Arteriovenous Crossing Patterns in Branch Retinal Vein Occlusion Jialiang Zhao, MD,l Srinivas M. Sastry, MD, MPH,l Robert D. Sperduto, MD,l Emily Y. Chew, MD,! Nancy A. Remaley, MS,1 The Eye Disease Case-Control Study Group 2 Purpose: The study was designed to evaluate the relative anatomic position of the crossing vessels at the site of occlusion in eyes with branch retinal vein occlusion (BRVO). Methods: Fundus photographs of 106 eyes (104 patients) with recent BRVO from the Eye Disease Case-Control Study were used to examine the relative position of artery and vein at occluded crossings. Three separate comparison groups were formed by identifying corresponding arteriovenous crossings for each occluded crossing in: (1) the ipsilateral but opposite vessel arcade within eyes affected by BRVO; (2) the same quadrant in unaffected eyes of BRVO patients; and (3) the same quadrant in eyes of patients without BRVO, matched by age, sex, and race with the BRVO patients. Results: The site of obstruction of the branch vein was an arteriovenous crossing in all affected eyes. In 99% of eyes with BRVO, the artery was located anterior to the vein at the obstructed site. In the three comparison groups, the artery was anterior to the vein in 62%, 61%, and 54% of the crossings, respectively, yielding statistically significant differences for each group of control crossings compared with BRVO cross- ings (P < 0.001). Conclusion: Finding the vein to be conSistently between the more rigid artery and the retina at almost all arteriovenous crossings affected by BRVO suggests a possible role for mechanical obstruction in the pathogenesis of BRVO. Ophthalmology 1993; 1 00:423-428 Obstruction of the vein in branch retinal vein occlusion (BRVO) almost invariably occurs at an arteriovenous crossing. 1-3 Anatomic features of arteriovenous crossings, Originally received: August 25, 1992. Revision accepted: October 13, 1992. 1 Department of Health and Human Services, Biometry and Epide- miology Program, National Eye Institute, National Institutes of Health, Bethesda, Maryland. 2 Members of the Eye Disease Case-Control Study Group are listed in the Appendix at the end of the article. Presented at the Association for Research in Vision and Ophthalmology Annual Meeting, Sarasota, May 1992. and the secondary effects of arteriolar sclerosis, mayex- plain the apparent vulnerability of the crossing sites to venous occlusion. Normal features of arteriovenous crossings-the proximity of thin-walled vein and thick- walled artery, the narrowing of the venous lumen that normally occurs at crossings,4 and the sharing by artery and vein of a common adventitial sheath-provide the setting for occlusion. In the presence of systemic vascular disease, a common finding in patients with BRVO, the risk of occlusion may be accentuated when arteriolar scle- rosis results in increased rigidity of the crossing artery and contraction of the common adventitial sheath. Reprint requests to Robert D. Sperduto, MD, Biometry and Epidemiology Program, National Eye Institute, National Institutes of Health, Bldg 31, 6A24, Bethesda, MD 20892. Recently, Duker and Brown 5 provided further support for a mechanical basis for BRVO when they examined the relative anatomic position of the crossing artery and vein at the site of occlusion in 26 eyes with BRVO. In 423
Transcript
Arteriovenous Crossing Patterns in Branch Retinal Vein Occlusion
Jialiang Zhao, MD,l Srinivas M. Sastry, MD, MPH,l Robert D. Sperduto, MD,l Emily Y. Chew, MD,! Nancy A. Remaley, MS,1 The Eye Disease Case-Control Study Group2
Purpose: The study was designed to evaluate the relative anatomic position of the crossing vessels at the site of occlusion in eyes with branch retinal vein occlusion (BRVO).
Methods: Fundus photographs of 106 eyes (104 patients) with recent BRVO from the Eye Disease Case-Control Study were used to examine the relative position of artery and vein at occluded crossings. Three separate comparison groups were formed by identifying corresponding arteriovenous crossings for each occluded crossing in: (1) the ipsilateral but opposite vessel arcade within eyes affected by BRVO; (2) the same quadrant in unaffected eyes of BRVO patients; and (3) the same quadrant in eyes of patients without BRVO, matched by age, sex, and race with the BRVO patients.
Results: The site of obstruction of the branch vein was an arteriovenous crossing in all affected eyes. In 99% of eyes with BRVO, the artery was located anterior to the vein at the obstructed site. In the three comparison groups, the artery was anterior to the vein in 62%, 61%, and 54% of the crossings, respectively, yielding statistically significant differences for each group of control crossings compared with BRVO crossings (P < 0.001).
