AQA A Revision Guide – Population 1. What has happened to World population over the years? The population rose dramatically in the 20 th century and continues today. This rapid ‘explosion’ of population is after referred to as ‘exponential growth’, where a larger population keeps on creating an even larger population. The population of the World is now estimated to be over 7 billion. 2. What is likely to happen to World population in the future? There is no mistake here! The map has been drawn in proportion to their estimated populations. By 2050, it is expected that 62% of all people will live in Africa and South and East Asia. LEDCs still tend to have a rising population, but it has been found that people in MEDCs are tending to have fewer babies. In fact, despite an increase in life expectancy, some countries have a falling population – e.g. Sweden. The UN believe that population will peak at 10 billion in 2200 and will then start to fall. 3. What are the key basic population terms that I need to know? Birth rate – the number of babies born per year per 1000 people Death rate – the number of deaths per year per 1000 of the population Natural increase – the number of people added to the population (or lost) per year per 1000 people. Population growth rate – the number of people added or lost from a population each year. This also includes migration. It is given as a percentage. 4. How can the way in which population has changed be modelled? The demographic transition model (DTM) was developed for this purpose. ‘Demography’ is the study of population, ‘transition’ means change and a ‘model’ is something that happens in real life. It was created following studies of European countries & places such as the USA & Japan, but it might not fit countries that are developing rapidly today. Stage 1: High birth and death rates (BR and DR). High BR due to lack of birth control, people marry young, children needed to work. High DR due to famine, disease, lack of clean water and poor access to medical care/ Stage 2: High BR, but falling DR. Same reasons for BR, but DR falls due better medicine, cleaner water, better food and sanitation.
Transcript
AQA A Revision Guide – Population
1. What has happened to World population
over the years?
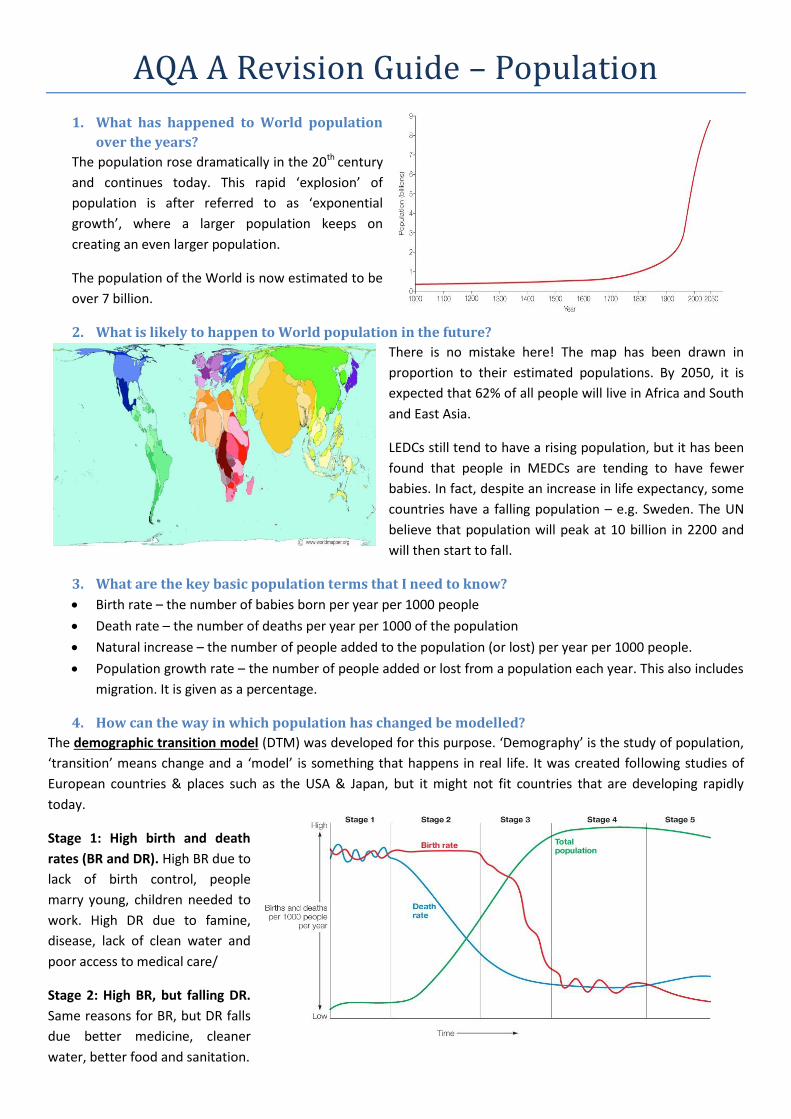
The population rose dramatically in the 20th century
and continues today. This rapid ‘explosion’ of
population is after referred to as ‘exponential
growth’, where a larger population keeps on
creating an even larger population.
