December 2009 >> $5 Mark A. Pippenger, MD PAGE 3 PHYSICIAN SPOTLIGHT PRSRT STD U.S. POSTAGE PAID FRANKLIN, TN PERMIT NO.357 ONLINE: ARKANSAS MEDICALNEWS. COM PRINTED ON RECYCLED PAPER November/December 2014 >> $5 FOCUS TOPICS IMAGING HEALTH EDUCATION MENTAL HEALTH NORTHWEST ARKANSAS New Biomedical Engineering Program Attracts 400 Students U of A opens $4.3-million wing for Biomedical Engineering Department (CONTINUED ON PAGE 6) BY BECKY GILLETTE FAYETTEVILLE--The University of Arkan- sas (U of A) Department of Biomedical Engineering launched in 2012 offering undergraduate and PhD degrees has already attracted 200 students in the cut- ting edge program designed to allow graduates to enter medical school, and also a wide range of other jobs in demand in the field. “The quick ramp up in the numbers of students is indicative of an acute pent up demand for the pro- gram in the state,” said Ashok Saxena, PhD, head of the Department of Biomedical Engineering. “These degree programs are the only ones of their kind in Arkansas and until now, students who wanted a de- gree in biomedical engineering were forced to leave the state. Further, there is a growing healthcare in- dustry in the state that will benefit from these new programs.” A small biomedical engineering program was embedded in the Biological and Agricultural Engi- neering Department in the College of Engineering, (CONTINUED ON PAGE 8) BY BECKY GILLETTE Starting at age 14, Ryan Gehrig, joined in a family tradition by leaving his home in Muenster, Texas, to attend Subiaco Academy, a Catholic College Preparatory boarding school. “My father and older brother went to Subi- aco, and it was great experience moving away from home at an early age and building a foun- dation in Benedictine principles of humility, ser- vice and hospitality,” Gehrig said. “I may have not have realized it at the time, but God certainly played a key role in my choice of careers. A higher power helped guide me.” His faith-based foundation has served him well in both his current role at Mercy Hospital Fort Smith and his previous healthcare manage- HealthcareLeader Ryan Gehrig President of Mercy Hospital Fort Smith To promote your business or practice in this high profile spot, contact Pamela Harris at Arkansas Medical News. [email protected]• 5012479189 Kartik Balachandran, shown here with one of his students, studies the way mechanical forces affect cells and organs. Using photolithography and nanoengineering techniques, Balachandran creates materials that mimic the properties of human tissues and tests the response of this material to different stresses and forces. Using these methods, he can examine the effects of everything from war injuries to high blood pressure. ON ROUNDS SHARE Makes It Possible for Different EHRs to Swap Information Moving electronic health data between points-of- care helps coordinate patient care Ray Scott, Arkansas Health Information Technology Coordinator, uses himself as the prime example of how the State Health Alliance for Records Exchange (SHARE) can help improve the quality of healthcare ... 4 Powerful Tesla MRI to Study Brain Coding Intention of research is to improve treatment for addictions and mental illness LITTLE ROCK – How does the brain code the progressive development of addictions? Why are some people more disposed to life-long drug use disorders?... 5
Transcript
a r k a n s a s m e d i c a l n e w s . c o m NOVEMBER/DECEMBER 2014 > 1
December 2009 >> $5
Mark A. Pippenger, MD
PAGE 3
PHYSICIAN SPOTLIGHT
PRSRT STDU.S.POSTAGE
PAIDFRANKLIN, TN
PERMIT NO.357
ONLINE:ARKANSASMEDICALNEWS.COM
PRINTED ON RECYCLED PAPER
November/December 2014 >> $5
FOCUS TOPICS IMAGING HEALTH EDUCATION MENTAL HEALTH NORTHWEST ARKANSAS
New Biomedical Engineering Program Attracts 400 Students U of A opens $4.3-million wing for Biomedical Engineering Department
(CONTINUED ON PAGE 6)
By BECKy GILLETTE
FAYETTEVILLE--The University of Arkan-sas (U of A) Department of Biomedical Engineering launched in 2012 offering undergraduate and PhD degrees has already attracted 200 students in the cut-ting edge program designed to allow graduates to enter medical school, and also a wide range of other jobs in demand in the field.
“The quick ramp up in the numbers of students is indicative of an acute pent up demand for the pro-gram in the state,” said Ashok Saxena, PhD, head of the Department of Biomedical Engineering. “These degree programs are the only ones of their kind in Arkansas and until now, students who wanted a de-gree in biomedical engineering were forced to leave the state. Further, there is a growing healthcare in-dustry in the state that will benefit from these new programs.”
A small biomedical engineering program was embedded in the Biological and Agricultural Engi-neering Department in the College of Engineering,
(CONTINUED ON PAGE 8)
By BECKy GILLETTE
Starting at age 14, Ryan Gehrig, joined in a family tradition by leaving his home in Muenster, Texas, to attend Subiaco Academy, a Catholic College Preparatory boarding school.
“My father and older brother went to Subi-aco, and it was great experience moving away from home at an early age and building a foun-
dation in Benedictine principles of humility, ser-vice and hospitality,” Gehrig said. “I may have not have realized it at the time, but God certainly played a key role in my choice of careers. A higher power helped guide me.”
His faith-based foundation has served him well in both his current role at Mercy Hospital Fort Smith and his previous healthcare manage-
HealthcareLeader
Ryan Gehrig President of Mercy Hospital Fort Smith
To promote your business or practice in this high profi le spot, contact Pamela Harris at Arkansas Medical News.
Kartik Balachandran, shown here with one of his students, studies the way mechanical forces affect cells and organs. Using photolithography and nanoengineering techniques, Balachandran creates materials that mimic the properties of human tissues and tests the response of this material to different stresses and forces. Using these methods, he can examine the effects of everything from war injuries to high blood pressure.
ON ROUNDS
SHARE Makes It Possible for Different EHRs to Swap InformationMoving electronic health data between points-of-care helps coordinate patient care
Ray Scott, Arkansas Health Information Technology Coordinator, uses himself as the prime example of how the State Health Alliance for Records Exchange (SHARE) can help improve the quality of healthcare ... 4
Powerful Tesla MRI to Study Brain CodingIntention of research is to improve treatment for addictions and mental illness LITTLE ROCK – How does the brain code the progressive development of addictions? Why are some people more disposed to life-long drug use disorders?... 5
2 > NOVEMBER/DECEMBER 2014 a r k a n s a s m e d i c a l n e w s . c o m
Since we’re singularly focused on medical malpractice protection, your mind is free to go other places. LAMMICO is not just insurance. We’re a network of insurance and legal professionals experienced in medical liability claims. A network that closes approximately 90 percent of all cases without indemnity payment. A network of robust in-person and online Risk Management educational resources to help you avoid a claim in the first place. LAMMICO’s a partner - so that when you insure with us, you’re free to do your job betteyou’re free to do your job better. And that’s a very peaceful place to be.
Free your mind to think aboutsomething other than med-mal.
a r k a n s a s m e d i c a l n e w s . c o m NOVEMBER/DECEMBER 2014 > 3
Mark A. Pippenger, MDAssociate clinical professor of neurology, UAMS
PhysicianSpotlight
By BECKy GILLETTE
Mark A. Pippenger, MD, a behav-ioral neurologist has 20 years of experi-ence in treating patients with Alzheimer’s Disease (AD) and other forms of dementia. What he would most like to communicate to healthcare providers in the state is that there are a lot of ways to help their behav-iors without using drugs.