Conclusion: Finding the vein to be conSistently between the more rigid artery and the retina at almost all arteriovenous crossings affected by BRVO suggests a possible role for mechanical obstruction in the pathogenesis of BRVO. Ophthalmology 1993; 1 00:423-428
Obstruction of the vein in branch retinal vein occlusion (BR VO) almost invariably occurs at an arteriovenous crossing. 1-3 Anatomic features of arteriovenous crossings,
Originally received: August 25, 1992. Revision accepted: October 13, 1992.
1 Department of Health and Human Services, Biometry and Epidemiology Program, National Eye Institute, National Institutes of Health, Bethesda, Maryland.
2 Members of the Eye Disease Case-Control Study Group are listed in the Appendix at the end of the article.
Presented at the Association for Research in Vision and Ophthalmology Annual Meeting, Sarasota, May 1992.
and the secondary effects of arteriolar sclerosis, mayexplain the apparent vulnerability of the crossing sites to venous occlusion. Normal features of arteriovenous crossings-the proximity of thin-walled vein and thickwalled artery, the narrowing of the venous lumen that normally occurs at crossings,4 and the sharing by artery and vein of a common adventitial sheath-provide the setting for occlusion. In the presence of systemic vascular disease, a common finding in patients with BRVO, the risk of occlusion may be accentuated when arteriolar sclerosis results in increased rigidity of the crossing artery and contraction of the common adventitial sheath.
Reprint requests to Robert D. Sperduto, MD, Biometry and Epidemiology Program, National Eye Institute, National Institutes of Health, Bldg 31, 6A24, Bethesda, MD 20892.
Recently, Duker and Brown5 provided further support for a mechanical basis for BR VO when they examined the relative anatomic position of the crossing artery and vein at the site of occlusion in 26 eyes with BR VO. In
423
Ophthalmology Volume 100, Number 3, March 1993
100% of BRVO eyes, the artery lay anterior to the vein, toward the vitreous cavity. In two sets of control crossings, the artery lay anterior to the vein less than 70% of the time.
We have attempted to replicate Duker and Brown's finding5 by evaluating the relative position of artery and vein at the site of occlusion in 106 eyes with recent BRVO. For comparison, we evaluated the crossing pattern at a similar order but non-occluded crossing in three different control groups. We also have compared the number of arteriovenous crossings in persons with and without BRVO to determine whether arteriovenous crossings are more common in persons with BRVO.
Methods
Cases of BR VO were identified between May 1986 and December 1990 in the Eye Disease Case-Control Study, a multicenter study of risk factors for several retinal disorders including BR YO. The study design has been described elsewhere.6 Patients with BRVO had to be between the ages of21 and 80 years, and BRVO had to have been diagnosed within the year before enrollment in the study. Patients with vasoproliferative retinopathy and intermediate or posterior inflammatory disease were excluded from the study. Controls for the Eye Disease Case-Control Study were enrolled concurrently with the cases and frequency-matched on age, sex, and race. Thirty-degree stereo fundus photographs were taken of fields 1 (centered on the disc) and 2 (centered on the macula),7 and the affected quadrant in eyes with BRVO. Stereo fundus photographs also were taken of fields 1 and 2 in the unaffected eyes of patients with BRVO and in one eye of the controls. Fluorescein angiography was performed on eyes with BRVO.
For purposes of this study, the following patients with BRVO were excluded because of difficulties in identifying or evaluating the arteriovenous crossings of interest:
1. Hemispheric BR YO. 2. BRVO involving small, macular vessels. 3. BRVO with extensive neovascularization or collat
eral vessels. 4. BRVO in which the crossing site of occlusion could
not be visualized because of extensive hemorrhage, poor quality photographs, media opacities, or multiple crossings of vessels in the region of the occluded crossing.
5. Cases with missing photographs.
Two physicians simultaneously examined the fundus photographs of eyes with BRVO, noting the clarity of the photographs, the quadrant of the occlusion, the order of the affected crossing, and the relative anatomic position of artery and vein at the site of occlusion. Fluorescein angiograms were used when necessary to assist in determining the artery-vein relationship. Disagreements between examiners were resolved by consensus.
