Challenges In Financing An Efficient Health Care System “Health Sans Frontieres” European Health Forum, Gastein 2006. Armin Fidler Sector Manager for Health, Nutrition, Population, Europe and Central Asia The World Bank. Why Everyone Talks About Health Financing …. - PowerPoint PPT Presentation
Challenges In Financing An Efficient Health Care System “Health Sans Frontieres” European Health Forum, Gastein 2006 Armin Fidler Sector Manager for Health, Nutrition, Population, Europe and Central Asia The World Bank
Transcript
Challenges In Financing An Efficient Health Care System
“Health Sans Frontieres” European Health Forum, Gastein 2006
Armin FidlerSector Manager for Health, Nutrition, Population,
Europe and Central AsiaThe World Bank
2
Why Everyone Talks About Health Financing ….
• Health and Economics – Why the health sector takes center stage:– Efficiency of public spending: Health as a large public outlay– Social safety nets, poverty, catastrophic events:
• Poverty as a determinant and an outcome of ill health– Labor market implications: Health as an engine of economic
growth?• Health as a commodity and “luxury good”?
• Major Cost Drivers as experienced during the transition period in NMS– Hospital Infrastructure– Pharmaceuticals– Staff salaries, labor mobility– Medical Technology
3
How To Go About Containing Costs?
• “Control knobs” to modulate health expenditures – Supply side: Health Technology Assessment (HTA)
• Master Planning for Infrastructure and equipment
• Demographic, epidemiological, economic factors
– Demand side: Demand modulation• Co-payments
• OTC pharmaceuticals
• But also: “supply induced demand” – critical role of physicians and the availability of technology.
4
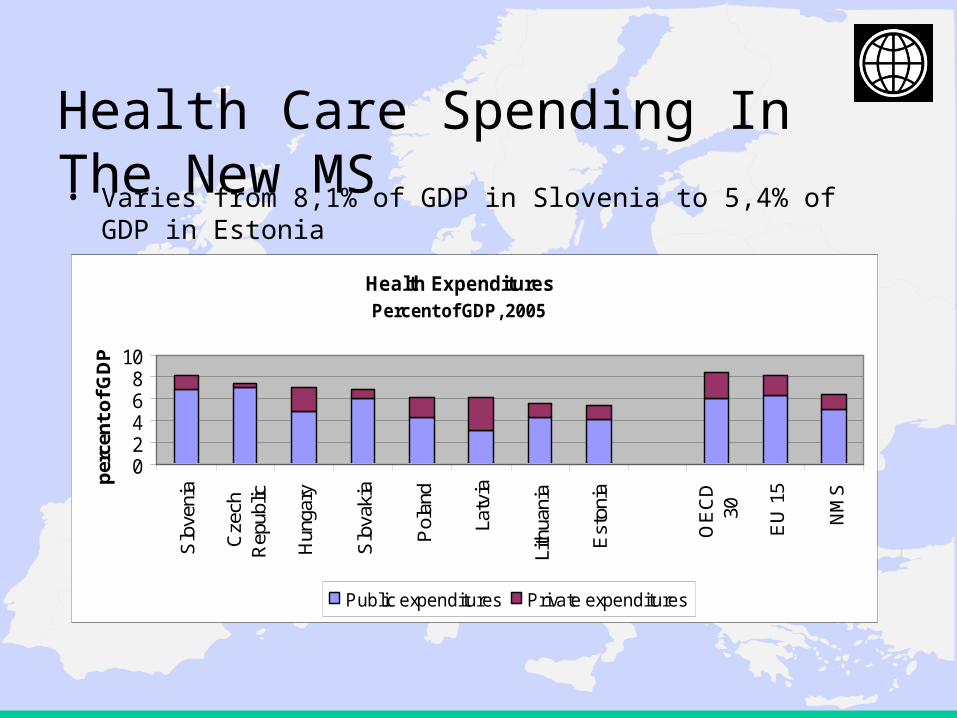
Health Care Spending In The New MS• Varies from 8,1% of GDP in Slovenia to 5,4% of GDP in Estonia
– carried out health sector reforms of variable scope – but no
discernable trend as far as directions and results.
• Health expenditures: not out of line compared to OECD, but
sector in debt where expenditures consistently exceed
revenues derived from payroll tax and budget allocations.