“There are all kinds of reasons that doctors think a prescription drug will help with the behavior of someone with de-mentia,” Pippenger said, who sees patients at the Walker Memory Clinic in the Uni-versity of Arkansas for Medical Sciences (UAMS) Center on Aging. “They might have started a patient on a drug and their behavior got better. But most likely it was not a result of the medicine. There are no real medicines that are effective for man-aging dementia.”
Pippenger has a mission to educate caregivers and doctors about the best ways to take care of people with AD and related diseases. The non-profi t group Alzheim-er’s Arkansas is a good resource for family caregiver support programs.
“That is the most important thing, supporting the caregiver,” Pippenger said. “We can do more good by educating caregivers than with any type of pill. For example, rather than try to explain things to them, correct them and tell them they are wrong, you have to be able to change the subject to something more interesting. It is something that is not very intuitive to learn to leave it alone when a person with dementia is saying things that aren’t so.”
The strategy can be similar to what some parents use with a toddler. Instead of
trying to argue or persuade, distract them with something else more positive.
One possible distraction is music.“Music is generally very useful in
managing people with AD,” Pippenger said. “Musical memory preserved beyond other forms of memory. People might re-member songs better than anything else. A lot of work being done is fi nding a major benefi t for regularly playing music for peo-ple with AD, especially if they can partici-pate by singing or playing an instrument.”
While working with dementia pa-tients is challenging, Pippenger said it is rewarding at the same time because a lot of times they can make a big difference.
Pippenger grew up in Jonesboro, and got his undergraduate degree in zoology where he developed a special interest in
dragonfl ies. While attending UAMS med-ical school, he became very intrigued with behavioral and cognitive neurology, and was able to interact with some of the big names in the fi eld including Jeffrey Cum-mings, MD, at UCLA – where Pippenger completed a fellowship in behavioral neu-rology and dementia
“Seeing them and how they evalu-ated patients was an inspiration,” Pip-penger said. “It was elegant the way they could do an evaluation and localize dis-ease processes to certain parts of the brain just by their exam, not a lab test. It was almost like a detective case, much more than other fi elds of medicine. We can tell where the pathology is even without neu-roimaging.”
Recent studies have indicated that AD may be the third leading cause of death in the U.S. Although the failure to fi nd a cure is leaving millions of people with suffering that can last from three to ten years, Pip-penger said there has been great progress made understanding the disease.
“We know a lot more than we used to know,” he said. “When I was starting out 20 years ago, we only knew about this vague protein amyloid in the brain. We still don’t know why people have it, but we are getting to that. There have also been im-provements in treatment. We have intro-duced the fi rst drugs that have been found to be actually effective in slowing down the symptoms of AD. They aren’t terribly ef-fective, but they have some benefi ts. There has also been progress in fi nding which drugs for behavior are not effective.”
One positive factor is that the in-cidence of new cases has slowed down in recent years. There are more people
with AD because of the nation’s aging population. But the incidence has slightly decreased – which Pippenger hopes is related to people taking prevention mea-sures such as exercising more, and eating healthier diets.
“Some of that may be starting to work,” he said. “It is at least hopeful that those measures might be having some ef-fect. My advice for doctors is to tell pa-tients that keeping mentally active is also helpful, but probably not as important as physical exercise. Better to get on an exer-cise bike than sit doing crossword puzzles and word games.”
Observational studies clearly show people with more curcumin– an ingredi-ent in the spice curry – have lower rates of AD.
“Why not use more turmeric?” he asks. “Get it in your food. Besides which, the food is pretty darn tasty.”
As for keeping his brain active, Pip-penger has a big interest in Irish tradi-tional music. He is a founding member of the Arkansas Celtic Music Society, and plays the traditional drum called a bodhran. He has helped bring Irish bands in for concerts in Little Rock, and is work-ing to learn Irish – which is a challenge because there aren’t a lot of people who speak Irish these days.
Pippenger also retains his special in-terest in dragonfl ies that he developed as an undergrad studying entomology.
“There are a lot more species than you might think,” he said. “There are more than 200 species of dragonfl ies and damselfl ies in Arkansas. I’m not collecting anymore, but I like to keep up with the research.”
For more information Contact Walter Rognrud
501-960-0658
Let us make your next exclusive event unforgettable at Little Rock’s only
Castle…
castleonstagecoach.com
HOLIDAY PARTIES
EVENTS
BOARD MEETINGS
INDOOR AND OUTDOOR OPTIONS
Subscribe to
Online Medical
News Free!Get the current
edition of Arkansas Medical News
delivered to your desktop. FREE!
arkansasmedicalnews.com
EMAIL NOTIFICATIONS
4 > NOVEMBER/DECEMBER 2014 a r k a n s a s m e d i c a l n e w s . c o m
Outpatient Mental Health Counseling Services• Individual, Couple & Family Counseling• Mental Health Paraprofessional Intervention• Psychiatric Evaluations• Psychological Evaluations• Medication Management• School-based Mental Health• In-home Services• Play Therapy
877.595.8869 • familiesinc.netCall today to �nd out more about if you or a loved one could bene�t from counseling.
Total Wellness Includes Mental HealthFor more than a decade, children, adolescents and adults
across Northeast, North Central and Central Arkansas have improved their lives with our therapeutic services.
LIFE is meant to be ENJOYED!
headline
By BECKy GILLETTE
Ray Scott, Arkansas Health Informa-tion Technology Coordinator, uses him-self as the prime example of how the State Health Alliance for Records Exchange (SHARE) can help improve the quality of healthcare in the state with a Health Information Exchange that allows differ-ent healthcare providers in the state to ex-change patient Electronic Health Records (EHR).
Scott gives the example of his per-sonal experience. He sees a cardiologist at St. Vincent Health System, an endocrinol-ogist at University of Arkansas for Medi-cal Sciences, and an ophthalmologist at Baptist. In most cases when someone has multiple providers likely to have different EHR systems, few providers at each place are exchanging information about each visit.
“SHARE is building a mechanism where an individual’s health information can be accessible to their providers at those various points of care,” Scott said.
“Few people get their entire healthcare from one organization or facility. The process of moving records from one point of care to the next is greatly enhanced if they are connected to and using SHARE.”
SHARE, basically, helps different
EHR systems at each healthcare provider or facility to communicate so that there can be an information exchange that is helpful to patients getting the best health-care, and to the healthcare system in re-ducing costs by preventing duplication of testing and facilitating a team approach to healthcare.
In the past and still too often today, much of the information sharing has been by fax machine. Scott says that is far less efficient than being able to read health in-formation electronically in real time at the point of care.
SHARE is not a data warehouse.“It is not about aggregating and stor-
ing huge amounts of data, but having the mechanism to move that information where it is needed when appropriate for HIPAA-permitted purposes,” Scott said. “The value of SHARE is not in having the data, but literally in sharing the data between different points of care. The tech-nology we are deploying has to be able to interface with any certified EHR. We must be brand agnostic.”