424
For each crossing with an occlusion, the same examiners then attempted to identify three control crossings. The three crossings, which were used to form three separate comparison groups, included:
1. A crossing in the ipsilateral but opposite vessel arcade within the eye with BRVO. For example, for a superotemporal vessel occlusion, a control crossing was sought in the inferotemporal vessel arcade. If the occluded crossing involved the first crossing of the main trunk of the branch retinal vein, then a similar first-order crossing was sought for the control crossing. Similarly, if the index crossing involved a second- or third-order crossing, a corresponding second- or third-order control crossing was sought.
2. A similar-order crossing in the corresponding vessel arcade of the fellow eye of affected patients. The two patients with bilateral vein occlusions contributed no information to this control group.
3. A similar-order crossing in the corresponding vessel arcade of a patient without BR YO. These patients were randomly selected from an age-sex-racematched pool of patients who served as controls in the Eye Disease Case-Control Study population and who had fundus photographs of good quality.
The number of the control crossings varied for each comparison group depending on whether a corresponding crossing could be identified for the index BRVO crossing.
For the control crossings, the examiners noted the clarity of the photographs and evaluated the anatomic relationship of the crossing vessels.
In addition to evaluating the relative position of artery and vein at the selected crossings, the total number and the relative position of artery and vein of all first- and second-order arteriovenous crossings visible in a standard 30° color fundus photograph centered on the disc were evaluated in the fellow eyes of BR VO patients and the eyes of the control persons without BRVO.
The chi-square test for independent sample comparison and the Wilcoxon signed-rank test for matched pairs were used for the statistical analyses.
Results
Of the 361 patients with BRVO in the Eye Disease CaseControl Study, 104 (106 eyes) met our study's eligibility requirements (Table I). The right eye was involved in 54% (55/102) of the unilaterally affected patients. The mean age of BR VO patients was 63.7 years (range, 31-80 years); 69% were older than 60 years of age. Men and women were almost equally affected (49% for men versus 51 % for women) (Table 2).
Sixty-six percent of occlusions involved the superotemporal quadrant. Only two occlusions occurred in a nasal quadrant (Table 2). The site of venous obstruction in all affected eyes was an arteriovenous crossing. Most
Zhao et al . Arteriovenous Crossing Patterns
Table 1. Eligible and Ineligible Patients with Branch Retinal Vein Occlusion
Eligible Ineligible
Hemispheric BRVO Small vessel occlusion Extensive new vessels Inadequate view of A V crossing Missing photos
Total
No. (0/0)
104
80 69 64 33 11
361
(28.8)
(22.2) (19.1) (17.7) (9.1) (3.0)
(100.0)
BRVO = branch retinal vein oclusion; A V = arteriovenous.
affected crossings were second- (52%) or third- (40%) order crossings.
In 99% (105/106) of crossings with BRVO, the artery was located anterior to the vein at the blockage site (Table 3; Figs 1 and 2).
In all but one eye with BRVO, a similar-order arteriovenous crossing was present in the ipsilateral but opposite vessel arcade of the same eye. In only 62% of these crossings, compared with 99% of the crossings at obstructed sites, the artery was located anterior to the vein (chi-square; P < 0.001) (Table 3).
Corresponding arteriovenous crossings could be identified in 83 fellow eyes. (Sixteen eyes did not have corresponding crossings in the photographed field and the quality of the photographs or the fluorescein angiogram was too poor for evaluation in three eyes.) The artery was located anterior to the vein in 51 (61 %) of the fellow-eye crossings, which was significantly less frequent than for obstructed crossings (chi-square; P < 0.001) (Table 3).
A corresponding arteriovenous crossing could be identified in 85 of the 104 age-sex-race-matched persons without BRVO. This control group included 51 men and 53 women; 77 were white. The mean age of the group was 63.8 years. The artery was located anterior to the vein in 46 (54%) of the 85 crossings, which again was significantly less than for obstructed crossings (chi-square; P < 0.001) (Table 3). There were no statistically significant differences in arteriovenous crossing patterns among the three control groups (Table 3).
The number of arteriovenous crossings was counted in fellow eyes of patients with BRVO and eyes of persons without BRVO, using 30° fundus photographs centered on the disc. In the 99 fellow eyes with adequate photographs, there was an average of six crossings. In eyes of age-sex-race-matched persons without BR YO, the average number of crossings was 5.4, which was significantly fewer (Wilcoxon signed-rank test; P < 0.02) (Table 4).
