55
Approach to acute abdomen • Supervised by , • Dr.B.Faki • Presented by, • Eman Al.harbi
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| View: | 214 times |
| Download: | 0 times |
Approach to acute abdomen
• Supervised by ,
• Dr.B.Faki
• Presented by,
• Eman Al.harbi


Introduction
defined as any clinical condition characterized by severe abdominal pain which develops over a period of 8 hrs. In pt who have been previously well.
rapid and accurate diagnosis is essential for morbidity and mortality process .
Pathophsiology
Visceral pain; due to stimulation of visceral afferent nerve plexus usually in midline result from contraction or distension against resistance & chemical irritation
usually colicky in nature .
Pathophsiology
• Parietal pain; 2dry to partial peritoneum irritation perceived through segmental somatic fibers reflex involuntary muscle wall rigidity may result from irritation of segmental sensory nerves.
• Hyperesthesia of the skin may be result from ipsilateral peritoneal irritation usually a sharp ache.

Abdomen

Epidemiology

Abdominal quadrant

Causes
• Gastrointestinal tract*•Acute appendicitis
•Meckl”s diverticulitis• bowelPerforated
ulcer Perforated peptic obstruction Small and large bowel herniaStrangulated DiverticulitisGastritisGastroenteritisInflammatory bowel disease lymphadinitis Mesenteric

spleen. and , liverBiliaryTractsCholangiti acute Cholecystitis acute Hepatic abscess tumor Ruptured hepatic
spleen Ruptured biliary colic , Hepatitis acute infarct Splenic
PeritoneumIntra-abdominal abscess*Primary peritonitisTuberculosis peritonitis
PancreasPancreatitis, acuteca pancreases
Urinary TractCystitis acutePyelonephritis acuteRenal infarctteral colicUre
Gynecological ;ruptured ectopic pregnancyRuptured ovarian follicular cystTwisted ovarian tumorDysmenorrhealEndometriosisacute salpingitis.PIDs

• Male reproductive tract. • Prostatitis • Cystitis• Torsion of testes• Vascular causes Acute ischemic colitis .
Mesenteric thrombosis*Ruptured arterial aneurysm*
Medical causes
• Pneumonia. • Myocardial infarction• Sickle cell crisis.• DKA• Leukemia• Herpes zoster• psychogenic

Approach to acute abdomen
• History.
1 .pain
2 .Associated symptoms, nausea, vomiting,
Change of bowel habitués, jaundice, anorexia,
Heamatemsis, melena, dyspepsia
3.Menstruatin & sexual history .

Cont..
• 4.ROS
• 5.past medical & surgical hx
• 6.hx /o medications
• 7.familay Hx
• 8.social Hx

Eg
• Acute appendicitis, constant ,progressive more severe start per umbilical move toward RIF.+ nausea, vomiting, low grade fever, anorexia &/or constipation.
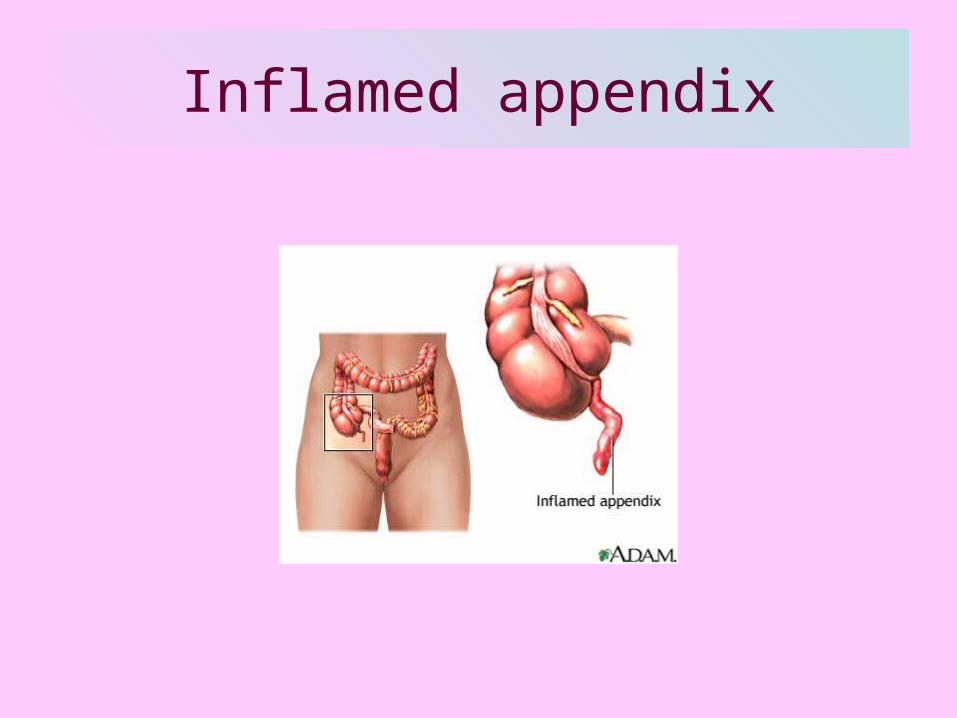
Inflamed appendix