One of the challenges is that while there are national certification require-ments for EHR products, how those com-panies meet those standards may vary widely. The bad joke in the industry is there are standards that are not standard. It would be like having an AT&T cell phone that would work only with other AT&T cell phones.
“Unfortunately, EHR communica-tion between different vendors is simply not possible in the current environment without a lot of human intervention,” Scott said. “That is why the HIE is a ne-cessity if physicians are going to exchange common patient data, especially if they are using different EHR systems. Connecting to SHARE can be the mechanism where information flows from your system to an unaffiliated system using a different prod-
uct. Our goal is to build interfaces with all Arkansas hospitals and practices. Every time we connect to another provider or facility, the value of SHARE increases for all providers and facilities.”
Scott said records from other health-care providers and hospital systems must be shared in a form that is meaningful to the end user. It must be in an appropri-ate format that is easy to read and search through, or it will be of limited value to providers.
Following the adoption of the HI-TECH (Health Information Technology for Economic and Clinical Health) Act in 2009, the federal government provided millions of dollars in incentives for physi-cians, clinics and hospitals to adopt EHR systems. The next phase is to move to producing proof that the electronic health information is being used to better coor-dinate care, eliminate duplicate tests, and avoid unnecessary costs.
SHARE hears from providers con-cerned about the cost of EHRs, and the fact that some of their systems don’t live up to what was promised.
“We have folks who have had great experiences transferring to an EHR, and others who have had difficult experiences with that,” Scott said.
There are at least 600 nationally cer-tified EHR products, with at least 50 to 75 being used in Arkansas.
“There are challenges on our side with the time, effort and cost it takes to build interfaces with all these products,” Scott said.
For clinics joining SHARE, the fee is between $50 and $75 depending on the number of primary clinical users access-ing the system. EHR vendors also charge practices and facilities for interfacing their software with SHARE
“Companies that are willing have en-tered into statewide licensing agreements that have brought the price to providers and facilities down for some products,” Scott said. “For example, we have one company with 108 practices in the state using their product, and as a result of our negotiated agreement, their price dropped by an average of $10,000 per practice per year.”
There are several persuasive reasons for clinics and hospitals not waiting to join SHARE, Scott said. Medicare and Medicaid have EHR incentive programs because the government wants to make
SHARE Makes It Possible for Different EHRs to Swap InformationMoving electronic health data between points-of-care helps coordinate patient care
From left, Deborah Lombas, Arkansas Health Information Technology Coordinator Ray Scott, and Latriana Robertson, COO of the Office of Health Information Technology discuss SHARE’s strategic growth.
(CONTINUED ON PAGE 9)
a r k a n s a s m e d i c a l n e w s . c o m NOVEMBER/DECEMBER 2014 > 5
By BECKy GILLETTE
LITTLE ROCK – How does the brain code the progressive development of addictions? Why are some people more disposed to life-long drug use disorders? A common risk factor for drug use, depression, anxiety disorders and other mental illnesses is experienc-ing assault or trauma. As a clue to their association, how does the ad-olescent brain respond to trauma?
Those are some of the big questions being explored at the University of Arkansas for Medi-cal Sciences (UAMS) Helen L. Porter and James T. Dyke Brain Imaging Research Center (BIRC), which is doing research aimed at not just better under-standing brain-behavior coding, but using that knowledge to develop more effective treatments for addictions and other forms of mental illness.
“I like both the complexity and excite-ment of using brain imaging,” said Clint Kilts, PhD, director of the BIRC. “The pri-mary goal is to understand the relationship between the brain and human behavior. How do different experiences reorganize the brain to facilitate adaptive or mal-adaptive outcomes? Every time the brain is stimulated by something like learning a second language or how to juggle, the brain is remolded in an active, ongoing process.” Unfortunately the relationship is also true for adverse experiences such as trauma ex-posures.
One major tool for exploring such re-lationships is a $3-million, 6,000-pound 3 Tesla MRI scanner that is able to produce a magnetic field 60,000 times stronger than the Earth’s.
Kilts said the 3 Tesla scanner is an im-portant tool in their work studying the func-tional organization of the human brain.
“One current $1.4 million grant from the National Institute on Drug Abuse (NIDA) is looking at how risk factors change the brain to increase susceptibility for drug addiction, specifically at how earlier life trauma predisposes women to addiction,” Kilts said. “We have spent a lot of time studying the brain to understand the causes of the chronically relapsing nature of addic-tion. Relapse is so common. There is grow-ing understanding of how the brain codes relapse. Circuits of the brain are activated when the brain experiences stress or another stimulus for relapse such as encountering a reminder of past drug use, or if the subject uses a drug of abuse. New approaches to treatment and prevention demand an un-
derstanding of how the brain biologically codes relapse.”
The purpose of the NIDA research is to develop prevention and invention strategies for at-risk adolescents.
“There is a high bar set on work like this being translational,” Kilts said. “It is not enough to do the science, but it should deliver outcomes that obviously lead to the betterment of the patient.”
A risk factor that predisposes girls aged 12 to 16 to drug abuse is physical or sexual assault.
“Until recently, we had no idea of how the brain responds to trauma and how that effect leads to greater risk for a drug use dis-order,” Kilts said. “And we have been fasci-nated with why certain individuals develop psychiatric disorders, not just addiction. We know a common risk factor for drug use, de-pression, anxiety disorder and other mental illnesses is experiencing assault or trauma. Trauma is so prevalent in our society and worldwide. It is such a dominant risk factor, more important than genetic risk factors, for example. We are very much involved in working to learn more about the brain consequences of the enormous risk factor of trauma and how that affects post traumatic stress disorder (PTSD), depression and drug use.”
To be translational, the research must inform the design of better modes of treat-ment.
The same types of treatment for mental health have been used for decades, but they don’t work in everyone and some people have only partial responses.
“We have been slow to develop better ones, largely because our understanding of what brain changes code the best individual treatment outcomes remains limited,” Kilts said. “We need to develop better therapies predicated on understanding how the pres-ent therapies work. A related challenge is
Powerful Tesla MRI to Study Brain CodingIntention of research is to improve treatment for addictions and mental illness
(CONTINUED ON PAGE 8)
Recipe for SuccessWith the holidays upon us, homes are filled with sounds of laughter. Gifts are being purchased. Trees are being trimmed. All types of goodies are being baked. Meals are being planned and grocery stores are flooded with folks buying ingredients to make their family favorites. As any good cook knows, a recipe is not complete if any of the ingredients are missing.
Are you missing the right ingredient to make your electronic health record your recipe for success? Is your documentation meeting standards? A pinch of this, a dash of that - Meaningful Use, Arkansas Healthcare Payment Improvement Ini-tiative (AHPII), PCMH, and ICD-10 are just some examples of the significant ingredients impacting healthcare organizations today. As the implementation of EHR software is increasing so is the demand for accurate, timely documenta-tion. Meeting government requirements is a daunting task. Is the time spent charting in your EHR getting in the way of patient care or possibly your own family time?
Speech recognition, when combined with an EHR, offers flexibility, conve-nience and efficiency. While some physicians may use the same EHR software, they may have vastly different styles of documentation, which an EHR alone typically cannot accommodate. Speech recognition along with point and click EHR templates allow for the capture of structured data as well as the narrative data needed to document the substance of an encounter.