The population of the World is now estimated to be
over 7 billion.
2. What is likely to happen to World population in the future?
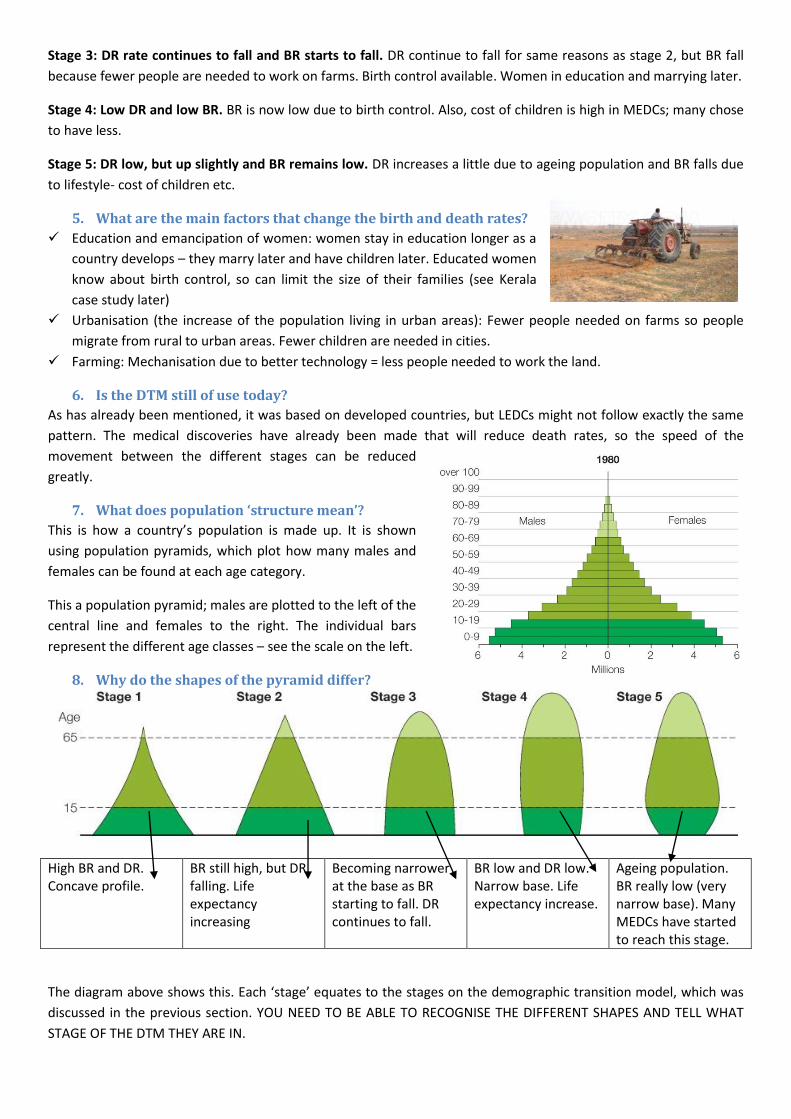
There is no mistake here! The map has been drawn in
proportion to their estimated populations. By 2050, it is
expected that 62% of all people will live in Africa and South
and East Asia.
LEDCs still tend to have a rising population, but it has been
found that people in MEDCs are tending to have fewer
babies. In fact, despite an increase in life expectancy, some
countries have a falling population – e.g. Sweden. The UN
believe that population will peak at 10 billion in 2200 and
will then start to fall.
3. What are the key basic population terms that I need to know?
Birth rate – the number of babies born per year per 1000 people
Death rate – the number of deaths per year per 1000 of the population
Natural increase – the number of people added to the population (or lost) per year per 1000 people.
Population growth rate – the number of people added or lost from a population each year. This also includes
migration. It is given as a percentage.
4. How can the way in which population has changed be modelled?
The demographic transition model (DTM) was developed for this purpose. ‘Demography’ is the study of population,
‘transition’ means change and a ‘model’ is something that happens in real life. It was created following studies of
European countries & places such as the USA & Japan, but it might not fit countries that are developing rapidly
today.
