33
SHAILESH KUMAR SAHU ARTIFICIAL BLOOD
| Date post: | 07-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | shadab-kamal |
| View: | 64 times |
| Download: | 0 times |

SHAILESH KUMAR SAHU
ARTIFICIAL BLOOD
Artificial Blood
Artificial blood or blood surrogate is a substance used to mimic and fulfil some functions of biological blood,usually in the oxygen carrying sense.
Main aim is to provide an alternative to blood transfusion,which is transferring blood or blood based products from one person to another.
It does not contain plasma,RBCs or WBCs.

The History of Artificial Blood
Milk was one of the first substances used as a blood substitute in order to treat patients with Asiatic cholera.
After several patients died by receiving milk transfusions, other substances were discovered as potentials :• Salt or saline solutions: used primarily as a plasma volume expander,
rather than as artificial blood• Hemoglobin isolated from red blood cells• Animal plasma could be used as a substitute for human blood.However,
since many of the materials in animal plasma are toxic to humans, this posed a problem to using it as a substitute
The problem of not having a workable substitute led to Ringer’s Solution…

Why artificial blood?
Increasing demandDecreasing supplySafety Infectious disease transmission Transfusion reactions ImmunosuppressionCost

Ideal Characteristics of Artificial Blood
Safe to useCompatible in the human bodyAble to transport and release oxygen where
neededStorable and durable for longer time periods free of pathogens and toxins Viscosity similar to bloodLow cost

Blood Substitute
O2 Carriers
Lack coagulation
Immune functionNutrition
Plasma protiens
HB Solutions PFC

Perfluorocarbons
These are chemically and biologically inert,water insoluble,synthetic aromatic or aliphatic compounds with F substituted for all H atoms of hydrocarbon.
water insoluble:so used as emulsion with Puronic-68,egg yolk phospholipids and triglycerides as emulsifying agent.
They achieve O2 delivery by using organic chemicals with high gas solubility.
The O2 carrying capacity of PFCs is linearly related to PO2 and obeys Henry’s law.

Short half life(2-4hr):eliminated from body unmetabolised through the lungs.
Process of production: Water, salts, and phospholipids
surfactant,antibiotics,vitamins,nutrients are added and emulsified through high-pressure homogenization
Purified through high temperatures of steam. Common PFCs:Perfluorodecalin Perfluorooctyl bromide(oxygent)

Perfluorocarbons (PFC) emulsionsStructure:
Perfluorocarbon core Surrounded by a phospholipid surfactant that reduces the surface tension of the liquid in which it is dissolved.

PFC
Synthetic organic liquid compounds
8-10 carbon atomsH+ atoms Halogens
!st GenerationFluosol 20%
•Stored Frozen•Limited O2 carrying capacity.Allergic reaction
!st GenerationFluosol 20%
•Stored Frozen•Limited O2 carrying capacity.Allergic reaction
2nd GenerationOxygent 90%
•Stored at 4’c•High O2 Carrynig capacity
2nd GenerationOxygent 90%
•Stored at 4’c•High O2 Carrynig capacity
First generation perfluorocarbon
FLUOSOL-DA20%-It consists of two PFCs, perfluorodecalin (PFD) and perfluorotrypropylamine (FTPA) and Pluronic F-68, as an emulsifying agent, and is able to maintain a balance between the oxygen carrying capacity and tissue retention.
It can deliver 0.4ml oxygen per 100ml.

Second generation perfluorocarbon
large oxygen dissolving capacityFaster excretion (4 days) and less tissue retentionLack of significant side effectse.g Perfluorooctyl bromide(Oxygent) Bisperfluorobutyl ethyleneOxygent can deliver upto 1.3 ml oxygen per 100 ml.

Advantages of Perfluorocarbons (PFC) emulsions
do not react with oxygen allow easy transportation of the oxygen to the body allow increased solubility of oxygen in plasma minimize the effects of factors like pH and temperature in blood
circulation

Disadvantages
causes flu-like symptomsunable to remain mixed as aqueous solutions –thus, must be prepared
as emulsions.a decrease in blood platelet count.PFC products cannot be used by the human body, and must be
discarded.this takes approximately 18-24 months.because PFCs absorb oxygen passively, patients must breathe at a
linear rate to ensure oxygenation of tissues.Require high FiO2

Adverse EffectsOf PFC
AllergyEspecially 1st Gen
Bleeding TendencyDecrease Plt Count
Increase Liver
Enzymes
•Acute Rt sided heart Failure •Pulmonary edema
•Early: Headache
•Late: Flu like symptoms

Hemoglobin-based Oxygen Carriers (HBOCs)
Hemoglobin-based Oxygen Carriers were created as a mechanism to mimic the oxygen-carrying role of hemoglobin in the body, while still reducing the need for real human hemoglobin. Hemoglobin:a tetramer with two alpha and two beta polypeptide
chains; each is bound to an iron heme group which successively binds to an oxygen molecule.it has a higher affinity for oxygen, thus making it an excellent source of blood substitutes.

HBTetramer
Monomers Dimers
1. Filtered by the kidney2.NO scavenger3.Increase plasma osmotic
pressure4.High O2 affinity
1. Ultrastructural modification
2. Artificial Blood Cells
HB Solutions

To avoid such spontaneous dissociation native Hb is modified by intramolecular cross-linking between alpha and beta Chains, polymerization, pyridoxylation, or conjugation to larger molecules, such as albumin or polyethyleneglycol ("pegylation"),encapsulation of hemoglobin into a liposome or polymer structure.

Cross linking(diaspirin)
Conjugation(Albumin,PEG)
Polymerization
Microspheres(Dendrimer,Polym
ersome)
Recombinant DNA
technology
Monomers and Dimers
1. Ultrastructural modification
Tetramers
Ultra purification

2. Artificial Blood Cells
Liposomes=
Pseudoerythrocyte
Nanocapsules
Encapsulated Hb in cell like structure
Coated withPhospholipid Bilayer and Cholesterol
Coated withPolylactide

PRODUCTION OF HBOCs
Synthetically produced Hb:E.coli(P678-54)
Isolated Hb:human or animal blood(bovine blood)

Current Hb-based oxygen carriers


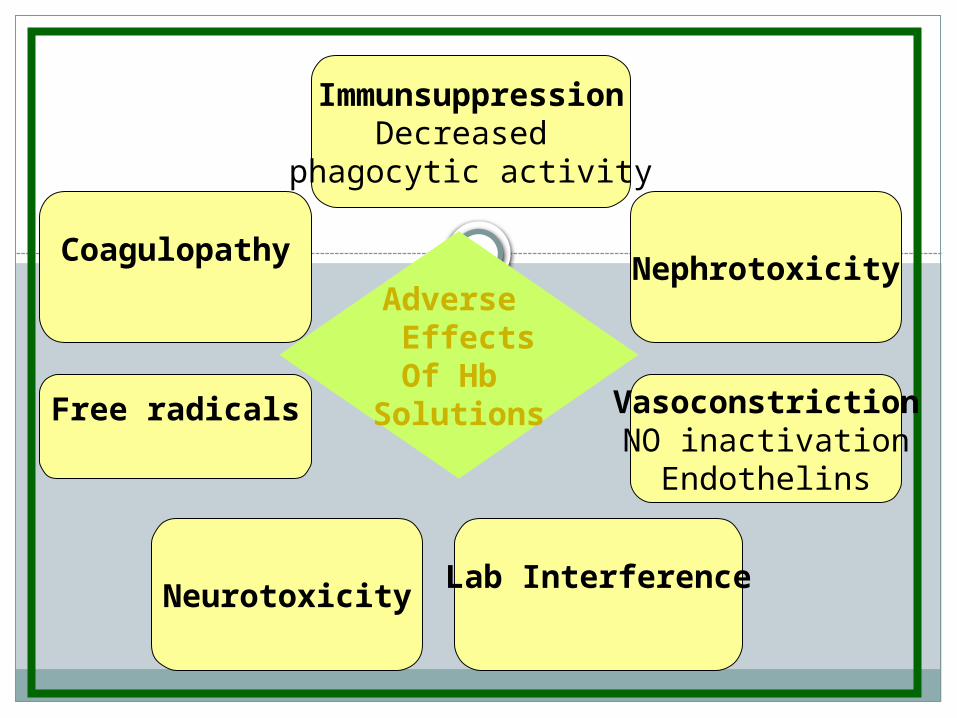
Adverse EffectsOf Hb
Solutions
ImmunsuppressionDecreased
phagocytic activity
NephrotoxicityCoagulopathy
Free radicals VasoconstrictionNO inactivation
Endothelins
NeurotoxicityLab Interference

AdvantagesAvailable in much larger quantitiesCan be stored for long durations.Can be administered rapidly without typing or cross-matching Can be sterilized via pasteurization
Disadvantagesreduced circulation half-lifedisrupts certain physiological structures, especially the
gastrointestinal tract.the release of free radicals into the body


1. Higher O2 Solubility Coefficient.
2. V. low viscosity
3. High Density
4. High N2 Solubility
5. Inactivate NO
• Resuscitation•Periop hemodilution•Organ preservation
•Sickle crisis
•Alveolar recruitment•Liquid ventilation•Decompression sickness
•Septic shock

Potential clinical applications
1. Therapeutic(a) Blood substitutes : hemorrhagic shock; hemorrhage (war,surgery); anaemia.(b) Whole-body rinse out : acute drug intoxication; acute hepaticfailure.(c) Local ischemia : acute MI; evolving MI; cardiac failure; braininfarction; acute arterial thrombosis and embolism; PTCA ofcoronary artery.(d) General ischemia : CO intoxication.
(e) Aid for organ recovery : acute renal failure; acute hepatic failure;acute pancreatitis.
(f) Adjuvant therapy : radiotherapy; chemotherapy2. Perfusional protection of organs during surgery –
cardiopulmonary bypass3. Preservation of donor organ.4. Drug carrier - drug-conjugated haemoglobin and
perfluorochemicals.5. Contrast agent - (Perfluoro-octylbromide)

Non-Clinical Applications1. Culture medium2. Chemical examination - oxygen sensor; standard
solution for oxygen calibrator3. BioreactorParadoxical Utilisations (of high-oxygen affinity)1. Oxygen absorbent2. Oxygen pulse therapy for malignant tumour in
combination with radiotherapy or chemotherapy.

Conclusion
Artificial blood is a good tool for the survival of patients at the time of surgery when blood loss is higher.
It carries oxygen to tissues and can support life temporarily until patients can either regenerate their own red cells or can be transfused with banked blood.
It can be sterilised against infectious diseases.In short term,the prospective benefits of artificial blood
overshadow the shortcomings.
THANK YOU

![Soft Artificial Life, Artificial Agents and Artificial ... Life-springer... · Soft Artificial Life, Artificial Agents and Artificial ... Introduction Artificial ... Stillings [22]](https://static.documents.pub/doc/80x56/5b0b2db47f8b9ae61b8d59e8/soft-artificial-life-artificial-agents-and-artificial-life-springersoft.jpg)















