33
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc
| Date post: | 12-Apr-2019 |
| Category: |
Documents |
| Upload: | truongtuong |
| View: | 217 times |
| Download: | 0 times |
ARDS Assisted ventilation and
prone positionICU Fellowship Training
Radboudumc

respiratory mechanics and other factors [10] such that it does not reliably reflect respiratory drive or effort. It is also influenced by the level of pressure support: under pressure support, respiratory rate can decrease indepen-dently from respiratory drive when mechanical insuf-flation is prolonged into the patient’s neural expiration (i.e., when the ventilator cycling is delayed) [11]. Some patients may also have high inspiratory effort in the absence of tachypnea.
To date, there is no direct measure of the central respir-atory center’s activity. However, if spontaneous breathing is preserved, respiratory center output can be assessed simply and non-invasively in mechanically ventilated patients by measuring the airway occlusion pressure or P0.1, i.e., the pressure developed in the occluded airway 100 ms after the onset of an inspiratory effort [12]. It was first described more than 40 years ago [13] and is now available on most modern ventilators. P0.1 is independent of respiratory mechanics and the patient’s reaction and is, importantly, unaffected by respiratory muscle weak-ness. Breath-to-breath variability of P0.1 is considerable
but the average of 3–4 values represents a reliable index of the patient’s drive.
Respiratory drive may also be inferred from measure-ments of inspiratory effort, despite maximal inspiratory effort being undoubtedly affected by muscle weakness. Severe muscle weakness may result in some discrep-ancy between drive and effort. Inspiratory effort can be directly measured using esophageal manometry to quantify the pressure–time product per minute (PTP) or the work of breathing (WOB) of the respiratory mus-cles [14]. It can be employed at the bedside with relative ease, but many clinicians are unfamiliar with the tech-nique. Inspiratory effort can be estimated non-invasively by diaphragm ultrasound. Diaphragm thickening during inspiration (quantified by the thickening fraction, TFdi) reflects diaphragm shortening during contractile acti-vation. TFdi is correlated with PTP [15] and electrical activity of the crural diaphragm (EAdi). Because of inter-observer and intraobserver variability, specific training is required. Additionally, respiratory drive may also affect
Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive during acute respira-tory failure. Respiratory centers in the brainstem send inputs to the respiratory muscle that generate ventilation. The main feedback signals include CO2 tension, acid/base status (pH), and oxygenation. Additional signals modify the respiratory drive either directly, by acting on other variables, or indirectly, by modifying the response of the servomechanism. Colored arrows represent the main determinants and gray lines represent more complex interactions. Some determinants arise from upper neural structures and others arise directly from the airway, chest wall, lung parenchyma, or respiratory muscles. Signals from the airways and lung parenchyma are conducted via vagal C fibers. Mechanoreceptors in muscle spindles, tendons, and joints are conducted through the spinoreticular pathway. Mechanical ventilation can influence all these mechanisms substantially. On the right, the consequences of an inappropriately high and low respiratory drive during mechanical ventilation are listed. P-SILI: patient self-inflicted lung injury; SBT: spontaneous breathing trial

In which patient should you worry?
• Tidal volume consistently > 6 -8 mL/kg IBW in relation to ventilated lung volume
• Severe lung injury
• Obvious excessive inspiratory efforts - use of accessory muscles
• Transpulmonary pressure > 20 - 22 cm H2O, PTP > 200
• P0.1 > 3 - 4 cm H2O
Low threshold for EAdi and Ppl measurement

P0.1
Marker for respiratory drive and WOB (normal 0.5 - 1.5 cm H2O)

Therapeutic measures
• Optimize patient-ventilator interaction
• Control the patient’s respiratory drive
✓Treat acidosis and hypoxemia + fever/pain
✓Provide sufficient sedation and analgesia
✓Use (partial) neuromuscular blockade
✓Extracorporeal CO2 removal
• Apply sufficient PEEP to maximize fluid-like lung behavior
Lower the level of spontaneous effort

