Corticosteroids in severe alcoholic hepatitis after recent upper GI
bleed
Dr. Jan Petrasek reviewing Rudler et al., J Hepatol. 2015 Apr;62(4):816-21. 10.1016/j.jhep.2014.11.003. Epub 2014 Nov 11.
Summary: GI bleed, if effectively controlled, should not be a contraindication to steroids in severe alcoholic hepatitis
Commentary: Both AASLD (American Association for the Study of Liver Disease) and EASL (European Association for the Study of the Liver) guidelines specify that patients with severe alcoholic hepatitis with recent upper GI bleed should not receive corticosteroid treatment. The reason for this may be a carryover from clinical trials performed in the 1970’s and 1980’s in which patients with upper GI bleeding were excluded due to the belief that corticosteroids caused gastroduodenal ulcers and also because no effective treatment of upper GI bleeding existed at that time. Since then, however, much has changed, including advent of proton pump inhibitors, endoscopic treatment of variceal bleeding and transjugular portosystemic shunting. In this issue of Journal of Hepatology, Rudler et al.have published the results of a retrospective analysis of survival among patients with severe alcoholic hepatitis (Maddrey’s Discriminant Function ≥ 32) who presented to hospital with upper GI bleed and compared them with patients with severe alcoholic hepatitis without GI bleeding. A total of 48 patients with upper GI bleed and 47 patients without GI bleed were analyzed. The two groups did not differ in presence of alcoholic hepatitis on biopsy (approximately 80%) or Maddrey’s Discriminant Function (63 and 65, respectively). After stabilization and effective endoscopic bleeding control, both groups were started on corticosteroids (40 mg of prednisolone daily for 28 days). The 6-month survival was similar in both groups (74% vs. 70%). The probability of developing an infection after starting corticosteroids was lower among subjects with upper GI bleed (24%) as compared with subjects without upper GI bleed (45%). This was attributable to the effect of antibiotic therapy (ceftriaxone) which is mandated in patients with acute GI bleed. If validated in prospective trials, this data indicate that patients with severe alcoholic hepatitis presenting with GI bleed may be safely treated with corticosteroids after achieving effective bleeding control. Link Out Via UTSW
Dr. Jan Petrasek reviewing Ge et al., JAMA. 2014 Aug 13;312(6):643-4.
Summary: Limited value of ammonia levels in liver diseases other than fulminant liver failure
Commentary: In this JAMA Diagnostic Test Interpretation article, Ge et al. review the utility of serum ammonia levels in patients with hepatic encephalopathy. It is common for ammonia levels to be obtained during the evaluation of chronic liver disease. However, the evidence does not support ammonia measurement under these circumstances. Hepatic encephalopathy is a clinical, not laboratory diagnosis, and normal ammonia level does not exclude a diagnosis of hepatic encephalopathy, nor does an elevated ammonia level establish a diagnosis of hepatic encephalopathy. Blood ammonia levels correlate poorly with the grade of hepatic encephalopathy in patients with chronic liver disease. The only clinical utility for measurement of serum ammonia levels is in patients with fulminant liver failure because ammonia levels correlate with the severity of encephalopathy and elevated levels greater than 150 to 200 μmol/liter are predictive of cerebral edema. Link out Via UTSW