Stage 1: High birth and death
rates (BR and DR). High BR due to
lack of birth control, people
marry young, children needed to
work. High DR due to famine,
disease, lack of clean water and
poor access to medical care/
Stage 2: High BR, but falling DR.
Same reasons for BR, but DR falls
due better medicine, cleaner
water, better food and sanitation.
Stage 3: DR rate continues to fall and BR starts to fall. DR continue to fall for same reasons as stage 2, but BR fall
because fewer people are needed to work on farms. Birth control available. Women in education and marrying later.
Stage 4: Low DR and low BR. BR is now low due to birth control. Also, cost of children is high in MEDCs; many chose
to have less.
Stage 5: DR low, but up slightly and BR remains low. DR increases a little due to ageing population and BR falls due
to lifestyle- cost of children etc.
5. What are the main factors that change the birth and death rates?
Education and emancipation of women: women stay in education longer as a
country develops – they marry later and have children later. Educated women
know about birth control, so can limit the size of their families (see Kerala
case study later)
Urbanisation (the increase of the population living in urban areas): Fewer people needed on farms so people
migrate from rural to urban areas. Fewer children are needed in cities.
Farming: Mechanisation due to better technology = less people needed to work the land.
6. Is the DTM still of use today?
As has already been mentioned, it was based on developed countries, but LEDCs might not follow exactly the same
pattern. The medical discoveries have already been made that will reduce death rates, so the speed of the
movement between the different stages can be reduced
greatly.
7. What does population ‘structure mean’?
This is how a country’s population is made up. It is shown
using population pyramids, which plot how many males and
females can be found at each age category.
This a population pyramid; males are plotted to the left of the
central line and females to the right. The individual bars
represent the different age classes – see the scale on the left.
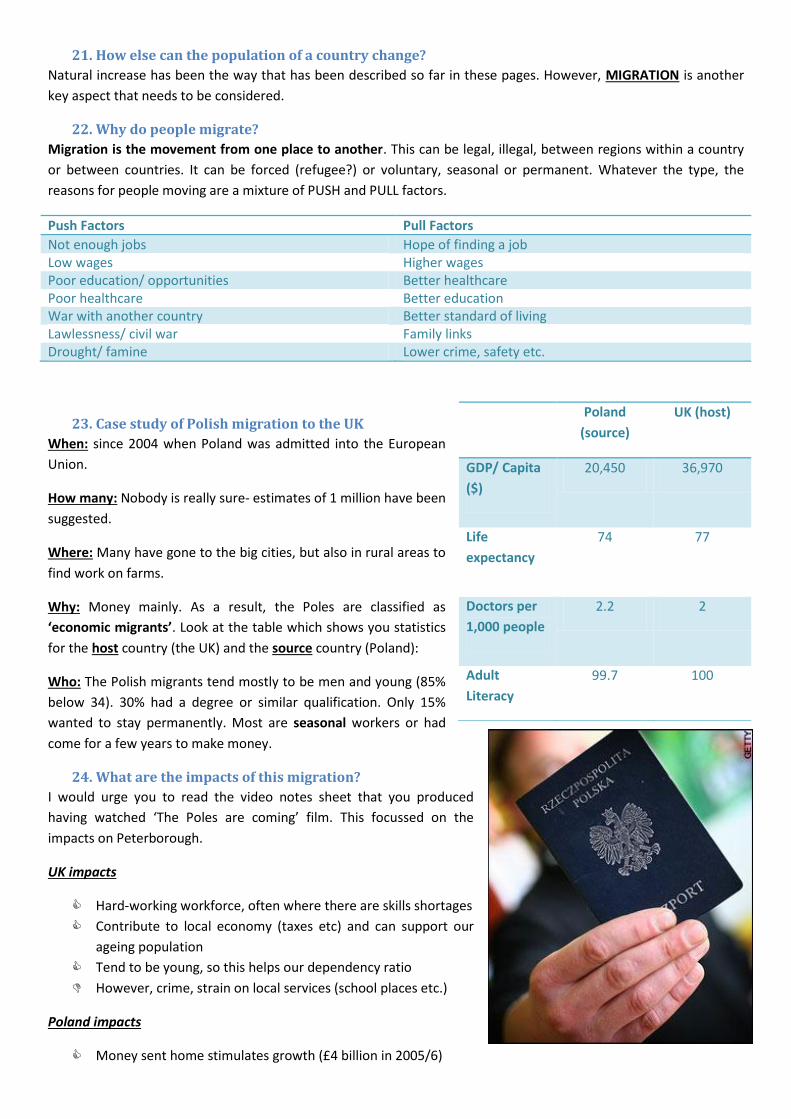
8. Why do the shapes of the pyramid differ?
High BR and DR. Concave profile.
BR still high, but DR falling. Life expectancy increasing
Becoming narrower at the base as BR starting to fall. DR continues to fall.
BR low and DR low. Narrow base. Life expectancy increase.
Ageing population. BR really low (very narrow base). Many MEDCs have started to reach this stage.
The diagram above shows this. Each ‘stage’ equates to the stages on the demographic transition model, which was
discussed in the previous section. YOU NEED TO BE ABLE TO RECOGNISE THE DIFFERENT SHAPES AND TELL WHAT
The table shows clearly, that in these cases, the higher the GDP (Gross Domestic Product, which is the value, in
dollars, of the goods and services that a country produces in one year) for a country results in more preferable
‘scores’ in terms of the population data. GDP is expressed as per capita, which is averaged out per person in the
country; PPP means purchasing power parity, where GDP is adjusted to reflect the purchasing power within the
different countries – i.e. the cost of living.
12. Why does it matter that population is growing in some countries?
It is often not sustainable and slows the development of a country. Income generated from farming and basic
industry does not provide for a growth in population. Pressure on resources can lead to:
Not able to feed the population – millions go hungry
Not enough money to provide schools – Millions have no education and therefore can’t obtain the skills that
could get them out of poverty. The country does not develop as a result.
Can’t afford to provide healthcare – millions dies from illness and disease
THE KEY IS TO HAVE POPULATION GROWTH THAT IS AT A LEVEL THAT DOESN’T PREVENT A COUNTRY FROM
DEVELOPING. Sustainable development is defined as ‘meeting the needs of the present without compromising the
ability of future generations to meet their own needs’. Clearly, a rapidly rising population will prevent this from
happening for the reasons discussed.
The average age in Afghanistan is just 17
13. What things can be done to control an expanding population?
You have two case studies for this: China and Kerala.
14. What was done in China?
i). Introduction: China had a rapidly rising population in the 1950s and 1960s and this
was seen as unsustainable. They didn’t have enough water, food and energy for that
growth in population so in 1979 China introduced the One Child Policy.
Essentially, couples were only allowed to have one child. Those that did received
welfare benefits and financial reward; those that did not were fined. There have been
awful stories of forced sterilisation and abortions. Many of you watched the ‘Dying
Rooms’ video and were horrified by what you saw.
ii). Has it been a success?: Yes and no. On the positive side, 300 million babies have not been born as result. One
could argue that this has led to sustainable development, but there have been a number of negative effects:
Social impacts Economic impacts
Children will need to look after more older people. More old people’s homes will be needed
Ageing population – they will need to be supported financially, as healthcare costs will increase
Chinese society prefers boys. Often baby girls have been abandoned – often in orphanages
China’s economy might not have enough workers to keep it expanding.
By 2020, men will outnumber women by 30 million. This could cause social unrest
The percentage of people over 65 will rise. 10% in 2009 will rise to 40% by 2050.
iii). The future? The policy could change. Reports in 2009 said that
couples in Shanghai were being encouraged to have 2 children (if they were single children themselves)
15. What was done in Kerala about a rise in population?
i). Where is Kerala? SW India
ii). Some facts: Population 32 million, densely populated and
very poor. BUT they have followed population policies that
have prevented a rapid rise in population.
iii). What have they done?
They made political decisions to invest in education and
women’s health. Almost all villages have access to medical
care and school within 2.5km
Economics – the area relies less on farming and more on
service industries – like tourism (farming results in more
children to help)
Quality of life indicator
Kerala India USA
Adult literacy %
91 61 96
Life expectancy males/ females
69/75 67/72 74/80
Infant mortality/1000
10 33 7
Birth rate/1000
17 22 16
Over 65
Children
iv). So what have been the impacts of these policies?
Kerala compares favourably to India in public services (better roads, schools, post offices, banks etc.)
Women’s health and education are the best in India.
Attitudes towards women are positive; more girls are in higher education than boys
Women marry on average 4 years later and have their first child 5 years later than other Indian women. They
only have 2 children on average and infant mortality is low.
v). Has this approach led to sustainable development?
It has controlled the growth in population – healthcare provision and education were key to this. THE MAIN
DIFFERENCE BETWEEN CHINA AND KERALA WAS THAT POPULATION WAS CONTROLLED THROUGH THE CHOICE OF
PEOPLE – THEY WERE NOT FORCED IN KERALA. However, Kerala is likely to face similar problems to China in that
they will have an ageing population. Examine the population pyramids for Kerala below.....
16. What are the problems with an ‘Ageing Population’?
I referred to the issue of an ageing population in the sections about Kerala and China. There are a number of
problems associated with this:
Health and fitness – older people suffer from more degenerative diseases (cancer, heart disease etc)
Housing – older people need specially adapted homes (bungalows, wide doorways, lower kitchen units for
those in wheelchairs etc.)
Increase care needs – old people might need to be placed in ‘sheltered accommodation’ (their own home,
but with carers visits for specific needs) or ‘nursing homes’ (where all needs are looked after). This is going to
cost!
Pension – they will claim for longer- how are we going to afford it? Impact on the economy?
Fewer workers – less young people to work and generate income? Less income from income tax and
National Insurance will be paid to the government. How will
we pay for our old people?
17. What can be done about an ageing population?
The Labour government in 2009 launched a strategy called ‘Building a
Society for All Ages’. The table on the right summarises what they
have done, but it would be far better to use Sweden as a case study
for trying to cope with an ageing population.
18. What did Sweden do combat an ageing population?
Sweden is in stage 5 of the DTM. As such, it has a population growth rate of almost zero and its fertility has dropped
from 2.1 in 1989 to 1.5 by 1999. To combat this ageing population they introduced the following measures:
13 months paid paternity leave for fathers at 80% of their salary
Extra money if couples had less than a 30 month gap between children
Child benefit for each child
Sick child care – 120 paid days per year per couple
All-day childcare and all-day schools
THESE POLICIES ARE DESCRIBED AS PRO-NATALIST! CHINA’S POLICY WAS ANTI-NATALIST.
19. What about the UK? Where do we stand in terms of our population?
Our population is ageing. The ‘oldest old’
(over 85) has risen considerably.
The average age of the UK population was
35 in 1983, but it was 40 in 2009.
Less young people will have to support the
pensioners. This is a similar situation to
that found in many other MEDCs.
The population pyramids on the right illustrates what is predicted to
happen.
It is worth noting some other key terminology here though, which is related
to the pyramids.
The lowest bars show the ‘young dependents’ – those under 15 years
old
The middle bar between the ages of 15 and 64 are the ‘economically
active population’ or ‘working population’.
The top bars over 65 years of age show the ‘elderly dependents’.
Clearly, an increase in the elderly dependents will cause problems as the
people of working age (working population) will have to support them.
20. What is the dependency ratio?
This provides an actual figure to show how many people depend on the
working population.
Children (under 15) + elderly (over 65) x 100
Working population The higher the number produced by the formula, the worse it is! In 2007, the UK had a dependency ratio of 61. Have a look at the pyramids on the right – what is going to happen? How do they compare to those shown in question 8?
21. How else can the population of a country change?
Natural increase has been the way that has been described so far in these pages. However, MIGRATION is another
key aspect that needs to be considered.
22. Why do people migrate?
Migration is the movement from one place to another. This can be legal, illegal, between regions within a country
or between countries. It can be forced (refugee?) or voluntary, seasonal or permanent. Whatever the type, the
reasons for people moving are a mixture of PUSH and PULL factors.
Push Factors Pull Factors
Not enough jobs Hope of finding a job Low wages Higher wages Poor education/ opportunities Better healthcare Poor healthcare Better education War with another country Better standard of living Lawlessness/ civil war Family links Drought/ famine Lower crime, safety etc.
23. Case study of Polish migration to the UK
When: since 2004 when Poland was admitted into the European
Union.
How many: Nobody is really sure- estimates of 1 million have been
suggested.
Where: Many have gone to the big cities, but also in rural areas to
find work on farms.
Why: Money mainly. As a result, the Poles are classified as
‘economic migrants’. Look at the table which shows you statistics
for the host country (the UK) and the source country (Poland):
Who: The Polish migrants tend mostly to be men and young (85%
below 34). 30% had a degree or similar qualification. Only 15%
wanted to stay permanently. Most are seasonal workers or had
come for a few years to make money.
24. What are the impacts of this migration?
I would urge you to read the video notes sheet that you produced
having watched ‘The Poles are coming’ film. This focussed on the
impacts on Peterborough.
UK impacts
Hard-working workforce, often where there are skills shortages
Contribute to local economy (taxes etc) and can support our
ageing population
Tend to be young, so this helps our dependency ratio
However, crime, strain on local services (school places etc.)
Poland impacts
Money sent home stimulates growth (£4 billion in 2005/6)