We have to do something like that to clear the backlog of 20 million blind eyes in India.
We perform only one million cataract surgeries a year. At this rate we cannot catch up.
Modern communication through satellites is reaching every nook and corner of the globe.
Even an old man like me from a small village in India knows of Michael Jackson and
Magic Johnson. Why can’t we bring eyesight to the masses of poor people in India, Asia,
Africa, and all over the world?
-Dr. V, founder of Aravind Eyecare System in 1992
In May 2005, Aravind Eyecare Systems (AECS), the largest and the most productive eye
care facility in India, set up their first Vision Centre (VCs) – envisaged by Vision 2020-Right
to Sight, a global initiative of International Agency of Prevention of Blindness (see Exhibit 1
for the structure of Vision 2020) in Theni District of Tamil Nadu . By the end of 2012
Aravind eye-care had set-up 45 vision centres in Tamil Nadu and is still expanding.
The aim of AECS setting vision centres is to provide primary eye care services to rural
communities. Aravind eye-care uses the concept of Tele-ophthalmology in their vision
centres. By using high speed wireless and broadband link and video-conferencing technique
doctors sitting at the satellite hospitals consult hundreds of patients in the VCs eliminating the
need of the patients to travel to hospital. This way the cost and time of both patients and
doctors are saved. The vision centres helped to increase outreach to the patients
phenomenally from 7% to 40% in its first year of operation to nearly 80% by the end of
fourth year.
Chief Medical Officer, Dr. Kim and Tele-medicine officer, Mr Nagendra Babu knew that
vision centres can help them increase their outreach and with the exponential growth of
telecom network in the country the solution seemed feasible. However, the rural mobile and
broadband penetration was still very low compared to the urban areas1. Broadband wireless
links were often not suitable for sustaining the required levels of video and sound quality for
tele-consultation. Establishing high speed reliable links in rural areas involved high capital
expenditure. Besides the private telecom operators AECS also leveraged upon Government
1–As per TRAI Press Release Feb 2013. By Dec 2012, the overall tele-density in India is 73.34%. The urban
teledensity is 149.9 and rural teledensity is 39.85. The rural broadband penetration was 36.83 compared to urban 63.53% in Oct 2012. Broadband penetration is among lowest among Asia- Pacific countries
owned agencies like ISRO-Telemedicine to scale up their operations at a faster pace. They
also knew that gradually private hospital chains are also entering the telemedicine space to
cater to the rural segments. Apollo Group has established their Telemedicine network and
others small private players were entering (see Exhibit 2 for the list of Renowned Tele-
ophthalmology Networks in India). Along with AECS, there were other entities working to
realise mission to eradicate blindness (See Exhibit 3 for mission statement of Aravind). So
question before them was what was the best strategy to realise their goal and that of Vision
2020?
Blindness problem
The term ‘Blindness’ is to used only for total vision loss and for conditions where
individuals have to rely predominantly on vision substitution skillsi (see Exhibit 4 for the
international definition of Blindness).Worldwide 195 million people are visually impaired
worldwide: 37 million are blind and 161 million are visually impaired. About 90% of the
world’s visually impaired live in developing countries. Globally, uncorrected refractive errors
are the main cause of visual impairment; cataracts remain the leading cause of blindness in
middle- and low-income countries. The number of people visually impaired from infectious
diseases has greatly reduced in the last 20 years. 70% of all visual impairment can be avoided
or cured. Globally the major causes of visual impairment are:
Cause
Percentage of
Blindness
Uncorrected refractive errors (myopia hyperopia or astigmatism) 43
Cataract 33
Glaucoma 2
(See Exhibit 5 for major reasons of blindness)
About 65% of all people who are visually impaired are aged 50 or older; while this age group
comprises about 20% of the world's population. With an increasing elderly population in
many countries, more people will be at risk of age-related visual impairment. An estimated
19 million children are visually impaired. Of these, 12 million children are visually impaired
due to refractive errors, a condition that could be easily diagnosed and corrected. 1.4 million
People are irreversibly blind for the rest of their lives ii.
Indian context
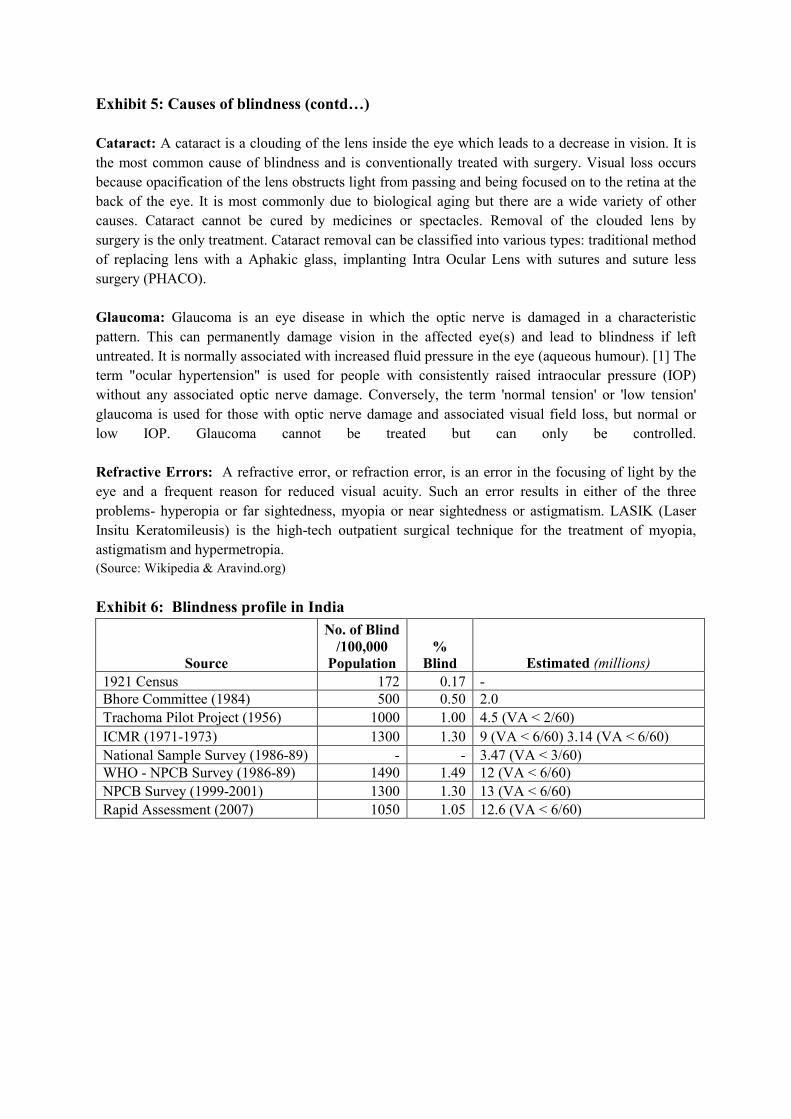
In India 12 million people are blind – the highest globally (See Exhibit 6 for blindness
profile in India). It is also home to the largest number of cataract patients. In line with the
global trend, around 75% of the blindness is avoidable or treatableiii. Blindness is prevalent
across the country at an average of 1.1% (see Exhibit 7 for a state wise distribution of low
vision prevalence in India). India has around 8000 optometrists while there is need for around
40,000.
