goods and services presented in Annex 6 and the expenditure schedules by component and by expenditure category respectively presented in Tables 4.6 and 4.7 below:
26
Table 4.6 : Expenditure Schedule by Component (in UA million)
COMPONENT 2006 2007 2008 2009 2010 Total
Improving access to quality health services 1.07 4.97 08.84 0.90 0.90 16.68
Promotion of mother/child health and disease control 0.53 2.14 01.68 1.22 0.53 06.09
4.8.2 The expenditure schedule by financing source is presented in the following table:
Table 4.8 : Expenditure Schedule by Financing Source (in UA million)
FINANCING SOURCE 2006 2007 2008 2009 2010 Total
ADF – loan 1.83 6.68 9.74 2.18 1.57 22.00
GOVERNMENT 0.21 0.75 1.09 0.25 0.18 2.47
TOTAL 2.04 7.43 10.83 2.43 1.74 24.47
5. PROJECT IMPLEMENTATION 5.1. Executing Agency 5.1.1 The management of project activities shall be entrusted to an autonomous structure. The creation of this new structure can be justified by several reasons. There is no pre-existing unit for an ongoing project supported by the Bank in the health sector that could have managed the current project. Furthermore, donors have not set up a common coordination structure to implement the various projects in the sector, at the national level or within the project area. Besides, administrative bottlenecks and the involvement of several departments of the Ministry of Health in project implementation raises fears that activities will be poorly coordinated if the project were entrusted to any of these departments. Indeed, project activities cover the areas of intervention of the following departments in the Ministry: the Health Zone Development Support Unit; the Infrastructure, Equipment and Maintenance Department; Department of Basic Hygiene and Sanitation; the National Directorate of Sanitary Protection; the Department of Family Health and the Department of Human Resources. All the above reasons justify the setting up of the Project Management Unit. 5.1.2 Considering the limited efficiency of public institutions, administrative bottlenecks and the burden of priority diseases on the population, project management will be based on the principle of contracting. Consequently, the Project Management Unit will give priority to multisectoral partnerships that bring together the State, the private sector, civil society, community-based
27
organizations, training institutes and other entities that will make it possible to build the capacity of State structures and speed up implementation of project activities. Only an autonomous structure can efficiently play this role. 5.1.3 The PMU staff shall comprise a coordinator, a procurements expert, an expert in participatory community development, a mutual fund management expert, a human resource expert, an infrastructure specialist, an administrator-manager, an accountant and an administrative assistant. The composition of the coordination team is justified by the complexity and volume of activities and the diversity of field actors involved in project implementation. The expert in participatory community development planning shall ensure the overall coordination and supervision of NGOs and other community actors involved in social mobilization on hygiene, disease control, promotion of mother/child health, development of mutual funds and institution of a healthcare system for indigent patients. The mutual funds expert will lend the necessary methodological support to NGOs and facilitate the process of setting up and sustaining mutual funds. One month after recruitment of the Coordinator, the Government shall submit his draft performance contract to the ADF for approval. The Government shall conduct the performance evaluation process annually and forward its results to the Bank by 31st March of each year, latest. 5.1.4 Given the scope and diversity of operational activities, the PMU shall be based in Bohicon and shall depend on teams from the departmental directorates of health and health zone management teams to coordinate the implementation and monitoring/evaluation of activities on the field. The choice of Bohicon in Zou Department as project headquarters stems from the construction of two zonal hospitals in this department compared to one in Donga and its larger population (618,192 inhabitants) compared to Donga (325,930 inhabitants). The volume of activities in Zou is therefore higher than in Donga. Furthermore, the relative proximity of Bohicon to the city of Cotonou will facilitate trips that PMU officials will certainly have to make for various administrative reasons, even though there are plans to set up an office in Cotonou to ensure administrative follow-up and maintain links with the central level. The said office shall be manned by an administrative assistant and shall be located within the DPP which serves as the Permanent Secretariat of the Project Steering Committee. The organization chart of the project management unit is found in Annex 7. 5.1.5 A procedures manual shall be drafted, which will include provisions to guide the project management unit on the implementation and monitoring of its activities. On the whole, the PMU will be responsible for the planning, coordination, financial management, contracting and monitoring of activities. It shall ensure that close cooperation and regular consultation is established with the various partners of the project, notably NGOs and civil society structures. It shall, on a regular basis, obtain information on the activities conducted by the other development partners in the project area. Lastly, the PMU will coordinate relations between the Government and the ADF. To that end, it shall be responsible for preparing quarterly status reports, monitoring the drafting of annual audit reports, mid-term review reports and project completion reports and the forwarding of such reports to the Bank. The procedures manual shall also outline the performance criteria for PMU staff. 5.2 Institutional Arrangements 5.2.1 At the central level, the Project Management Unit shall be placed under the authority of the Secretary General of the Ministry of Public Health. A Tripartite Steering Committee (State, private sector, civil society) shall be set up and will include representatives of the MCPFD (1), MFE (2), MPH (3, including the DPP), MPSL (1), MFSWS (1), MEHTP (1), the representative of sector partners (1), denominational private sector (1), and civil society (2 including one women’s
28
association). This committee shall meet twice a year to monitor project implementation and propose solutions to problems encountered; its secretarial services shall be provided by the DPP. 5.2.2 At the intermediate and peripheral levels, the two departmental directorates of health in Zou/Collines and Atacora/Donga as well as the zonal management teams shall be the direct technical partners of the PMU. The management and community participation structures (Board of Directors of the DGH, Governing Council, health committees and management committees) shall monitor the implementation of activities with the technical support of departmental maintenance services, the technical services of the DDPH and DGHs as well as zonal management teams. It will be necessary to hold meetings of all partners intervening in the project areas in order to ensure exchange of information and complementarity of training activities. 5.2.3 The implementation of sensitization activities and certain training courses will be entrusted to civil society structures and MFSWS staff who have better knowledge of the field and greater experience in the provision of community services. The MPH and MEHTP Departments could be key partners in the preparation of training and impact assessment modules for certain activities. The private sector could be invited to join in preparing the content of sensitization messages. 