47
Articulators PRESENTED BY: SEHAR HANIF MARIAM MAHMOOD
| Date post: | 22-Oct-2014 |
| Category: |
Documents |
| Upload: | hamadkayani774954 |
| View: | 399 times |
| Download: | 5 times |
Articulators
PRESENTED BY: SEHAR HANIF MARIAM MAHMOOD
Introduction
Definition An articulator is a mechanical device that
represents the TMJ and jaws, to which maxillary and mandibular casts may be attached to simulate some or all mandibular movements.
They are used to study the functional and para functional contact relations between teeth, arrangement of artificial teeth and development of occlusal surfaces of cast fixed restorations
There are two basic forms of Articulators.
1. Simple forms 2. Complex forms
Simple Forms of Articulators The simplest forms consists of two
arms or bows united by a hinge. These enable and accurate record
of a single static relationship between the jaws.
The only movement which can be made is an opening and closing one about the hinge.
Complex Forms These are able to assume
relationship other than single static relationship.
These articulators vary considerably in their capacity to simulate jaw movements and relationships.
History of Articulators1805 Gariot Develop a hinge articulator made of the metal.1840 Evans Develop the first anatomical articulator.1854 Bonwill Propose a Bonwill's triangle.1859 Bonwill Propose a Three points contact occlusion.1859 Bonwill Develop the anatomical articulator which becomes the
archetype of the condylor articulator.1866 Balkwill Propose a Balkwill angle.
1890 Spee Propose the theory of the Spee's curve.1896 Walker Develop the first adjustment Articulator of the arcon
type.1901 Christensen Release a Christensen phenomenon. Develop a
check bite technique at the same time.
1908 Gysi Develop Adaptable Articulator which is the first Articulator for Gysi. An incisal guide table can adjust it by installing an exclusive adapter.
1914 Schroder,RumpelDevelop a Schroder-Rumpel Articulator. A clutch is stuck to the joint part of the Adaptable articulator of Gysi, and it learns to fix a centric occlusion.
1919 WadsWorth Develop the Articulator of WadsWorth that the general idea of the lateral incisal guide table which split in two was adopted in the Articulator.
1921 McCollm Develop how to measure a Hinge axis.
1926 McCollm,StallardEstablish California Gnathological Sociaty.
1934 McCollm Develop the Gnathoscope Articulator.
1944 Beyron Develop the Dntatus Articulator.
1950 Thomas Release the Cusp fossa waxing (wax corn technique) and Tripodism which aimed at giving it an Organic occlusion.
1950 Thomas Release the Cusp fossa waxing (wax corn technique) and Tripodism which aimed at giving it an Organic occlusion.
1958 Hanau Develop a Hanau H2-O Articulator. 1961 Lucia Propose that a wrong point arises in the convalescence of the Orel rehabilitation.
1962 Posselt Publish the figure (Posselt's banana) which the limit movement way of the lower incisal tooth was drawn in three-dimensionally.