VISION 2020 and India
Launched in 1999, Vision 2020: The Right to Sight is a global initiative to eradicate
avoidable blindnessiv. The programme is a strategic partnership between WHO and
International Agency for Prevention of Blindness (IAPB)2. 193 WHO member states are
committed to investing in eye care. A WHO Action plan for prevention of blindness and
visual impairment has been adopted at 2009 World Health Assembly. Recent data suggests
that the current estimates of blind people are around 39 million against original projected
estimate of 60 million (See Figure 1). The huge reduction in the number of blindness cases is
testimony to the impact of this initiative.
India is a strategic partner of the Vision 2020: Right to sight initiative. There has been
substantial increase in the number of eye surgeries in the past decade and a half. Though the
number of surgeries is supposed to increase from 3.38 million in 2001 to 7.63 million in
2020, the number of cataract blindness would increase from 7.75 million in 2001 to 8.25
million in 2020. So data suggest that the gap between supply and demand still exists and
complete elimination of cataract blindness cannot be achieved by 2020. Aravind Eye Care
system is a strategic partner of the Vision 2020: Right to Sight, India initiative.
Figure 1: Projected Global estimates made at the launch of VISION 2020 of the number of
blind people in the world in 2000 and how that would increase over the next two decades and
the latest 2010 data estimate of 39 million. Courtesy Dr Allen Foster.
2 International Agency for Prevention of Blindness (IAPB) is a large organization consisting of eye-care
professionals and NGOs involved in eye-care
Telemedicine Ecosystem in India and Tele-ophthalmology
World Health Organization (WHO) defines Telemedicine as “The delivery of health care
services, where distance is a critical factor, by all health care professionals using information
and communication technologies for the exchange of valid information for diagnosis,
treatment and prevention of disease and injuries, research and evaluation, and for the
continuing education of health care providers, all in the interests of advancing the health of
individuals and their communities”v. Telemedicine technology can be categorised intovi.
a. Real time or synchronous :
b. Store and forward
c. Remote monitoring
The real time or synchronous transmission allows simultaneous interaction of the doctor,
paramedics and the patients. Video conferencing is one of the most common forms of real
time telemedicine technology and demands high speed and bandwidth connection. The store
and forward technology is suitable for offline assessment of medical images, and patient
history. This technology finds application in tele-opthalmology, tele-radiology, tele-
dermatology and tele-pathology. Remote monitoring is beneficial for managing patients when
the patients cannot reach the doctors easily or the costs/time involved are unreasonably high
In accessing the doctors.
In India current doctor-population ratio has been worked out to be 1:1953vii. There is extreme
shortage of doctors and the ratio is even more skewed in the rural areas. Around 70% of the
Indian population still resides rural areas whereas around 70% of the doctors are concentrated
in the urban areas. The ratio in rural area stands as 1:25,000. The estimated shortage of
doctors is 600,000 and that of nurses is 1 million. The gruesome statistics of the state of
healthcare in India makes telemedicine all the more a necessity.
The major stakeholders involved in telemedicine ecosystem are the government, medical
fraternity, IT companies and network providers. (See Exhibit 8 on the Stakeholders in
Telemedicine and Exhibit 9 for Telemedicine ecosystem in India). The telemedicine policy
initiatives in India are still in their nascent stage (See Exhibit 10 for Policy initiatives for
telemedicine by govt. of India). But the telemedicine market in India has witnessed
significant growth in the recent years. In 2012 it is estimated to have a market size of $7.5
million and is expected to have a CAGR of 20% for the next five years.viii
Teleophthalmology in India
In India the Ophthalmologist to patient ratio is 1:100,000 of the population and more than
70% of them reside in urban areasix. This acute shortage of ophthalmologists in India caused
tele-ophthalmology3 to be one of the most popular forms of telemedicine delivery model in
3 It is the branch of telemedicine that delivers eye care through digital medical equipment and
telecommunications technology. Today, applications of teleophthalmology encompass access to eye specialists
India. A number of Tele-ophthalmology networks exist (See Exhibit 2 for Renowned Tele-
ophthalmology Networks in India) and Aravind eye care is one of the foremost players in this
sector. The most common form of delivery model is through mobile camps and mobile vans
where tele-consultation is delivered through satellite links (often government sponsored
satellite links like ISRO’s VSAT).
Barriers to Telemedicine in Indiax:
The telemedicine industry in India is still in its inception stage. The barriers to telemedicine
are not only lack of low cost innovations but negative attitude of the people especially among
rural people due to lack of education and awareness. The acceptance among patients is found
to be satisfactory but physicians often show resistance due to aversion to change from the
traditional practices. The lack of reliable telecom coverage and the skewed distribution in the
rural areas is also a barrier that impedes its rapid adoption. Also there is an acute shortage of
skilled manpower that are educated enough to handle the telemedicine equipment and the IT
software. Finally there are no concrete policy initiatives from the Govt. of India which can
facilitate dissemination of the technology.
Aravind Eye Care System: Tele-ophthalmology
Starting with a 11-bed hospital in Madurai in 1976 Aravind Eye Care has grown into 7
hospitals with more than 4000 beds. By March 2012 over 2.8 million outpatients were treated
and over 140,000 surgeries were performed.4 Over the years Aravind has grown into a system
with its own manufacturing division-Aurolab, research institute and training institute
producing country’s best ophthalmologist (See Exhibit 11 for Aravind Eye Care System –
Services). Although more than 60% of its surgeries are done for free, AECS still manages to
generate surplus and ploughs it back to the expand its operations.
Mr Subeesh, Cornea Clinic Manager said:
Optimal usage of resources and economies of scale are critical to our success. 60%
of our workforces are paramedics and we hire girls directly after class 12 instead of
hiring them after BSc. In this way we train them for purpose specific to our needs.
Also while recruiting we look more for attitude than skills because of our
philanthropic roots. Doctors perform two surgeries at the same time- two table
approach. Our doctors perform around 2000 operations per year where the national
average is around 500.
In order to increase its reachability Aravind adopted Tele-ophthalmology (See Exhibit 12 for
Aravind’s Tele-ophthalmology network). Its primary aim is to provide low-cost and
accessible eye-care service by reducing the travel cost and time. Tele-ophthalmology is
delivered mainly through Vision Centres (VCs). The first VC was established in Theni in
2004. Presently there are 41 VCs in various parts of Tamil Nadu which has helped the eye-
for patients in remote areas, ophthalmic disease screening, diagnosis and monitoring; as well as distant learning. http://en.wikipedia.org/wiki/Teleophthalmology, accessed on March 9, 2013 4 http://www.aravind.org/ClinicalServices.aspx, accessed on March 12, 2013
care service reachability increase from 7% to 80% within 4 years of operation in the area.
The cost of setting up a VC is around INR 0.3 million and cost of running it is INR 30,000.
Vision Centres
A Vision Centre (VC) is a permanent community eye care facility which acts as the first point
of interface of the population with comprehensive eye care services provided by an exclusive
skilled eye care workerxi. Vision 2020 attributes the following main characteristics to the
VCsxii.