5.2.4 Activities to promote traditional medicine shall be placed under the responsibility of the Department of Pharmacy and Laboratories of the MPH. The management of activities to promote environmental hygiene shall be entrusted to the DHBS of the MPH. Under the contracting strategy, the DLM of the MPH shall guide and supervise actions carried out on the field by NGOs selected on the basis of their competence and experience in controlling priority diseases. 5.2.5 To facilitate execution and monitoring of construction work, a delegated project owner (DPO) shall be recruited through a competitive process among the structures existing in Benin. Indeed, there are 3 (three) structures that have agreements with the Government and act on its behalf as delegated project owners for the construction of infrastructure in rural and urban areas. They have proper procurement procedures that are acceptable to multilateral institutions. They recruit consultancy firms, technical control firms and enterprises through consultations and a bidding process. A contract shall be signed between the Government and the selected DPO. The DPO, acting in cooperation with the PMU, shall select the consultancy firms responsible for architectural and technical designs and preparation of bidding documents for construction work and select control consultancies. The consultancy firms selected shall also carry out supervision of construction work, draft instructions to contractors, prepare status reports and accept the facilities under the supervision of the DPO and the PMU. The control firms shall ensure the technical control of the works and construction material. The DPO shall provide the project accountant with all documents and reports in accordance with Bank regulations and procedures. Furthermore, he shall inform the PMU coordinator and the other institutions concerned of any difficulties encountered during implementation so that they can take the necessary corrective measures in time. 5.3 Implementation and Supervision Schedules Project implementation will cover 5 years. The projected implementation plan (details in Annex 8) is summarized below:
29
Table 5.1 : Projected project Implementation plan
ACTIVITIES DATES SERVICE IN CHARGE Approval by Board April 2005 ADF Entry into force December 2005 Government/ADF Project launching/start-up mission January 2006 ADF Preparation of bidding documents for construction work July 2006 to August 2006 UGP/DPO/consultancy Bidding for construction work September 2006 to December 2006 ADF/PMU/DPO Construction work/Equipment January 2007 to January 2009 ADF/PMU/DPO Procurement of furniture and equipment January 2006 to January 2009 ADF/PMU/UNDP Training/sensitization April 2006 to September 2010 MPH/MFSWS/PMU/NGO Mutual funds April 2006 to December 2009 PMU/NGO Mid-term review mission June 2008 ADF/ Government/ PTF Audit February 2007 to February 2011 PMU/audit firms Operation January 2006 to December 2010 ADF/ Government Government completion report December 2010 Government ADF completion report March 2011 ADF/ Government 5.4 Procurement Arrangements 5.4.1 The procurement arrangements are summarized in Table 5.2 below. All procurements financed by the Bank shall be made in accordance with the list of goods and services in Annex 6 and the Bank’s rules of procedure on procurement or, as the case may be, the Bank’s rules of procedure for the recruitment of consultants, using the relevant Bank standard bidding documents.
30
Table 5.2 : Procurement Arrangements (In UA Million)
In UA thousand EXPENDITURE CATEGORY ICB NCB Other Short list Total
1. Works * Extension of Borgou DGH 1.30 1.30 * Construction of zonal hospitals and offices (4.70) 4.70
Sub-total: Works 6.00 (4.70) 0.00 0.00 0.00 6.00 2. Goods * Medical furniture, equipment and instruments 3.74 (2.92) 3.74 * Specialty drugs + consumables and reagents (0.78)* 0.78 * Aerial communication network (0.56) 0.56 * Ambulances (0.28) 0.28 * Pick up and 4-wheel drive vehicles 0.14 (0.03) 0.14 * Motorcycles and bicycles (0.06) 0.06 * Office furniture 0.64 (0.61) 0.64 * Computer, office automation and audio-visual equipment 0.16 (0.14) 0.16 * Kits for village midwives, Educational material for EONC and IMCI, EONC equipment for maternities (1.58) 1.58 * Treated mosquito nets (0.41) 0.41 * Coartem and rapid diagnosis tests for malaria (2.11) 2.11 * Sanitation equipment (0.44) 0.44 * Medicinal plants (0.005)* 0.00
Sub-total: Goods 8.69 (7.87) 1.47 (1.27) (0.78) 0.00 10.91 3. Services * Para-medical training (0.79)* 0.79 * Medical training (0.92)* 0.92 * Training in planning and administrative management (0.20)* 0.20 * Training courses on mutual funds (0.06) 0.06 * Training of trainers in EONC and IMCI (0.17)* 0.17 * Sensitization campaigns and IEC (0.10) 0.10 * Appraisal studies/diagnosis and implementation (0.18) 0.18 * Studies and supervision of works 0.64 (0.47) 0.64 * Control of works (0.18) 0.18 * Works supervision by delegated project owner (0.34) 0.34 * Training/Promotion of MCH (0.04)]**** 0.04 * Training/Disease control (0.69)**** 0.69 * Mobilization activities (0.17) 0.17 * Preparation, monitoring & evaluation of IEC activities (0.22) 0.22 * Technical assistance for the PMU (0.19) 0.19 * Audit (0.04) 0.04
Sub-total: Services 0.00 0.00 0.00 0.00 (3.03) 2.13 (1.97) 5.16 4. Operations * Leasing of PMU headquarters (0.06)*** 0.06 * Monitoring & evaluation of comp. I activities by MPH (0.28)* 0.28 * Environmental management of activities by MEHTP (0.05)**** 0.05 * Monitoring & evaluation of comp. I activities by MPH (0.06)**** 0.06 * Missions to supervise activities by PMU (0.07)*** 0.07 * Headquarter missions (0.03)*** 0.03 * PMU staff allowances (0.70) 0.70 * PMU consumables (0.47)*** 0.47
Sub-total: operation 0.00 0.00 (1.01) (0.70) 1.71 5. Miscellaneous * Setting up of mutual funds (0.49) 0.49 * Payment of mutual fund contributions for the indigent (0.20) 0.20
Sub-total: Miscellaneous 0.00 0.00 0.00 (0.69) 0.69 Total project cost (in UA million) 14.69 (12.57) 1.44 (1.27) (4.87 ) 3.47 (3.29) 24.47
* Direct negotiation; ** National shopping; *** Operating expenses **** Direct agreement ( ) Loan financing
5.4.2 National laws and regulations governing the procurements system in Benin were examined and deemed acceptable. The Project Management Unit (PMU) shall be responsible for procurement arrangements. Procurements will be conducted as follows:
31
5.4.3 Works: (UA 6 million) International competitive bidding (UA 6 million) for the construction of zonal hospitals and offices; 5.4.4 Goods: (UA 10.91 million)
i) International competitive bidding (UA 8.69 million) for the procurement of: (i) biomedical furniture and equipment (UA 3.74 million); (ii) treated mosquito nets (UA 0.41 million); (iii) Coartem and rapid diagnosis tests for malaria (UA 2.11 million); (iv) ambulances (UA 0.28 million); (v) aerial communication network systems (UA 0.56 million) and (vi) educational material for EONC and IMCI and midwifery kits (UA 1.58 million);
ii) National competitive bidding (UA 1.44 million) for procurement of: (i) general
furniture for hospitals and the PMU (UA 0.64 million); (ii) office automation, computer and audiovisual equipment (UA 0.16 million); (iii) vehicles (UA 0.20 million) and (iv) sanitation equipment (UA 0.44 million). The maximum amount per contract is UA 200,000. The type and quantity of equipment to be procured may not interest external suppliers. Meanwhile, there are local suppliers who are sufficiently qualified to guarantee competition.
