36
DR SREEKRISHNA R PG RESIDENT IN PAEDIATRICS MGM MEDICAL COLLEGE INDORE
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | sreekrishna-raveendran |
| View: | 183 times |
| Download: | 2 times |
DR SREEKRISHNA R
PG RESIDENT IN PAEDIATRICS
MGM MEDICAL COLLEGE INDORE
DIAGNOSTIC CHOICES ;Reliance on clinical v/s EEG seizures
ETIOLOGIC EXPLANATIONS; Multiple prenatal /neonatal conditions with variable time of onset and duration.
TREATMENT DECISIONS; WhICH,WhenAND HOW long
PROGNOSTIC QUESTIONS ;Mechanism of injury based on underlying disorder v/s vulnerability of
immature brain to seizures
Definition:-
A seizure is defined clinically as
a paroxysmal alteration in neurologic
function, i.e. motor, behavior and/or
autonomic function.
1.EPILEPTIC SEIZURE phenomena associated
with
corresponding EEG seizure activity e.g. clonic seizures
2. NON EPILEPTIC SEIZURE: clinical seizures
without corresponding EEG correlate e.g. subtle
and generalized tonic seizures
3. EEG SEIZURES: abnormal EEG activity with
no clinical correlation.
Immature CNS cannot sustain a synchronized, well orchestrated generalized seizure
Neurite outgrowth—dendritic and axonal ramifications—inprocess
Synaptogenesis not completeDeficient myelination in cortical efferent systems
CLINICAL CLASSIFICATION
SUBTLE SEIZURES;Clinical
manifestations are mild and often missed, most
common type
1. Ocular - Tonic horizontal deviation of eyes or
sustained opening with ocular fixation or cycled
fluttering
2. Oral–facial–lingual movements - Chewing,
tongue- thrusting, lip-smacking, etc.
3. Limb movements - Cycling, paddling, boxing-jabs,
4.Autonomic phenomena - Tachycardia or bradycardia
5. APNEA
CLONIC SEIZURESThey are rhythmic movements of muscle groups. They
have both fast and slow components, occur with a