lung (Fig. 1b). Therefore, in contrast to mechanical breaths, plateau PL (i.e., at end-inspiration) potentially underestimates maximal dependent lung stress/stretch during vigorous effort in ventilated patients with ARDS. Third, vigorous effort appears to increase injury in the dependent lung—the same region in which spontaneous effort increases inspiratory distension [4].
The key mechanism is inhomogeneous pressure trans-mission in the presence of “solid-like” injured lung (Sup-plemental Figure). Here, the negative deflection in Ppl resulting from diaphragm contraction is poorly trans-mitted to the remainder of the pleural surface, and thus “confined” to the dependent lung [3, 4, 14]. The higher distending pressure in the local lung will tend to draw gas from the non-dependent lung (this is called pendel-luft [14]), or from the trachea and ventilator, towards the dependent lung. This causes a transient overdistension [3, 4, 14] and tidal recruitment in the dependent lung
[3, 4] during early inspiration (i.e., the peak phase of PL), corresponding, in space and time, to maximal intensity of the diaphragm contraction and the peak negative value of deflection (swing) in Pes. Importantly, such injurious inflation is likely observed in the presence of vigorous effort, and “solid-like” atelectatic lung tissue due to insuf-ficient PEEP [4, 5, 15].
Clinical implicationsLimitations of VT and Paw are validated clinical approaches to lessen ventilator-induced lung injury dur-ing ventilator breaths, but effort-dependent lung injury is not preventable using such global parameters [3, 4, 14].
(ϸ) Paw (cmH2O)
(Ϲ) Flow (L/s)
(Ϻ) Pes (cmH2O)
(ϻ) PL (cmH2O)
(ϼ) Regional Lung Stretch (∆Z)Nondependent
(Ͻ) Regional Lung Stretch (∆Z)Dependent
Time (S)
Peak Plateau
40
01
-1
0
20
525
-5
2000
0
0
700
0 6
0
Time (S)
30
0 2
-2
0
18
0
20
-10
2000
0
0
2000
0 4
(ϸ) Paw (cmH2O)
(Ϲ) Flow (L/s)
(Ϻ) Pes (cmH2O)
(ϻ) PL (cmH2O)
(ϼ) Regional Lung Stretch (∆Z) Nondependent
(Ͻ) Regional Lung Stretch (∆Z) Dependent
Peak Plateau
0
(A)
(B)
Fig. 1 a Local inflation pattern during a mechanical breath: this is a representative description in a severe ARDS porcine model (i.e., repeated surfactant depletion + injurious mechanical ventilation). Two consecutive breaths are presented: the first, without interruption, and the second with an inspiratory hold. Volume-controlled ventila-tion with square flow was provided, as indicated in the tracings of Paw (i) and flow (ii). There were no negative deflections in Pes (iii). PL was calculated as [Paw − Pes] (iv), and regional lung stretch (∆Z) was deter-mined using electrical impedance tomography (EIT; PulmoVista®500, Dräger, Lübeck, Germany) with the thorax divided into two zones: non-dependent and dependent (v and vi, respectively). Maximum inflation of the non-dependent and dependent lung (v and vi) was achieved at end-inspiration (i.e., plateau phase, blue line), but not at peak phase (red line). b Local inflation pattern during a spontaneous effort: this is a representative description in a severe ARDS porcine model (i.e., repeated surfactant depletion + injurious mechanical ventilation). Two consecutive breaths are presented: the first, without interruption, and the second with an inspiratory hold. The presence of spontaneous breathing caused a negative deflection in Paw (i) and increased tracheal gas flow after triggering (ii), resulting from a negative deflection in Pes (iii). Early in inspiration, peak PL (iv) occurred, corresponding to the time when the swing in Pes from spontaneous effort reached most negative, but not corresponding to the time when Paw reached peak. This is contrast to the findings during muscle paralysis (a). Non-dependent (v) and dependent lung (vi) show local stretch, reflected by delta Z (i.e., relative change in air content). Peak PL corresponds to the duration of maximum inflation of the depend-ent lung (red dot in vi), but not the non-dependent lung (red dot in v). Moreover, the maximal stretch in the dependent lung occurred despite the presence of residual inspiratory tracheal gas flow (ii). When the Pes began to rise, corresponding to the start of diaphragm relaxation, the dependent lung began to deflate (vi) and the gas moved into non-dependent lung (v), together with residual inspira-tory flow from the ventilator. As a result, the non-dependent lung continued to inflate (v) and its stretch was maximal at end-inspiration (blue triangle in v). Paw airway pressure, Pes esophageal pressure, PL transpulmonary pressure
▸
Explain what you see!

A recent case
• Male, 30
• PMH: negative
• 22/09: admission with progressive dyspnea
• Diagnosis: metastasized nonseminoma testicular cancer

A recent case
Chest X-ray admission CT scan 03/10

Patient
• 20/10
✓PSV: 6/6, Tv 650 - 700 mL
✓RR: 20
✓P0.1: 5 cmH2O
✓Dynamic compliance 90 - 100 mL/cmH2O