1968 Swanson,Wiph Develop a TMJ Articulator.
1968 Granger Develop a Simulator Articulator.
1970 Mitsuya,Yamasita Develop a Cosmax Articulator.
1974 Guichet Develop a Denar D5A Articulator.
1975 Guichet Develop a Denar ・ Mark II Articulator.
1976 Broadrick Develop an Occlusal plane analyzer
Classification of dental Articulators
Simple hinge or plane-line articulators
Average value articulators Adjustable articulators a. Semi-adjustable 1. Arcon type 2. Non-Arcon
type b. Fully-adjustable
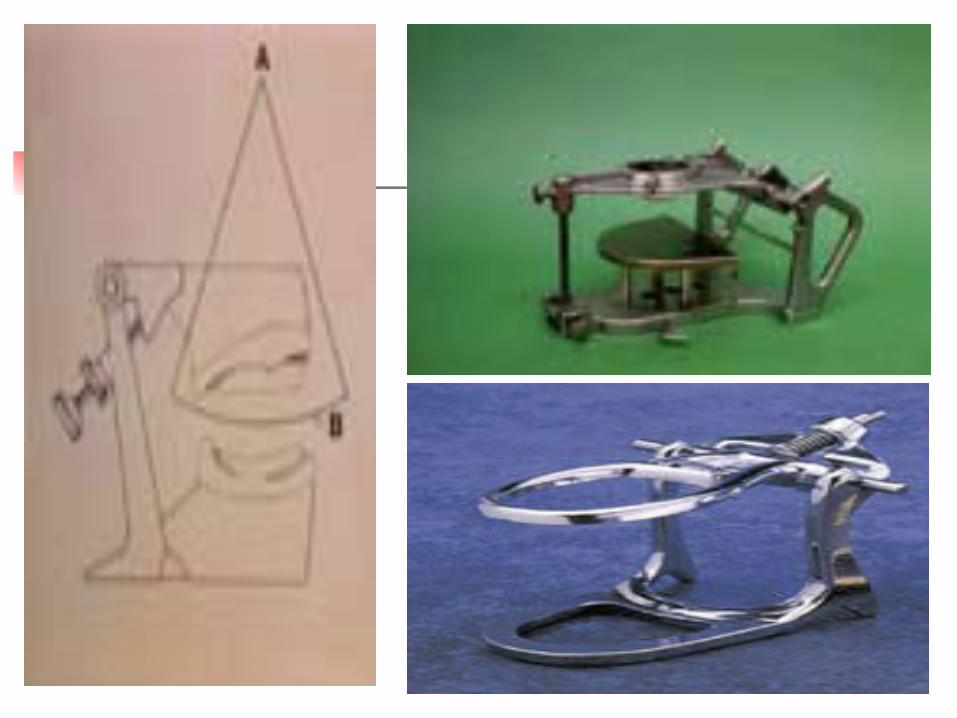
Plane Line Articulators History:- in 1805 Gariot invented the
simple hinge articulator made of metal plates.
Definition This simple articulator holds the
casts in a prescribed relationship using the ICP, and allows separation and approximation of the casts.
The hinge is in no way related to the hinge axis of mandible . There is no attempt to reproduce mandibular movements.
Uses It is possible to produce even occlusal
contact only in the static jaw relation. It is used in circumstances where the
occlusion is to be restored to an existing stable ICP and where the excursive guidance of the remaining natural teeth will ensure separation of those teeth replaced by the partial dentures.
Shortcomings of Plane Line Articulators Tilting of dentures Cuspal interference Reduced efficiency Pain
Average value Articulators Articulators of these type have their
origin in the work of Monson, Bonwill and Gysi who recorded measurements from anatomical specimens and clinical subjects in order to develop articulators whose dimensions reflected those anatomical features which influence mandibular movements.