•Acute cholecytitis
• Constant moderate pain in RUQ radiated to Rt shoulder tip + nausea, bilious vomitus, low grade fever & jundice

• Perforated peptic ulcer,
• Sudden onset of pain in midepigastrium that spreads and is aggravated by movement; patient appears acutely ill and is reluctant to move; rigid abdomen; grunting respiration; bowel sounds absent

• Ectopic pregnancy, • Pain sudden, severe,persistent,following a
missed or abnormal period, typically epigastric; associated with hypotension and tachycardia
• Ovarian cystPain constant with sharp, sudden onset, usually in ipsilateral hypogastrium; may have nausea and vomiting following the pain.
• Pelvic inflammatory disease.
• Pain at end of or after normal menstrual period, bilateral lower quadrant pain aggravated by cervical manipulation; anorexia, nausea, and vomiting rare; possible cervical discharge; fever

• Urinary stone,
• Pain location changes with movement of stone, may radiate to testicle, groin of involved side, pain very severe; patient cannot get comfortable
Physical examination
• 1.general appearance, 2. Vital signs.
• 3.abdomial exam
• 4.rectal exam
• 5.pelvic exam (female pt)

?

investigation
• 1.CBCs,
• WBCs & differential.
• RBC & hct, degree of anemia & hemocon.
• Platelet count, evidence of cougalopathy.
• 2.electrolyte,
• (G, Na, K, Cl, Ca ,Mg, Po)
• Indicative of volume status, GIT loss,

.
•3.ABG,
•Indicate metabolic acidosis or alklosis. M.acidosis with generalized abdominal pain in elderly is ischemic colitis till proven other wise.

.
•4.liver function test •Bilirubin (D or ID), ALP elevation in biliary
obstruction & transaminase elevation in case of hepatocellular injury.
•5.RFT•Urea, creatinin elevation in renal
insufficiency •Serum albumin decrease in edema /
ascitis.
.
•6 .serum amylase
•Seen in pancreatitis although non specific may be elevated in mesenteric ischemia, perforated peptic ulcer, rupture ovarian cyst & renal failure. But lipase more sensitive.

.
•7.serum B_HCG
•Mandatory for all women in childbearing period.
•8.urinalysis
•See WBC RBC & casts.

Radiological evaluation
•1.CXR,
•Look for pneumonia, free gases under diaphragm .pleural effusion suggest sub diaphragmatic inflammatory process.

.
•2.abdominal Xray.
•)Erect & supine position(
• *bowel distension & air fluid level
•*bowel gas cut off vs air through rectum.
•*sentinel loop vs pancreatitis
•*abn calcification vs ch.pancreatitis,stone
•*pnumatosis vs omnious sign of dead gut.

Intestinal obstruction

.
•3.ultrasound,
•*hepatobiliray tree(stones,mass,thickining of the wall)
•*pancreases
•*kidney
•*pelvic organ
•*intrabdominal fluid collection