Extended report: Prediction of cardiovascular risk in rheumatoid arthritis: performance of original and adapted SCORE algorithms Dr. Brian Skaug reviewing Arts, et al. Ann Rheum Dis. 2015 Feb 17. pii: annrheumdis-2014-206879. doi: 10.1136/annrheumdis-2014-206879 Summary: Efforts toward an accurate cardiovascular risk assessment in rheumatoid arthritis patients Commentary: Rheumatoid arthritis (RA) confers an elevated risk of cardiovascular disease (CVD) and CVD-related mortality that cannot be fully explained by traditional risk factors such as age, lipid values, smoking, and hypertension. To account for this risk the European League Against Rheumatism (EULAR) has recommended a 1.5x multiplication factor to CVD risk scores for RA patients with two of three criteria (disease duration >10 years, + RF and/or anti-CCP antibodies, or extra-articular manifestations). However the benefit of incorporating this recommendation is not supported by strong evidence. Therefore development of an RA-specific CVD risk prediction algorithm is desirable. In this report the authors tested whether variables such as RF and anti-CCP antibodies, inflammatory biomarkers, and clinical disease activity assessments could improve the predictive ability of the systematic coronary risk evaluation (SCORE), which is a widely used algorithm in Europe similar to the Framingham score used more commonly in the US. They compared the ability of an adapted algorithm to the traditional SCORE algorithm for their ability to predict fatal and non-fatal cardiac events in a large European cohort of RA patients with no CVD at baseline. Unfortunately the authors’ adapted algorithm did not show an increased ability to identify patients at risk for cardiac events compared to the traditional SCORE algorithm. Similar to the traditional SCORE algorithm, the adapted algorithm tended to underestimate the risk of cardiac events in those with low scores, and overestimate the risk in those with high scores. Their results highlight a gap in our ability to predict cardiac events in RA patients even when RA-related variables are taken into account. This difficulty may be due to an inadequate understanding of CVD pathogenesis in patients with autoimmune/inflammatory disease. Future research on CVD pathogenesis in RA patients could reveal which variables might better predict CVD risk. Link Out Via UTSW
Pulmonary/Critical Care Trial of Early, Goal-Directed Resuscitation for Septic Shock [The Protocolised Management in Sepsis (ProMISe) Trial]
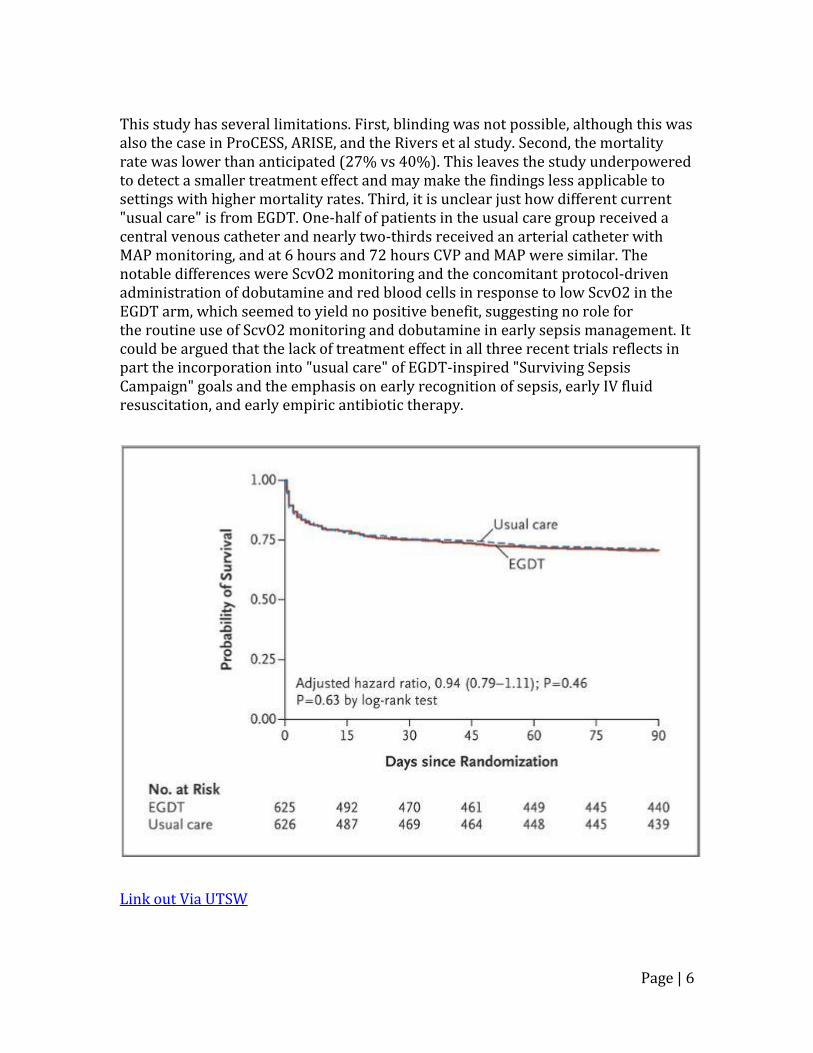
Dr. James Galloway reviewing Mouncey PR et al. N Engl J Med. 2015;372(14):1301-11. Summary: If patients are identified early in sepsis or septic shock and given appropriate antibiotics fluids early, then the protocol used afterwards, Early goal directed therapy, protocol, or usual care is less important. Patients do not need CVP or SV02 monitoring to improve outcomes. Commentary: This is the third of three recent trials (with ARISE and ProCESS) comparing the effect of the "early, goal-directed therapy (EGDT)" protocol with current usual care on mortality in sepsis. The other two trials demonstrated no mortality benefit with EGDT