PSV 6/6Flow
Pes
TPP
TDP
EDi
Pairway
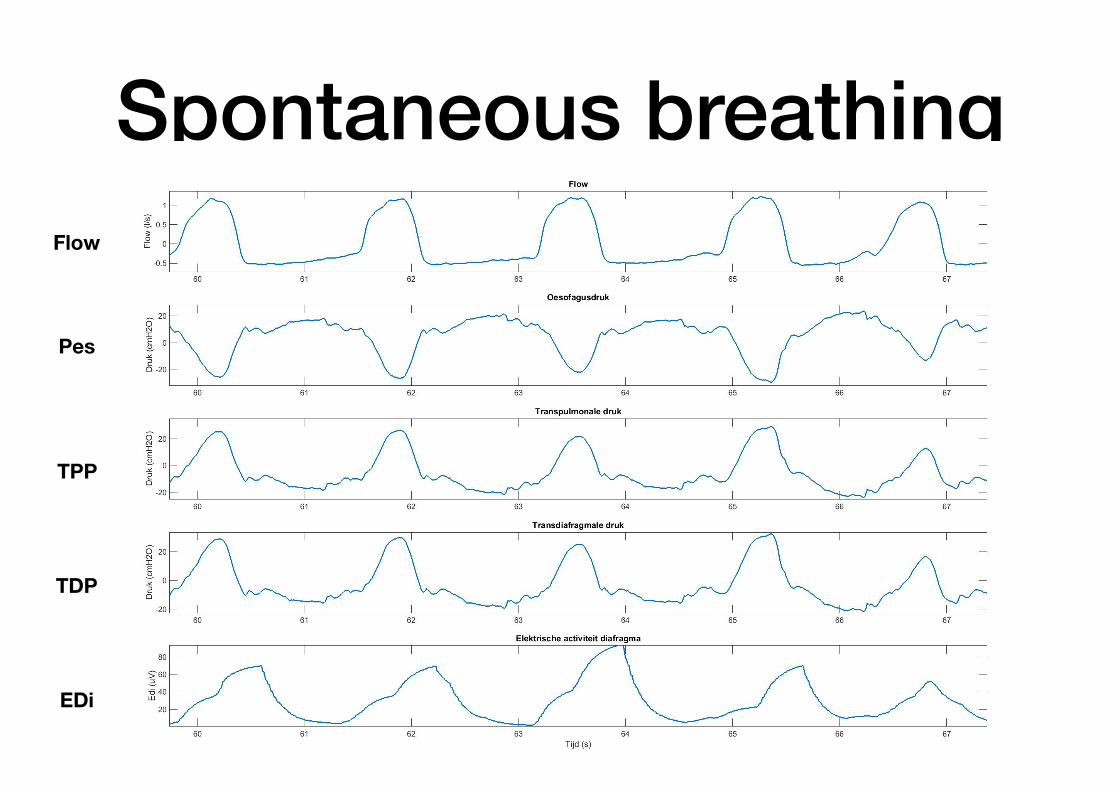
Spontaneous breathingFlow
Pes
TPP
TDP
EDi

Work of breathingPSV 6/6 Spontaneous breathing
WOB J/L (N ≈ 0.35) 3.16 3.64WOB J/min (N ≈ 2.4) 58.23 62.27

22/10
A recent case• 23/10:
• Passes SBT
• Extubation - transfer to intermediate care unit

Conclusion
• High respiratory drive in spontaneously breathing patients or on assisted ventilation may induce lung injury
• However, it is unclear exactly when P-SILI starts and has an impact on outcome
• Rethink your strategy when danger signs are present especially in inhomogeneous lungs with solid like behavior

Ventilator Induced Lung Injury
Stress / Strain
Mechanical power
Mechanical heterogeneity
Disease stage and VILI
predispositionReduced lung
capacity
Mechanical heterogeneity
Vigor spontaneous
efforts
pH and vascular
pressures