Gall stone\ appendicolith

.
•4.CT_scan
•Helpful in case of abdominal pain without clear etiology better in evaluation of abdominal oartic aneurysm.
•5.helical CT_scan
•Provide rapid cost effictive dignostic tool.
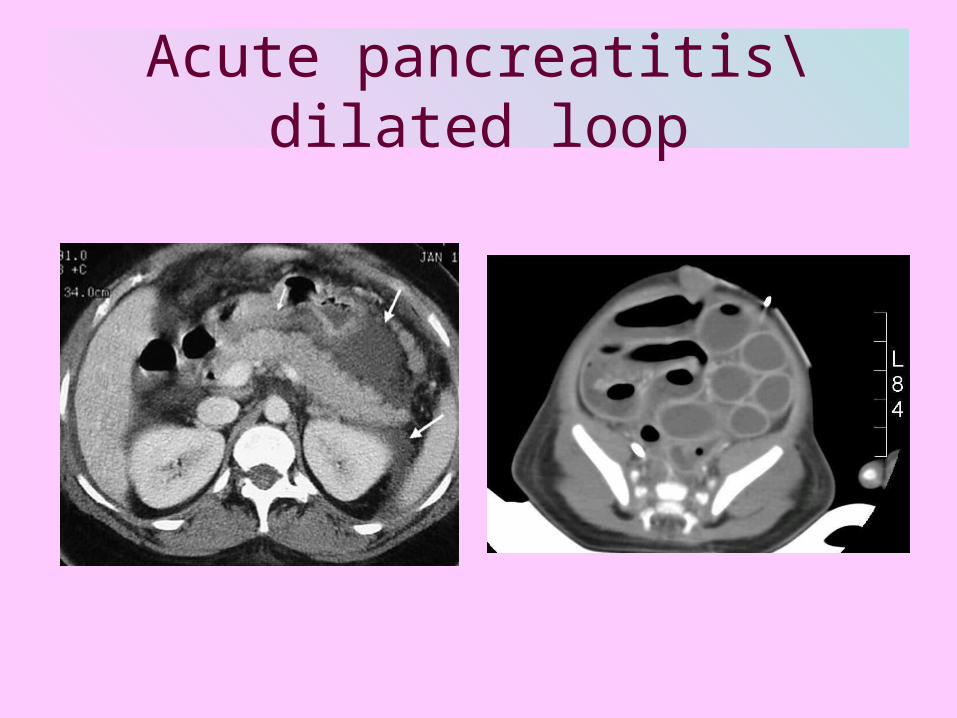
Acute pancreatitis\dilated loop

.
•5.contrast study
•A. barium study
•*perforation,
•*discering point of obstruction in small bowel.
•*avoid if colonic diverticuilitis is suspected

Multiple stones in CBD
.
•B_ intravenous pyelogram
•For dignosis of ureteral stone or obstuction
•C_angiography
•For mesenteric ischemia

angiograph

Other study
•6.endoscopy,
•EGE, for evaluation epigastric pain in non acute setting.& git bleeding
•Sigmoid\colonoscopy
•*colonic obstruction
•*dig IBD,ischimic colitis lower bleeding,
•*nonstrangulated sigmidal volvulus

ERCP

.
•7.paracentesis &\or peritoneal lavage
•*spontaneous bacterial peritonitis in cirrhotic pt
•*peritoneal lavage may be useful bedside test in diagnosis of mesenteric infarction in critically ill pt.

.
•8.culdocentesis
•Valuable in diagnosis of rupture ectopic pregnancy.
•9.laproscopy
•*D & ttt of suspected gynec.cause
•*appendectomy if appendicitis is found in a women in childbearing period .

laparoscopy

Plan of treatment
•*promote timely work up in first 4_6hrs.
•*keep pt Npo till the diagnosis is firm & ttt plan is formulated.
•*IV fluid. based in expected fluid loss.
•*heamodynamic monitoring.
•*NGT bleeding ,vomiting ,sign of obstruction or when urgent laparoscopy is planned in pt not NPo.

.
•Foley catheter to monitor fluid out put decisions
•Immediate surgery
• *what is the timing of operative intervention( does pt need time for resuscitation)
•*what incision should be used ?
.
• *what are the likely findings?
•*develop primary operative plan.
• *consider alternative diagnosis & plan.
• *use appropriate pre-operative antibiotic based on suspected pathology.
.
•2 .admit & observe for possible operation.•*serial examination every 2-4 hrs during
the first 12-24 hrs in case without definite diagnosis; minimal use of narcotics & sedatives to avoid masking physical sign & symptoms.
•*monitor vital signs frequently•*serial lab exam may be useful ;repeat
CBC every 4-6hrs .

.
•3.no operation develop ttt plan for further diagnostic workup or non operative therapy.

Case
36 yrs old female pt status post oratic valve replacement who present with one week hx of acute abdominal pain becoming severe over last 24hrs
O\E tachycardia, PR=145\min, B.P=100\45 temp=38. abd. Distended , rigid with moderate tenderness.wbc=23. amy=200 LDH=1500.

.
•What is mostly like diagnosis?
•What is the investigation of choice?
•Management plane?


.
Thanks

