frequency of 1-3 jerks per second
Tonic seizures:
refers to a sustained flexion or extension of axial
or
appendicular muscle group
MYOCLONIC SEIZUREsingle or multiple lightning fast jerks of limbs
Rapid speed
Absence of slow return and predilection for flexor muscle
groups
Myoclonic seizures carry the worst prognosis in
terms of neuro-developmental outcome and
seizure recurrence.
Focal clonic seizures have the best prognosis.
Jitteriness or tremors
Normal movements seen more commonly
in preterm infants
1. Benign neonatal sleep myoclonus
2. Fragmentary myoclonic jerks
3. Eye movements: Roving or dys-conjugate
eye movements
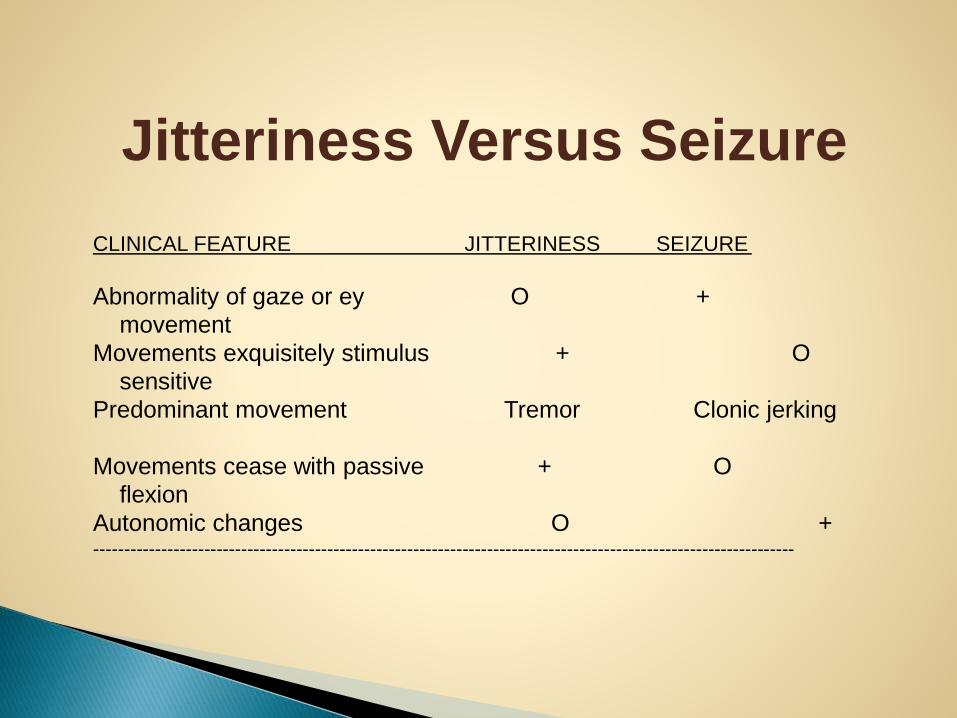
Jitteriness Versus Seizure
CLINICAL FEATURE JITTERINESS SEIZURE
Abnormality of gaze or ey O +
movement
Movements exquisitely stimulus + O
sensitive
Predominant movement Tremor Clonic jerking
Movements cease with passive + O
flexion