• Near term outlook: Drive for modernization, upgrading of
technology and legacy of past creates pressure on expenditures
and mandates to raise extra revenue and to contain costs.
6
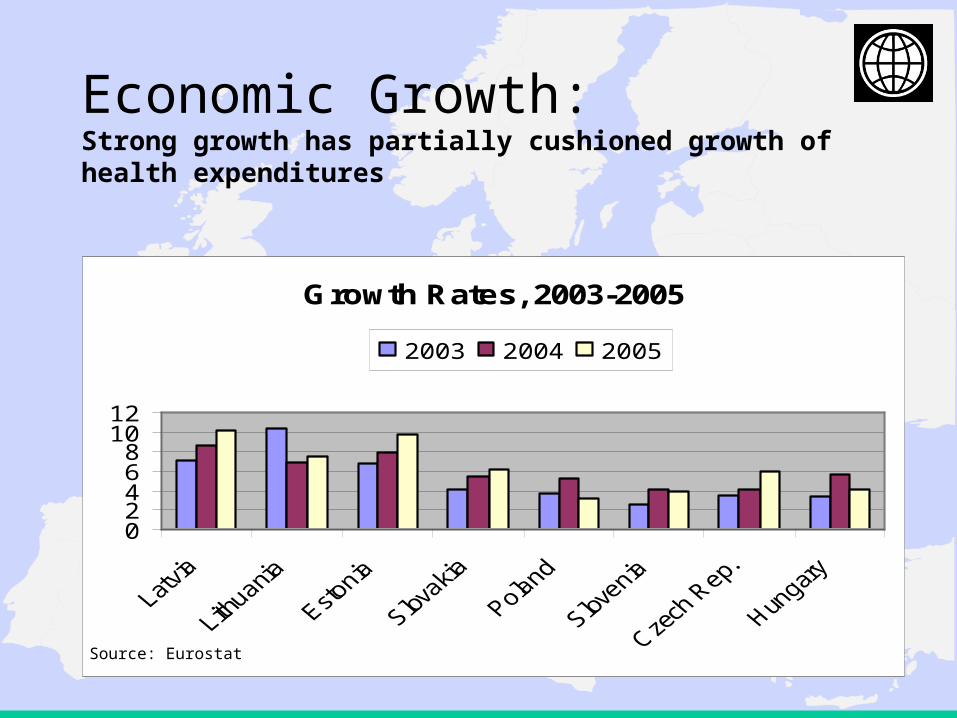
Economic Growth: Strong growth has partially cushioned growth of health expenditures
Growth Rates, 2003-2005
02468
1012
2003 2004 2005
Source: Eurostat
7
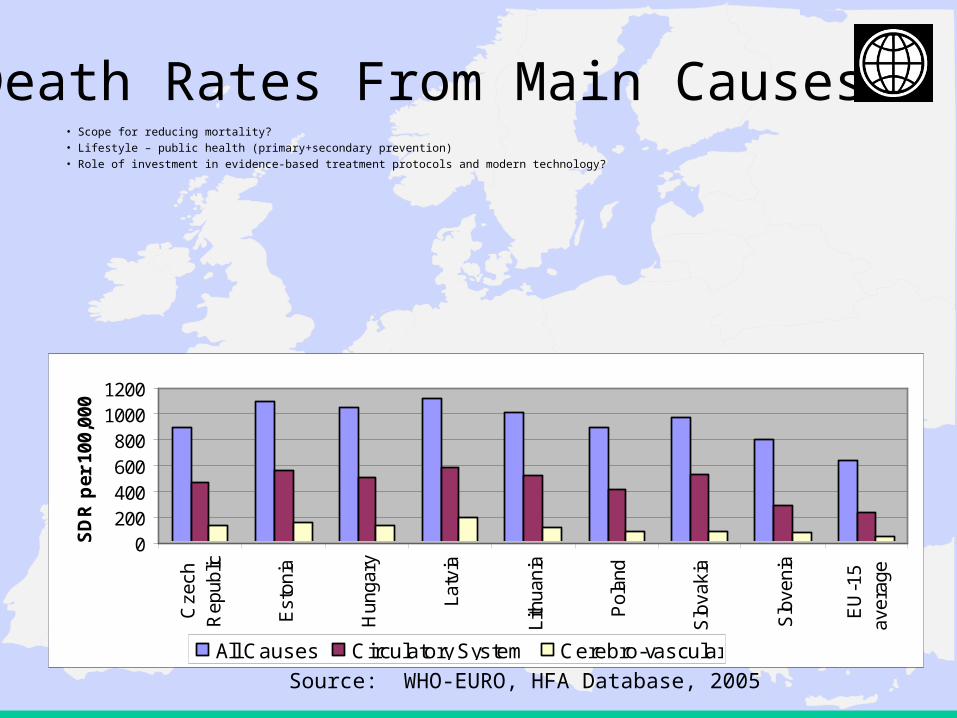
Death Rates From Main Causes• Scope for reducing mortality?• Lifestyle – public health (primary+secondary prevention)• Role of investment in evidence-based treatment protocols and modern technology?