at 60 days, but neither trial could rule-out a possible 8% ARR in 90-day mortality for EGDT. ProMISe was designed with 80% power to detect this outcome. It also included a cost-effectiveness analysis. ProMISe is a randomized, controlled trial conducted at 56 hospitals across England. Patients were randomized within 6 hours of presentation to the ED and within 2 hours of meeting the inclusion criteria: >= 18 years of age with 2 or more SIRS criteria, known or presumed infection, and either hypotension (SBP<90 or MAP<65) refractory to 1L of IV fluids or blood lactate >= 4 mmol/L. 1260 patients underwent randomization; fewer than 1% was lost to follow up. Patients were similar at baseline with respect to presence of refractory hypotension, lactate level, illness severity (as measured by Apache II and similar scores), comorbidities, and source of infection. In general, patients were treated similarly between the two groups. All patients received empiric antibiotic therapy prior to randomization. A similar number of patients in each group (97%) received IV fluids prior to randomization (median of 2L in each group); it is important to note that the groups received similar volumes of fluid in the 1st 6 hours, which was different from the original River's study, where early fluid resuscitation was less aggressive. After the 1st 6 hours of EGDT vs usual care, care was at the discretion of the treating clinician. Intention-to-treat analysis showed no difference in 90-day mortality between EGDT and usual care (RR 1.01 [95% C.I. 0.85-1.20; P=0.90]; ARR -0.3% [95% C.I. -5.7%-4.7%]). Patients in the EGDT group had worse organ failure scores, longer ICU stays, and were subjected to greater treatment intensity (more total IV fluids, vasoactive drugs, and red blood cell transfusions). Adherence to the EGDT protocol was good (86-95%) and analysis disclosed no "learning curve effect" to explain the lack of a positive result. There was no significant difference in adverse events or health-related quality-of-life. The probability that EGDT was cost-effective was <20%.
Page | 6
This study has several limitations. First, blinding was not possible, although this was also the case in ProCESS, ARISE, and the Rivers et al study. Second, the mortality rate was lower than anticipated (27% vs 40%). This leaves the study underpowered to detect a smaller treatment effect and may make the findings less applicable to settings with higher mortality rates. Third, it is unclear just how different current "usual care" is from EGDT. One-half of patients in the usual care group received a central venous catheter and nearly two-thirds received an arterial catheter with MAP monitoring, and at 6 hours and 72 hours CVP and MAP were similar. The notable differences were ScvO2 monitoring and the concomitant protocol-driven administration of dobutamine and red blood cells in response to low ScvO2 in the EGDT arm, which seemed to yield no positive benefit, suggesting no role for the routine use of ScvO2 monitoring and dobutamine in early sepsis management. It could be argued that the lack of treatment effect in all three recent trials reflects in part the incorporation into "usual care" of EGDT-inspired "Surviving Sepsis Campaign" goals and the emphasis on early recognition of sepsis, early IV fluid resuscitation, and early empiric antibiotic therapy.