Rescue therapies
• Prone position
• NO or prostacyclin inhalation
• High frequency oscillation
• Extra corporeal life support
Oxygenation improvement with iNO is enhanced when hypoxic pulmonary vasoconstriction is preserved. Fur-thermore, iNO reduces elevated pulmonary artery pres-sure and right ventricle afterload, and reduces the risk of acute cor pulmonale, an independent factor of mortal-ity [9]. Prone position and iNO have an additive effect on oxygenation. The potential harmful effects of iNO include platelet aggregation inhibition, elevation of pul-monary artery occlusion pressure, and risk of acute kid-ney injury. Randomized trials showed improvement in oxygenation but failed to demonstrate improvement in patient mortality [10]. Therefore, systematic use of iNO is not recommended in ARDS. Of note, lung protective ventilation was not used in these trials. It is unknown if their results would have been different if lower tidal vol-umes had been used. Inhaled NO can be used in refrac-tory hypoxemia on a case-by-case basis. Reassessment of the response should be done after 1–2 days to allow for dose reduction,with the dose being tapered over a few hours to minimize the risk of rebound hypoxemia and increased pulmonary artery pressures. During iNO
exposure vasoconstrictive molecules like endothelins are increasingly produced to balance the vasodilator effect of iNO, and, after the sudden iNO interruption, they become predominant potentially leading to a deleterious rebound effect.
High-frequency oscillation (HFO) is a non-conven-tional ventilatory support where rapid and small cyclical swings in pressure are around a relatively constant mean airway pressure. The potential benefits stem from the delivery of very small tidal volumes at higher mean air-way pressures—functionally equivalent to PEEP—while still avoiding cyclic alveolar overdistention. The side effects include the need of a specific device, the uncer-tainty about the real applied intrathoracic pressure due to the resistive pressure drop, and the risk of hemody-namic compromise. Initial clinical trials in ARDS were promising. Enthusiasm for adult HFO has, however, waned significantly since the publication of two large trials in a broader population of moderate-severe ARDS patients, which showed no effect on mortality, and even increased mortality in HFO patients [11]. These trials
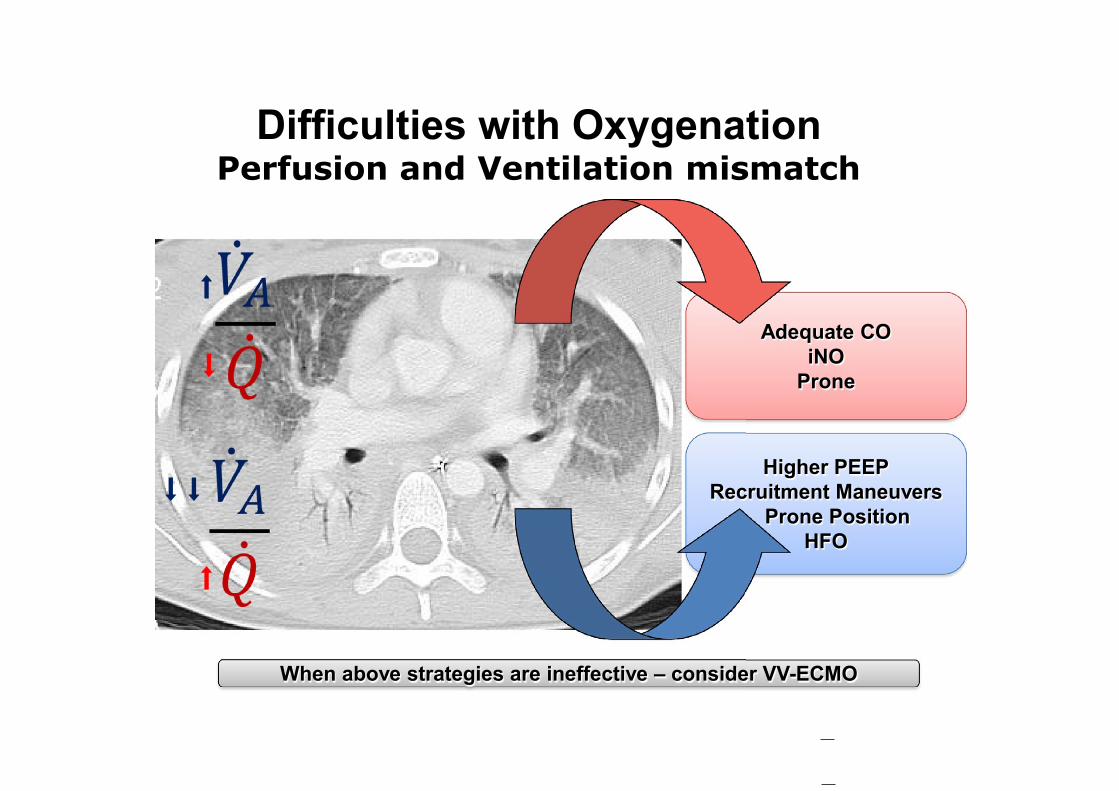
Higher PEEPRecruitment Maneuvers
Prone PositionHFO
Adequate COiNO
Prone
Difficulties with Oxygenation
When above strategies are ineffective – consider VV-ECMO
⬇
⬇
⬇
⬇
⬇
Fig. 1 Mechanisms of action of adjunct therapies during severe ARDS on ventilation/perfusion !
V̇A
Q̇
"
distribution. Due to massive loss of aeration and increase in lung tissue as shown on the lung CT slice, hypoxemia results from large amounts of shunt and V̇A
Q̇ mismatch, which may be due to
low alveolar ventilation !
V̇A"
as compared to lung perfusion !
Q̇"
or to more lung perfusion relative to V̇A. This latter occurs when hypoxic pulmonary vasoconstriction is impaired making the lung perfusion predominant in non-aerated lung regions. To improve V̇A
Q̇ matching and hence oxygenation,
interventions may act on both sides of the equation. By increasing perfusion in well ventilated regions, inhaled nitric oxide (iNO) and intravenous fluid challenges redistribute lung perfusion and cardiac output (CO) to well-aerated areas and better match V̇A
Q̇. PEEP can increase aeration in non- or
poorly ventilated areas thereby improving V̇AQ̇
. CO may decrease with PEEP, which also contributes to V̇AQ̇
improvement. High frequency oscillation and recruitment maneuvers improve V̇A
Q̇ by increasing V̇A. Prone position increases V̇A in the vertebral lung regions where Q̇ remains prevalent and,
furthermore, makes the distribution of V̇AQ̇
homogeneous across the lung

Beneficial effects of prone position
Supi
ne h
ighe
r—Pr
one
high
er
0
1
2
Day 1 Day 2 Day 3
P/F increase 27 - 39%
Meta-analysis N = 929
Sus S. Intensive Care Med 2010;36:585-599
In total 70 - 80% of patients responded
Patie
nts
(%)
0
10
20
30
P/F response (mmHg)< -40 -40 - 0 0 - 40 40 - 80 80 - 120 120 - 160 160 - 200 200 - 240 > 240
33
7
1114
22
26
10
3
N = 209
Gattinoni L. Crit care Med 2003;31:2727-2733

