20
Asbestos Exposure Frans Naude

Asbestos Exposure
Frans Naude

Pneumoconioses
Fibrotic
Silicosis,coal workerpneumoconiosis, asbestosis, berylliosis, talcosis
Non fibrotic
SiderosisStannosisbaritosis

Asbestos Exposure
• Inhalation of asbestos fibers
Pleural Pulmonary Extra thoracic
Pleural plaque
Diffuse pleural thickening
Pleural effusions
Malignant mesothelioma
Fibrosis (asbestosis)
Bronchial carcinoma
(usually in lower zones)
Round atelectasis (pseudo tumor)
Peritoneal mesothelioma
Other extra thoracic malignancies

• Asbestosis– Def : diffuse interstitial pulmonary fibrosis that
occurs secondary to the inhalation of asbestos fibers

Diagnostic imaging chest I 2-38
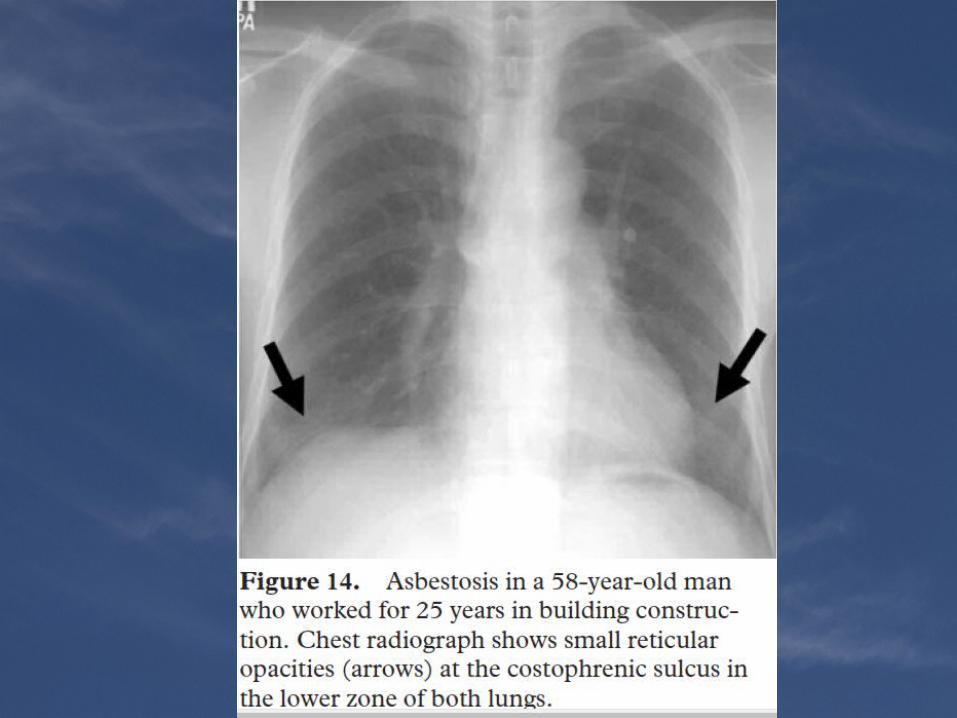

Radiography
• May be normal (10-20%)• Peripheral lower zone predominance
– Irregular reticular or small nodular opacities– "Shaggy" cardiac silhouette in advanced disease
• Late: Endstage honeycombing• Pleural plaques (25%)• Lung cancer: Lower zone predominance in contrast to the upper zone predominance in the general population of smokers
• Progressive massive fibrosis extremely rare

Small subpleural nodules (straight arrows),Patchy ground-glass opacities (curved arrows), Interlobular septal thickening (arrowhead) suggestive of early-stage asbestosis.

Pleural plaque : band like pleural thickening (arrowheads) in the lower lobe of both lungs

Asbestosis : subpleural consolidation (arrow) in the lower lobe of the left lung, with reticulation, ground-glass
opacities, and honeycombing

Pt with asbestos exposure: subpleural consolidation (arrow), pleural thickening (arrowheads)
and effusion.

Parenchymal bands in asbestosis
Webb

Subpleural Lines
• curvilinear opacity a few millimeters or less in thickness,
• less than 1 cm from the pleural surface• nonspecific indicator of atelectasis, fibrosis, or
inflammation• more common in patients who have
asbestosis than in those who have IPF or other causes of UIP

Asbestosis VS idiopathic pulmonaryfibrosis
• IPF more basal and sub pleural fibrosis• presence of parietal pleural thickening in
association with lung fibrosis is the most important feature differentiating asbestos-
induced pulmonary fibrosis from IPF• asbestos bodies in bronchoalveolar lavage
fluid
Case
• H/O asbestos exposure



References• RadioGraphics 2006; 26:59–77 Pneumoconiosis: Comparison of Imaging
and Pathologic Findings• Diagnostic imaging chest I 2-38 • High-Resolution CT of the Lung -webb













![Asbestos Disease Awareness Organization - ADAO - Asbestos ......AMERICAN JOURNAL OF INDUSTRIAL MEDICINE 60:437-442 (20] 7) Case Report Malignant Mesothelioma Due to Asbestos Exposure](https://static.documents.pub/doc/80x56/602a29585cd9200d697cd4db/asbestos-disease-awareness-organization-adao-asbestos-american-journal.jpg)