• A permanent basic eye care facility servicing a population of 50,000.
• Networked with a secondary eye care institution (service centre) preferably within a
distance of 50 KM for taking care of referrals.
• Financially sustainable within a span of 2-3 years of establishment.
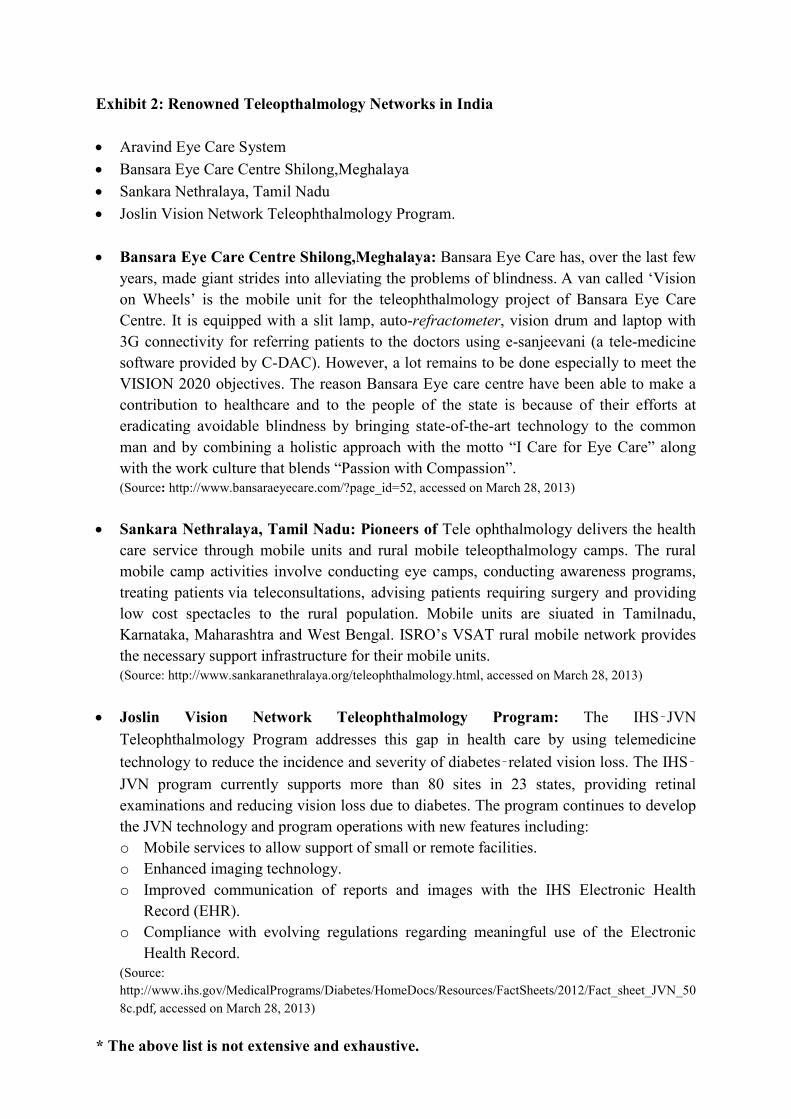
• An estimated number of 20,000 VCs (See Exhibit for Eye-care Delivery Pyramid in
India by Vision 2020 programme, India) is required to achieve the goals set by Vision
2020 programme.
Aravind eye care set up its vision centre in an aim to increase its outreach in the rural areas
and improve the utilization of the services and resources (doctors). The service delivery
model of VCs adopted by AECS is shown in Figure 2.
Figure 2: Patient flow process- Vision Centre
(Source: Aravind Eye care, http://www.aravind.org/telemedicine/vc.htm, accessed on February 23, 2013)
A Visit to the Aravind Eye Care at Coimbatore
Vision Centre
We the case writers reached Hotel Le Meridien at around 10.30 am in the morning where
the International Telemedicine Conference 2012: Telemedicon 125 hosted by Aravind
Eyecare system was going on. Mr. Subeesh, Cornea clinic manager received us and then we
stared out journey for the nearest VC at Kinathukadavu, Coimbatore. The journey by car
took around 20-25 mins. It was a rented building having around 200-250 sq. ft. of area.
(Exhibit 13 shows the picture of VC at Kinathukadavu, Coimbatore). The functioning time
of VC is from 9 am to 5 pm and is open for all weekdays except Sunday. It handles around
25-30 patients each day. Patients are charged Rs. 20 for registration and Rs 40 for blood
sugar test (insisted for patients with age above 40).
Mr Subeesh said-
VCs are established in an area with population of 50,000-1, 00,000. Before
establishing any VC, a detailed survey about the demographic and eye-care facilities
available in the area is done. A report is prepared (photos of few pages of the report
was taken). Also several pamphlets and flyers on eye-care awareness are made
available in the VC in Tamil language.
Entering the VC, there was a reception area (See Exhibit 16 for Vision Centre Required
Material List). There was a desktop computer where patients came and registered
themselves. The registration process took less than 1 min. The registration was completed
using application software, an in-house creation of the AECS (Exhibit 15 shows the patient
registration system at Aravind’s Vision Centre). After registration the patients waited in
the reception area. The reception area has a small pitcher containing drinking water, posters
of eye and eye ailments, treatment were hung on the wall to increase awareness among the
patients. There was a white board on which the progress report of the VC since its inception
(31st Oct. 2007) (Exhibit 15) in terms of OT patients, number of patients referred to main
hospital, number of spectacle lenses ordered, etc. are written. The normal waiting time in the
reception was observed to be not more than 4-5 minutes. In some cases there was no waiting
time also.
A clinical attendant calls 2-3 patients from the reception area to the clinical testing room and
asks them to wait a bench in the room while she attends a patient one by one.
There was a slit-lamp unit. Also there is a broadband system for accessing internet access, a
web cam, a digital camera. There is also all the arrangement for checking the refractive
power of the lenses for vision correction.
The entire workflow was in accordance with the flowchart given in Aravind website (Figure
3).
5 8th Annual Conference of the Telemedicine Society of India, to be held at Hotel Le Meridien, Coimbatore
during Nov 29th to Dec 1st 2012
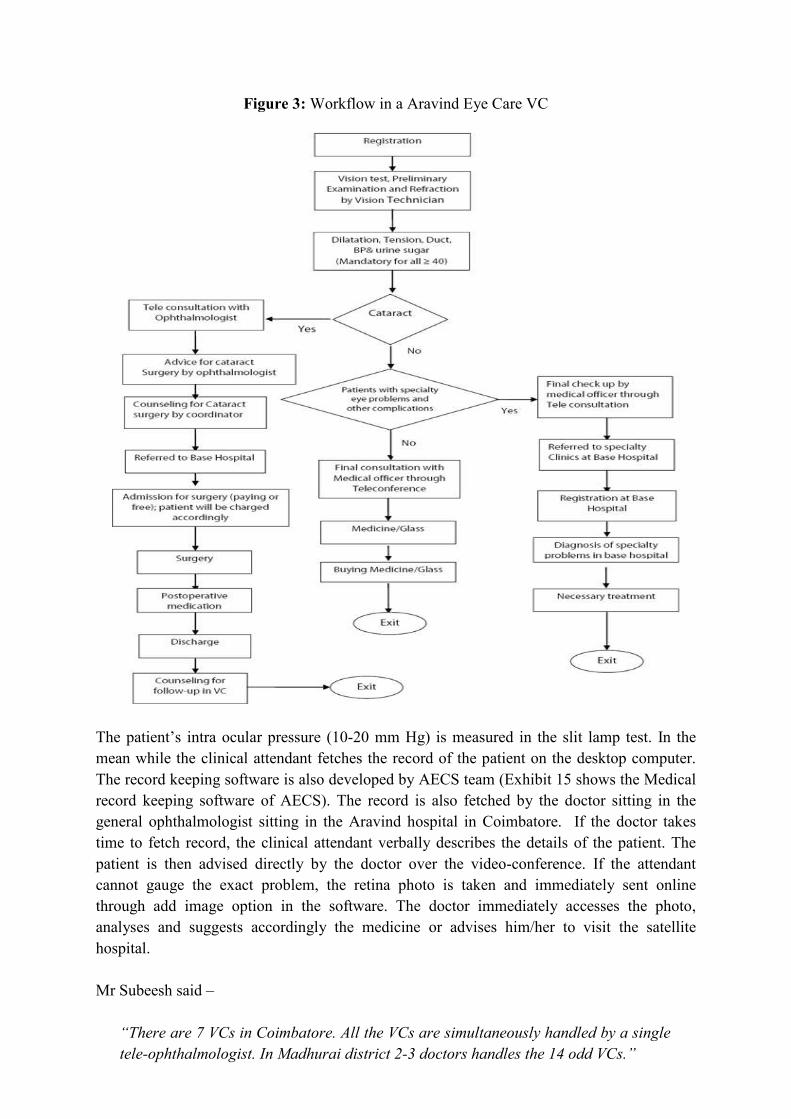
Figure 3: Workflow in a Aravind Eye Care VC
The patient’s intra ocular pressure (10-20 mm Hg) is measured in the slit lamp test. In the
mean while the clinical attendant fetches the record of the patient on the desktop computer.
The record keeping software is also developed by AECS team (Exhibit 15 shows the Medical
record keeping software of AECS). The record is also fetched by the doctor sitting in the
general ophthalmologist sitting in the Aravind hospital in Coimbatore. If the doctor takes
time to fetch record, the clinical attendant verbally describes the details of the patient. The
patient is then advised directly by the doctor over the video-conference. If the attendant
cannot gauge the exact problem, the retina photo is taken and immediately sent online
through add image option in the software. The doctor immediately accesses the photo,
analyses and suggests accordingly the medicine or advises him/her to visit the satellite
hospital.
Mr Subeesh said –
“There are 7 VCs in Coimbatore. All the VCs are simultaneously handled by a single
tele-ophthalmologist. In Madhurai district 2-3 doctors handles the 14 odd VCs.”
There was a generator unit to meet the power requirements during power cuts .The entire
process from registration to entire consultation takes 15-20 minutes.
Aravind eye hospital, Coimbatore
This Aravind hospital managed all the VCs in Coimbatore and the nearby areas. It acts as the
central hub for the VCs (the spokes6) where doctors tele-consulted the patients visiting the
VCs. They use the IHMS (Integrated Hospital Management Software). Each clinic in addition
has its own special management software. Whenever a patient enters the clinic he/she is
checked into the system and a similar entry is made when they leave.
During the visit, on interaction with different personnel the different inputs gathered on
telemedicine, its viability in the long run (from Aravind’s management perspective) and
barriers to growth.
Telemedicine- equalizer for access to rural health
• To increase reachability. Initially we could reach only 7% of the affected patients. But
now with the installation of VC within one year of operation around 40% of the
patients are reached and within 4 yrs. of operation 83% of the patients are reached.
We are now able to reach around 700 patients per day through VCs which would not
have been possible otherwise.
• They become the primary screening centres (eye camps are secondary and
hospital-tertiary). Common eye problems like irritation, change of specs, etc. get
solved at the place itself. So it creates a win-win situation both for patients and the
Hospital. For patients it leads to reduced cost of patient to travel to the hospital and no
loss of one day of wage. For Aravind it leads reduced the cost of hospital in catering
to so many patients at the hospital. It leads to better management, reduced service
time and better allocation of scare resources among more critical case. Less than 10%
of the patients visiting the VCs are actually referred to hospital. Cost of setting up a
VC is around 5 lakhs (capital expenditure).
Issues faced for Telemedicine set-up:
• Last mile connectivity
Connectivity which is prime enabler for the telemedicine also remains the foremost
constraint.
The health data in real time requires reliable, high bandwidth link from the distant
outlet to transfer data to the speciality hospital. The basic infrastructure had to be
developed from the scratch, first connect the marked geographical area with the
6 Hub & Spoke Model, http://en.wikipedia.org/wiki/Spoke-hub_distribution_paradigm, accessed on March 23,
2013
hospital. The connectivity options are broadband and wireless link in free spectrum
(2.4 and 5.8 GHz).There are pros and cons to both of these mode of connectivity.
For wireless link between Vision centres and Aravind Eye Hospital, the project was
initiated with the help of Intel Research Berkeley lab in 2006. Over a period of time, it
helped in penetration in far flung areas. In current scenario, at times Wireless links
were unreliable. The cost of installing them was also quite high- they required
repeaters at frequent distance.
For fixed lines, the network of Broadband line is strengthening in our country due to
various initiatives like SWANs (State Wide Area Network). Now Broadband line is
used in places where there are already fixed lines available and preferred over
establishment of wireless link.
• IT backbone and various connectivity platforms
For the Telemedicine set up to be up and running smoothly a team of IT and
networking professional is a prerequisite, along with doctor and Para-medical staff. In
present scenario, when there is explosion of myriad range of software and platforms
available, the best suitable customised package as per the AECS operational
requirement is to be evolved by the AECS IT team.
The connectivity options are to be wisely considered from the available options of
wired Broadband, wireless links and FTTx.
Dr Kim said:
“In 2yrs time we are going to set up a hospital in Chennai. Presently there are
42-43 VC s and we plan to take it to around 100.”
• Manpower Issues
Human resource is the main issue faced by AECS. There is no substantial attrition
rate among doctors, but when there is a need to set up a VC in rural area it is difficult
to find willing people, so in most cases AECS recruit and train the locals. Generally
AECS recruit freshers in technician and doctor position so they can be easily groomed
and inculcate the work culture and are enthusiastic attitude towards social
entrepreneurship
The Decision
Dr. Kim wondered what should be the best strategy to realise the vision 2020. In the short run
he wants to reach the maximum number of patients in Tamil Nadu and nearby geographic
areas (South India). With recent boom of telecom network in the state increasing the number
of VCs has become more feasible (See Exhibit 17 for rural teledensity of Tamil Nadu). But
he was yet undecided on the capacity expansion in order to meet the vision of Vision 2020.