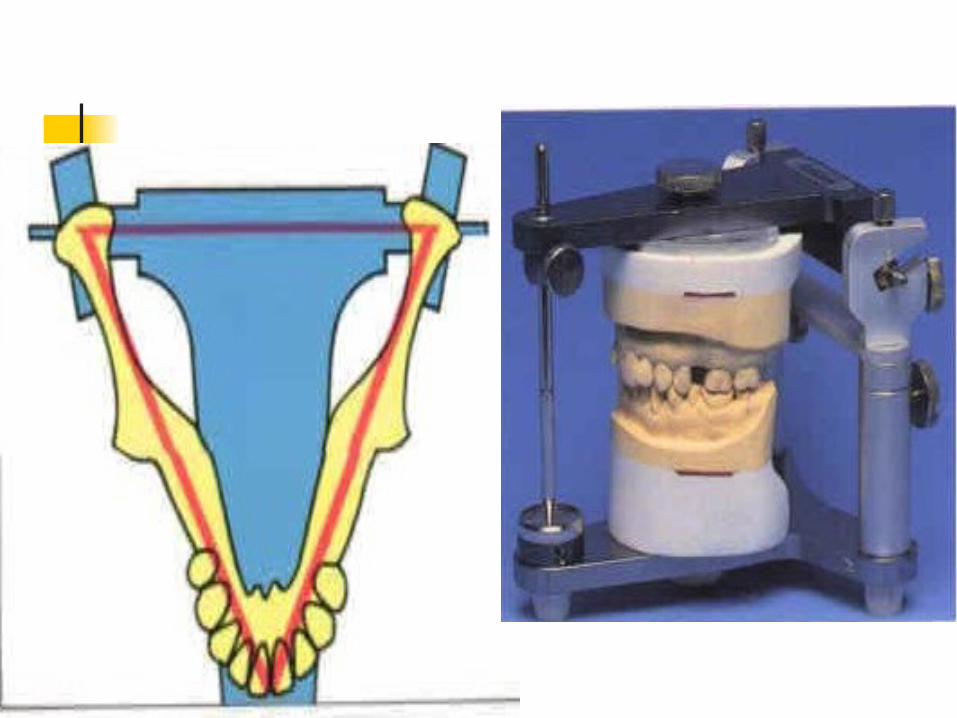
Average Measurements The dimensions of these articulators
reflect the average measurement recorded by Bonwill of 10cm between the central points of mandibular condyles and the midpoint of the incisal edges of lower anterior teeth.
These dimensions form an equilateral triangle known as Bonwill triangle.
These also incorporate the condylar path representing the average sagittal condylar guidance angle of approx. 30
Adjustable Articulators These attempt to reproduce jaw
movement of each patient’s jaw, by trying to reproduce the anatomy of the jaw joints and related structures.
They can be called “Moving-condyle articulators”.
Advantages of Adjustable Articulators Balanced occlusion Stability Reduced trauma Functional movements Efficiency Saving time
Balanced Articulation
Definition:- an arrangement of the teeth so
that in any jaw relationship as many teeth as possible are in occlusion, and when changing from one position to another they move with a smooth, sliding motion, free from cuspal interference and maintaining even contact.
Factors for Balanced Articulation Articulators which would copy the
anatomical jaw movements. Means by which these relationships are
measured and transferred to articulators. Understanding of the factors which
influence arrangement of the anterior and posterior teeth to produce balance.
Posterior teeth with cusp angles which will permit them to be set in balanced articulation.
Types Of Adjustable Articulators There are two types: a) Semi-adjustable
articulators 1. Arcon type 2. Non-arcon type b) Fully adjustable
articulators
Semi-adjustable articulators
These articulators are adjustable to conform to those anatomical features, such as incisal guidance and condylar guidance which influence those movements.
They take into account the bodily shift of the mandible (Bennette movement) during lateral excursions.
Advantages of Semi-adjustable articulators These are less complicated than
adjustable articulators Greater functional efficacy than
plane-line articulators. More conveniently accepts the
arbitrary face-bow records and interocclusal records.