Mechanical effects of proning
Med
ian
0
10
20
30
40
Ecw (cmH20/l) El (cmH2O/l) Pplat (cmH2O) Rl (cmH2O/L/s)
15
25
32
1114
24
32
10
Supine Prone
P < 0.05 NS P < 0.05 P < 0.05
Riad Z. Am J Respir Crit Care Med 2018

Prone position in patients with ARDS
• All evidence points to the fact that in the prone position blood flow is greatest in the dorsal (non-dependent) parts demonstrating the importance of the arterial tree
• Total ventilation may increase by a more homogenous pleural pressure and by elimi-nating the weight of the heart and liver
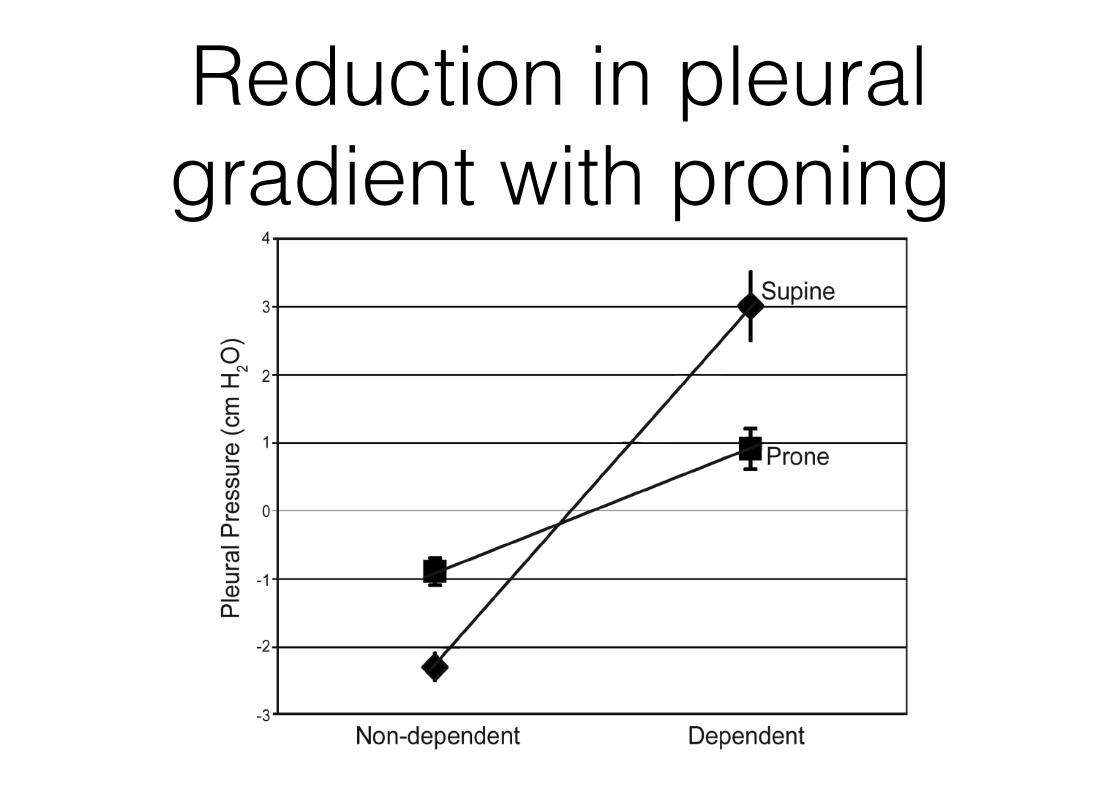
Reduction in pleural gradient with proning

The position of the heart
Prone position in severe ARDS
• MC (27) RCT
• Severe ARDS and MV < 36 hrs with PF < 150 mmHg, FiO2 ≥ 0.6 and PEEP ≥ 5
• Tv 6 mL/kg PBW
• After inclusion stabilization period of 12 - 24 hrs
Guérin C. N Engl J Med 2013