Autonomic changes O +------------------------------------------------------------------------------------------------------------------
Certain clinical seizures in the human newborn
originate deep cerebral structures (limbic
regions), or in diencephalic, or brain stem
structures and thereby are either not detected
by surface-recorded EEG or inconsistently
propagated to the surface
A. PERINATAL CAUSES
1. Neonatal encephalopathy
(hypoxic ishaemic) – 40 – 50 %
2. Intracranial hemorrhages- CNS
trauma, SAH, PVH,
Hypoglycemia Hypocalcemia – most common metabolic cause
for NNS Hypomagnesemia Hypo / Hypernatremia Pyridoxine dependency IEM - Disorders of amino acid metabolism
Intracranial
- Meningitis
- encephalitis – herpes, coxachie, echo, CMV,
- Toxoplasmosis,Rubella
Extracranial
– septicemia
- Tetanus
◦ Cerebral Dysgenesis
◦ Hydrocephalus
◦Microcephaly
◦ Neuronal migration defects-
Lissencephaly or pachygyria.
E.DRUGS-Narcotic withdrawal of mother
F.BENIGN FAMILIAL SEIZURE does not
continue after neonatal period
G.CEREBRO VASCULAR LESIONS
H.IDIOPATHIC 3- 25 %
DIAGNOSTIC
APPRAOACH
HISTORY EXAMINATION INVESTIGATION
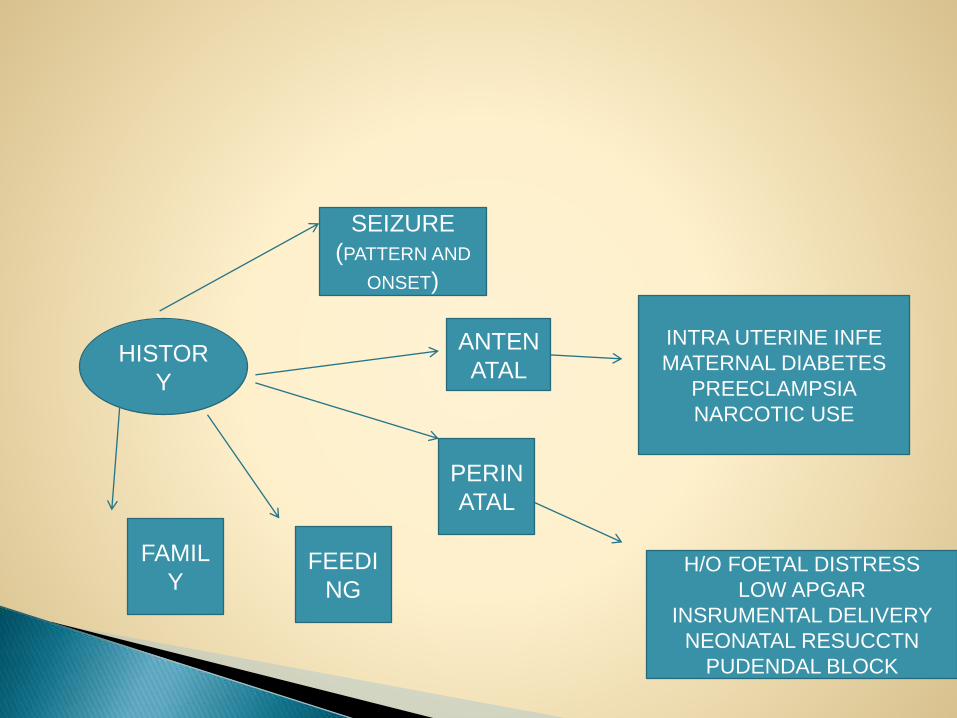
HISTOR
Y
SEIZURE
(PATTERN AND
ONSET)
ANTEN
ATAL
PERIN
ATAL
FEEDI
NG
FAMIL
Y
INTRA UTERINE INFE
MATERNAL DIABETES
PREECLAMPSIA
NARCOTIC USE
H/O FOETAL DISTRESS
LOW APGAR
INSRUMENTAL DELIVERY
NEONATAL RESUCCTN
PUDENDAL BLOCK
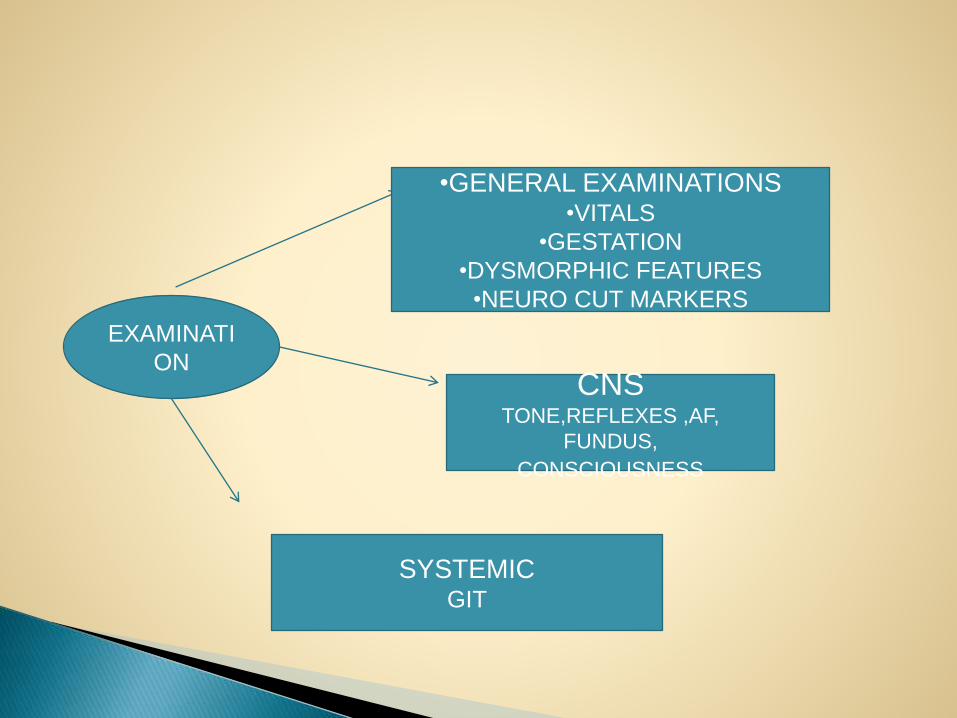
EXAMINATI
ON
•GENERAL EXAMINATIONS•VITALS
•GESTATION
•DYSMORPHIC FEATURES
•NEURO CUT MARKERS
CNSTONE,REFLEXES ,AF,
FUNDUS,
CONSCIOUSNESS
SYSTEMICGIT
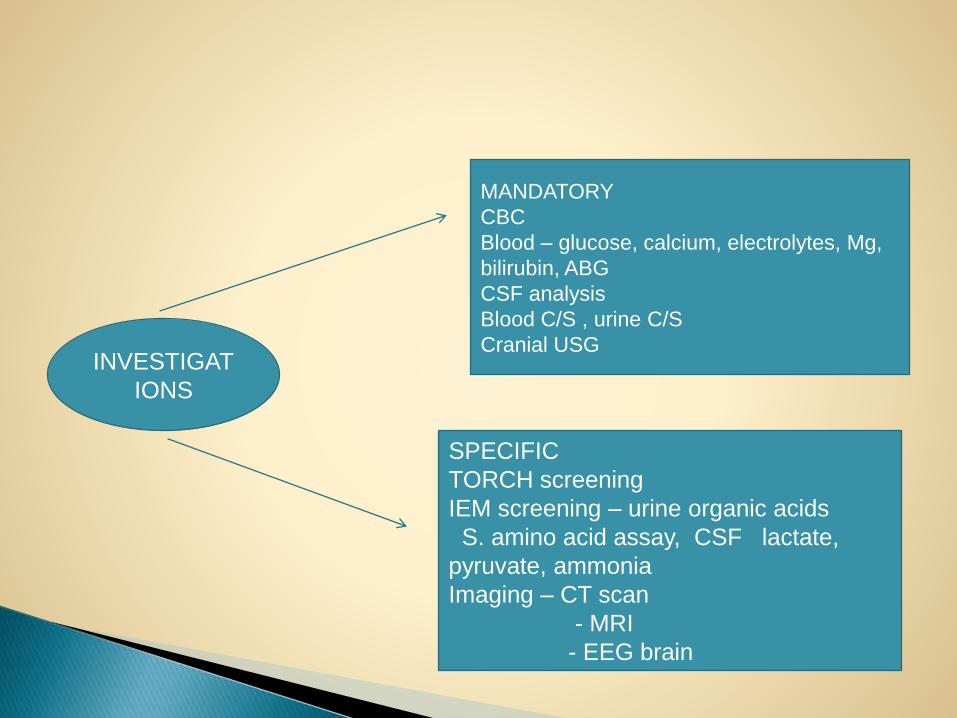
INVESTIGAT
IONS
MANDATORY
CBC
Blood – glucose, calcium, electrolytes, Mg,
bilirubin, ABG
CSF analysis
Blood C/S , urine C/S
Cranial USG
SPECIFIC
TORCH screening
IEM screening – urine organic acids