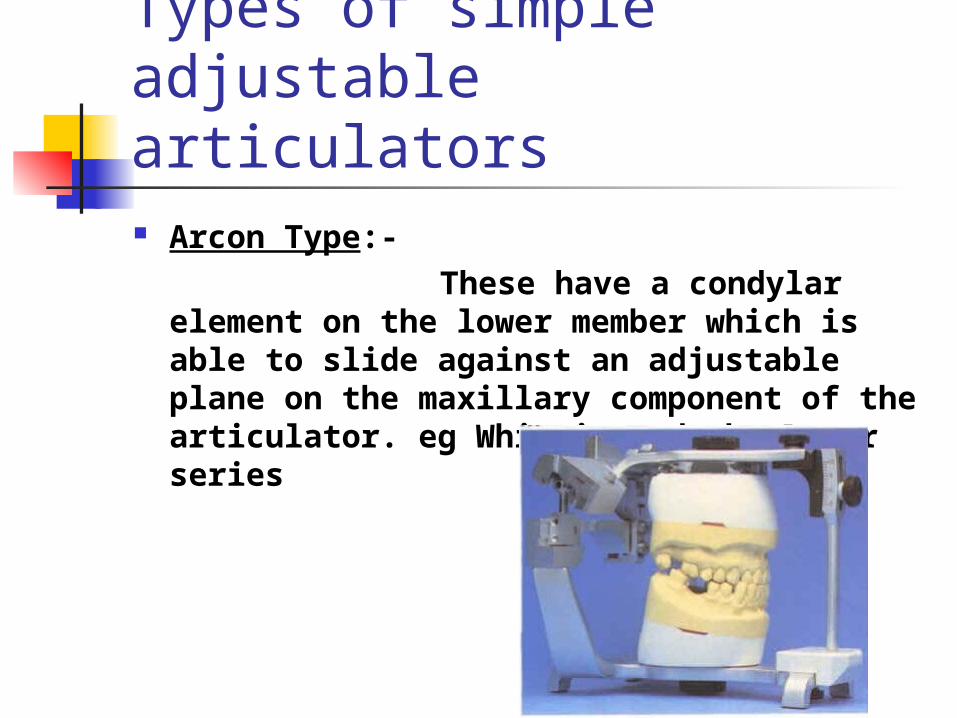
Types of simple adjustable articulators Arcon Type:- These have a condylar element
on the lower member which is able to slide against an adjustable plane on the maxillary component of the articulator. eg Whipmix and the Denar series
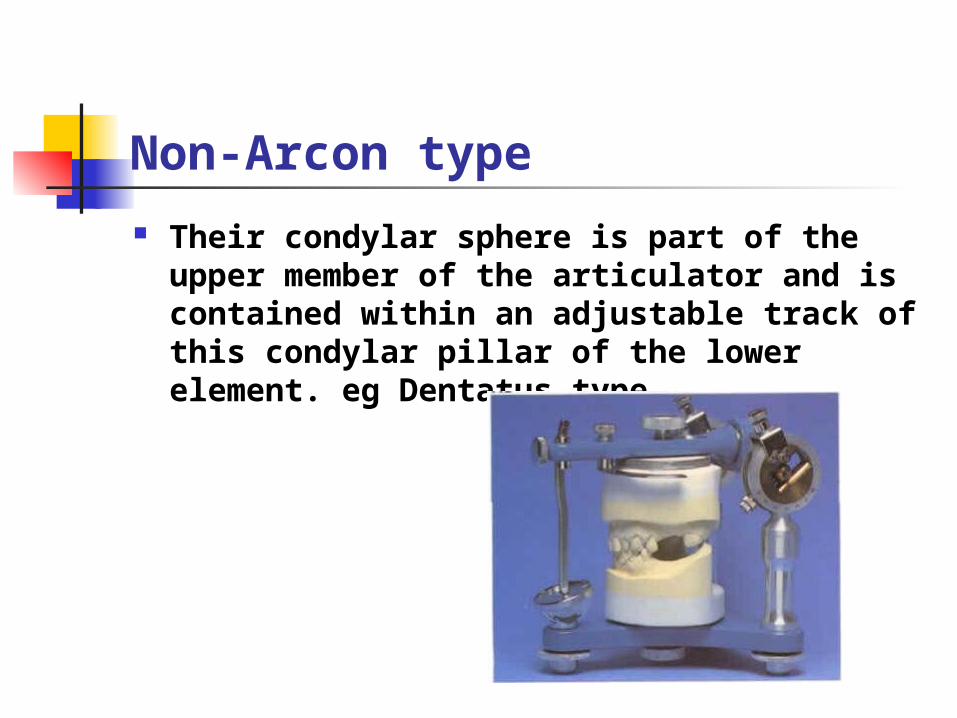
Non-Arcon type
Their condylar sphere is part of the upper member of the articulator and is contained within an adjustable track of this condylar pillar of the lower element. eg Dentatus type
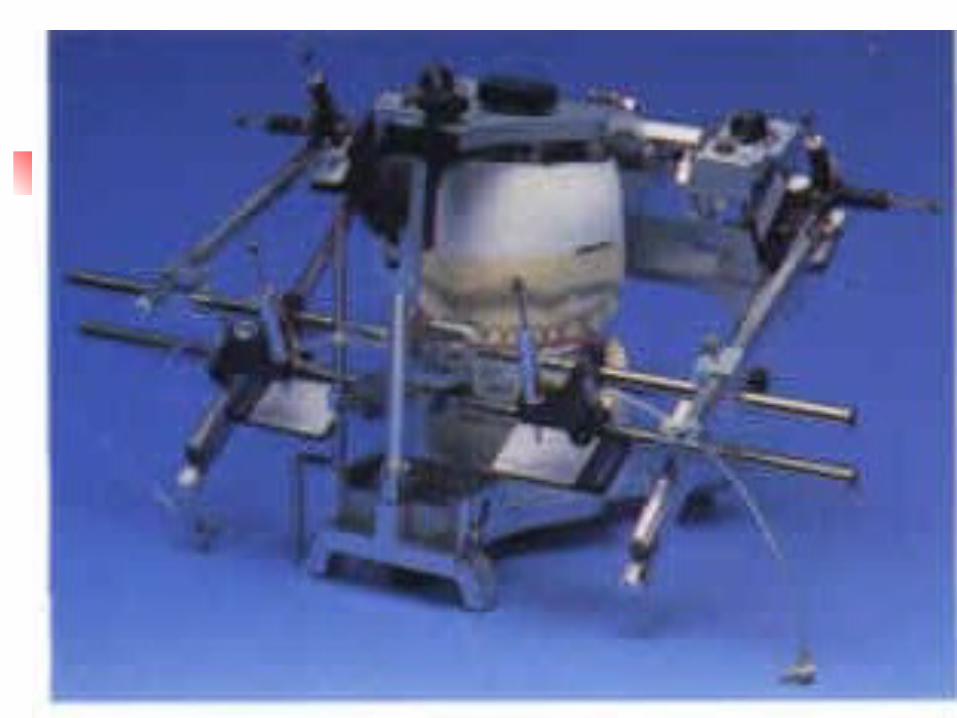
Fully Adjustable articulators These are sophisticated articulators with
a more comprehensive system of adjustment which gives them the potential for increased accuracy in the reproduction of mandibular movements.
Various methods have been devised for programming these instruments. eg obtaining traces of mandibular movements in 3 planes and then transfer these records to articulator.
Disadvantages These require high degree of skill.
ie clinical and technical skill. Clinical procedure is time
consuming.
Face-Bow registration Definition:- it is a caliper like device
which is used to record the relationship between the intercondylar axis and either the maxillary or the mandibular arch.