0200400600800
10001200
Cze
chR
epub
lic
Est
onia
Hun
gary
Latv
ia
Lith
uani
a
Pol
and
Slo
vaki
a
Slo
veni
a
EU
-15
aver
age
SD
R p
er 1
00,0
00
All Causes Circulatory System Cerebro-vascular
Source: WHO-EURO, HFA Database, 2005
8
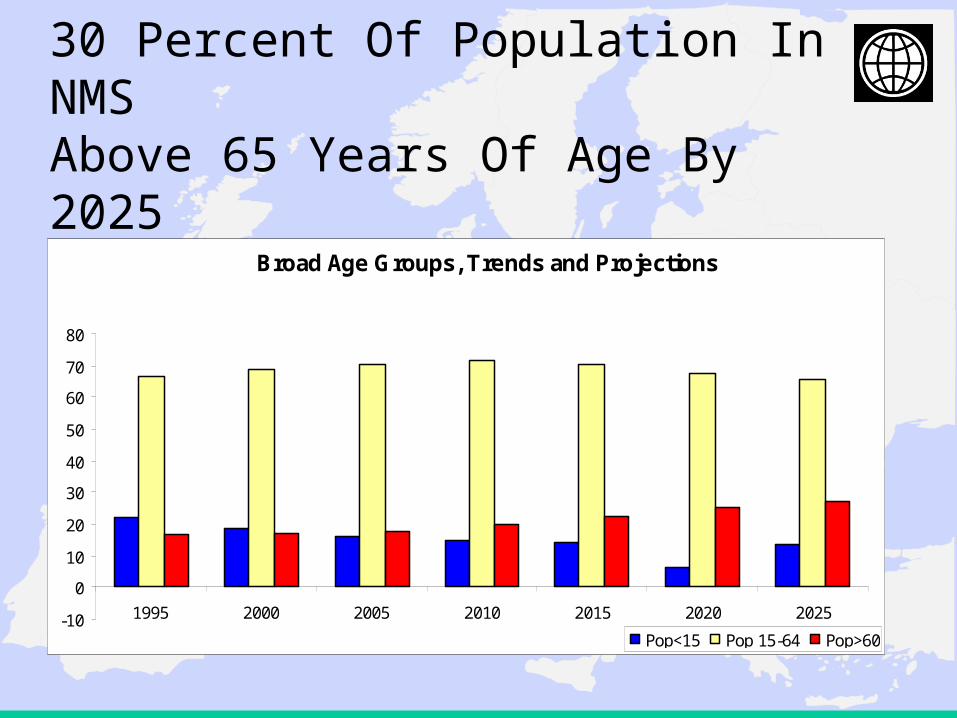
30 Percent Of Population In NMS Above 65 Years Of Age By 2025
Broad Age Groups, Trends and Projections
-10
0
10
20
30
40
50
60
70
80
1995 2000 2005 2010 2015 2020 2025
Pop<15 Pop 15-64 Pop>60
9
Ageing And Changing Demographics• Difficult to quantify the impact that an ageing population
will have on health expenditures – Bulk of health expenditures will still occur in last year of life– But increased life expectancy despite multi-morbidity will take toll
• But there is little doubt that an increasing proportion of people over 65 will exert some upward pressures on health care costs
• A critical issue is long-term care for the very old, which can become a significant financial burden as informal family-based care begins to decline– Few NMS have drawn up credible long-term strategies for LTC– EHFG Session on Saturday, sponsored by EU and WB!