Prone position in severe ARDS
• Prone for at least 16 consecutive hrs
• PEEP and FiO2 from table: Pplat < 30 and pH 7.20 - 7.45
• Clear criteria for stopping prone position (P/F ≥ 150 + PEEP ≤ 10 + FiO2 ≤ 0.6 in supine position
• Strategy followed for up to 28 days
• Proning as rescue in the supine group strictly controlled
Guérin C. N Engl J Med 2013
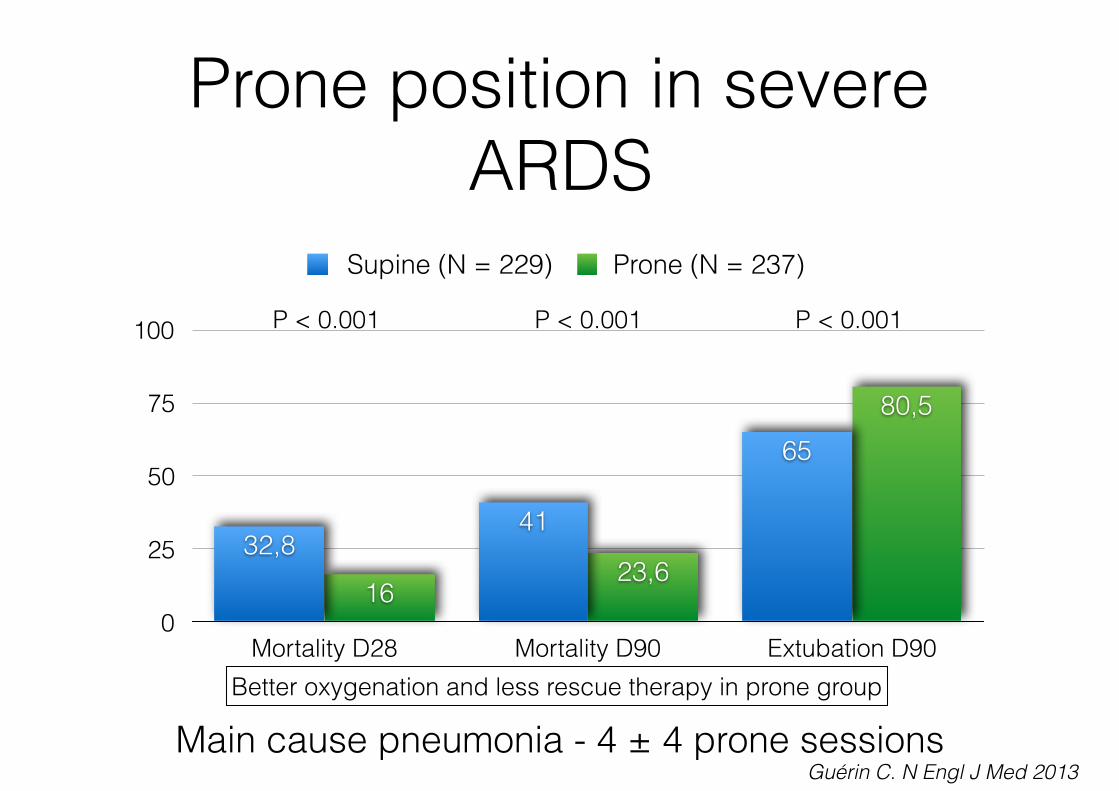
Prone position in severe ARDS
0
25
50
75
100
Mortality D28 Mortality D90 Extubation D90
80,5
23,616
65
4132,8
Supine (N = 229) Prone (N = 237)
Main cause pneumonia - 4 ± 4 prone sessions
P < 0.001 P < 0.001 P < 0.001
Better oxygenation and less rescue therapy in prone group
Guérin C. N Engl J Med 2013

Prone position - meta-analysis
Sus S. CMAJ 2014;186:E381

Prone position - meta-analysis
Beitler JR. Intensive Care Med 2014;40:332-341
Homogenous distribution of lung stress along the vertical gradient