A Randomized Trial of Icatibant in ACE-Inhibitor-Induced Angioedema
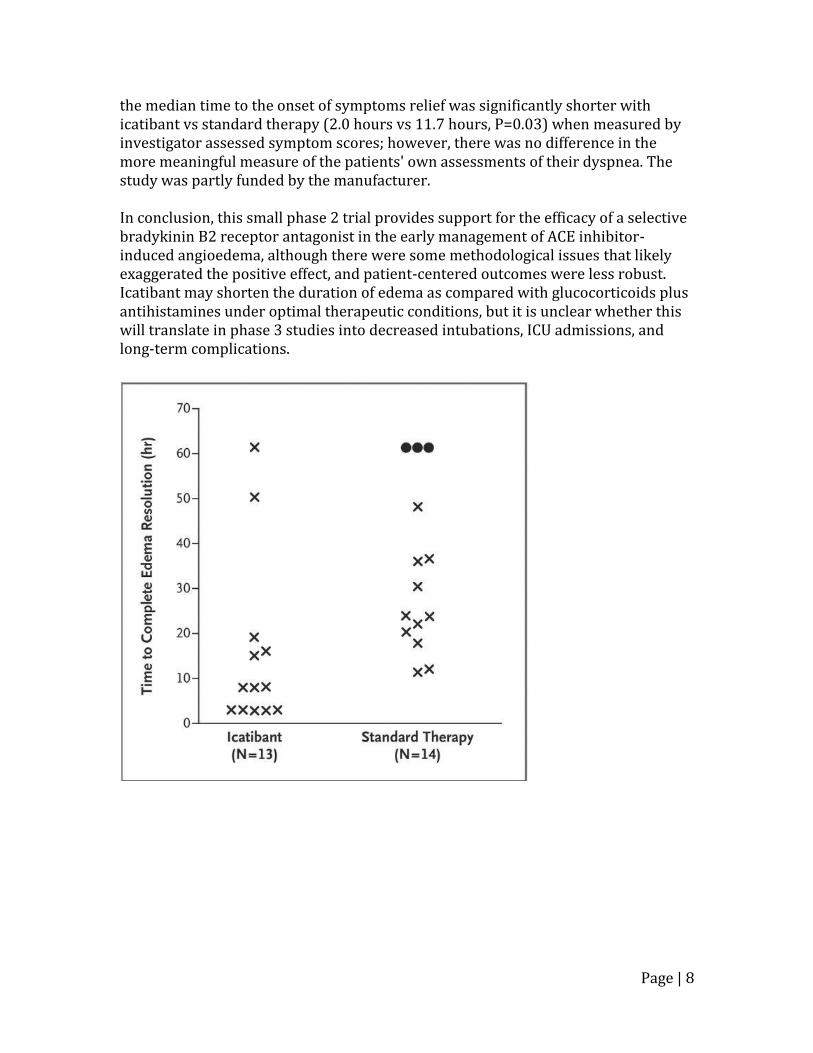
Dr. James Galloway reviewing Bas M, et al. N Engl J Med. 2015;372(5):418-25. Summary: There is growing information that Icatibant, a bradykinin B2 receptor antagonist might be of therapeutic benefit in ACEI induced angioedema, but there is limited data so far on its clinical significance. Commentary: ACE-inhibitors are responsible for one third of cases of angioedema of the upper aerodigestive tract. The mechanism is believed to be bradykinin-mediated, but at present there is no FDA approved, mechanistically-guided intervention for this condition. This is a small, multicenter, double-blind, double-dummy, randomized phase 2 trial assessing the efficacy and safety of a selective bradykinin B2 receptor antagonist (icatibant 30 mg subcutaneous injection) compared to standard therapy (IV prednisolone 500 mg plus antihistamine clemastine 2 mg) in the treatment of ACE inhibitor-induced angioedema limited to the upper aerodigestive tract. 32 patients were screened and 27 patients were included in the analysis. Patients were randomized within 10 hours of symptom onset in variable block sizes in a 1:1 ratio to ensure equal group sizes. There were no statistically significant differences in baseline patient characteristics. The study had >90% power using two-sided significance testing. No patients discontinued the study owing to adverse events; however, 4 patients, all from the control group, were lost to follow up at day 14, casting doubt on the validity of the safety analysis, although likely not affecting the immediate efficacy outcomes. A per protocol analysis was conducted, reflecting efficacy under optimal therapeutic conditions. No patients in the experimental group failed treatment. Three patients in the control group failed standard therapy at 6 hours and received "rescue therapy" with the study agent and 500mg IV prednisolone; one of them required a tracheotomy; these 3 patients were arbitrarily assigned the maximum recorded time to complete resolution of edema (61.2 hours), which exaggerated the difference in primary endpoint between the two groups. The primary efficacy end point was time to complete resolution of edema, which was evaluated using a composite of 3 scores: patient-assessed dyspnea, blinded investigator-assessed dyspnea, and blinded investigator-assessed edema on physical exam or endoscopy. The median time to complete resolution of edema was 8.0 hours with icatibant (IQR 3.0-16.0 hours) as compared with 27.1 hours (IQR 20.3-48.0 hours) with standard therapy (P=0.002). Among the secondary endpoints,
Page | 8
the median time to the onset of symptoms relief was significantly shorter with icatibant vs standard therapy (2.0 hours vs 11.7 hours, P=0.03) when measured by investigator assessed symptom scores; however, there was no difference in the more meaningful measure of the patients' own assessments of their dyspnea. The study was partly funded by the manufacturer. In conclusion, this small phase 2 trial provides support for the efficacy of a selective bradykinin B2 receptor antagonist in the early management of ACE inhibitor-induced angioedema, although there were some methodological issues that likely exaggerated the positive effect, and patient-centered outcomes were less robust. Icatibant may shorten the duration of edema as compared with glucocorticoids plus antihistamines under optimal therapeutic conditions, but it is unclear whether this will translate in phase 3 studies into decreased intubations, ICU admissions, and long-term complications.
High-Sensitivity Troponin T and N-Terminal Pro-B-Type Natriuretic Peptide (NT-proBNP) and Risk of Incident Heart Failure in Patients with CKD: The Chronic Renal Insufficiency Cohort (CRIC) Study. Dr. Natalia Rocha reviewing Bansal N, et al. JASN 2015; 26:946-956 Summary: The use of high sensitivity Troponin T and NT-proBNP even in CKD patients is still a strong predictor of the incidence of heart failure. Commentary: The use of high sensitivity troponin T (hsTnT) and NT-proBNP as predictors of heart failure in CKD patients has been limited due to concerns that elevations might simply be a reflection of decrease biomarker clearance from decreased GFR. In this prospective cohort analysis, the authors studied 3483 patients with mild to severe CKD enrolled in the Chronic Renal Insuficiency Cohort (CRIC) study with no heart failure. They examined the association between baseline hsTnT and NT-proBNP and subsequent incident HF. The authors concluded that even after adjusting for a vast range of cardiovascular risk factor such as older age, sex, race, higher BP, diabetes and lower rejection fraction, hsTnT and NT-proBNP were both strong predictors of incident heart failure in patients with mild to moderate CKD and may represent subclinical injury that can ultimately progress to HF.
Preoperative renin–angiotensin system inhibitors use linked to reduced acute kidney injury: a systematic review and meta-analysis
Dr. Natalia Rocha reviewing Cheungpasitporn W, et al. Nephrol. Dial. Transplant. 2015; doi: 10.1093/ndt/gfv023 Summary: The meta-analysis suggesting negative outcomes with the use of RAS inhibitors pre-operatively may have been limited by confounding factors. Limiting these confounding factors by the use of propensity scores has actually shown a decrease in AKI postop with the use of preoperative RAS inhibitors. Commentary: Acute kidney injury (AKI) is one of the most frequent postoperative complications and it is linked to higher hospital mortality. A previous meta-analysis of observational studies showed that the preoperative use of a renin-angiotensin system (RAS) inhibitor was associated with increased incidence of AKI postoperatively and for this reason, discontinuation of RAS inhibitors prior to surgery has been proposed as a preventative measure for postoperative AKI. The study of Cheungpasitporn et al suggests that the previous meta-analysis might have been limited by the effect of confounders such as the fact that patients on RAS inhibitors are usually the ones with heart failure, hypertension and diabetes, which are all risk factors for AKI. The authors found that by utilizing propensity scores, which reduced confounding effect, there was a significant association between preoperative RAS inhibitor use and lower incidence of AKI. The association was stronger when RAS inhibitor was used for > 2 weeks prior to surgery. The physiological explanation for this protective effect is that reducing RAS response to renal ischemia during surgery leads to decrease in systemic vascular resistance and improve renal plasma flow.
Which drug should we use for stroke prevention in atrial fibrillation? Dr. Douglas Darden reviewing Lau, Yee C.; Lip, Gregory Y.H. Current Opinion in Cardiology. 2014 July 29 (4): 293-300. Summary: This article reviews the latest evidence and development of new oral anticoagulants for the prevention of ischemic stroke, as well as bleeding risk assessment, mitigation and management. Commentary: Decision-making for stroke prevention has evolved towards the initial identification of 'low-risk' patients who do not need any antithrombotic therapy. Subsequent to this step, patients with at least 1 stroke risk factor can be offered effective stroke prevention, which is OAC. There is increased morbidity and mortality amongst warfarin users, if time in therapeutic range is poor. New oral anticoagulants (such as dabigatran, rivaroxaban, apixaban and edoxaban) offer relative efficacy, safety and convenience compared to warfarin, in relation to stroke prevention in atrial fibrillation. Bleeding risk can be assessed by HAS-BLED score, whereas the new SAMe-TT2R2 score can predict the patient's suitability for vitamin K antagonists. It is well-known that vitamin K antagonists (VKAs), such as warfarin, is highly effective and has been shown to reduce stroke risk by 64% and all-cause mortality by up to 26% in atrial fibrillation. However, the use of VKA is complicated by its potential interactions with food and medications, genetic polymorphisms conferring differing susceptibilities, as well as the potential for major hemorrhage. And of course, the effectiveness of VKA treatment depends on the time spent in therapeutic range, with maximum benefit achieved if time spent in therapeutic range exceeds 70%. The limitations of VKA have led to the development of NOACs, ‘novel’ or ‘non-VKA oral anticoagulants’. Through reversible inhibition of thrombin by dabigatran or Factor Xa by rivaroxaban, apixaban or edoxaban, the NOACs exhibit a predictable pharmacology that allow for fixed dosing that makes monitoring unnecessary (see table 1 for the major RCTs). Dabigitran was studied in the RE-LY trial, where it was found to be superior to warfarin for prevention of both ischemic stroke and systemic thromboembolism, with an annual event of 1.11% in the 150 mg group and 1.53% in the 110 mg group against warfarin-treated patients at 1.69% (P < 0.001). Dabigatran was also non-inferior to warfarin for major bleeding with annual event rates of 3.11% in the 150 mg group vs. 2.71% in the 110 mg group vs. 3.36% in the warfarin-control group. It was also superior to warfarin in reducing intracranial hemorrhage by more than half.
Page | 13
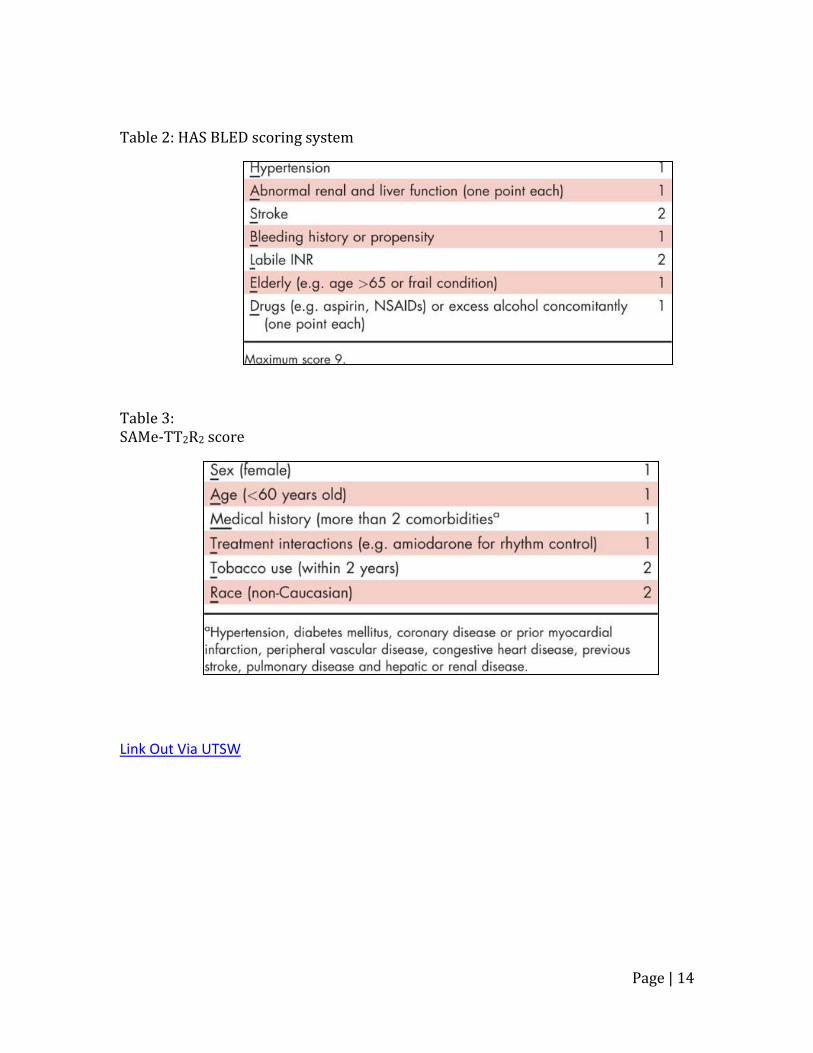
Rivaroxaban was studied in the ROCKET-AF trial and showed to be non-inferior compared to warfarin the prevention of ischemic stroke. Apixaban, on the other hand, was showed to be superior to warfarin in the ARISTOTLE trial, with the annual event rate of 1.27% in the apixaban group vs. 1.6% in the warfarin group. One of the drawbacks currently with the NOACs is that there is no antidote. In assessing the stroke and bleeding risk for patients, we all know to use the CHA2DS2-VASc score and HASBLED score. To note, a high HAS-BLED score should identify potential risk factors that can be treated, rather than withhold anticoagulation (table 2). To aid in deciding between VKA and NOACs, the SAMe-TT2R2 score (table 3) has been created to identify those who will do well on VKA (score 0-1). Lastly, as there is insufficient on NOACs in ESRD and prosthetic heart valves, VKA is still the preferred option. Table 1: Randomized controlled trials for NOACs in Atrial Fibrillation
Page | 14
Table 2: HAS BLED scoring system Table 3: SAMe-TT2R2 score
EKG CHALLENGE: Contributed by Dr. Jeanney Lew A 57 year-old male with T2DM, HTN, and current tobacco use presents to the ED with a 3-day history of severe intermittent chest pain, which he describes as 7/10 “crushing” substernal pressure. These episodes have been associated with shortness of breath and diaphoresis, seemingly triggered by exertion, resolving after 10 minutes of rest. This morning the pain felt so severe that he “took a couple aspirin and called 911.” Upon arrival to the ED, his chest pain had resolved – He was resting comfortably, not in
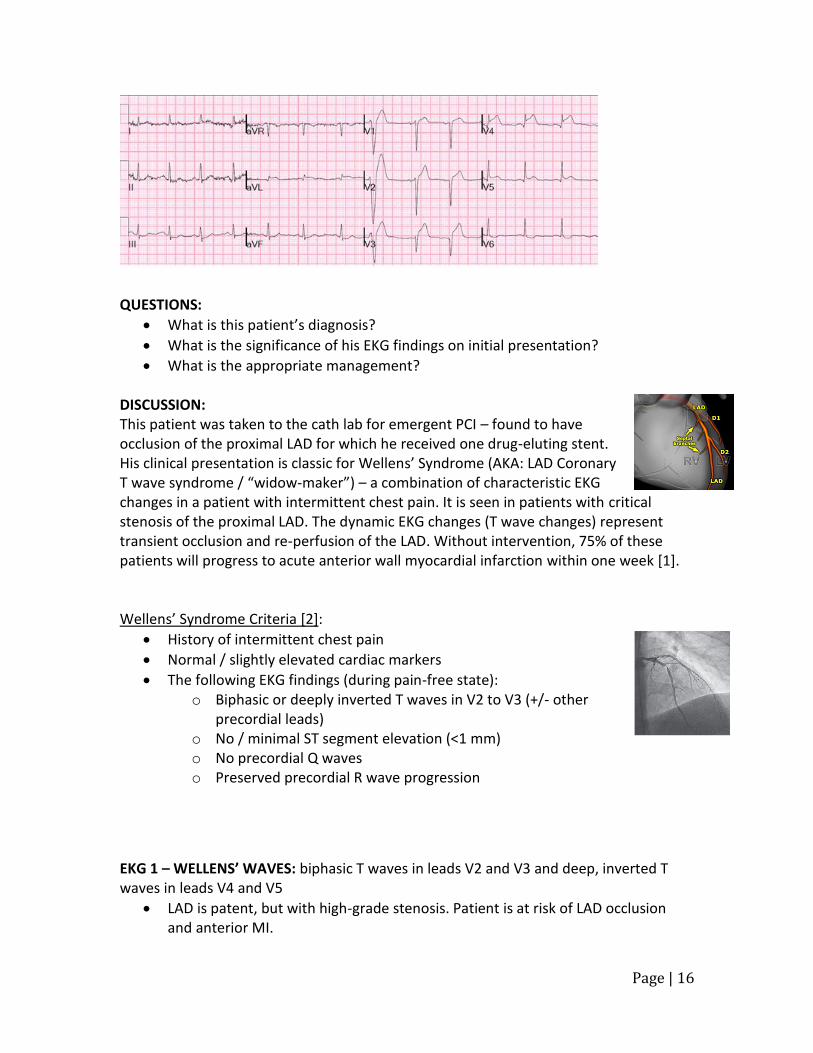
distress. His vitals: T 37 C, P 90, BP 142/88, RR 16, SpO2 99% on RA. Initial troponin T was 0.01 and EKG performed at this time (EKG 1) was significant for biphasic T waves in leads V2 and V3 and inverted T waves in leads V4 and V5. EKG 1
After 2 hours of sitting in the ED, patient suddenly develops severe 10/10 crushing substernal pain, SOB, and palpitations. He appears diaphoretic and in significant distress. Repeat troponin T was drawn – measured 0.24 and STAT EKG revealed the following: EKG 2