Arteriovenous crossings were most common in the superotemporal quadrant. The differences between quadrants were not statistically significant in the fellow eyes of patients with BRVO. However, in eyes of persons with-
out BRVO, crossings were significantly more common in the superotemporal quadrant than either the inferotemporal or inferonasal quadrants (Wilcoxon signed-rank test; P < 0.05 when accounting for multiple comparisons)8 (Table 4).
The number and percentage of crossings in which the artery lay anterior to the vein in fellow eyes of BR VO patients and matched eyes of persons without BRVO is presented in Table 4. There were no statistically significant differences for all quadrants combined or between quadrants for the two groups of eyes (chi-square; P < 0.05) (Table 4).
Discussion
Our findings confirm Duker and Brown's observationS that the artery is positioned anterior to the vein at almost all arteriovenous crossing sites affected by BRVO. Duker and Brown noted an anterior location for the artery in all of 26 crossings with BR YO; we noted the finding in all but one of 106 affected crossings. For comparison, we identified corresponding crossings in: (1) a different vessel arcade in the eye with BRVO, (2) the fellow eye of patients
Table 2. Characteristics of Patients with Branch Retinal Vein Occlusion
Location of BR VO Superotemporal 70 (66) Inferotemporal 34 (32) Superonasal 2 (2) Inferonasal 0 (0)
Order of affected crossing First order 9 (8) Second order 55 (52) Third order 42 (40)
00 = right eye; as = left eye; BRVO = branch retinal vein occlusion.
425
Ophthalmology Volume 100, Number 3, March 1993
Table 3. Relative Anatomic Position of Artery and Vein at Occluded and Control Crossings
No. of Control Group Patients
withBRVO 1 2 3
No. with artery anterior to vein (%) 105/106 (99) 65/105 (62*) 51/83 (61*) 46/85 (54*)
BRVO = branch retinal vein occlusion.
* Patients with BRVO versus each control group (P < 0.(01). Differences among control groups were not significant (P > 0.30).
with BRVO, and (3) an eye of an age-sex-race-matched patient without BR YO. The artery was located anterior to the vein less than 65% of the time in each set of control crossings, a finding consistent with both Jensen's9 and Duker and Brown's5 reports that the vein is superficial to the artery in approximately 30% of normal arteriovenous crossings. The difference in findings for obstructed and each set of control crossings was highly significant in our study. Finding a similar relationship for comparisons involving three different sets of controls strengthens the validity of our observation.
Since arteriovenous crossings are involved in such a high proportion of BVROs, a greater number of arteriovenous crossings might theoretically increase the risk of occlusion. Indeed, we found evidence that arteriovenous crossings were more common in patients with BRVO than persons without BR YO. That suggests that a higher number of arteriovenous crossings may increase the risk of BRVO. The average number of crossings was greater in each quadrant for fellow eyes ofBRVO patients compared with eyes of persons without BR YO, but a statistically
significant difference was found only for the inferotemporal quadrant (P < 0.05).
Finding the vein to be consistently between the more rigid artery and the highly cellular retina at almost all arteriovenous crossings affected by BR VO suggests an important role for mechanical obstruction in the pathogenesis of BR VO. However, other factors also must play a role, because in approximately 60% of normal arteriovenous crossings the artery lies anterior to the vein, and relatively few of these crossings are affected by BR VO. Systemic hypertension, diabetes mellitus, and atherosclerosis are reportedly more common in patients with BR VO. 10 Arteriolar sclerosis, which is associated with these systemic vascular conditions, may result in a further compromise of the lumen of the vein, when increased rigidity of the wall of the crossing artery and contraction of the adventitial sheath shared by artery and vein occurs. Mechanical compromise of the vein's lumen may result in turbulent blood flow producing intimal damage, and the sequence of events leading to occlusion of the vein.