Exhibits:
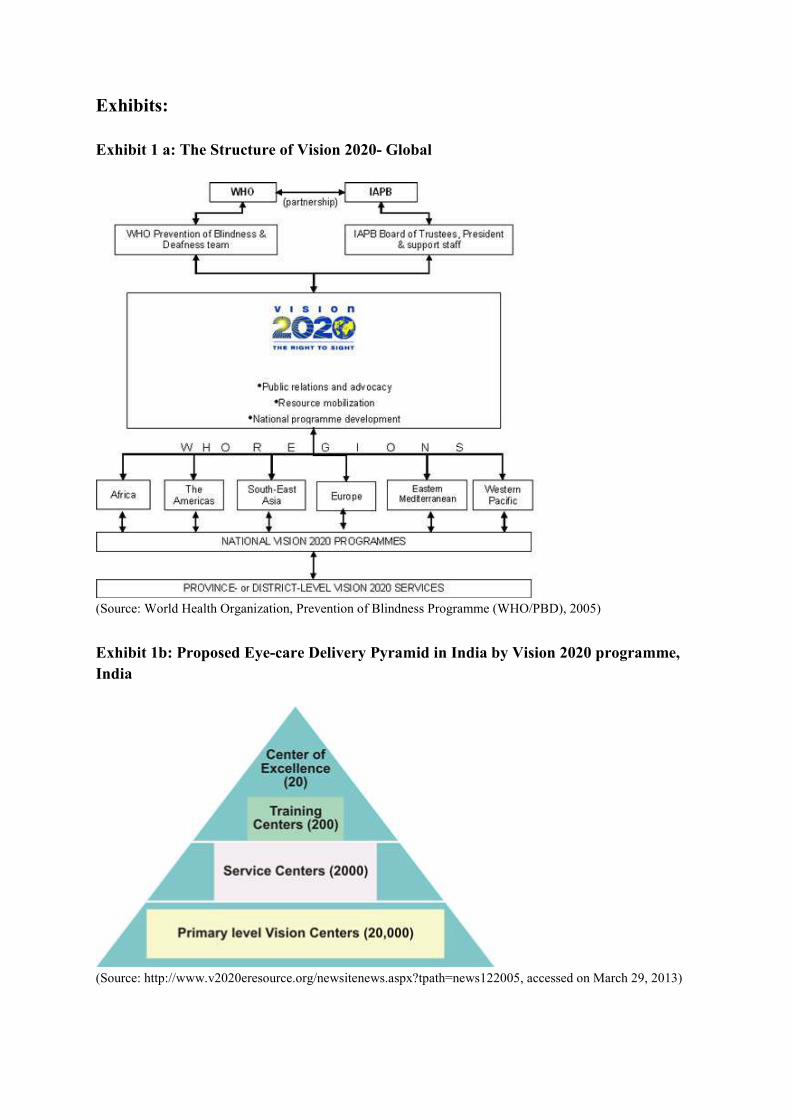
Exhibit 1 a: The Structure of Vision 2020- Global
(Source: World Health Organization, Prevention of Blindness Programme (WHO/PBD), 2005)
Exhibit 1b: Proposed Eye-care Delivery Pyramid in India by Vision 2020 programme,
India
(Source: http://www.v2020eresource.org/newsitenews.aspx?tpath=news122005, accessed on March 29, 2013)
Exhibit 2: Renowned Teleopthalmology Networks in India
To eradicate needless blindness by providing appropriate compassionate and high quality
eye care to all.
Exhibit 4: Definition of Blindness: Resolution adopted by the International Council of
Ophthalmology Sydney, Australia, April 20, 20027 (abridged)
WHEREAS lack of clarity about the appropriate use of the term “Blindness” has led to confusion
about its definition and to varying reports about its prevalence and incidence and
WHEREAS the mission of ophthalmology and the International Council of Ophthalmology is not
limited to the prevention of blindness, but also includes the prevention and remediation of lesser
levels of vision loss, which do not fit under the term “blindness”,
THEREFORE, be it resolved that the International Council of Ophthalmology, at its meeting in
Sydney, Australia, April 2002.
(A) Recommends to the World Vision Community the use of the following terminology8:
• Blindness – to be used only for total vision loss and for conditions where individuals have to rely
predominantly on vision substitution skills.
• Low Vision – to be used for lesser degrees of vision loss, where individuals can be helped
significantly by vision enhancement aids and devices.
• Visual Impairment – to be used when the condition of vision loss is characterized by a loss of
visual functions (such as visual acuity, visual field, etc.) at the organ level. Many of these
functions can be measured quantitatively.
• Functional Vision – to be used to describe a person’s ability to use vision in Activities of Daily
Living (ADL). Presently, many of these activities can be described only qualitatively.
• Vision Loss – to be used as a general term, including both total loss (Blindness) and partial loss
(Low Vision), characterized either on the basis of visual impairment or by a loss of functional
vision.
7 A full discussion of the rationale behind these recommendations can be found in the ICO report “Visual Standards – Aspects and Ranges of Vision Loss, with emphasis on Population urveys”, prepared by August Colenbrander, MD, for the 2002 meeting. The report can be down-loaded from the ICO web site: www.icoph.org/pdf/visualstandardsreport.pdf. 8 This terminology does not preclude the possibility that the visual condition could subsequently be improved by medical, refractive or surgical intervention
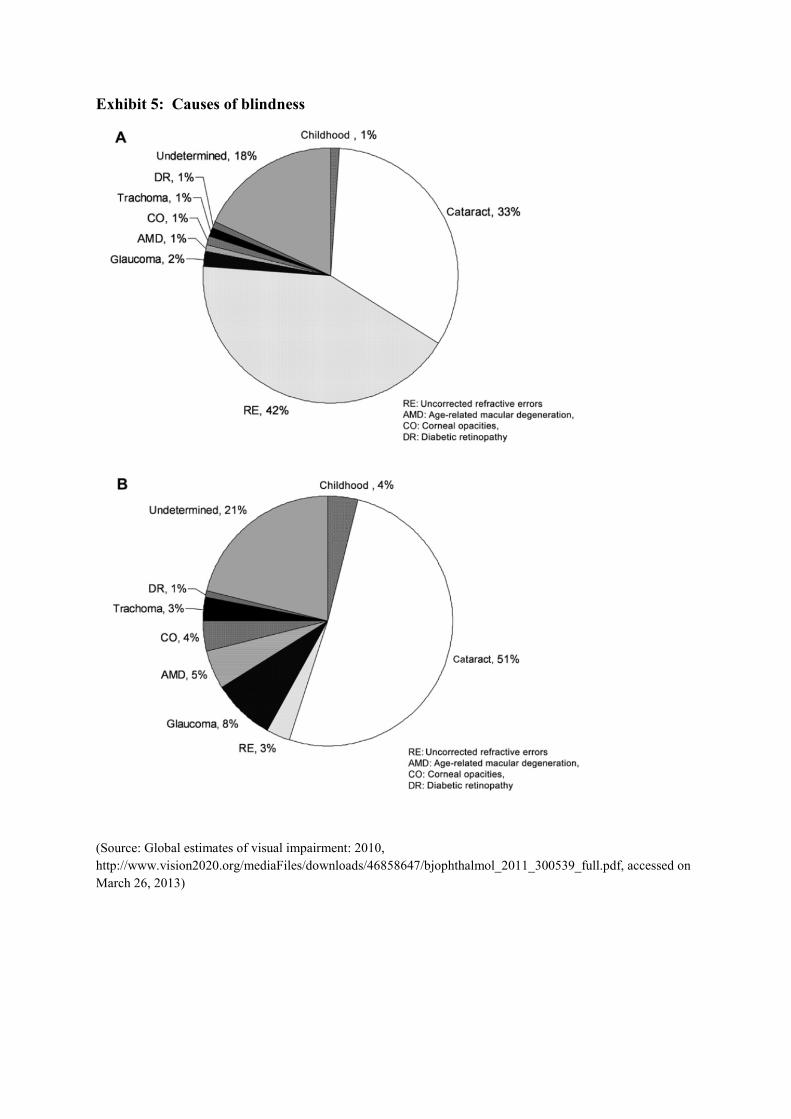
Exhibit 5: Causes of blindness
(Source: Global estimates of visual impairment: 2010,
http://www.vision2020.org/mediaFiles/downloads/46858647/bjophthalmol_2011_300539_full.pdf, accessed on
March 26, 2013)
Exhibit 5: Causes of blindness (contd…)
Cataract: A cataract is a clouding of the lens inside the eye which leads to a decrease in vision. It is
the most common cause of blindness and is conventionally treated with surgery. Visual loss occurs
because opacification of the lens obstructs light from passing and being focused on to the retina at the
back of the eye. It is most commonly due to biological aging but there are a wide variety of other
causes. Cataract cannot be cured by medicines or spectacles. Removal of the clouded lens by
surgery is the only treatment. Cataract removal can be classified into various types: traditional method
of replacing lens with a Aphakic glass, implanting Intra Ocular Lens with sutures and suture less
surgery (PHACO).
Glaucoma: Glaucoma is an eye disease in which the optic nerve is damaged in a characteristic
pattern. This can permanently damage vision in the affected eye(s) and lead to blindness if left
untreated. It is normally associated with increased fluid pressure in the eye (aqueous humour). [1] The
term "ocular hypertension" is used for people with consistently raised intraocular pressure (IOP)
without any associated optic nerve damage. Conversely, the term 'normal tension' or 'low tension'
glaucoma is used for those with optic nerve damage and associated visual field loss, but normal or
low IOP. Glaucoma cannot be treated but can only be controlled.
Refractive Errors: A refractive error, or refraction error, is an error in the focusing of light by the
eye and a frequent reason for reduced visual acuity. Such an error results in either of the three
problems- hyperopia or far sightedness, myopia or near sightedness or astigmatism. LASIK (Laser
Insitu Keratomileusis) is the high-tech outpatient surgical technique for the treatment of myopia,
astigmatism and hypermetropia.
(Source: Wikipedia & Aravind.org)
Exhibit 6: Blindness profile in India
Source
No. of Blind
/100,000
Population
%
Blind Estimated (millions)
1921 Census 172 0.17 -
Bhore Committee (1984) 500 0.50 2.0
Trachoma Pilot Project (1956) 1000 1.00 4.5 (VA < 2/60)
Exhibit 7: State wise blindness distribution in India
Prevalence of Blindness and Estimated Number of Blind Persons in India (2004)
States/UTs
Census
Population
(2001)
Annual
Growth
Rate*
Estimated
Population
2004
Prevalence
of
Blindness
Estimated
Blind
Persons
(in Lakh)
Andaman and Nicobar Islands 356265 2.39 381809 0.67 0.03
Andhra Pradesh 75727541 1.3 78680915 1.5 11.8
Arunachal Pradesh 1091117 2.33 1167386 1.23 0.14
Assam 26638407 1.73 28020940 1.34 3.75
Bihar 82878796 2.5 89094706 0.78 6.95
Chandigarh 900914 3.39 992537 1.89 0.19
Chhattisgarh 20795956 1.66 21831595 1.61 3.51
Dadra and Nagar Haveli 220451 4.65 251204 1.07 0.03
Daman and Diu 158059 4.42 179018 1.07 0.02
Delhi 13782976 3.81 15358370 0.63 0.97
Goa 1343998 1.39 1400043 2.03 0.28
Gujarat 50596992 2.03 53678349 1.07 5.74
Haryana 21082989 2.47 22645238 1.13 2.56
Himachal Pradesh 6077248 1.62 6372602 0.7 0.45
Jammu and Kashmir 10069917 2.55 10840266 1.61 1.75
Jharkhand 26909428 2.09 28596649 0.78 2.23
Karnataka 52733958 1.59 55249368 1.78 9.83
Kerala 31838619 0.9 32698262 0.56 1.83
Lakshadweep 60595 1.59 63485 0.89 0.01
Madhya Pradesh 60385118 2.18 64334305 1.16 7.46
Maharashtra 96752247 2.04 102673485 95 9.75
Manipur 2388634 2.63 2577097 0.65 0.17
Meghalaya 2306069 2.62 2487326 0.22 0.05
Mizoram 891058 2.56 959491 0.65 0.06
Nagaland 1988636 4.97 2285142 0.38 0.09
Orissa 36706920 1.48 38336707 1.4 5.37
Pondicherry 973829 1.87 1028461 0.78 0.08
Punjab 24289296 1.8 25600918 1.01 2.59
Rajasthan 56473122 2.49 60691664 1.55 9.41
Sikkim 540493 2.85 586705 0.45 0.03
Tamil Nadu 62110839 1.06 64085964 0.78 5
Tripura 3191168 1.46 3330941 1.18 0.39
Uttar Pradesh 166052859 2.3 177510506 0.94 16.69
Uttaranchal 8479562 1.76 8927283 0.56 0.5
West Bengal 80221171 1.64 84168053 1.19 10.02
India 1027015247 1.93 1087086789 1.1 119.72 Note: *: Census of India 2001.
Compiled from the statistics released by: Rajya Sabha Unstarred Question No. 1712, dated
17.12.2004
Exhibit 8: Stakeholders in Telemedicine
Exhibit 9: India’s telemedicine ecosystem
Government initiatives:
• ISRO (Indian Space Research Organisation) has initiated a number of Telemedicine pilot
projects. These projects consist of, linking through Indian National Satellite (INSAT),
remote/rural areas like Jammu, Kashmir & Ladhakh in north near Himalayas, Offshore
Islands of Andaman and Lakshadweep, North Eastern States District Hospitals/Health
Centres. RO’s telemedicine initiative includes providing connectivity between remote/rural
hospital and super specialty hospital for tele-consultation, treatment and training, Continuing
Medical Education (CME) and Mobile Telemedicine units for rural and community health.
Presently ISRO’s Telemedicine Network consists of 245 Hospitals – 205
Remote/Rural/District Hospital/Health Centre connected to 40 Super Specialty Hospital
located in the major cities. ISRO has also evolved the concept of Village Resource Center
(VRC) and implemented through a partnership with M S Swaminathan Research Foundation
(MSSRF). This satellite based project, ISRO-MSSRF-VRC, aims for digital connectivity to
remote villages for providing multiple services such as telemedicine, tele-education and
remote sensing applications through a single window.
• DIT (Department of Information & Technology, Govt. of India): DIT has taken
initiatives for development of technology, initiation of pilot schemes and standardization of
Telemedicine in the country. It has established more than 75 nodes all over India and support
research and development as under:
o Development of telemedicine software systems under the project “Development of
Telemedicine technology and its applications towards optimisation of medical resources”
by C-DAC and validation for three premier medical institutions- viz. SGPGIMS,
Lucknow, All India Institute of Medical Sciences (AIIMS), New Delhi and Postgraduate
Institute of Medical Education and Research (PGIMER), Chandigarh using ISDN &
Satellite connectivity.
o For diagnosis & monitoring of tropical diseases in West Bengal using Wide Area
Network (WAN), developed by Webel (Kolkata), Indian Institute of Technology,
Kharagpur and School of Tropical Medicine (2 nodes).
o Kerala Oncology Network for providing services for cancer detection, treatment pain
relief, parient follow-up and continuity of care in peripheral hospitals of regional Cancer
Center, (RCC), Trivendrum (5 nodes). A Telemedicine solution to provide specialty
health services to remote areas of north-eastern states of India at Naga Hospital Kohima
and remote states of Mizoram and Sikkim with support from Marubeni India Ltd., Govt.
of Nagaland and Apollo Hospital, Delhi.
o Undertook initiative, in a project mode, for defining “The framework for Information
Technology Infrastructure for Health (ITIH)” to efficiently address information needs of
different stakeholders in the healthcare sector.
• Ministry of Health & Family Welfare (MoH & FW), Govt. of India:
o Approved tele-ophthalmology project to provide eye care specialty services to the
patients of rural and remote areas of Punjab, Uttar Pradesh, West Bengal states of India
through tele-ophthalmology mobile van.
o Draft proposal for National Telemedicine Grid has also been prepared by ISRO and
submitted to MoH&FW
o Has set up a National Task Force on Telemedicine in the year 2005 is addressing various
issues in telemedicine in national context. Various sub-committees are working on these
issues to develop a national policy document.
• Ministry of External Affairs (MEA):
o SAARC telemedicine network: In the 14th SAARC Summit held in New Delhi in April
2007 it was decided to evolve a joint telemedicine project. The preparatory work for pilot
project connecting one/two hospitals in each of the SAARC countries with 3-4 Super
Speciality hospitals in India by the end of this year has started. The Super Specialty
hospitals in India include the AIIMS, New Delhi; SGPGIMS, Lucknow; PGIMER
Chandigarh and the CARE Hospital, Hyderabad.
o Pan-African e network project: The Ministry of External Affairs, Government of India
is implementing this project through Telecommunications Consultants India Ltd. (TCIL),
which has been designated as implementing agency, to establish a VSAT based Tele-
Medicine and Tele-Education infrastructure for African Countries in 53 nations of the
African Union by a satellite and fiber optic network that would provide effective Tele-
Education, Tele-Medicine, Internet, Videoconferencing and VoIP services and also
support e-Governance, e-Commerce, infotainment, resource mapping and meteorological
services. Ten super specialty hospitals in India have been identified to provide telehealth
services to 53 remote African hospitals.
• National Informatics Centre (NIC):
o Initiated the telemedicine activities for the peripheral doctors of the Orissa and North East
region of the country.
o Published a hand book on “e-Governance through ICT” summarizing the e-Governance
projects including health across the country.
Govt. Hospitals cum Academic Initiatives:
• AIIMS Delhi
• PGIMER Chandigarh
• SGPGIMS Lucknow
• TMH
• PBDSPGIMS
• CSMMU
IT software providers: The following is a list of integrated telemedicine solution provider
• Mercury
• TELEMED
• Sanjeevani
• Televital
• Telemedik
• Sanjeeva
• Medintegra
• Tele-Doctor
• Prognosis
• i- Diagnosis
Policy initiatives for telemedicine by govt. of India:
• Department of Information Technology (DIT), Ministry of Communications and Information
Technology (MCIT), has taken initiative on the evolution and adaptation of standards of
telemedicine under the aegis of the “Committee for Standardization of digital information to
facilitate implementation of telemedicine systems using information technology (IT) enabled
services”.
• National Task Force on Telemedicine by Ministry of Health & Family Welfare
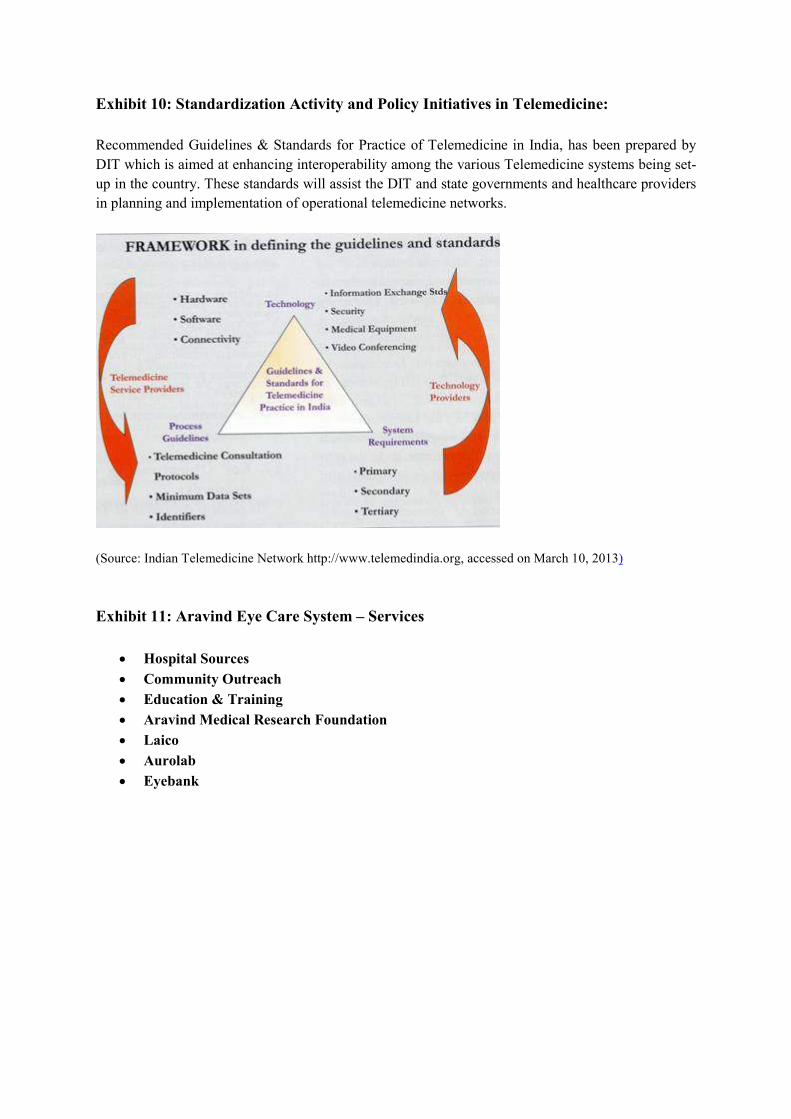
Exhibit 10: Standardization Activity and Policy Initiatives in Telemedicine:
Recommended Guidelines & Standards for Practice of Telemedicine in India, has been prepared by
DIT which is aimed at enhancing interoperability among the various Telemedicine systems being set-
up in the country. These standards will assist the DIT and state governments and healthcare providers
in planning and implementation of operational telemedicine networks.