Having the Right IngredientsAHIN Professional Services has partnered with Nuance Healthcare to offer physicians an alternative to template style documentation. With Dragon Medi-cal Practice Edition 2, clinicians can efficiently navigate and dictate medical decision-making and treatment plans directly into a patient’s record. The result allows accelerate adoption of their chosen EHR.
Dragon Medical allows clinicians to use a narrative format to dictate a patient encounter in their own words, including the HPI, ROS, PE, Assessment and Plan. This gives referring physicians and ancillary providers a clearer and more detailed patient assessment and prognosis.
Combining Dragon Medical with an EHR system, providers can feel more confident their patient encounter documentation will support the coding level truly reflecting the work you are doing. Dragon Medical Practice Edition is the leading speech recognition solution in healthcare today. It is 99% accurate ‘out of the box’ and includes over 90 medical specialty vocabularies while support-ing multiple regional accents. It includes a macro library for standard notes and ‘medical normals’ by body system; allowing for navigation to different areas of the chart, software programs and websites, all while dictating into the medical record.
Perfecting the RecipeIf you ever tried to emulate a mother or grandmother’s recipe you understand even if you follow directions distinctly it still doesn’t quite taste like hers. With experience comes knowledge and the recipe becomes perfection. The quali-fied team at AHIN Professional Services has both experience and knowledge. We understand that each physician practices differently. We will evaluate your physicians EHR workflows and create a solution to integrate Dragon Medi-cal into your practice. Our staff will travel to your location to provide more information and a FREE demo of Dragon Medical to you and your colleagues. Have you already purchased Dragon Medical? In addition, we provide educa-tion on how to get the most out of your voice recognition software – from set up to implementing and utilizing the system to the fullest. Don’t be caught without a vital ingredient needed to complete your recipe for success! Let AHIN Professional show you how you can make the most of your EHR through voice recognition.
Happy Holidays from the Staff at AHIN Professional Services! We look for-ward to working with you in the New Year!
Kim Allen, CPEHRManager, Health Information Technology
(501) 378-2446 • www.ahinservices.com
AHIN Professional Services
@AHINPro
Dr. Clint Kilts
6 > NOVEMBER/DECEMBER 2014 a r k a n s a s m e d i c a l n e w s . c o m
and was involved in biomedical engineer-ing education and research for at least ten years prior to 2012. When the department was announced, several students in the biomedical stream of biological engineer-ing transferred to the new program.
“We were thus able to have gradu-ates in the spring of 2013 and more in the spring of 2014,” Saxena said. “At the same time, Arkansas students who were planning to go outside the state for studying biomedical engineering decided to stay within the state by joining our program and that contributed to its very rapid growth.”
In addition to being a good undergraduate degree for students who plan on attending medi-cal school, the depart-ment is also preparing students to work as pro-fessionals to manage and plan the introduction of new technology in hospitals and clinics, provide user training on specialized equip-ment, and design, operate and maintain sophisticated medical equipment.
“This range of expertise will be in-valuable to manufacturers of medical equipment, and also to hospitals and clin-ics that want to continuously upgrade technology for direct patient care,” Sax-ena said. “The graduates will not only un-derstand the medical terminology needed to communicate with doctors and nurses, but will also be able to assist them in
adopting new medical technology to en-hance patient care.”
In late August, the College of Engi-neering dedicated the biomedical engi-neering wing that had undergone $4.3 million in renovations. Located on the first floor of John A. White Jr. Engineer-ing Hall, it contains office space for the faculty and staff, and two new teaching laboratories.
“We’ve been saying for the past few years that we intend to capitalize better on our core research strengths, and the for-mation of this department is one way we are making good on that effort,” said Uni-versity of Arkansas Chancellor G. David Gearhart. “The completion of this reno-vation is another exciting step forward for this department. I anticipate big things and big ideas out of this department and the faculty.”
Saxena said the pro-grams are particularly im-portant in view of the fact that over the past two de-cades, engineering has es-tablished a good niche for
itself in the medical field through technol-ogy development and innovation.
“It is now regarded as an integral part of a good quality healthcare system,” Saxena said. “Applications of engineering in medicine include advances in drug de-livery and drug design, non-invasive bio-imaging, prosthetic devices to replace human organs, early diagnosis of killer diseases such as cancer and heart problems, treat-ment of traumatic injuries, sensors for continuous monitoring of health con-ditions, and robot-assisted surgeries; the list goes on and on.”
There is a need for researchers in biomedical engineering in research hospitals and in the bio-medical device industry, and there are needs for implementing the latest technologies in all hospi-tals. “One can thus argue that biomedical research-ers and professionals are needed in Arkansas in all aspects of the medical profession much like doctors and nurses,” Saxena said.
The department is interested in part-nering with the medical community to (a) provide their students with an opportunity for hands-on experience as interns so they can become better engineers, and (b) seek collaboration for clinical studies. Faculty works with clinicians to assist them in clinical trials or to engage them in clinical trials as part of faculty research projects.
Faculty members include Tim Mul-doon, MD, PhD, Jeff Wolchok, PhD and David Zaharoff, PhD, who have each earned federal grants from the National Institutes of Health. Wolchok and Kartik Balachandran have jointly received Na-tional Science Founda-tion funding for research related to brain injuries.
Muldoon is working on a non-in-vasive method of looking at cells in the body. Combined with contrast agents, substances that help medical professionals differentiate between types of tissues, this imaging technology could make it easier to diagnose, treat and monitor diseases
like cancer. Muldoon plans to further de-velop these technologies with the goal of making them available to hospitals and medical clinics.
Balachandran studies the way me-chanical forces affect cells and organs. Using photolithography and nanoengi-neering techniques, Balachandran cre-ates materials that mimic the properties of human tissues and tests the response of this material to different stresses and forces.
Zaharoff focuses on delivery systems for cancer vaccines and immunotherapies. He is developing a way to train the im-mune system to recognize and eliminate cancer. He has demonstrated in animal trials that encapsulating protein antigens in a biomaterial called chitosan enhances the body’s immune response and gener-ates a better vaccine. .
Xianghong Qian, PhD, is doing re-search focusing on understanding im-
portant biochemical processes at the molecular level using both computational and experimental tools.
Narasimhan Rajaram, PhD, has three areas of research interest: Diagnosis, optical spectroscopy and imaging for early cancer screening; discovery, quantitative tumor biology and prognosis, functional optical imaging of biomarkers of radiation resistance and recurrence.
Michelle Kim, PhD, is focused on teaching undergraduate courses and on guiding undergraduate research projects.
The department’s major areas of re-search areas are:
• Novel cancer treatments and im-munotherapy
• Bioimaging for early screening/detection and progression of cancer and for investigating ischemia/re-perfusion events
• Biomaterials and regenerative med-icine such as regeneration of skeletal muscles
• Cell and tissue mechanics for pro-gression of cardiovascular diseases and prognosis
• Understanding biochemical pro-cesses
New Biomedical Engineering Program Attracts 400 Students, continued from page 1
Ashok Saxena
Dr. Tim Muldoon
Jeff Wolchok, shown here with one of his students, investigates the effects of traumatic brain injury on a type of brain cell called an astrocyte using a novel benchtop “crash tester.”
David Zaharoff focuses on delivery systems for cancer vaccines and immunotherapies. He is studying a biomaterial called chitosan. He has demonstrated in animal trials that encapsulating protein antigens in chitosan enhances the body’s immune response against that specific antigen.
a r k a n s a s m e d i c a l n e w s . c o m NOVEMBER/DECEMBER 2014 > 7
FAYETTEVILLE— Medical Asso-ciates of Northwest Arkansas (MANA), a physician-owned group practice with 74 physicians representing 11 specialties at 17 different clinics in Northwest Arkan-sas, makes a big impact not just delivering healthcare, but also playing a major role in charitable giving.
Since 2006, the MANA Charitable Fund (MCF) has plowed tens of thousands of dollars worth of donations from its staff and patrons into a wide variety of chari-table services ranging from the scholarship for students in allied health programs to community health initiatives.
The MCF was established in 2006 when physicians and staff identified a need for a venue to provide charitable services to the community.
MANA makes it easy for its employ-ees to have contributions with a payroll deduction program to help fund programs that make a difference in Northwest Ar-kansas. Staff members can have as little as $2 or $5 per paycheck that goes into the MCF, although many participate at higher amounts. Participants vote on 12 charities to receive the donations each year.
Instead of having its own separate charity, MANA chose to have the funds managed by the Arkansas Community
Foundation (ACF). MANA Chief Finan-cial Officer Paula Storment said it makes sense to have MANA structured to raise funds to give to charities rather than try-ing to run the charitable programs itself because of the administrative cost and ex-pertise required to form and run your own charitable organization.
“We are in the medical service business and want to focus our human resources on taking care of patients,” Stor-ment said. “Arkansas Community Foun-dation takes that administrative burden off of us while still allowing us to give do-nations to charitable groups and provide scholarships.”
Employees love it, said MANA mar-keting director Carole Masterson.
“Each month a different charity gets that donation,” Masterson said. “We do check presentations each month where we learn more about each charity. We donated $24,000 in 2013, and will do the same thing for 2014.”
MCF has a Community Health Grant program that local charities can apply to fund special projects. The board includes both physicians and community. The board chooses the grant applica-tions from charities that make the biggest impact on the health of the community. Some of the charities that have received support include the Arkansas Children’s Hospital & Angel One, Little Rock, Habi-tat for Humanity and the 7 Hills Shelter in Fayetteville, and the Peace at Home Family Shelter, Northwest Arkansas Food Bank, the Springdale Children’s Safety Center and the Northwest Arkansas Chil-dren’s Shelter, all in Springdale.
“The 7 Hills Homeless Center has thoroughly enjoyed being a beneficiary of
the MANA charitable giving programs,” said Chelsea Miller, outreach liaison for the 7 Hills Homeless Center. “Through
our partnership, 7 Hills has been able to provide a variety of medical benefits to our clients including direct medical care, educational materials, and items essen-tial to the health and well being of our clients.”
One of MCF’s most popular events is a 5K fun run fundraiser usually held the last weekend in March. This event does double duty providing an activity that is healthy in itself, encouraging in-dividuals and families to get out and ex-ercise, in addition to raising money for local charities.
The MCF provides the materials for free health screenings at health fairs in the community throughout the year. Screenings include total cholesterol, glu-cose, body mass index, blood pressure and breast cancer risk assessment.
Another popular activity that other businesses can participate in is a MCF jeans day button.
“We provide posters and buttons to
ARKANSAS on the MEND BY BECKY GILLETTE
MANA Charitable Fund Reaches Far with Donations Helping Charities in NW ArkansasUsing Arkansas Community Foundation to administer funds removes the burden of administrative costs
How Can You Help?
Have a jeans day fundraiser for MANA Charitable Fund at your company.
Volunteer Your TimeVolunteer opportunities to
help with flu clinics, free health screenings, and the annual 5K fun-draiser.
Make a DonationVisit www.mana.md/chari-
tablegiving to make a donation.
Spread the WordLet students in allied health
programs know about the Murray T. Harris Scholarship to help with their school expenses.
For more information go online to www.mana.md/charitablegiving/
(CONTINUED ON PAGE 9)
8 > NOVEMBER/DECEMBER 2014 a r k a n s a s m e d i c a l n e w s . c o m
For more information: www.neabaptist.com
Founded in 1992, Arkansas Healthcare Personnel, based in Little Rock was formed to meet the growing demand for temporary healthcare personnel. Since that time, we have become one of the most trusted and
preferred provider of nurses in Arkansas.
We serve all of Arkansas, providing quality nurses, CNAs and respiratory therapists to many different types of facilities.
Due to our solid reputation and unwavering commitment to our customers and employees, AHP is able to recruit professional employees and
become partners with some of the leading medical facilities in the state.
Call Us Today For Your Nursing Needs!
800-959-4625 or 501-666-1825
425 NORTH UNIVERSITY AVE. | LITTLE ROCK, AR 72205
501-666-1825 FAX : 501-666-8544
www.ahpnurses.comPLACEMENT MARKET: THROUGHOUT THE STATE OF ARKANSAS
ment positions. At Mercy, the mission statement is, “As the Sisters of Mercy be-fore us, we bring to life the healing ministry of Jesus through our compassionate care and exceptional service.”
By keeping the goal of service to oth-ers at the forefront, Gehrig has made great strides in the two years he has been at the helm of Mercy Fort Smith. Fort Smith, which serves a 13-county rural area with a high poverty rate among the 440,000 residents, is extremely underserved by phy-sicians. It needs to add 134 primary care physicians just to meet national minimum standards.
In October the new $42-million Mercy Orthopedic Hospital in Fort Smith opened as a 24-bed stand-alone hospital designed to provide complete care for healthy pa-tients in need of total joint replacement. Mercy Fort Smith, which has 2,100 em-ployees, is soon to be a 500-bed system.
Mercy has also added three new clinics this year. Gehrig said the new facilities are critical for attracting more physicians. This August the hospital opened a new $5.3-mil-lion Mercy branded clinic and celebrated a $5.1-million expansion and renovation of the radiation oncology department inside the Hembree Mercy Cancer Center.
“If you are recruiting physicians and can’t show them where they will practice, and they have five or six other options, you are not going to be successful,” Geh-rig said. “That has been why we have been very focused on building new state-of-the-
art clinics. We have built three clinics the past two years with the third set to open in November. Each one is hiring 10 to 15 practitioners.”
Mercy also has four school-based clin-ics that are located in Mansfield, Waldron, Cedarville and Magazine.
“I would venture to say we have more system-based partnerships with school clin-ics than any other large provider in the state,” Gehrig said. “The farther someone has to drive for care, the more likely they are to delay or forgo care. Our school part-nerships work well. The schools have been able to secure grants for buildings that were no longer in use. Being able to get care at the clinic reduces school and work absen-teeism for people leaving to drive to Fort Smith.”
When they opened the school clinic in Cedarville, ten students got glasses who couldn’t see well enough to read, and one child who was severely underweight be-cause his teeth hurt too much to chew got dental care.”
Preferential treatment is given to students, but the clinics are open to the community. And services are available re-gardless of the ability of the patient to pay.