iii) Direct negotiation with:
a) CAME (UA 0.78 million) for the procurement of drugs, consumables and reagents.
CAME, a social and autonomous structure, is responsible for supplying drugs to health structures in Benin and is statutorily and effectively involved in combating illicit sale of drugs. The procurement procedures used by CAME comply with the fundamental principles supported by Bank policies on eligibility, transparence and economy. This institution also has unique expertise in the areas of procurement, evaluation, storage and supply of drugs. Consequently, CAME will be the agent responsible for acquisition of drugs, consumables and reagents for the project by using procurement procedures approved by the Bank;
b) The Department of Pharmacy and Exploratory Diagnosis in the Ministry of Public
Health for medicinal plant gardens (UA 0.005 million). This department has unique expertise in counseling and evaluation of traditional protocols and creation of medicinal plant gardens. The committed expenditure covers only the cost of medicinal plant gardens.
5.4.5 Services (UA 5.16 million)
i) Limited shopping (UA 2.13 million) for the selection of: (i) the delegated project owner to supervise construction and extension work (UA 0.34 million); (ii) consultancies to conduct architectural and technical studies, supervise construction work on zonal hospitals and offices and oversee extension of DGH-Borgou (UA 0.82 million); (iii) experts to provide training in mutual fund management (UA 0.2 million); (iv) specialists to implement IEC activities (UA 0.32 million); (v) experts to conduct diagnostic, evaluation and follow-up studies (UA 0.18 million); (vi) experts to give technical assistance to the PMU and project audit (UA 0.23 million); (vii) specialists in mobilization and sensitization actions, organization of radio
32
programs (0.17 million) and (viii) trainers and instructors for refresher and training workshops coordinated by the MPH and MFSWS.
ii) Direct negotiation (UA 2.3 million) with the IRSP, vocational training schools
(INMES and ENIIAB) and medical and maintenance training schools in the sub-region for: (i) medical training (UA 0.92 million); (ii) para-medical training (0.79 million); (iii) training of trainers in EONC and IMCI (UA 0.17 million); (iv) training in administrative planning and management (UA 0.20 million); and training in maintenance (0.22 million). These institutions are capable of providing the theoretical, practical and multidisciplinary training courses planned under the project. The Bank’s approval is required for the proposal of training institutions formulated by the PMU and the MPH.
iii) Direct agreement with the departments in the Ministry of Public of Health (UA 0.73
million): (i) Department of Basic Hygiene and Sanitation (DHBS) for the planning of hygiene and sanitation activities; (ii) the Disease Control Department (DLM) for the planning of priority disease control and STI/HIV/AIDS control activities; (iii) the Department of Pharmacy and Diagnostic Exploration for the training of 250 traditional healers. These departments have adequate expertise and wide experience in their respective areas of activity. The project will only fund real expenses (per diems, transport expenses, rent for premises, etc.) for the various activities conducted by the different departments. Direct agreements signed with these departments shall be submitted to the Bank for review.
5.4.6 Operations (UA 1.71 million):
(i) National shopping (UA 0.46 million) for PMU consumables as well as repair and maintenance of equipment and vehicles. The maximum contract amount shall not exceed UA 10,000;
(ii) Short list of individual consultants for the recruitment of PMU staff (UA 0.70
million). The selection procedure shall be based on a shortlist established after a study of applications;
(iii) Direct agreement (UA 0.39 million) with the Ministry of Public Health and the
Ministry of the Environment, Housing and Town Planning for monitoring and evaluation of project activities. Agreements shall be signed between the PMU and these structures and submitted to the Bank for review. The expenditure relating to these services only covers the cost of their production;
(iv) Rents for the headquarters in Bohicon and missions to supervise PMU activities (UA
(i) Limited shopping (UA 0.49 million) for NGO services to set up mutual funds and manage the contributions paid by the project for indigent patients (UA 0.2 million).