Types of Face-bows
1. Simple face-bows 2. Hinge axis face-bows
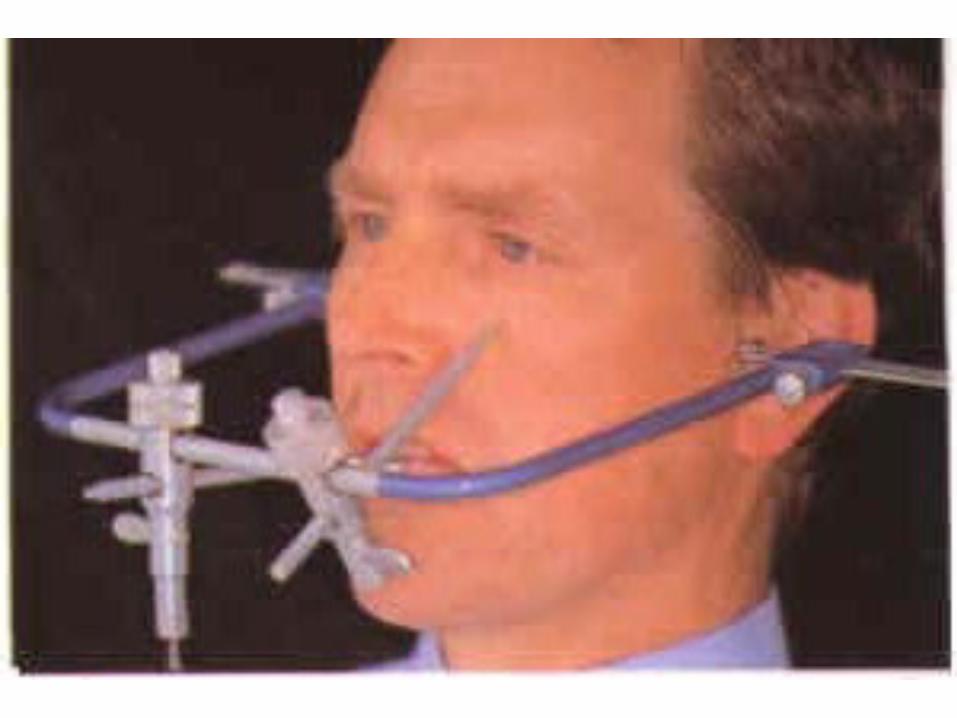
Simple face-bows Definition:- These face-bows
consist of a U-shaped body having calibrated adjustable condyle indicators at each side. The body of the face-bow carries a joint for securing a fork having an off-set rod attached, and another for an orbital pointer.
How to use a Simple face-bow
Condyle Indicators:- The lateral poles of the condyle are
located by a combination of estimation of their position and palpation.
The average anatomical position of the condyle is some 12mm from the posterior of the tragus of the ear along an imaginary line joining the upper border of the external auditory meatus and outer canthus of the eye.
After determining this point the ball of the finger is placed over it and the patient is asked to make small mouth opening and closing movements. When movements of the tissues overlying the lateral pole of the condyle will be appreciated.
The site as determined should be marked on the skin of the face using a small self adhesive paper marker or china graph pencil. Both condyles should be located.
Fork:- The fork of the face bow is attached to upper
occlusal rim or where the natural teeth are present in the upper jaw, to a wax record of occlusal and the incisal surface of the teeth.
The occlusal rim or wax record are placed in position in the mouth leaving the rod of the fork protruding from the mouth.
All joints on the body of the face-bow are loosened and the joint of the face-bow fork is slipped into position.
Recording:- The condylar guidances are placed in
contact with the previously recorded marks.
Centering of the face-bow is carried out by ensuring that the condyle indicators show equal graduations while maintaining contact with the skin markers.
Fork joint is then tightened.
Use of an orbital pointer:- The patient is instructed to close the
eye while the tip of the pointer is carried towards the lowest part of the orbit.
The joint on the body of the orbital pointer is tightened.
After slackening of the condyle indicators the face-bow, together with the upper occlusal rim or wax template is removed from the patient.
Mounting the models on Articulators The condyle markers are placed in position of
on joint mechanism of articulator. Provisions for face-bow transfer are made on
average value and adjustable articulators. Condyle indicators are then centred so that
equal graduations appear on both sides. Orbital indicator is made to contact the
appropriate site near the top of articulator. This fixes the horizontal plane of records. The cast is luted to the upper bow of
articulator.
The upper cast is now attached to the upper bow in the same relationship to the hinge of the articulator as the maxilla of the patient bears to the intercondylar axis.
The lower cast can then be attached to the lower bow of the articulator by means of record of retruded jaw relationship.

Hinge-axis face-bow This instrument was introduced by
McCollum in 1930 and is used to determine the centre of rotation or hinge axis of the condyles.