(Source: Indian Telemedicine Network http://www.telemedindia.org, accessed on March 10, 2013)
Exhibit 11: Aravind Eye Care System – Services
• Hospital Sources
• Community Outreach
• Education & Training
• Aravind Medical Research Foundation
• Laico
• Aurolab
• Eyebank
Exhibit 12a: Aravind Tele-Ophthalmology network
Exhibit 12 b Arvind Tele-opthalmology Networks’s Scope of Work
(Source: http://www.aravind.org/telemedicine/index.htm, accessed on March 16, 2013)
Exhibit 14: List of Vision Centres of Aravind
LIST OF VISION CENTRES
Presently Aravind has the following 41 Vision Centres which are functioning very well.9
Base Hospitals Vision Center Functioning from
Madurai
Alanganallur 16-Apr-07
Tiruppuvanam 16-Apr-07
Rameshwaram 13-Jun-07
Gandhigram 17-Sep-07
Natham 28-Jan-08
Sholavandan 10-Mar-08
Manamadurai 29-Sep-08
Usilampatti 12-Dec-08
Sattur 11-Mar-10
Singampunari 12-Mar-10
Kariapatti 04-Jun-10
Peraiyur 03-Sep-10
Kalaiyarkoil 10-Sep-10
Srivilliputhur 02-Sep-11
Vedachandur 17-May-12
Devakottai 02-Aug-12
Theni
Andipatti 01-Dec-04
Bodi 14-Sep-05
Chinnamanur 20-Mar-06
Periyakulam 24-May-06
Thevaram 17-Oct-08
Batlagundu 29-Oct-08
Kandamanur 19-Jan-11
Tirunelveli
Kallidaikurichi 30-Apr-07
Srivaikuntam 02-May-07
Surandai 22-Feb-08
Vilathikulam 25-Feb-08
Valliyur 13-Oct-08
Kadayanallur 05-Dec-11
Coimbatore
P.N.Palayam 08-Aug-07
Kinathukadavu 10-Oct-07
P.Puliyampatti 22-Feb-08
Annamalai 19-Nov-08
Thondamuthur 30-May-12
Pongalur 16-Jul-11
Uthukuli 18-Aug-11
Pondicherry
Tirukkanur 18-Jun-07
Marakkanam 14-Jul-07
Kurunchipadi 06-Feb-08
Nellikuppam 11-Apr-08
Ulundurpet 19-Jan-11
9 As obtained from Aravind’s website on 23 April 2012
Exhibit 15: Vision Centre at Kinathukadavu, Kovai, Coimbatore, TN, India
Reception Area of the VC
Exhibit 16 shows the snapshot of Medical record keeping software of AECS
Exhibit 17: Vision Centre Required Material List
VISION CENTER REQUIRED MATERIAL LIST
1 Ophthalmic Equipment
Ophthalmoscope 1
Slit lamp 1
90 D lens 1
Schiotz Tonometer 1
2 Medical apparatus
Stethoscope 1
BP apparatus 1
Weighing machine (optional) 1
Thermometer 1
Glucometer 1
Sterilizer needle 1
Single Drum Surgical Autoclave (14" X 12") 1
First aid box
3 Refraction unit
Trial set with frame 1
Streak retinoscopy 1
Snellen's chart (Drum) 1
Mirror used in the refractive cubicle 1
JCC and IPD Scales 1 set
Near vision chart 1
Torchlight 1
4 Computer & Communication
Computer (monitor),CPU,UPS 1
Digital camera/Webcam with better resolution 1
Head phone with mike 1
Speaker 1 set
Printer 1
Phone 1
Internet Connectivity/wi-fi 1
4 Optical dispensing
Grinding edging kit&machine 1
Frame warmer 1
5 Furniture and Fixtures (Minimum)
Table 2
Computer table 1
Bench to measure tension and duct 2
Chairs 9
Examination chairs 2
Cupboard 1
Rack to store case sheets 1
Spectacle Display arrangement 1
Aravind Eye Care System
Exhibit 18: Teledensity of Tamil Nadu
Telephone per 100 Population (Teledensity) in Urban/Rural Areas in Tamil Nadu
(As on 31.12.2011)
Circle
Tele-Density (%) Telephones %age of
Rural
Phones to
Overall
Phones Overall Urban Rural Overall Urban Rural
Tamil Nadu 105.96 160.17 53.95 63852256 47259185 16593071 25.99
Chennai 170.18 NA NA 15268853 15162303 106550 0.70
India 76.86 167.46 37.52 926547689 611157850 315389839 34.04
Number of Villages with Direct Access to Telecom Facilities in Tamil Nadu
(As on 31.03.2011)
Circle
No. of Villages
(Rev. W.e.f.
Oct.07)
Villages Covered with VPTs as on
PCOs (PSUs) as on
(Local+ STD+ Highway) Public Private*
Total
VPTs
Tamil Nadu 13837 13837 0 13837 155319
Chennai 1655 1655 0 1655 75121
India 593601 575663 3425 579088 1570574
Endnotes
iReport prepared for the International Council of Ophthalmology, at the 29th International Congress of Ophthalmology Sydney, Australia, April 2002 ii Visual impairment and blindness Fact Sheet N°282, June 2012 http://www.who.int/mediacentre/factsheets/fs282/en/, accessed on March 12, 2013 iii Vision 2020 website: http://www.vision2020india.org/index.php, accessed on March 12, 2013 iv Vision 2020: the right to sight http://www.vision2020.org/main.cfm, accessed on March 12, 2013 v WHO. A health telematics policy in support of WHO’s Health-For-All strategy for global health development: report of the WHO group consultation on health telematics, 11–16 December, Geneva, 1997. Geneva, World Health Organization, 1998. vi http://en.wikipedia.org/wiki/Telemedicine#Types_of_telemedicine, accessed on March 1, 2013 vii PMO pushing to ramp up poor doctor-patient ratio, Kounteya Sinha, TNN Mar 6, 2012 http://articles.timesofindia.indiatimes.com/2012-03-06/india/31127057_1_health-ministry-nchrh-bill-human-resources, accessed on March 6, 2013 viii KIT: Telemedicine market in India http://www.business-standard.com/article/management/kit-telemedicine-market-in-india-112040900033_1.html ix http://laico.org/v2020resource/files/teleophthalmolog_in_india.PDF, accessed on March 9, 2013 x http://www.telemedindia.org/telemedicine.html#E, accessed on March 11, 2013 xi Definition adapted from Vision Centre manual of VISION 2020: The Right to Sight INDIA Publication, Dec 2011. Pg-7. http://www.vision2020india.org/pdfs/Vision-Centre-Manual-2012.pdf, accessed on March 16, 2013 xii See Vision centre manual, Dec 2011 of Vision 2020 for more details. http://www.vision2020india.org/pdfs/Vision-Centre-Manual-2012.pdf, accessed on March 6, 2013