“We are blind to who is paying or if they have insurance,” Gehrig said. “We are a ministry, but operate as a business. It is a healthy balance. This region is eco-nomically distressed, so it is fortunate the state took advantage of the Medicaid ex-pansion.”
Mercy Clinic has added 30 new physi-cians to the system in the past 18 months, and now has 125 primary care physicians and 25 advanced practitioners. They are continuing to recruit. Primary care visits have increased from 3,000 visits per month three years ago to close to 12,000.
“And we are nowhere near to address-ing the access to care issue,” Gehrig said. “We will continue with aggressive physi-cian recruitment, and will be looking into establishing a mobile clinic, more use of telemedicine and improving transporta-tion. Sometimes patients still need to come to Fort Smith for care, and don’t follow up because they simply can’t afford the gas. All of the proceeds from our Foundation Gala will go to funding a non-emergency trans-portation system.
Gehrig also has his sights set on im-proving the safety culture at Mercy Fort Smith. His goal is a culture where any worker feels comfortable speaking out if something is seen that could affect the safety of a patient. The hospital is about a year into implementing a Lean Hospital Quality Improvement Program.
“Lean is not about cutting costs, but creating a culture where co-workers are problem solvers instead of everything being escalated to administration,” Gehrig said. “It is a process of coaching and mentor-ing our workers to enable them to prob-lem solve. It takes patience. It takes a lot of time.”
One example of how this can work is that their inpatient rehab facility was av-eraging seven falls per month. At the time Gehrig was interviewed for this article, the unit had gone 50 days without a fall. He attributes that in part to the daily huddles on the unit as well as the leadership team meeting every morning at 9 a.m. to talk about flow stoppers, patient safety con-cerns, and other issues.
“It is amazing to see how just doing that has improved teamwork through col-laboration and respect for each other and their respective challenges,” he said.
Another goal is continued outreach to fulfill their mission of addressing commu-nity health needs.
“I feel like we are doing better, but it
takes time to build relationships and trust and have a cohesive approach to serving the community,” Gehrig said. “It isn’t that you solve everything, but as a community have a cohesive approach.”
Promoting physician leadership is also a vital goal. Gehrig said Mercy is serious about integration strategies that mean not just that physicians have a voice at table, but are a part of the decision-making pro-cess and a lot of times leading the decisions, implementing them and rolling them out.
For his personal life, Gehrig has a focus on being a good husband to his wife, Kristen, and father to their three children, Alyssa, 9, Drew, 8, and Anna, 2.
The family loves getting outdoors, par-ticularly on the river, and Gehrig is a fan of stand-up paddle boarding, which he jok-ingly refers to as redneck surfing. This past summer, the family visited 13 states while logging 5,200 miles on their motorhome.
“Once you are a camping family, that is your idea of a great vacation,” he said. “No email, no screen time, and lots of time for creative play.”
Healthcare Leader: Ryan Gehrig, continued from page 1
Mercy at a GlanceMercy’s footprint runs throughout western and northwestern Arkansas. Hospital facilities are:
•Mercy Hospital Fort Smith
•Mercy Orthopedic Hospital Fort Smith
•Mercy Hospital Rogers
•Mercy Hospital Berryville
•Mercy Hospital Booneville
•Mercy Hospital Ozark
•Mercy Hospital Paris
•Mercy Hospital Waldron
There are also more than 300 Mercy Clinic providers (doctors and advanced practitioners) in nearly 100 locations from Bella Vista to Waldron.
taking a clinic-delivered therapy and repro-ducing it in a MRI to capture the effects of therapy.”
Another prong of the research involves how the brain codes our differing cognitive abilities. If there was better understanding of why some people have poor memory recall and others have excellent recall, it could lead to treatment to help people improve their cognitive abilities.
“We are interested in studying some-thing few people have studied in the past,” Kilts said. “We are studying human varia-tion. Our science has the ability to provide personal descriptions of how the brain varies to produce differing cognitive abilities. We want to align the brain imaging center with the personalized medicine initiative.”
An important part of the work is educa-
tion and training.“This is a very complex technology,
and applications are complex,” Kilts said. “While my generation has done a lot in developing this and related technology, the next generation is going to be more im-pacting. We have an obligation to train the next-gen imaging scientists. We are actively involved in training the scientists of tomor-row who want careers focused on the scien-tific and technological challenges of defining the neurobiology of human behavior and all of its variation. We are engaging the BIRC with enthusiasm and training this genera-tion across many ages and disciplines. We have a busy, active and successful training program. When we want to impress visitors to our center, we let the young trainees do the talking, and it makes the day.”
Powerful Tesla MRI, continued from page 5
a r k a n s a s m e d i c a l n e w s . c o m NOVEMBER/DECEMBER 2014 > 9
sure that records are used in a meaning-ful way. SHARE can help providers meet these incentives for Meaningful Use by fa-cilitating the Transitions of Care summa-ries being exchanged between unaffiliated providers. This is the first year the state Medicaid program has implemented the Patient-Centered Medical Home (PCMH) model that sets expectation and require-ments for how practices are going to man-age Medicaid patients, which includes coordination of specialty care, medication compliances, and making sure necessary tests are done. If a practice qualifies and enrolls in the PCMH initiative, one re-quirement is to join SHARE to receive in patient discharge and transfer informa-tion. These “event notifications” will alert the practice of emergency department and hospital admissions, enhancing coordina-tion of care for follow-up visits and reduc-ing the cost of care.
“If a patient goes to a hospital and someone else admitted them, what Medic-aid has found out is often the primary care provider that has primary responsibility for that patient may not get timely noti-fication that the patient was admitted or discharged from the hospital,” Scott said. “You can’t manage what you don’t know about. It is not about blaming anybody. It is simply fixing the way the system should work in managing chronic conditions. The folks responsible for care need ac-cess to information about their patients.” Currently more than 270 healthcare facili-ties in Arkansas are connected to SHARE, and there are more than 850,000 discrete patient records in the system. “We think at the rate things are going now it may hit a million before the end of the year,” Scott said.
T A K E A D E E P B R E A T H . . . C A R T I C A N H E L P Y O U B R E AT H E E A S I E R .
In Arkansas, lung cancer is the leading cause of cancer death, causing more deaths than breast, colonand prostate cancers combined. But now there is hope with Low-Dose CT screenings, which areexpected to reduce lung cancer deaths by 20 percent in high-risk patients.
Low-Dose CT scans are recommended for those who meet the following criteria:
• Current or former smokers (aged 55 to 74 years old)• Smoking history of at least 30 pack years (number of packs per day x number of years = pack years)
• No history of lung cancer
carti.com
To learn more about Lung Cancer Screenings, talk to your physician or call CARTI at 1-800-482-8561.
Ad Sponsored by:
American Cancer SocietyAmerican Medical AssociationAmerican College of Chest PhysiciansAmerican Lung AssociationAmerican Society of Clinical Oncology
American Society for Radiation OncologyAmerican Society of Thoracic SurgeonsAmerican College of RadiologyNational Comprehensive Cancer NetworkU.S. Preventive Services Task Force
The following major medical societies endorse Lung CancerScreenings with Low-Dose CTs:
SHARE, continued from page 4
For more information visit www.sharearkansas.com or http://ohit.arkansas.gov/
a company for the fundraiser,” Masterson said. “Employees who choose to partici-pate pay $5 to wear jeans and they get a MCF jeans day button. It helps bring awareness to MCF and raise money. So far we have done it at MANA clinics and Arvest Bank, but hope to expand in the next year.”