33
General procurement notice: The general procurement notice (GPN) adopted with the borrower during loan agreement negotiations will be issued for publication in Development Business, as soon as the loan proposal is approved by the Board of Directors. Review procedures: The following documents shall be submitted to the ADF for approval before they are published: specific procurement notices, shortlists and invitations to bid, bidding documents, bid evaluation reports containing recommendations to award contracts, and draft contracts if the contract models included in the bidding documents have been modified. 5.5 Disbursement Arrangements 5.5.1 ADF disbursements will be made in accordance with the expenditure schedule. To that end, a special account shall be opened in the Central Bank of West African States to receive project resources. A second account, destined to receive the Borrower’s contribution to project financing shall be opened in the Treasury. All transactions in both accounts shall be subject to the principle of double signature of the project coordinator and the project accountant. Each year, the Government shall make a timely contribution to the financing of activities planned for the current year. 5.5.2 Disbursements into the special account by the ADF will be used to finance recurrent expenditure covering 4 months activity for the project. Disbursement decisions shall be made on the basis of activity programs acceptable to the ADF and justification of the use of at least 50% of the previous disbursement, if necessary. With regard to direct payment of contractors, suppliers and consultants, this will be done in accordance with the normal Bank procedures. 5.6 Monitoring and Evaluation 5.6.1 A monitoring/evaluation system shall be set up that is based on analysis of the starting situation as well as the mid-term and project completion reviews. The starting data will be collected through surveys conducted at the beginning of the project. All structures involved in the project will then draft and forward quarterly and annual status reports to the PMU, in accordance with Bank guidelines. The PMU shall compile these reports, draft the synthesis report and forward it to the ADF and MPH. A mid-term review shall be conducted in the third year of the project. At the end of the project, the PMU shall draft and forward a project completion report to the ADF. To that end, the PMU coordinator and the procurements officer shall visit the headquarters of the Bank shortly after taking up duty, to learn about Bank procedures. Supervision 5.6.2 After approval of the loan, the ADF shall organize a launching and assistance mission to help the Government fulfill loan effectiveness conditions and conditions precedent to first disbursement. During the launching, a seminar shall be organized during which the roles of the various stakeholders will be defined. The ADF shall conduct periodic supervision missions (at least twice a year) to the different sectors and sites of the project. The teams for these missions shall be composed in such a way as to include multidisciplinary expertise (health, architecture, procurements, data processing, etc.) that address the various project components. Copies of the mission reports shall be submitted to the authorities so that the necessary measures can be taken. Mid-term review 5.6.3 A 3-week mid-term review shall be organized at the end of about 30 months of project implementation to appraise project implementation status in relation to its development objectives
34
and propose any corrective measures. It shall involve all parties involved in project implementation, notably the representatives of beneficiaries, civil society organizations and development partners. Furthermore, during portfolio reviews, project status will also be reviewed. The reports and conclusions of these missions shall be submitted to the project implementation organs which shall take the appropriate measures. The schedule for supervision and mid-term review missions is presented hereunder:
Year Type of mission Number of missions Composition of missions
5.6.4 The mid-term review shall be conducted according to the following indicators:
Indicators Intermediate indicators 2008 Indicators at project end 2010 1. Referral and counter-referral
- 50% of construction work done - Contracts concluded for drugs, furniture and equipment.
- Construction completed 100% - 100% of goods supplied
3. Mutual funds and coverage of indigent patients
- 4 persons at the central level and 1 per health zone trained in mutual fund management - 10 sensitization campaigns conducted on mutual funds - At least one mutual fund set up in each of the 15 districts selected
- 20 sensitization campaigns conducted - At least 27,768 members and 6,942 indigent patients covered financially in the 15 mutual funds (3/district)
2. Staff capacity building
- 100% of trainees in long specialization courses are completing the 1st year - 3 members per EEZ trained in human resource management, financial and material resource management, supervision and monitoring - 20 trainers trained in EONC and IMCI, 10 in RH/FP - 410 health workers trained in EONC, 360 in IMCI - 125 malariologists trained
- 20 sensitization campaigns conducted on STI/HIV/AIDS, malaria, family health, hygiene and environmental sanitation - 360 radio programs broadcast
8. Training of members of the community
- 360 members of COGES trained in budget planning, management of contracts with mutual funds and the private sector in the area of maintenance - 5 local private healthcare providers per health zone work within the framework of contracts signed with the management committee - 626 village midwives trained in mother/child health techniques, STI/HIV/AIDS - 100 members of women’s associations trained in the management of mosquito net tontines - 1000 mothers trained in the home treatment of fever presumed to result from malaria
- 520 chat sessions organized with the communities - At least 60% of malaria cases treated correctly in the health centers of the project area - The curative consultation rate is 60% in Zou and 50% in Donga - The PNC coverage rate is 90% in Donga
- 250 traditional doctors trained in sensitization techniques and the psychosocial management of HIV/AIDS, diagnosis and treatment of simple malaria and referral of serious malaria - 360 community relay agents trained in hygiene and sanitation - 75 masons trained in the construction/maintenance of latrines
- The obstetrical coverage rate is 70% in Donga and 90% in Zou
5.7 Financial and Audit Reports 5.7.1 As soon as the activities start, an accounting firm shall set up an accounting management system that is compatible with the project components. The administrator manager of the project shall prepare the financial reports and keep an updated accounting system according to expenditure category, component, financing source and currency type. To that end, it shall be provided with the appropriate Bank manuals, notably “The Guidelines on the Drafting of Financial Reports and Auditing of Project Accounts” and “The Disbursements Manual”.
35
5.7.2 The accounts of the project shall be audited annually by an external and independent firm selected from a shortlist previously approved by the Bank. The auditor shall exercise technical and financial control by having access to the general accounting of the project and the specific accounting of technical partners involved in the project and supported by agreements (mutual funds, MOD). The audit reports shall be submitted to the Bank within a maximum period of six months after the close of the accounting year. Recommendations shall be made to national officials in charge of project implementation to enhance management of activities and bookkeeping. 5.8 Coordination of Assistance The Ministry of the Economy and Finance coordinates all donor interventions in the country. With regard to the health sector, the partners set up a consultation framework headed by the Swiss Cooperation Office. During the identification, preparation and appraisal missions, the Bank held meetings with health sector partners to have them validate the actions it intends to implement under the current project. In the design of the project, the presence of the leader of the donor community on the steering committee is justified by the Bank’s concern to reinforce the consultation framework. Furthermore, the PMU shall regularly report to the donor community on project activities. All these measures prepare the ground for the Bank’s future participation in lending budget support to the health sector, all the more so since the DPP, which serves as the permanent secretariat of the project steering committee, is the Government’s privileged link with partners in the planning and monitoring/evaluation process of health interventions. At the departmental level, the PMU will strengthen collaboration with the other partners and develop initiatives to create a consultation framework at the local level. 