Many complex variations of this instrument exists. It is not commonly used for removable denture prosthetics as the simple face-bow. The validity of the hinge-axis concept is considered to be controversial.
Criteria for selection of an Articulator The articulator should be rigid and maintain all
centric and eccentric positions. It should accept an arbitrary face-bow records. It should have an incisal guidance table. It should have an adjustable condylar
inclination and be able to accept a protrusive record.
It should have an adjustable Bennet’s angle and have Bennet movement programmed into it; Hanau suggested a formula to set the Bennet angle on Hanau articulator.
Bennet angle=condylar inclination/8+12
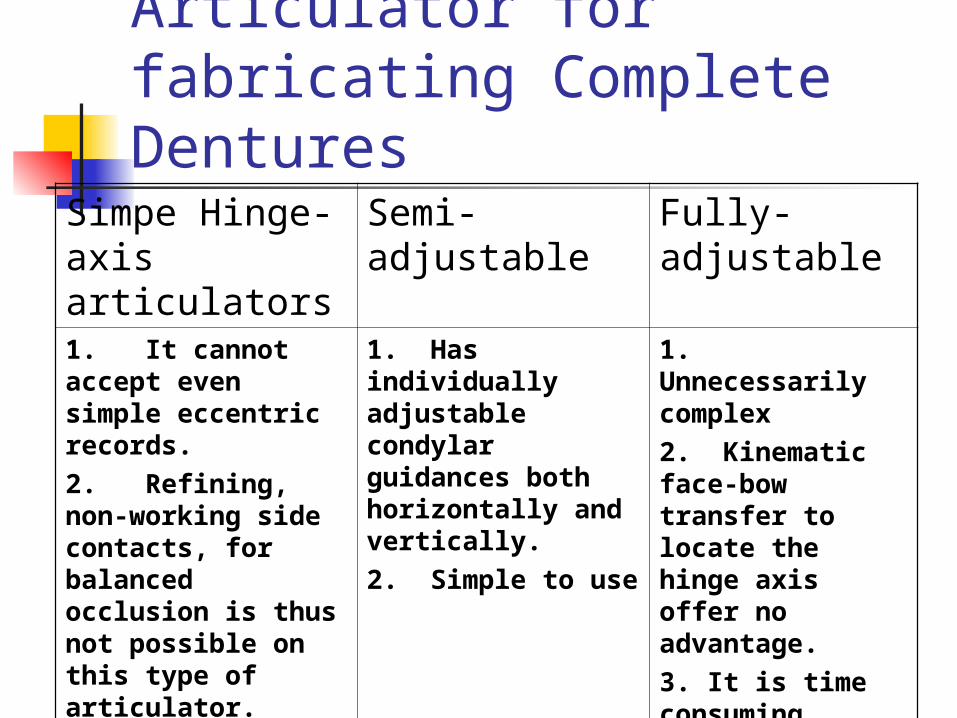
Selection of Articulator for fabricating Complete Dentures
Simpe Hinge-axis articulators
Semi-adjustable
Fully-adjustable
1. It cannot accept even simple eccentric records.2. Refining, non-working side contacts, for balanced occlusion is thus not possible on this type of articulator.
1. Has individually adjustable condylar guidances both horizontally and vertically.2. Simple to use
1. Unnecessarily complex2. Kinematic face-bow transfer to locate the hinge axis offer no advantage.3. It is time consuming4. greater clinical skills











![KaVo Price list Articulators. - MEDIPRO | Medipro ... Catalogue...PROTAR®evo Articulators Mat.-No. Price [€] Articulator PROTAR®evo 7 1.002.3320 1.211,-adjustable are HCI, bennett](https://static.documents.pub/doc/80x56/5af148bf7f8b9abc788e3d2d/kavo-price-list-articulators-medipro-medipro-catalogueprotarevo-articulators.jpg)