There is also a program to help healthcare employees who have been harmed by natural disaster, fire or other misfortunes.
“Any healthcare employee can apply who has had an emergency,” Masterson said. “It started when we saw a need to help some of our coworkers, and we have been able to help a lot of people that way. The MANA Charitable Disaster and Emergency Hardship Relief Fund pro-vides assistance to healthcare employees who have experienced a disaster or emer-
gency hardship beyond their control or one in their immediate family. It seeks to assist healthcare employees who lack the necessities of life, involving physical, men-tal, or emotional well-being, as a result of poverty or temporary distress.”
Examples of needy persons include a person who is financially impoverished as a result of low income and lack of financial resources, a person who temporarily lacks food or shelter and the means to provide for it, and someone who is temporarily not self-sufficient as a result of a sudden and severe personal or family crisis such as being the victim of a crime of violence
or being physically abused.Another important effort helps ad-
dress healthcare workforce needs by providing three Murray T. Harris scholar-ships per year for students in allied health programs. The scholarships focus on pro-fessions within the healthcare sector that are currently underserved to help attract qualified candidates in these fields. The grant making committee at the Fayette-ville Area Arkansas Community Founda-tion evaluates applicants. Financial need is considered, but does not have to be the primary consideration.
MANA Charitable Fund Reaches Far, continued from page 7 Online Event Calendar
To submit or view localevents visit the Arkansas Medical News website and click on the calendar icon on the right hand sidebar.
arkansasmedicalnews.com
10 > NOVEMBER/DECEMBER 2014 a r k a n s a s m e d i c a l n e w s . c o m
Mercy Opens New Orthopedic Hospital in Fort Smith
FORT SMITH: More than 200 peo-ple gathered on a beautiful fall day to celebrate a new destination for health-care in Fort Smith. After more than two years of planning and construction, the 24-bed Mercy Orthopedic Hospital opened to patients in October. The fa-cility is thoughtfully designed to cater specifically to patients in need of total joint replacement.
Baby boomers (the generation born between 1946 and 1964) are an estimated 76 million strong – about 26 percent of the population. As these Americans grows older and enjoy lon-ger life spans, the need for orthopedic services is increasing. Healthcare think tank Sg2 estimates the number of in-patient orthopedic procedures done in Arkansas will increase by 22 percent in the next five years.
The Mercy Orthopedic Hospital is unique to the region and represents not only greater access to care for those in the community but also an opportuni-ty to attract patients from outside the area.
The 69,000 square foot hospital is two stories and attaches seamlessly to the existing surgery center.The hospi-tal’s first floor includes:
• 10,138 square foot outpatient re-habilitation clinic with a therapy pool serving more than 100 pa-tients per day
• Pre-operative screening area where patients will come prior to surgery for a physical, EKG, x-ray and lab screening
• Surgery waiting and registration•Café serving breakfast, lunch and
a light dinner with seating for 50 and patio dining available.
The second floor consists of:• 24 fully-furnished patient rooms
designed for the comfort of post-surgical patients
• Shell space for 12 additional beds bringing the potential hospital capacity to 36 beds
•Chapel•Waiting/vending area for families
Intensivist Joins Sparks Health System
FORT SMITH: Fiorella Nawar, MD, is now providing care for patients in the Intensive Care Unit at Sparks Regional Medical Center.
She most recently practiced medicine at Cooper University Hospi-tal in Camden, New Jer-sey. She has spent much of her career in ICU’s caring for surgical and pulmonary patients.
As an intensivist, Dr. Nawar will work closely with a patient’s primary care phy-sician, as well as critical care nurses and other medical staff to provide superior care for the hospital’s most seriously ill patients such as those suffering from car-diac arrest, respiratory failure, strokes, or infections.
Nawar earned her Doctor of Medi-cine from Lebanese University in Beruit in 2005. She is fluent in English, French and Arabic.
Neurosurgeon Adib Abla Joins UAMS
LITTLE ROCK: Neurosurgeon Adib Abla, M.D., has joined the University of Arkansas for Medical Sci-ences (UAMS) and will see patients at the Jackson T. Stephens Spine & Neuro-sciences Institute.
Abla offers both sur-gical and minimally inva-sive endovascular (inter-ventional) therapy for aneurysms, AVMs (arteriovenous malformation), cavernous malformations, and carotid disease. He performs surgical bypass for ischemic disease and unclippable, uncoilable an-eurysms and offers interventional intraar-terial therapy for acute stroke.
Abla is also an assistant professor of neurosurgery in the UAMS College of Medicine. He came to UAMS from the University of California at San Francisco School of Medicine where he completed a vascular neurosurgery fellowship and was a clinical instructor in the Depart-ment of Neurological Surgery.
Abla received his medical degree at the University of Pittsburgh School of Medicine in Pittsburgh in 2006. In 2013, he completed a neurosurgery residency and a cerebrovascular and skull base fel-lowship at Barrow Neurological Institute in Phoenix.
NEA Baptist Clinic Expands Hilltop Clinic and Urgent Care
JONESBORO: NEA Baptist Clinic is undergoing an expansion of the fam-ily practice and urgent care facilities at their Hilltop location – located at 4901 E. Johnson, across the street from their new medical campus.
The expansion of the Hilltop clinic includes the addition of space – ap-proximately 2300 sq. ft, including 9 exam rooms, a procedure room, 2 offices and a separate entrance and waiting room for
Occupational Medicine. Ryan Brenza, DO, will be joining Melissa Yawn, MD, MRO, Jeffery Barber, DO, MRO, and Tim Shown, DO.
Ryan Brenza, DO, has practiced with NEA Baptist Clinic for more than 3 years. He is a board certified family prac-tice physician with more than 10 years of experience in emergency care, family medicine and occupational medicine.
Patients who are established at the Trumann Clinic can also choose to con-tinue receiving care at that clinic with Dr. Brannon Treece and new physician, Dr. Ronald Barnett, both board certified in Internal Medicine\Pediatrics.
NARMC EMS Paramedic is named Arkansas Paramedic of the Year
HARRISON: North Arkansas Re-gional Medical Center EMS Paramedic John Robinson was given the honor of being named Ar-kansas Paramedic of the Year. This honor, which is awarded each year at the Arkansas State Emergen-cy Medical Services (EMS) Conference, is bestowed upon a paramedic who’s dedi-cation, motivation and drive places them at the top of the industry. Robinson, a 21 year veteran paramedic with NARMC EMS, was selected for the honor by a se-lection committee who reviewed pack-ets of information on paramedics from across the entire state.
Robinson was born at North Ar-kansas Regional Medical Center, raised in Western Grove, and currently lives in Diamond City with his family. .
Dr. Brian Baltz Joins Dr. Dennis Parten at Monette Family Practice Clinic
MONETTE: Brian Baltz, M.D., has joined Dr. Dennis Parten as a primary care physician at Monette Family Prac-tice Clinic in Monette.
Baltz earned his Medical Degree from the University of Arkansas for Medi-cal Sciences in Little Rock and has been in private practice at Pocahontas Medi-cal Clinic for the last two years.
Prior to that he completed a fam-ily practice residency through the Area Health Education Center-Northeast at St. Bernards, serving as chief resident during his last year. He holds an undergraduate degree from the University of Arkansas in microbiology and a master’s degree from UAMS in physiology and biophysics.
Parten has served as a family prac-tice physician in Monette for the last 26 years, having founded the Monette clinic in 1988. He holds an M.D. degree from UAMS and completed a family practice residency through the Area Health Edu-cation Center-Northeast at St. Bernards.
Medical News is pleased to provide space for press releases by providers in our Grand Rounds section. Content and accuracy of the releases is the sole responsibility of the issuer.
SOUTHCOMMChief Executive Officer Chris FerrellChief Financial Officer Patrick Min
Chief Marketing Officer Susan TorregrossaChief Technology Officer Matt Locke
Chief Operating Officer/Group Publisher Eric Norwood
Director of Digital Sales & Marketing David Walker
Controller Todd PattonCreative Director Heather Pierce
Director of Content / Online Development Patrick Rains
GrandRounds
Dr. Fiorella Nawar
Dr. Adib Abla
John Robinson
4/5 Exam RoomsWaiting/Reception, Triage, Offices,
First floor, 1,863 rsf Easy Access - Great location!
Medical Space Available
BRECKENRIDGE PROFESSIONAL BUILDING
Call Cheryl White or Drew Mentzer
375-3200
a r k a n s a s m e d i c a l n e w s . c o m NOVEMBER/DECEMBER 2014 > 11
Mutual Interests. Mutually Insured.
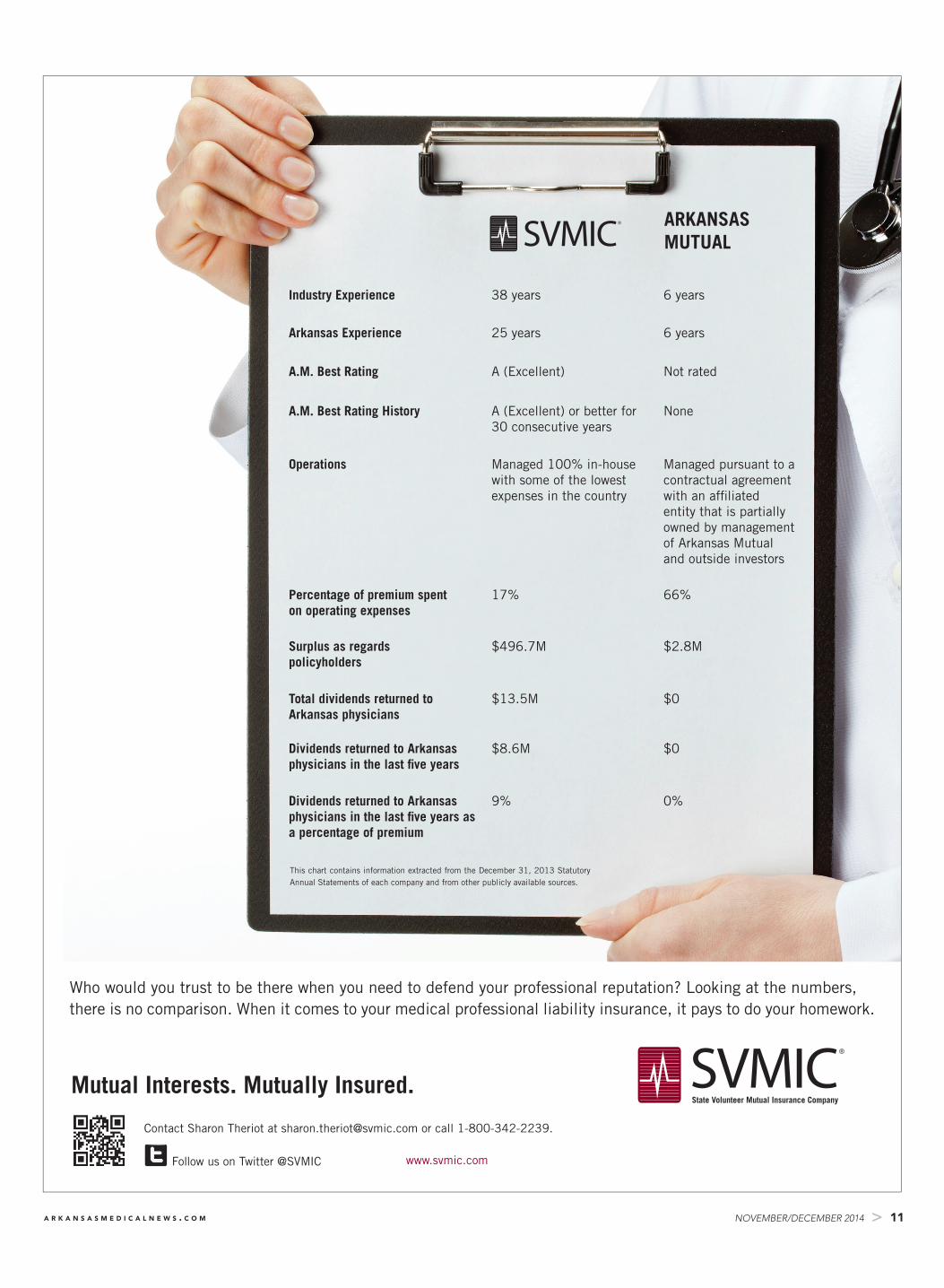
Who would you trust to be there when you need to defend your professional reputation? Looking at the numbers, there is no comparison. When it comes to your medical professional liability insurance, it pays to do your homework.
A.M. Best Rating History A (Excellent) or better for 30 consecutive years
None
Operations Managed 100% in-house with some of the lowest expenses in the country
Managed pursuant to a contractual agreement with an affiliated entity that is partially owned by management of Arkansas Mutual and outside investors
Percentage of premium spent on operating expenses
17% 66%
Surplus as regards policyholders
$496.7M $2.8M
Total dividends returned to Arkansas physicians
$13.5M $0
Dividends returned to Arkansas physicians in the last five years
$8.6M $0
Dividends returned to Arkansas physicians in the last five years as a percentage of premium
9% 0%
This chart contains information extracted from the December 31, 2013 Statutory Annual Statements of each company and from other publicly available sources.
“When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of my life. And I said, ‘time out – if I have cancer, I’m going to UAMS.’ My comprehensive care included chemotherapy followed by a double mastectomy, radiation and reconstruction. It gave me incredible comfort to know that I had a team of brilliant doctors who are among the best in the U.S. Today I am grateful to be a cancer survivor, always mindful of how precious it is to be alive.”
“Every morning I wake up and am thankful for UAMS. They pulled me through, and it’s a new day.”
UAMShealth.com/cancer
Stacy Sells, Breast Cancer SurvivorStacy Sells, Breast Cancer SurvivorStacy Sells, Breast Cancer SurvivorStacy Sells, Breast Cancer SurvivorStacy Sells, Breast Cancer Survivor
the“When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of “When I was diagnosed with stage IIIB inflammatory breast cancer, I knew I was in for the fight of