10
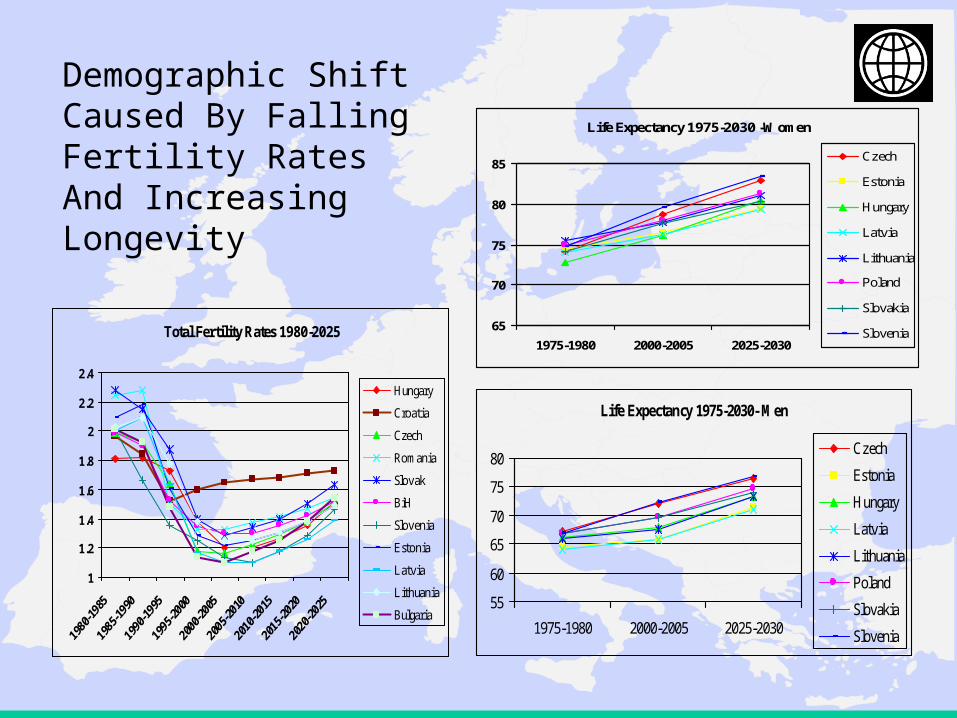
Demographic Shift Caused By Falling Fertility Rates And Increasing Longevity
Total Fertility Rates 1980-2025
1
1.2
1.4
1.6
1.8
2
2.2
2.4
Hungary
Croatia
Czech
Romania
Slovak
BiH
Slovenia
Estonia
Latvia
Lithuania
Bulgaria
Life Expectancy 1975-2030- Men
55
60
65
70
75
80
1975-1980 2000-2005 2025-2030
Czech
Estonia
Hungary
Latvia
Lithuania
Poland
Slovakia
Slovenia
Life Expectancy 1975-2030 -Women
65
70
75
80
85
1975-1980 2000-2005 2025-2030
Czech
Estonia
Hungary
Latvia
Lithuania
Poland
Slovakia
Slovenia
11
Principle Challenges for a Sustainable Health Financing System
(i) Hospital Infrastructure
(ii) Pharmaceuticals
(iii) Staff salaries
(iv) Medical Technology
12
(i) Hospital Infrastructure• Extensive hospital infrastructures expensive to maintain
– many structures not appropriate (location, use , size)
• Oversupply of hospital infrastructure in NMS is a historic legacy –
– but also highly prevalent in OECD
• Almost all countries have taken steps to reduce hospitals and
acute-care hospital beds
– but there are only few success stories.
• The problem of debts and contingent liabilities in countries with
dominant public hospital sector
13
(ii) Pharmaceuticals
• Drugs and medical devices seem to be the single largest cost drivers in most countries
• Rx total cost = Price x Volume• Questions related to:
– Extent of publicly financed benefit vs. OTC– Role of co-payments to control prescription and
consumption– Clinical practice guidelines and prescription practices based
on evidence– HTA and pharmaco-economics
14
(iii) Human Resources - Wages• Salaries account for more than 50 - 60% of health expenditures in most
countries, this trend is increasing the pressure on overall health spending
• The pressure on salaries has increased in EU NMS
– Health sector salaries in NMS rise faster then the average salaries in the economy
– from low starting point
• Example: Lithuania
70% of medical staff leaving Lithuania indicates “higher salaries” in the target
country as reason for leaving, 50% leaves because of the “higher living
standard” and 40% because of “better career possibilities”.