At this point, Cardiology was consulted and another STAT EKG showed the following changes: EKG 3
Page | 16
QUESTIONS:
What is this patient’s diagnosis?
What is the significance of his EKG findings on initial presentation?
What is the appropriate management? DISCUSSION: This patient was taken to the cath lab for emergent PCI – found to have occlusion of the proximal LAD for which he received one drug-eluting stent. His clinical presentation is classic for Wellens’ Syndrome (AKA: LAD Coronary T wave syndrome / “widow-maker”) – a combination of characteristic EKG changes in a patient with intermittent chest pain. It is seen in patients with critical stenosis of the proximal LAD. The dynamic EKG changes (T wave changes) represent transient occlusion and re-perfusion of the LAD. Without intervention, 75% of these patients will progress to acute anterior wall myocardial infarction within one week [1]. Wellens’ Syndrome Criteria [2]:
History of intermittent chest pain
Normal / slightly elevated cardiac markers
The following EKG findings (during pain-free state): o Biphasic or deeply inverted T waves in V2 to V3 (+/- other
precordial leads) o No / minimal ST segment elevation (<1 mm) o No precordial Q waves o Preserved precordial R wave progression
EKG 1 – WELLENS’ WAVES: biphasic T waves in leads V2 and V3 and deep, inverted T waves in leads V4 and V5
LAD is patent, but with high-grade stenosis. Patient is at risk of LAD occlusion and anterior MI.
Page | 17
EKG 2 – “PSEUDO-NORMALIZATION” of the T waves: upright “hyperacute T waves” in anterior leads
Reciprocal changes in inferior leads (II, III, aVF)
KEY POINTS:
Wellens’ waves are bipashic or deeply inverted T waves in anterior leads (esp V2, V3)
Wellens’ syndrome = Wellens’ waves in a patient with history of intermittent chest pain
o During pain-free intervals; troponins are normal or minimally elevated o LAD is patent, but at high risk of occlusion, resulting in acute anterior wall
MI o This is an indication for urgent cardiac cath
“Pseudo-normalization” (upright, hyperacute T waves) = occlusion of the LAD o Represents early phase of myocardial infarction o Accompanied by chest pain, rising cardiac enzymes
REFERENCES: 1. Mead, N.E. and K.P. O'Keefe, Wellen's syndrome: An ominous EKG pattern. J
Emerg Trauma Shock, 2009. 2(3): p. 206-8. 2. Yusuf Muharam, M., R. Ahmad, and M. Harmy, The ' widow maker':
Electrocardiogram features that should not be missed. Malays Fam Physician, 2013. 8(1): p. 45-7.