6. SUSTAINABILITY AND RISKS OF PROJECT 6.1 Recurrent Expenditure 6.1.1 Project implementation will generate recurrent expenditure amounting to an annual estimate of CFA.F 190,130,000. The breakdown of this amount is as follows: CFA.F 140,730,000 for maintenance of infrastructure, furniture and equipment; CFA.F 38,400,000 for allowances paid to project staff; CFA.F 3,000,000 for the operating expenses of 3 zonal hospitals, the 3 zonal offices and the extension of DGH-Borgou; CFA.F 143,600,000 to pay contributions of indigent persons in mutual fund; and lastly CFA.F 6,500,000 for monitoring and evaluation of disease control and MCH promotion activities. 6.1.2 The cost of training administrative staff, members of management committees and beneficiary populations shall all be borne by the project. Such costs will not become recurrent expenditure at the end of the project since the training courses are programmed to address capacity-building problems over a period of 5 years. The teams that have been trained will completely take over training in the structures concerned (health structures, MPH, civil society organizations). 6.1.3 The recurrent costs of the project shall be borne by the Government. Indeed, these recurrent costs which amount to an annual sum of UA 0.251 million, represent only 0.035% of the State’s operating budget and 0.4% of the budget allocated to the health sector for 2004. Furthermore, the Government is benefiting from HIPC (Heavily Indebted Poor Countries) resources which constitute an additional contribution that helps to defray recurrent expenses. Moreover, the cost-recovery system based on the billing of medical services and the purchase of essential and generic drugs by users generated CFA.F 3,656,000,000, representing 29% of the operating budget (excluding personnel expenditure) of the Ministry of Public Health (CFA.F 12,692,000,000). The improvement of the health system management capacity within the framework of decentralization
36
will enable local councils and communities to participate in the maintenance of equipment and facilities. 6.2. Sustainability of Project 6.2.1 The concerns of all health sector actors and partners were taken into account during project design and formulation. Arrangements have been planned to also ensure their participation in project implementation through community actors, management committees, NGOs and the steering committee. Such participation of the various stakeholders will encourage their ownership of the project and so ensure its sustainability. Investing human resource training will help to enhance the quality of medical staff and so have a positive impact on the quality of health services. In addition to developing their own personal skills, all those trained in the various specialties will henceforth constitute potential trainers thereby guaranteeing continuity in the transfer of knowledge and good professional practices. The constructed hospital infrastructure and the equipment will serve for several years as a result of better maintenance provided by the management committees; hence, they will contribute for a long time to the improvement of the people’s health. Furthermore, community and private sector participation in the implementation of activities will promote ownership of project achievements by the people and ensure project sustainability. 6.2.2 Promoting greater use of health services through mutual funds and provision of financial coverage to indigent patients will have a positive impact on the general health status of the people, and help to increase national production. The financing of a mutual fund program by the project for a certain period of time will give the population enough time to develop confidence in risk-sharing. Such confidence in the system will lead to an increase in membership, thereby laying the foundation for the mutual funds to become self-financing at the end of the project. Indeed, the more the membership grows, the greater the possibilities for the funds to be self-financing and sustainable. However, while the funds stand a great chance of attaining self-financing capacity through a growing membership, ensuring sustainable financial coverage for indigent members will depend on better (decentralized) management of credits allocated to that end by the Government. 6.2.3 The mutual fund unit within the DNPS, to be set up with project financing, will gain experience in the coordination of mutual fund programs thanks to the technical assistance of the mutual funds expert in the PMU. The same shall apply to community mutual fund management organs. This wealth of experience acquired during the project execution phase will ensure sustainability of activities once the project comes to an end. With regard to the financial coverage of indigent patients, the Government will continue providing such financing by increasing the credits voted annually for that purpose. The decentralized management of such financing will be improved through various other experiences, including that of the project and of the actors involved in the management of indigent patients. 6.2.4 Benin benefits from debt forgiveness under the Heavily Indebted Poor Country (HIPC) Initiative. Accordingly, CFA.F 5.8 billion was allocated to the Ministry of Public Health in the national budget for 2004 out of a total projection of CFA.F 16.7 billion (Report of the joint mission to review budget support, September 2004). This annual financial endowment, which is likely to continue, will help to cover expenses relating to the effects of the project after cessation of ADF financing, especially as a large proportion of HIPC financing is allocated to management committees to cover subsidies for certain categories of health sector beneficiaries, especially the indigent.
37
6.3 Main Risks and Mitigative Measures 6.3.1 One of the main risks of the project is failure to implement the findings of the study on human resource development in disadvantaged areas. Indeed, the newly constructed and equipped infrastructure as well as the ambulances and ACN systems cannot improve on the management of referrals if there is no competent staff. This risk is mitigated by the determination of donors who give priority to this study and the implementation of its findings. Moreover, the current application of alternative measures by the Ministry of Public Health, such as the signing of a notarial agreement requiring staff to serve in disadvantaged areas, also attests to the Government’s determination to forge ahead in solving this thorny human resource problem. 6.3.2 The low absorption capacity of the Ministry, as evident in the low budget execution rate for 2004 after delegation of credits to departmental directorates of health and health zones, also appears to be a risk factor. This low capacity was identified by the joint partners-Government budget support review mission and recommendations were made to put monitoring mechanisms in place that will make it possible to improve budget programming and management at the central and decentralized levels. Training in financial and material resource management, provided for under the project, will also help to mitigate this risk. 6.3.3 The low attendance in health structures, mainly due to financial reasons, also constitutes a risk in the realization of project objectives. The study on the billing system planned by the Government will mitigate this risk by proposing rates that are more commensurate with the production cost of medical services and the purchasing power of the people. 6.3.4 Successful implementation of project activities will also depend on the level of community participation. Indeed, community-based health services, notably services promoting mother/child health and disease control can only have an impact on health status if they are used by the population. Sensitization actions carried out under the project and the execution of such services by community members themselves will mitigate the risk of low utilization of community-based health services. 6.3.5 Low membership in the mutual fund program is a major risk that could undermine attainment of project objectives. A steady growth in the number of contributors will not only guarantee the system’s sustainability, but also improve health status through greater use of health services by mutual fund members. To mitigate this risk, the project plans to organize a major drive to explain and raise public awareness through the media so that people can consciously sign up for the mutual fund program. This explanation and sensitization drive will also mitigate another potential risk of the reticence of contributing members when they notice that the contributions of indigent members are paid by the project. Furthermore, the definition and application of rigorous criteria for the selection indigent persons, involving the management committees, local NGOs and social welfare services will also help to mitigate this risk. Similarly, the manifest political will of the Government to forge ahead with decentralization of budget management reduces the risk of an eventual cessation of State subsidies to indigent persons. 7. PROJECT BENEFITS The project has many social and economic benefits, which include: (i) contributing to poverty reduction, especially in rural areas; (ii) improving the health status of the people; and (iii) encouraging good governance.