DISCUSSION
In patients with ARDS ventilated with protective ventilation andmaximal alveolar recruitment, we observed that PP reduced RVafterload and increased cardiac preload. PP increased cardiac in-dex in half of the patients. Significant preload reserve was docu-mented in this group of patients. In the remaining patients,cardiac index did not change with PP and no preload reservewas documented.
Some studies have found that PP had no or minimal hemody-namic effect (23–31) but they have been conducted under different
ventilator settings (23, 24, 26, 29–31) and investigated hemodynam-ics a long time after proning (23, 31). Other studies have shownthat PP increased cardiac output (32, 33) but the responsible mech-anisms were not fully investigated, in particular because RV after-load was not assessed. Finally, in patients with acute corepulmonale, Vieillard-Baron and coworkers (8) have shown thatPP improved RV function and increased cardiac output. Theirstudy was not conducted with protective ventilation and maxi-mal alveolar recruitment (8). Moreover, it described hemody-namic effects 18 hours after PP. Thus, the acute hemodynamiceffects induced by PP remained to be documented.
Figure 2. Changes in hemodynamic var-iables before and during prone position-ing in patients with nonsignificant andsignificant changes in cardiac index in-duced by prone positioning. In box andwhiskers, the median line corresponds tomedian, the lower and upper limits of thebox to the extremities of the interquartilerange, and the error bars to the extrem-ities of the 5th–95th percentiles. Thegray lines correspond to individual data.n ¼ 18. *P less than 0.05 versus beforeprone positioning.
Jozwiak, Teboul, Anguel, et al.: Hemodynamic Effects of Prone Positioning 1431
expiratory pressure (PEEP) level was titrated to obtain a plateau pres-sure of 28–30 cm H2O (16, 17). Respiratory rate was adjusted to pre-vent hypercapnia and to avoid dynamic intrinsic PEEP. Intrinsic PEEPwas calculated as the difference between the total PEEP measuredduring an end-expiratory occlusion and the external PEEP. The frac-tion of inspired oxygen was adjusted to obtain an oxygen saturationgreater than or equal to 90%. The compliance of the respiratory systemwas calculated as tidal volume / (plateau pressure – total PEEP). Inpatients receiving nitric oxide, the dose was kept constant during theentire study time. Nitric oxide was not added in any other patient.
Hemodynamic Measurements
Patients were monitored by a pulmonary artery catheter (Edwards Life-Sciences, Irvine, CA) and a PiCCO2 device (Pulsion Medical Systems,Munich, Germany). The pressure transducers were pasted on thepatient’s thorax at the midaxillary line and were kept in this position.The pulmonary vascular resistance (PVR) was calculated as (meanpulmonary artery pressure – pulmonary artery occlusion pressure)/cardiac index. The ratio of venoarterial carbon dioxide gradient overthe arteriovenous oxygen content difference was calculated to estimateanaerobic metabolism (18, 19). The product of the LV end-systolic areatimes the arterial systolic pressure was calculated and used to estimatethe LV afterload.
Echocardiographic Measurements
With transesophageal echocardiography (Envisor Philips B0; PhilipsHealthcare, Andover, CA) we assessed the anteroposterior and septo-lateral diameters of the left ventricle, the LV eccentricity index, theLV ejection fraction, and the presence of a paradoxical motion ofthe interventricular septum in the short-axis cross-sectional view andthe end-diastolic area of the right and left ventricles in a long-axisfour-chamber view.
IAP Measurements
IAPwas estimated from the bladder pressure by injecting 25ml of salinein the bladder after clamping the urinary drainage bag (AA6118 Folysil;Coloplast, Humlebaek, Denmark) (20). The abdominal pressure
transducer was fixed to the patient on the lateral side of the pelvis, 2cm below the anterior superior iliac spine.
Hemodynamic, respiratory, and the IAP signals were continuouslycomputerized (HEM4.2; Notocord Systems, Croissy-sur-Seine, France).All measurements were performed at end-expiration.
Study Design
All patients were lying on an air-cushioned bed. Initially, a first set ofmeasurements including hemodynamic, echocardiographic, respiratory,and IAP variables was performed. Then, to assess the preload reserve,a passive leg raising (PLR) test was performed (21, 22). Hemodynamicand IAP measurements were recorded when the maximal effect ofPLR on cardiac index was reached (21).
Just before PP, a second set of measurements was performed. PPwas performed without any thoracic or pelvic support. In the proneposition, one arm was placed over the head and the other was parallelto the rest of the body. Thereafter, PP started. After PP, we measuredthe plateau pressure and external PEEP was adjusted to obtain a pla-teau pressure of 28–30 cm H2O, as in supine position. The abdominaland blood pressure transducers were zeroed versus the atmosphericpressure. After stabilization of all variables (i.e., within 20 min),a third set of measurements was performed. Excepting PEEP, venti-lator settings and other treatment were unchanged during the studyperiod.
Statistical Analysis
Variables were summarized as median and interquartile range. Vari-ables before and during PLR and before and after PP were comparedby a Wilcoxon test. The presence of preload reserve was defined bya PLR-increase in cardiac index greater than or equal to 10% (21).Patients in whom PP increased cardiac index greater than or equal to15% were compared with the other ones by a Mann-Whitney U testor by a Fisher exact test as appropriate. P less than 0.05 was consid-ered statistically significant. Statistical analysis was performed byusing MedCalc 11.6.0 software (MedCalc Software, Mariakerke,Belgium).
RESULTS
Study Population
Eighteen patients were included in the study. Their characteris-tics are summarized in Table 1. Sixteen percent of patientsreceived inhaled nitric oxide.
Changes in Respiratory Data
PP showed a trend toward increased compliance of the respira-tory system (Table 2). The ratio of the partial pressure of arte-rial oxygen over the fraction of inspired oxygen significantlyincreased. The arterial carbon dioxide partial pressure showeda trend toward decrease during PP (Table 2).
Figure 1. Theoretical hemodynamic effects of prone positioning. Theresultant effect of these mechanisms on cardiac output depends ontheir respective weight. LV ¼ left ventricular; RV ¼ right ventricular.
TABLE 1. PATIENTS’ CHARACTERISTICS AT BASELINE
Sex, F/M 8/10Age, yr 72 (48–76)Cause of ARDS (pulmonary/extrapulmonary) 14/4Septic shock 15SAPS II 46 (41–57)PaO2
/FIO2, mm Hg 134 (113–154)
PaO2, mm Hg 83 (77–91)
PaCO2, mm Hg 34 (30–40)
Lactate, mmol/L 1.8 (1.4–2.5)Patients receiving norepinephrine 15Dose of norepinephrine, mg/kg/min 0.53 (0.13–0.72)
Definition of abbreviations: ARDS ¼ acute respiratory distress syndrome; SAPS ¼simplified acute physiology score.N ¼ 18; data are expressed as median (interquartile range) or number.
Jozwiak, Teboul, Anguel, et al.: Hemodynamic Effects of Prone Positioning 1429
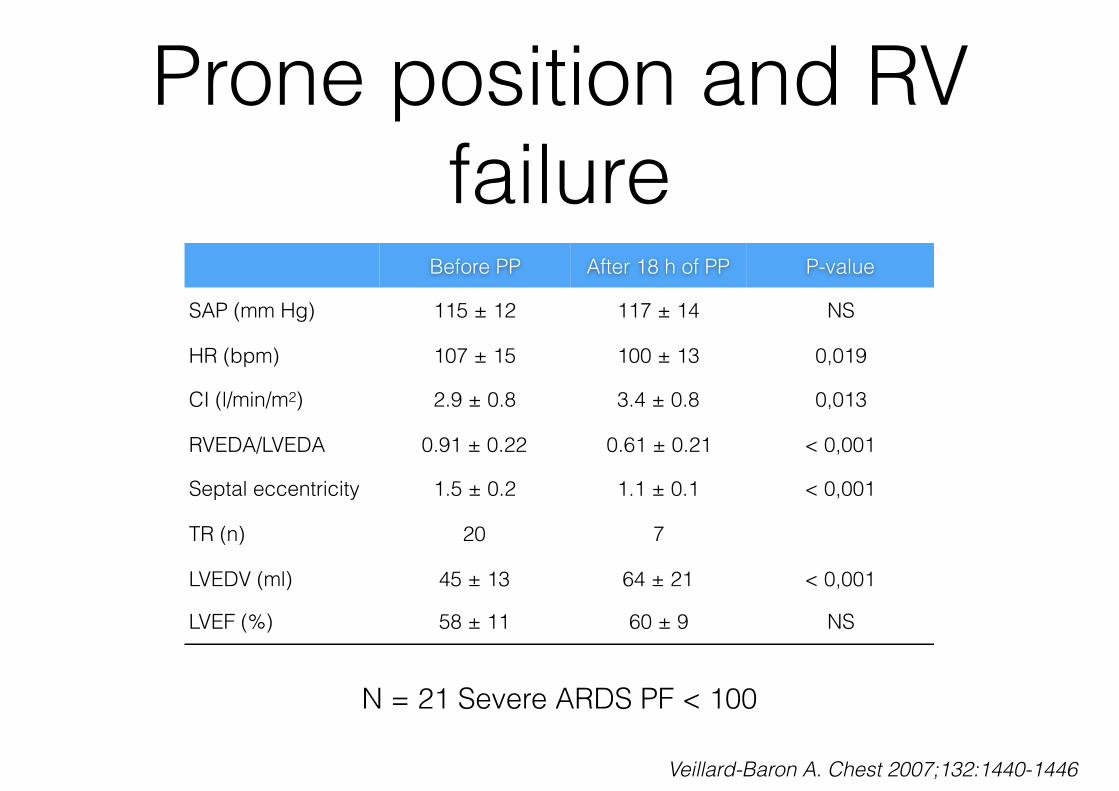
Prone position and RV failure
Before PP After 18 h of PP P-value
SAP (mm Hg) 115 ± 12 117 ± 14 NS
HR (bpm) 107 ± 15 100 ± 13 0,019
CI (l/min/m2) 2.9 ± 0.8 3.4 ± 0.8 0,013
RVEDA/LVEDA 0.91 ± 0.22 0.61 ± 0.21 < 0,001
Septal eccentricity 1.5 ± 0.2 1.1 ± 0.1 < 0,001
TR (n) 20 7
LVEDV (ml) 45 ± 13 64 ± 21 < 0,001
LVEF (%) 58 ± 11 60 ± 9 NS
N = 21 Severe ARDS PF < 100
Veillard-Baron A. Chest 2007;132:1440-1446

Adverse effects?
• Pressure ulcers (RR 1.29 [1.16,1.44])
• ET obstruction (RR 1.58 [1.24,2.01])
• Thoracostomy tube dislodgement (RR 3.14 [1.02,9.69])
Sus S. Intensive Care Med 2010;36:585-599

Prone position and ICP
0
5
10
15
20
25
30
Supine Prone 10
min
Prone 1 h Prone 3 h Supine 10
min
Supine 1 h
kPa
PaO2 PaCO2
N = 11
Thelandersson A. Acta Anaesthesiol Scand 2006;50:937-941

Prone position and ICP
0
10
20
30
40
50
60
70
80
90
100
Supine Prone 10
min
Prone 1 h Prone 3 h Supine 10
min
Supine 1 h
mm Hg
ICP CPP
Thelandersson A. Acta Anaesthesiol Scand 2006;50:937-941
N = 11

