S. amino acid assay, CSF lactate,
pyruvate, ammonia
Imaging – CT scan
- MRI
- EEG brain
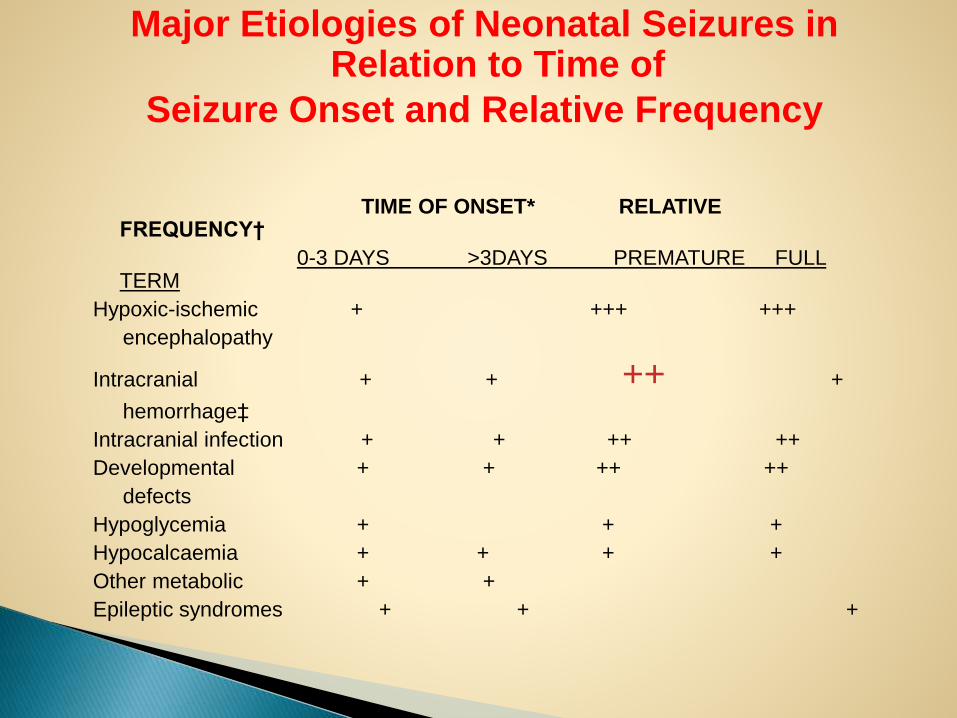
Major Etiologies of Neonatal Seizures in Relation to Time of
Seizure Onset and Relative Frequency
TIME OF ONSET* RELATIVE FREQUENCY†
0-3 DAYS >3DAYS PREMATURE FULL TERM
Hypoxic-ischemic + +++ +++
encephalopathy
Intracranial + + ++ +
hemorrhage‡
Intracranial infection + + ++ ++
Developmental + + ++ ++
defects
Hypoglycemia + + +
Hypocalcaemia + + + +
Other metabolic + +
Epileptic syndromes + + +
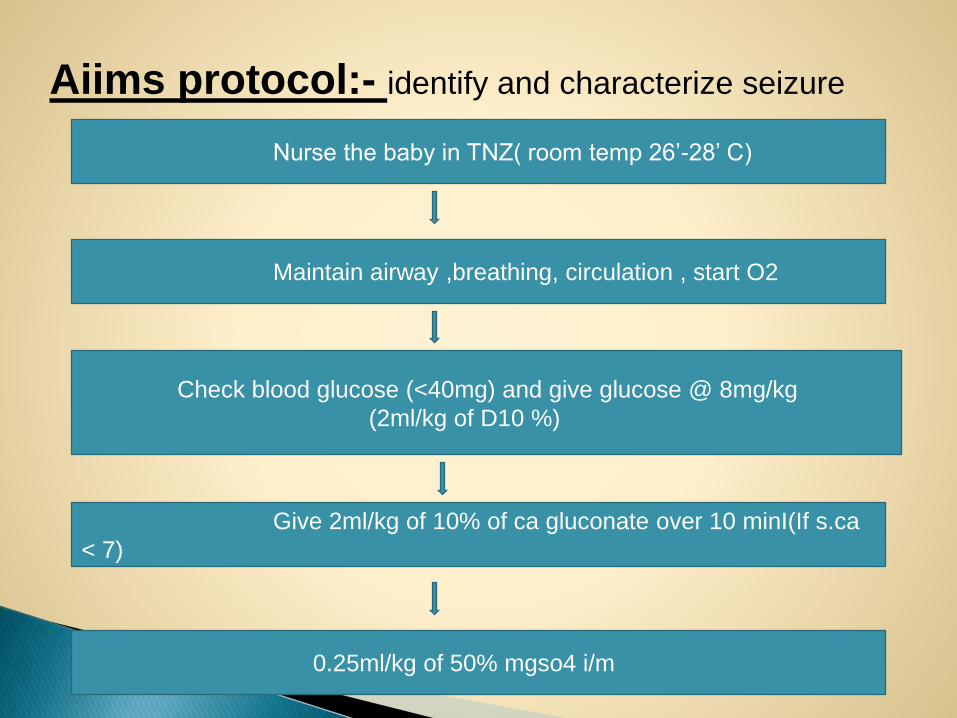
Aiims protocol:- identify and characterize seizure
Nurse the baby in TNZ( room temp 26’-28’ C)
Maintain airway ,breathing, circulation , start O2
Check blood glucose (<40mg) and give glucose @ 8mg/kg
(2ml/kg of D10 %)
Give 2ml/kg of 10% of ca gluconate over 10 minI(If s.ca
< 7)
0.25ml/kg of 50% mgso4 i/m
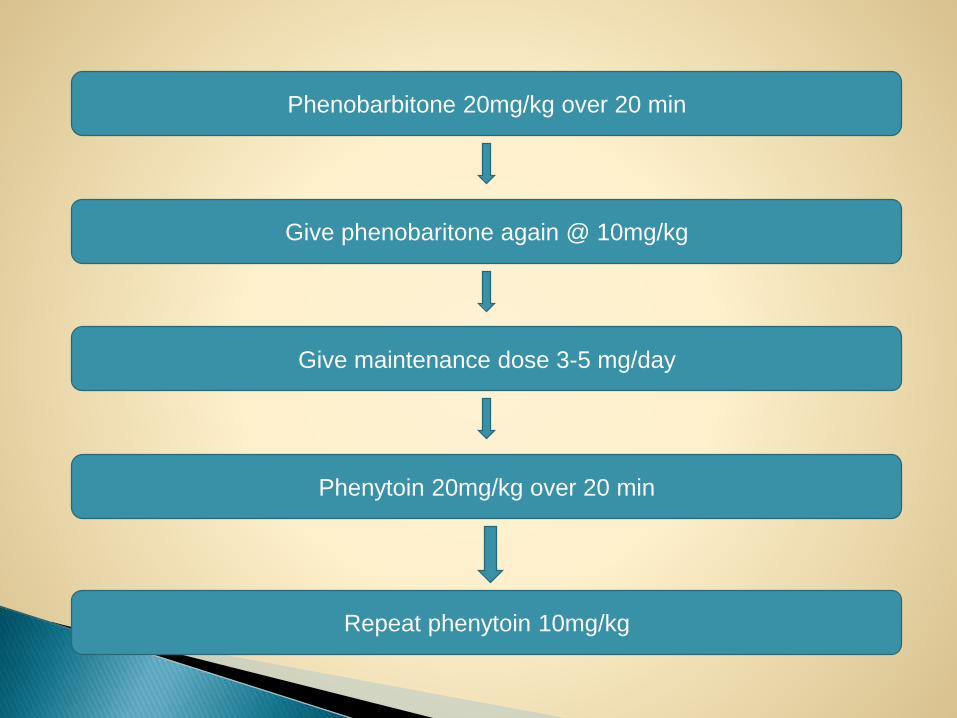