38
7.1 Economic Impact 7.1.1 The project contributes to poverty reduction through its different activities, since it falls in line with the PRSP. It contributes to the attainment of PRSP objectives, notably increasing access to social services and enhancing their quality. From the economic standpoint, the project will contribute to poverty reduction, especially in rural areas. Indeed, financial resources will be injected into Benin’s economy through the investments that will be made. The private sector will be the main beneficiary, notably through the conduct of architectural and technical studies, implementation of construction work and procurement of goods. Consequently, there will be job creation, greater consumption of goods and services and the long-term effects of human investment through the training of beneficiaries. Small and medium-sized enterprises will win contracts and create jobs. The involvement of local private service providers in the maintenance system will generate additional revenue for this segment of the labor force. The improvement of the health sector management system will serve as an example of good governance in the country and a factor for generating savings and increasing the effect of investments. 7.1.2. Furthermore, the project will contribute to human resource development in Benin. Indeed, the country has to build its human resource potential as a factor for economic and social development, which are crucial to participation in international trade in this era of globalization. Upgrading the skills of the labor force will give rise to new types of jobs that are tailored to the needs of the national, regional or international markets, thereby helping to reduce poverty. 7.1.3 The promotion of hygiene and the control of diseases such as malaria and STI/HIV/AIDS, will help to reduce the number of disease episodes and new HIV infections. The number of avoided episodes of disease, especially for malaria, translates into an equivalent number of working days gained and consequently an improvement in agricultural productivity, especially as malaria is rife during the farming season. HIV/AIDS is a major obstacle to economic development since it affects the most productive segment of the population, thereby aggravating the poverty situation in households and communities. Labor force productivity and growth decline while health expenses skyrocket. The preventive actions envisaged under the project will help to mitigate such risk. Similarly, activities that target women’s associations will increase the income of women. Furthermore, the improvement of infant health will enable women to save part of their resources since they generally bear the healthcare expenses of their children. It will also give them free time to take up economic activities. Furthermore, the reduction of infant mortality from 89 per 1,000 in 2001 to 75 per 1,000 by 2010 will make it possible to save the lives of 121,137 children aged below one year (considering that the population growth rate is 3.25% per year), which corresponds to a life expectancy at birth of 59 years, representing a gain of 7,025,946 potential life years. 7.2 Impact on Women 7.2.1 Apart from its economic benefits, the project will have many social benefits for women. Indeed, it will provide 394,385 women of childbearing age in the project area (23.64% of 1,668,293 inhabitants) with cheap and efficient health services which they could not afford in the past, through the community health services that will be developed by the project as well as the mutual fund program and the financial coverage system for indigent patients. In fact, membership of the mutual fund covers the entire family and it has been decided that the majority of indigent members whose contributions will be paid by the project will be women. The consequent greater use of maternity services will reduce maternal mortality and improve the sexual health of girls and women. In particular, female genital mutilation and complications of poorly managed deliveries such as fistulas will decline, hence easing the psycho-social burden borne by individuals and families with regard to the social marginalization of women with fistulas. Family planning services
39
will help women to manage their births better. In Donga, one of the departments with the lowest maternal health indicators in the country, 90% of pregnant women will have access to prenatal consultation services and 70% of them will give birth under technically acceptable conditions. In Zou department, obstetrical coverage will attain 90%. 7.2.2 Apart from the above health benefits, the training given to health staff and members of the community will also benefit women. The increase in the number of female medical specialists and service providers will boost the social standing of women in Benin society. 7.3 Social Impact 7.3.1 The entire population of Borgou, Donga and Zou, representing 1,668,293 inhabitants, will benefit from efficient health services with: (i) the training of qualified staff in the areas of health, management and maintenance; (ii) the construction and equipment of three zonal hospitals and expansion of the DGH in Parakou; and (iii) the supply of drugs and laboratory reagents. In particular, the technical quality of healthcare will be improved through the training of 5 physicians per specialty in surgery, pediatrics, obstetrics/gynecology and anesthesia/resuscitation. Surgical and obstetrical emergencies will be better managed through the supply of 5 ambulances and 5 aerial communication network systems. 7.3.2 The community-based health services, mutual funds and the subsidy system for the indigent will lead to an increase in the use of health services and a consequent improvement in the general health status of the population. All inhabitants of the project area will benefit from community-based health services provided by 626 trained village midwives, 626 trained community relay agents, 1000 trained mothers and 250 trained traditional healers. Overall, about 944,122 persons in Donga and Zou will benefit from communication for behavior change activities carried out by these community actors in the areas of hygiene, STI/HIV/AIDS and malaria. To combat malaria, 187,500 treated mosquito nets will be disseminated through the community distribution network, mainly for the protection of pregnant women and children under 5. Community participation in health center management will be strengthened through the training of 360 members of management committees. The inhabitants of Donga and Zou will also be influenced by health coverage benefits that will accrue to the 34,710 members of mutual funds set up by the project. This will steadily increase the number of potential candidates for mutual fund membership, thereby reinforcing the health coverage, the sustainability of the mutual fund system and the subsidy system for indigent persons. Indeed, the greater the membership of the mutual funds, the greater the possibility of ensuring the system’s sustainability and the greater the profits that can be used to subsidize healthcare for the indigent. 8. CONCLUSIONS AND RECOMMENDATIONS 8.1 Conclusions
This project, whose preparation stages are presented in Annex 9, constitutes significant support for the implementation of the Government’s health policy. The outcome of the project will help to improve the health status of the population in general and of women and children in particular. Hence, the project is a major step towards attainment of the millennium development goals. The likelihood of all the project activities being implemented will be increased by the fact that project design and formulation was based on a participatory approach that ensured the effective involvement of the various stakeholders (beneficiaries, Government, civil society, NGOs) and close consultation with technical and financial partners of the health sector in Benin. Furthermore, the
40
lessons drawn from the Bank’s experience in the health sector were taken into account in the definition of the project management module and in the technical and institutional measures that had to be adopted to guarantee excellent performance. 8.2 Loan Recommendations and Conditions 8.2.1 In the light of the foregoing, it is recommended that an ADF loan not exceeding UA 22 million be awarded to the Government of Benin for implementation of the project described in this report, subject to the following special conditions: A. Conditions Precedent to Loan Effectiveness 8.2.2 The loan agreements shall become effective, subject to the Borrower’s fulfillment, to the ADF’s satisfaction, of the conditions in Section 5.01 of the ADF’s General Conditions for Loan Agreements and Guarantee Agreements. B. Undertaking Prior to Disbursement 8.2.3 The Government shall undertake to institute a statutory framework for mutual funds in Benin, in conjunction with the main partners, prior to any disbursement of the loan (Paragraph 4.5.9 and 4.5.10). C. Conditions Precedent to First Disbursement 8.2.4 Besides the commitment and entry into force of the loan agreement, disbursement of the first loan tranche by the ADF shall be subject to the fulfillment of the following conditions by the Borrower, to the satisfaction of the ADF:
i) Provide the ADF with evidence of the creation of a Project Management Unit
(Paragraph 5.1.1) ; ii) Forward to the ADF, after the recruitment process, the list of persons selected to
occupy the positions of coordinator, procurements expert, participatory community development expert, mutual fund management expert, human resource expert, infrastructure specialist, accountant and administrative assistant within the PMU as well as the list of support staff; (Paragraph 5.1.3) ;
iii) Provide evidence to the ADF of the opening of a special account in BCEAO to
receive project resources and an account in the Treasury to receive national counterpart funds (Paragraph 5.5.1);
iv) Supply the ADF with administrative decisions allocating land for the construction of
three new zonal hospitals (Paragraph 4.5.4); and v) Provide evidence to the ADF of the creation of a steering committee responsible for
coordinating project activities, composed of representatives of the following structures: MCPFD (1), MFE (2), MSP (3), MPSL (1), MFSWS (1), MEHTP (1), development partners (1), denominational private health sector (1) and 2 from civil society (Paragraph 5.2.1).