Like others,1O we found that most occlusions (98%)
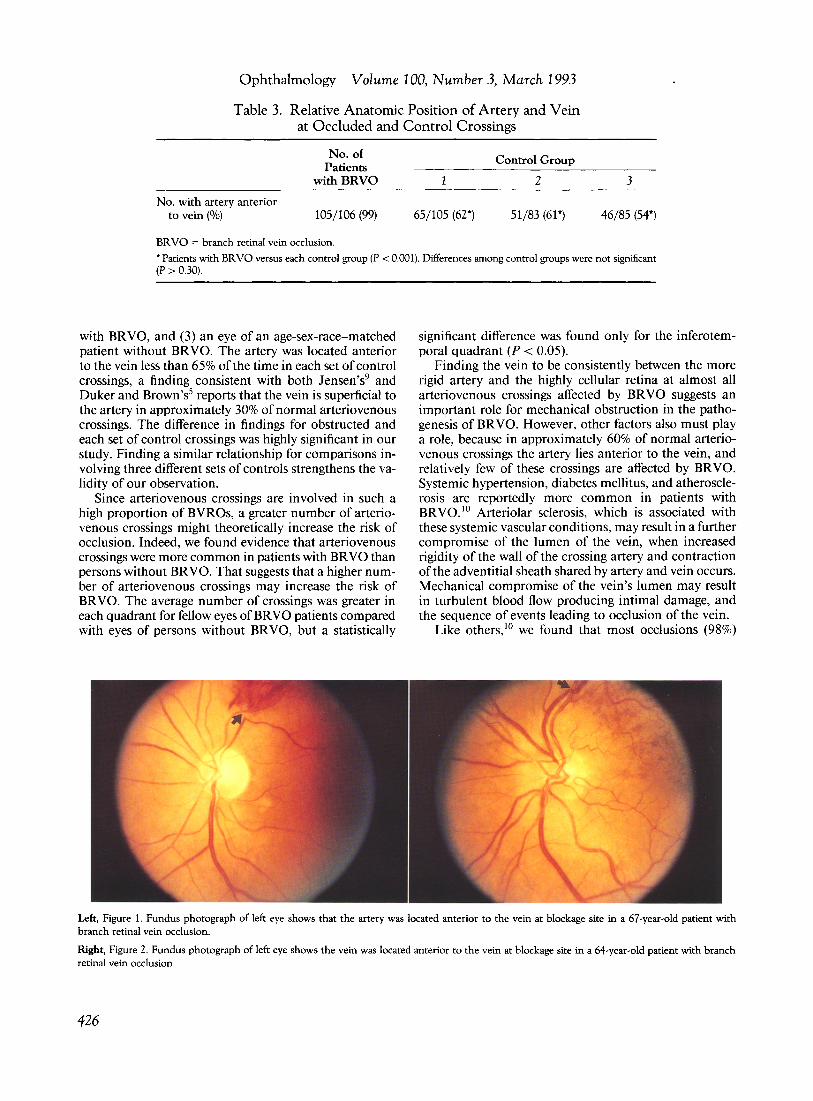
Left, Figure 1. Fundus photograph of left eye shows that the artery was located anterior to the vein at blockage site in a 67-year-old patient with branch retinal vein occlusion.
Right, Figure 2. Fundus photograph of left eye shows the vein was located anterior to the vein at blockage site in a 64-year-old patient with branch retinal vein occlusion.
426
Zhao et al . Arteriovenous Crossing Patterns
Table 4. The Number of Arteriovenous Crossings and the Relative Anatomic Position of Artery and Vein in Fellow Eyes of Ninety-nine Patients with Branch Retinal Vein Occlusion and Eyes
of Matched Persons without Branch Retinal Vein Occlusion
Superotemporal Inferotemporal Superonasal Inferonasal Total
Fellow Eyes of BRVO Patients No. of A V crossings 170 140 144 137 591 Average no. of AV crossings 1.7 1.4 1.5 1.4 6.0' No. with artery anterior to
vein(%) 106 (62) 84 (60) 80 (56) 96 (70) 366 (62) Eyes of Patients without BRVO
No. of A V crossings 161 109 135 125 530 Average no. of AV crossings 1.6 1.1 1.4 1.3 5.4" No. with artery anterior to
BR VO = branch retinal vein occlusion; A V = arteriovenous .
• Average number of AV crossings was significantly different in eyes of patients without BRVO than in fellow eyes of patients with BRVO (P < 0.02).
were on the temporal side of the retina, and 66% were noted in the superotemporal quadrant alone. One possible explanation for this finding is that patients with superotemporal occlusions may be more likely to be seen by physicians than patients with occlusions in other quadrants because superotemporal occlusions are more likely to affect vision. It also has been suggested that perhaps there is a larger number of crossings in the superotemporal quadrant, increasing the risk of occlusion in that quadrant.1O Jensen9 found that in normal eyes most of the vessel crossings are found in the upper temporal quadrant of the fundus. We found more arteriovenous crossings in the superotemporal quadrant than in the other three quadrants, but the difference was statistically significant only for two comparisons, the superotemporaljinferotemporal and superotemporaljinferonasal comparisons in eyes of persons without BRYO. Our comparison of the number of crossings between quadrants and between eyes must be interpreted with caution, because we only counted the number of crossings in single standard, 30° fields centered on the optic disc. We cannot be certain whether examination of a larger area of the retina would have yielded different results.