Phenobarbitone 20mg/kg over 20 min
Give phenobaritone again @ 10mg/kg
Give maintenance dose 3-5 mg/day
Phenytoin 20mg/kg over 20 min
Repeat phenytoin 10mg/kg
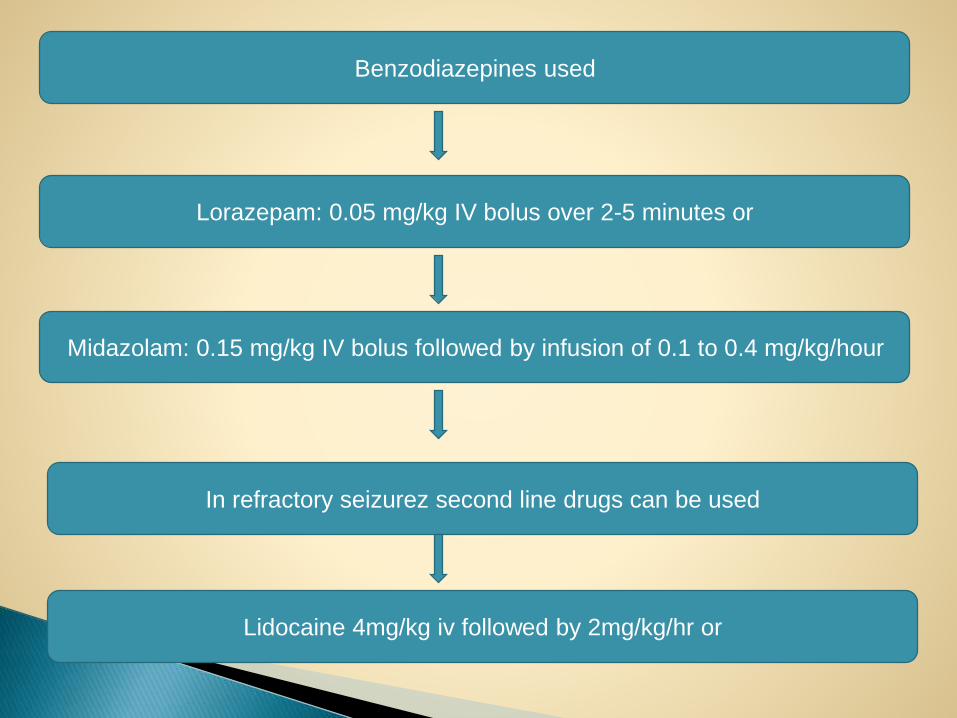
Benzodiazepines used
Lorazepam: 0.05 mg/kg IV bolus over 2-5 minutes or
Midazolam: 0.15 mg/kg IV bolus followed by infusion of 0.1 to 0.4 mg/kg/hour
In refractory seizurez second line drugs can be used
Lidocaine 4mg/kg iv followed by 2mg/kg/hr or
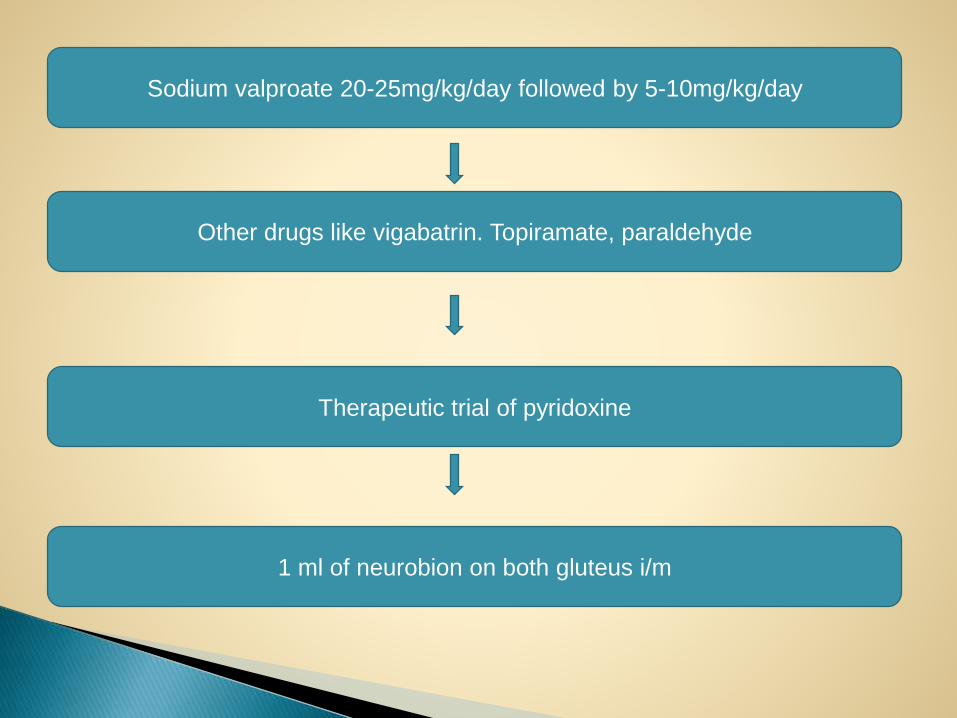
Sodium valproate 20-25mg/kg/day followed by 5-10mg/kg/day
Other drugs like vigabatrin. Topiramate, paraldehyde
Therapeutic trial of pyridoxine
1 ml of neurobion on both gluteus i/m
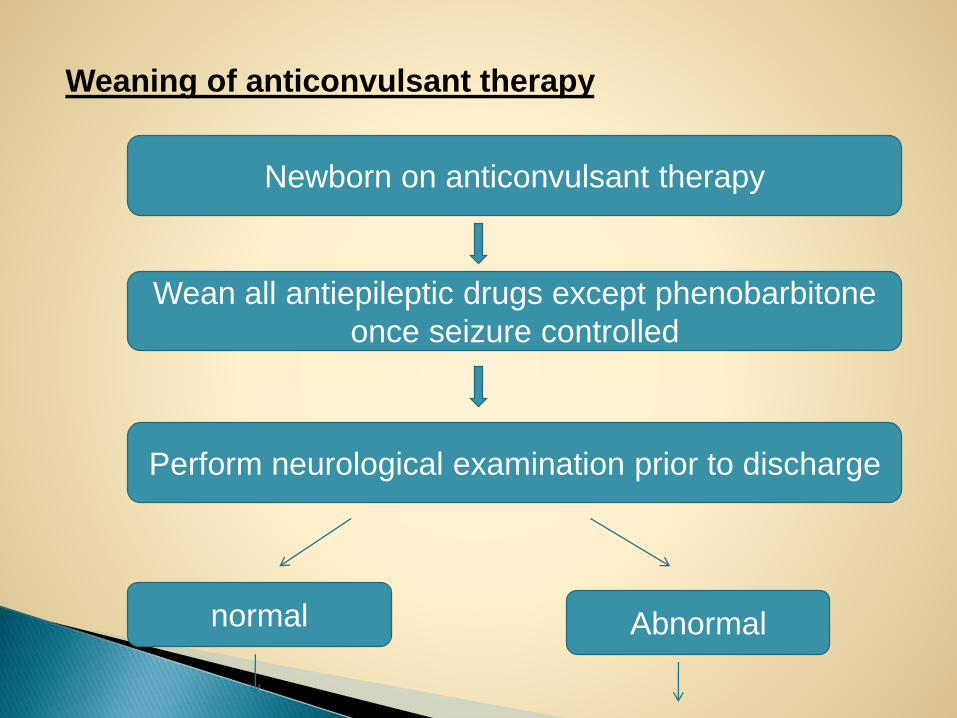
Weaning of anticonvulsant therapy
Newborn on anticonvulsant therapy
Wean all antiepileptic drugs except phenobarbitone
once seizure controlled
Perform neurological examination prior to discharge