41
D. Other Conditions 8.2.5 Furthermore, the Borrower shall:
i) Provide the ADF with the detailed program for all training courses together with the
list of candidates, training structures and periods, six months after setting up the PMU; (Paragraphs 4.5.11-4.5.14 ; 4.5.16 ; 4.5.17 ; 4.5.19 and 4.5.20) ;
ii) Forward to the ADF, 1 (one) month before departure of candidates, the notarial
agreements signed by scholarship beneficiaries in which they undertake to serve in project area for at least 5 (five) years; (Paragraph 4.5.11);
iii) Provide the ADF with a copy of the law governing health mutual funds in
Benin, not later than 31 December 2008; (Paragraph 4.5.9); iv) Forward to the ADF, one month after the Project Coordinator’s recruitment, the
performance contract signed between him and the Government, and whose terms and conditions shall have been previously approved by the ADF (Paragraph 5.1.3);
v) Forward to the ADF, not later than 31 March of each year, the results of the Project
Institutional support ATACORA, DONGA, MONO, COUFFO
5 408
German cooperation Institutional support, disease control, decentralization, family health
ZOU, COLLINES, BORGOU, ALIBORI
2 145
French Cooperation Institutional support, healthcare quality, mother and child health, disease control
Countrywide 298
Swiss Cooperation Institutional support, decentralization, family health
BORGOU, COLLINES, ATLANTIQUE
2 509
American Cooperation
Institutional support, family health, disease control
Countrywide 4 408
World Bank Institutional support, family health, decentralization, disease control
Countrywide 800
IsDB Institutional support ATACORA, OUEME, BORGOU, PLATEAU
970
ABEDA Institutional support ALIBORI, ATLANTIQUE, ZOU, LITTORAL, COLLINES, OUEME, PLATEAU
4 807
World Fund Malaria, HIV/AIDS, Tuberculosis
Countrywide 3 725
ANNEX II Page1/1
REPUBLIC OF BENIN HEALTH SYSTEM DEVELOPMENT SUPPORT PROJECT
(HEALTH III PROJECT)
ADMINISTRATIVE MAP OF BENIN AND PROJECT AREAS
Project areas
ANNEX III
Page1/1
REPUBLIC OF BENIN HEALTH SYSTEM DEVELOPMENT SUPPORT PROJECT
(HEALTH III PROJECT)
SUMMARY OF COORDINATOR’S TERMS OF REFERENCE
Under the aegis of the Secretary General of the Ministry of Public Health, the Project Coordinator shall:
i) Ensure the supervision, monitoring/evaluation and coordination of all project activities and the performance of all stakeholders;
ii) Ensure and encourage sound cooperation between the ministries, technical and
financial intermediaries and other partners involved in implementation;
iii) Ensure that the project staff efficiently perform their duties in compliance with the terms of reference, appropriate working methods and the agreed schedule;
iv) Prepare the annual program of activity and the budgets related thereto;
v) Ensure compliance with the project implementation schedule;
vi) Ensure the application of Bank rules in the procurement of goods, services and
works for the project;
vii) Keep accurate accounting records and make them available to the national counterpart;
viii) Maintain relations with the ADF for the preparation and regular transmission of all
documents relating to program activities (status and audit reports, payment requests, working capital requests and other correspondence).
Qualifications required: Candidates for this post must have the following qualifications:
- hold at least a postgraduate diploma in development planning or a medical diploma in public health; - have at least five years professional experience in the management of development
projects/programs with external financing; - be able to manage, guide and work with a team; - have confirmed experience in the use of computers; - have perfect knowledge of the country’s environment and the French language.
ANNEX IV Page 1/1
REPUBLIC OF BENIN HEALTH SYSTEM DEVELOPMENT SUPPORT PROJECT
(HEALTH III PROJECT)
SUMMARY OF SOCIO-ENVIRONMENTAL MEASURES
Description of the main socio-environmental components of the project To increase and improve access to quality health services, the project plans, inter alia, to construct and extend health infrastructure (3 zonal hospitals, 3 zonal offices and the extension of DGH-Borgou) including the construction of latrines and water points. Main socio-environmental impact The project is classified under environmental category II since it has minimal impact on the environment. Protection program and mitigative measures The project provides for measures to set up technical facilities such as incinerators and systematically decontaminate all used medical equipment before incineration to mitigate the negative impacts of contaminated hospital waste. Moreover, it shall be prescribed in the terms of reference for construction works that enterprises awarded contracts shall take measures to mitigate negative impacts or optimize positive impacts on the environment in the final execution of works. Monitoring program and additional initiatives The officials in the Project Management Unit and the regional offices of the MPH and the MEHTP shall be responsible for environmental monitoring. They shall choose project sites and material to avoid the felling of trees, erosion, gullying and water stagnation problems. The principle of periodic control will be developed in the terms of reference with an exhaustive list of the elements that will be evaluated on a regular basis. Institutional provisions and capacity building The project will, through a certain number of activities, provide the opportunity to raise daily popular awareness on environmental issues. The training component will comprise the promotion of environmental hygiene (body hygiene, washing hands before meals and after visiting the toilet, promotion and management of latrines, management of domestic waste). Public consultations and access to information It is important to involve the people in the design of infrastructure projects that concern them, through chat sessions before the start of construction work, and in the management of household garbage. The sessions will take place in the communities targeted by the project and will be open to everyone wishing to get informed and to NGOs operating in the project areas. The various status reports containing information on environmental protection activities, shall be accessible to the various partners involved in project implementation. Implementation schedule and reports Environmental monitoring will be done regularly and continuously since it is an integral part of project implementation. The quarterly status reports of the Project Management Unit and the supervision reports shall be produced in accordance with the project implementation schedule.