One final possibility that might explain the increased frequency of occlusion on the temporal side is that the artery-vein relationship may differ in different quadrants. Michaelson 11 has postulated three kinds of relationship for crossing arteries and veins: (1) at some arteriovenous crossings, the vessels are not in intimate contact with each other; (2) at some crossings, the vessels are in contact over a smaller or larger part of their surface, but each has its individual wall and there is no apparent fusion; and (3) at some crossings, the adventitia of the vein is continuous with that of the artery, the contribution of the vein to the common wall being little more than a layer of endothelium. Different relationships for the crossing vessels in
different quadrants might explain differences in susceptibility to occlusion. Histopathologic studies are needed to evaluate this hypothesis.
Appendix
The Eye Disease Case-Control Study Group Participating Centers
Manhattan Eye, Ear and Throat Hospital, New York, NY: Principal Investigator, Lawrence A. Yannuzzi, MD, Co-Investigator, John A. Sorenson, MD; Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, MA: Principal Investigator, Johanna M. Seddon, MD, Co-Investigators, Evangelos S. Gragoudas, MD, Carmen A. Puliafito, MD; Medical College of Wisconsin, Milwaukee, WI: Principal Investigator, Thomas C. Burton, MD; The University of Illinois at Chicago, Chicago, IL: Principal Investigators, Marilyn D. Farber, DrPh, Norman Blair, MD, Co-Investigators, Thomas Stelmack, 00, Alan Axelrod, MD; The Wilmer Ophthalmologic Institute at Johns Hopkins University Hospital, Baltimore, MD: Principal Investigator, Julia Haller, MD, Co-Investigators, Sharon Pusin, MD, Gary Cassel, MD; National Eye Institute, Bethesda, MD: Study Co-Chairmen, Daniel Seigel, ScD, Robert D. Sperduto, MD, DirectorojDataAnalysis, Rita Hiller, MS, Project Officer, Richard Mowery, PhD, Co-Investigators, Emily Chew, MD, Ashlesha Tamboli, MD; Nutritional Biochemistry Branch, Division of Environmental Health Laboratory Sciences, Center for Environmental Health and Hygiene Control, Centers for Disease Control, Atlanta, GA: Principal Investigator, Dayton T. Miller, PhD, Co-Investigators, Anne L. Sowell, PhD, Elaine W. Gunter, BS; Coordinating Center, Orkand Corporation, Silver Spring, MD: Director, Marsha Dunn, MPH.
427
Ophthalmology Volume 100, Number 3, March 1993
References
I. Gass JDM. A fluorescein angiographic study of macular dysfunction secondary to retinal vascular disease. II. Retinal vein obstruction. Arch Ophthalmol 1968;80:550-68.
2. Patz A, Yassur Y, Fine SL, et al. Branch retinal venous occlusion. Trans Am Acad Ophthalmol Otolaryngol 1977;83:0P373-8.
3. Frangieh GT, Green WR, Barraquer-Somers E, Finkelstein D. Histopathologic study of nine branch retinal vein occlusions. Arch Ophthalmol 1982; I 00: 1132-40.
4. Seitz R. The Retinal Vessels: Comparative Ophthalmoscopic and Histologic Studies on Healthy and Diseased Eyes. St. Louis: CV Mosby, 1964;28.
5. Duker JS, Brown GC Anterior location of the crossing artery in branch retinal vein obstruction. Arch Ophthalmol 1989; I 07:998-1 000.
428
6. The Eye Disease Case-Control Study Group. Risk factors for neovascular age-related macular degeneration. Arch Ophthalmol 1992; 110: 170 1-8.
7. Diabetic Retinopathy Study Research Group. Report 7. A modification of the Airlie House classification of diabetic retinopathy. Invest Ophthalmol Vis Sci 1981 ;21 :210-26.
8. Miller R. Multiple comparisons. In: Kotz S, Johnson NL. Encyclopedia of Statistical Sciences. Vol. 5: Lindeberg Condition to Multitrait-Multimethod Matrices. New York: John Wiley & Sons, 1985;679-89.
9. Jensen VA. Studies on the branchings of the retinal bloodvessels. Acta Ophthalmol 1936;14:100-9.