normal Abnormal
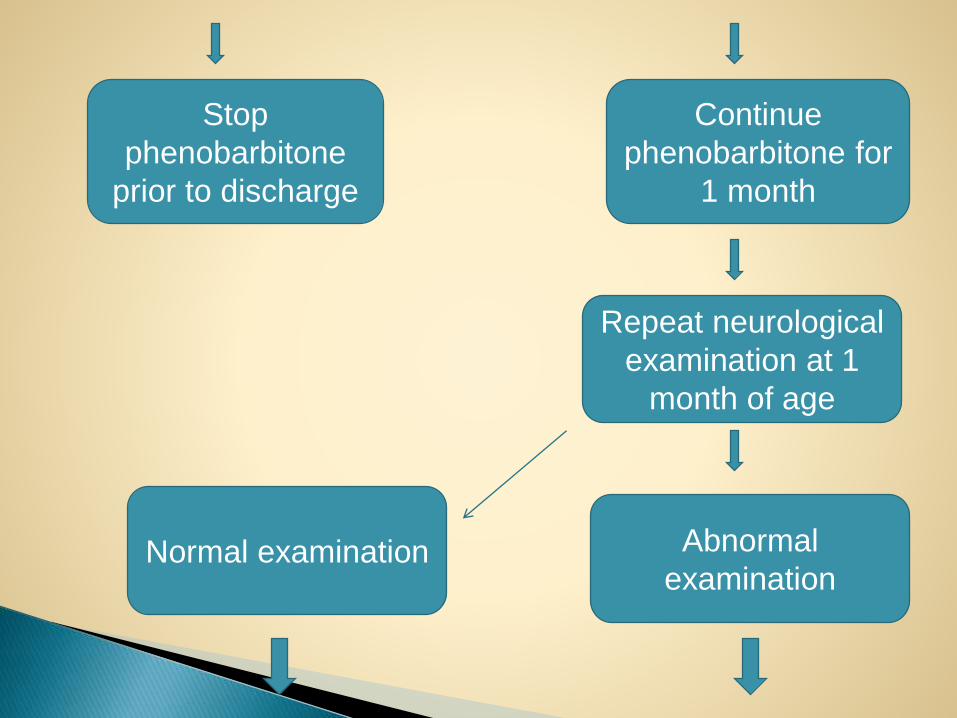
Stop
phenobarbitone
prior to discharge
Continue
phenobarbitone for
1 month
Repeat neurological
examination at 1
month of age
Abnormal
examinationNormal examination
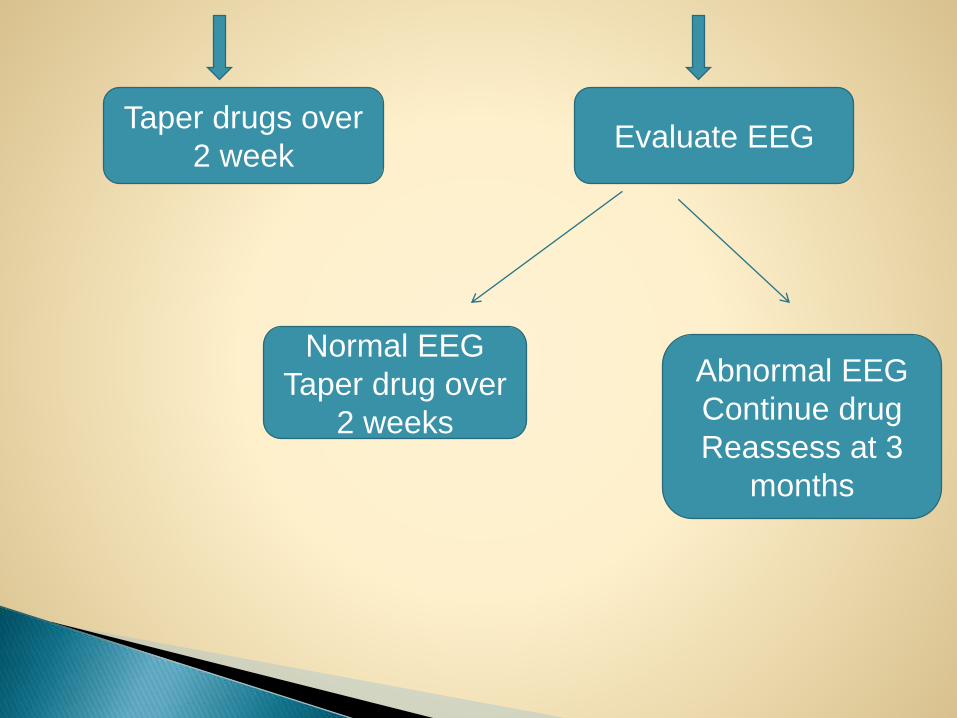
Taper drugs over
2 weekEvaluate EEG
Normal EEG
Taper drug over
2 weeks
Abnormal EEG
Continue drug
Reassess at 3
months
Outcome depends on1. Level of maturity
2. Etiology
3. Neurological examination
4. EEG / Imaging studies
Uncomplicated hypoglycemia
Narcotic withdrawal
SAH
Low APGAR score ≤ 6 at 5min
Onset o seizures within 24 hrs of life
Presence of myoclonic attacks
Abnormal EEG
3 or more days of uncontrolled seizures
Cerebral palsy
Hydrocephalus
Epilepsy
Spasticity
Feeding difficulties
CLOHERTY TEXT BOOK OF NEONATOLOGY
MEHARBAN TEXT BOOK OF NEONATOLOGY
AVERY TEXT BOOK OF NEONATOLOGY

THANKYOU

