ANNEX V
Page 1/2
REPUBLIC OF BENIN HEALTH SYSTEM DEVELOPMENT SUPPORT PROJECT
(HEALTH III PROJECT)
SUMMARY OF DETAILED PROJECT COSTS
COMPONENT I : IMPROVING ACCESS TO QUALITY HEALTH SERVICES Total CFA.F million Total UA million
A/- Works - Extension of DGH - Borgou - Construction of two zonal hospitals in Zou - Construction of one zonal hospital in Donga - Construction 3 zonal offices
Basic cost Contingencies Price increases
Sub-total: Works
927.300
2 105.600 1 052.800
180.800 4 265.70
213.29 67.18
4 546.17
1.22 2.78 1.39 0.24 5.63
0.28 0.09
6.00 B/- Goods
- Equipment and furniture for extension of DGH-Borgou - Equipment and furniture for 3 zonal hospitals - Equipment and furniture for 3 zonal offices - Drugs, biomedical consumables and reagents - ACN - Vehicles
Basic cost Contingencies
Price escalation Sub-total: Goods
591.800
2 503.800 51.00
550.00 400.00 290.60
4 387.20 219.36 78.31
4 684.87
0.78 3.30 0.07 0.73 0.53 0.38 5.79
0.29 0.10
6.18 C/- Services
- Training / DGH-Borgou staff - Training/capacity-building for health zone staff - Training/mutual funds - Training/ Maintenance - Studies and supervision of works
- Technical control of works - Supervision by delegated project owner - Situational and appraisal studies
Basic cost Contingencies
Price escalation Sub-total: Services
252.00
1 064.54 39.15
155.55 454.57 127.97 241.01 130.00
2 464.81 123.24 43.65
2 631.70
0.33 1.40 0.05 0.21 0.60 0.17 0.32 0.17 3.25
0.16 0.06
3.47 D/- Operations
- Monitoring/evaluation of activities - Environmental monitoring of activities
Basic cost Contingencies
Price escalation Sub-total: Operations
200.00
37.50 237.5
11.9 0.00
249.38
0.31 0.02 0.01
0.33 E/- Miscellaneous
- Supporting the setting up of mutual funds - Subsidizing the contributions of indigent mutual fund members
REPUBLIC OF BENIN HEALTH SYSTEM DEVELOPMENT SUPPORT PROJECT
(HEALTH III PROJECT) SUMMARY OF DETAILED PROJECT COSTS
COMPONENT II : PROMOTION OF MOTHER/CHILD HEALTH AND DISEASE CONTROL
TOTAL CFA.F million Total UA million
B/- Goods - Promotion of mother/child health - Disease control
Basic cost Contingencies
Price escalation Sub-total: Goods
1 123.24 2 129.63 3 252.86
162.64 58.06
3 473.57
1.48 2.81 4.29
0.21 0.08
4.58 C/- Services
- Training for the promotion of mother/child health - Training for disease control - Communication for behavior change campaigns - Mobilization actions - Preparation, monitoring and evaluation of IEC program
Basic cost Contingencies
Price escalation Sub-total: Services
188.52 490.54
72.00 124.00 158.00
1 033.06 51.70 18.30
1 103.10
0.25 0.65 0.10 0.16 0.21 1.37
0.06 0.03
1.46 D/- Operations
- Monitoring of training and activities - Evaluation of malaria control and family health
SECRETARIAT GENERAL OF THE MINISTRY OF PUBLIC HEALTH
Hierarchical relationship
Cotonou Office
PROCUREMENTS EXPERT
INFRASTRUCTURE SPECIALIST
HUMAN RESOURCE EXPERT
COMMUNITY DEVELOPMENT EXPERT
ACCOUNTANT
Project Steering Committee
ADMINISTRATIVE ASSISTANT
Headquarters in Bohicon
Government Civil society
MUTUAL FUND MANAGEMENT EXPERT
ANNEX VIII Page 1/1
REPUBLIC OF BENIN HEALTH SYSTEM DEVELOPMENT SUPPORT PROJECT
(PROJET SANTEIII)
PROJECT IMPLEMENTATION SCHEDULE
ANNEX IX Page I/1
REPUBLIC OF BENIN HEALTH SYSTEM DEVELOPMENT SUPPORT PROJECT
(HEALTH III PROJECT)
APPRAISAL REPORT PREPARATION PROCESS
MAIN ACTIVITIES DATE COMMENTS
Identification mission: consultation of the people, opinion leaders, local elected representatives, civil society organizations, development partners and administrative authorities in Cotonou and in the Departments of Atlantique, Borgou,Ouémé and Zou
10-30 August 2004 Take the results of these consultations into account during project formulation
Preparation mission: consultation of local elected representatives, civil society organizations, development partners and administrative authorities in Cotonou
31 October-13 November 2004
Take the results of these consultations into account during project formulation Differences on the choice of part of the project area
Appraisal mission 10 –23 December 2004 Final formulation of project; Final agreement on objectives, components and project area
Drafting of the mission and appraisal reports 3 – 25 January 2005 Communication of mission findings to the Gov’t
Meeting of the internal working group 26 January 2005 Meeting comments taken into account for the drafting of the report for the interdepartmental working group
Meeting of the inter-departmental working group to examine the project appraisal report
11 February 2005 Meeting comments taken into account for the finalization of the report for submission to the Loan Committee
Meeting of the Senior Management Committee 25 February 2005 Meeting comments taken into account for the finalization of the report for submission to the Board of Directors
Forwarding of report to General Secretariat
ANNEX X Page1/1
REPUBLIC OF BENIN HEALTH SYSTEM DEVELOPMENT SUPPORT PROJECT