15
(iv) Medical Technology
• Absorption of available and new technologies puts pressure on health expenditures
• Modern health care is most information and technology-intense industry – difficult to saturate!– ECA countries – transformation from pre-transition
production model to modern health delivery system – not fully concluded yet, despite 15 years of reform and investments
– Therefore much room for either big mistakes and “dead ends” but also opportunities to leapfrog to leadership position – avoiding mistakes of others.
16
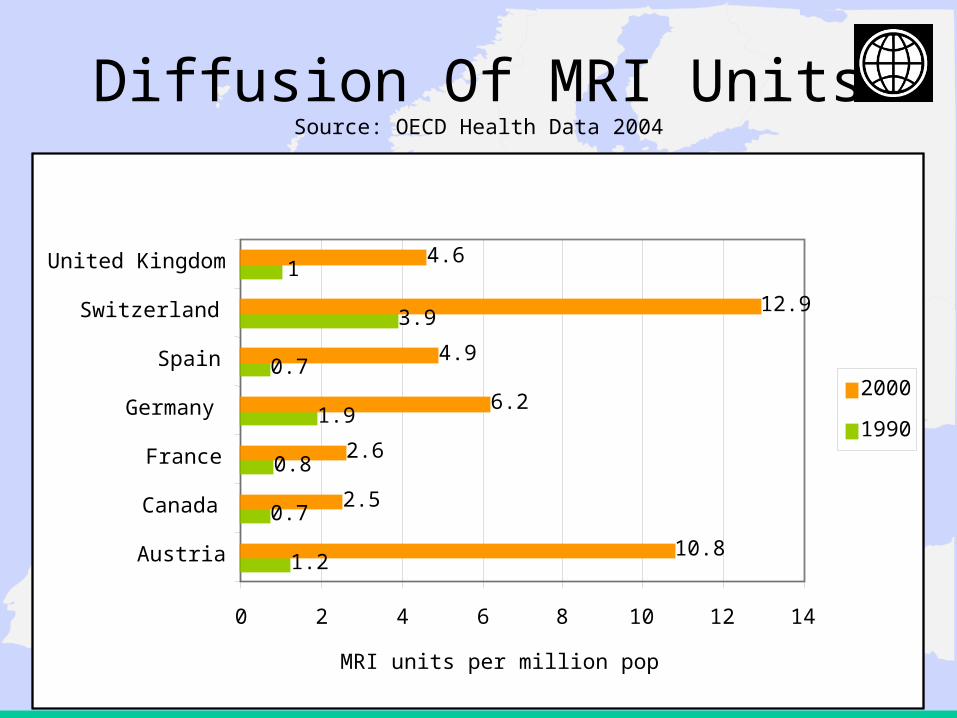
Diffusion Of MRI UnitsSource: OECD Health Data 2004
1.2
0.7
0.8
1.9
0.7
3.9
1
10.8
2.5
2.6
6.2
4.9
12.9
4.6
0 2 4 6 8 10 12 14
Austria
Canada
France
Germany
Spain
Switzerland
United Kingdom
MRI units per million pop
2000
1990
17
Health Technology Assessment (HTA)
• “policy research that systematically examines short- and long-term consequences of health and resource use, of the application of a health technology, a set of related technologies or a technology related issue”
• “a bridge between the world of research and the world of decision-making”
• Together with evidence-based medicine (EBM) and clinical practice guidelines (CPG) it builds a body of best practice initiatives
– Session on HTA and Quality of Care (Jan Bultman, WB) at EHFG
18
Objectives Of HTA
• Assist decision makers in deciding which technologies to adopt (C-E, certificate of use, etc.)
• Encourage the appropriate use of health technology, based on established evidence
• Provide impartial comprehensive information through the collection and analysis of information concerning the effectiveness and cost of health technology and health impact
19
Evidence When HTA Used Effectively
• Provides information from an independent, impartial perspective
• Supports and assists decision makers in making informed policies and decisions in health care
• Is an essential element of a health care system that seriously
• Creates a bridge between researchers, decision-makers, health care providers and the public
• Leverages health research investment in order to create a cost-effective health care system
20
Health Sector Modernization – Recalibration of Financing And...
• MoH stewardship – intergovernmental action (MOF – HIF)- Final goal must be population health outcomes - Payer could efficiently purchase “wrong” health service!
• MOF – HIF: Difficulty in many countries to sustainably raise revenues for health: