39
Asbestosis A Case study By Erica Ducker
| Date post: | 21-Dec-2015 |
| Category: |
Documents |
| Upload: | louise-gilmore |
| View: | 216 times |
| Download: | 0 times |
AsbestosisA Case studyBy Erica Ducker

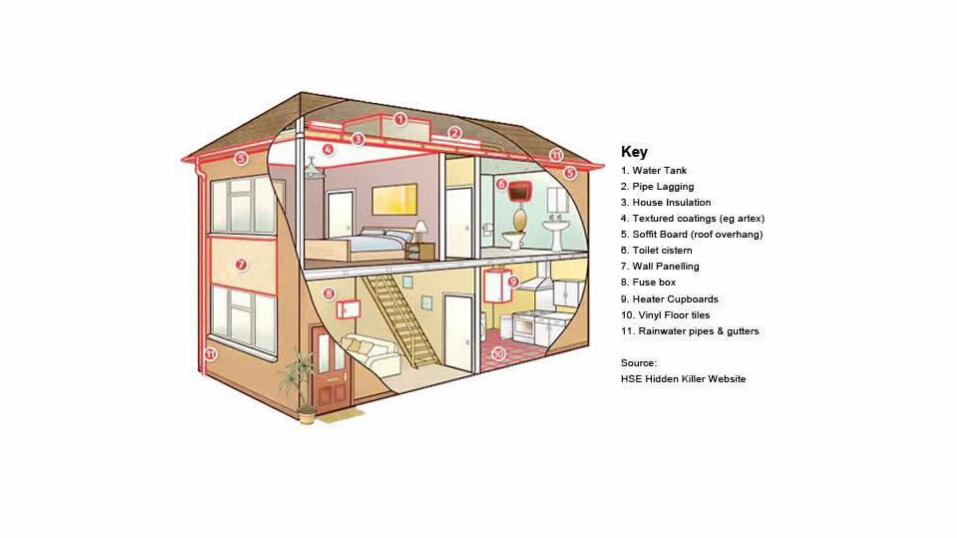
What is Asbestos?
Consists of naturally occurring silicate minerals.
In the 19th Century, it was increasingly mined and used because of its ability to absorb sound, its high tensile strength, resistance to fire, heat, electrical damage, and affordability.



Asbestosis
Asbestosis is defined as a type of pneumoconiosis caused by the inhalation of asbestos fibers.
In the 1920’s, scientists first recognized the link between asbestos and pulmonary fibrosis.
In the 1960’s, firmly established link between asbestos and both bronchogenic carcinoma and malignant mesothelioma.
Current strict regulation of asbestos has significantly decreased risk of developing asbestosis.
Asbestosis
Causes no symptoms in the early stages.Progressive cough, shortness of breath, weakness, fatigue develop over time.
Clinical asbestosis is decreasing in frequency but asbestos-related lung cancer deaths are becoming more common.
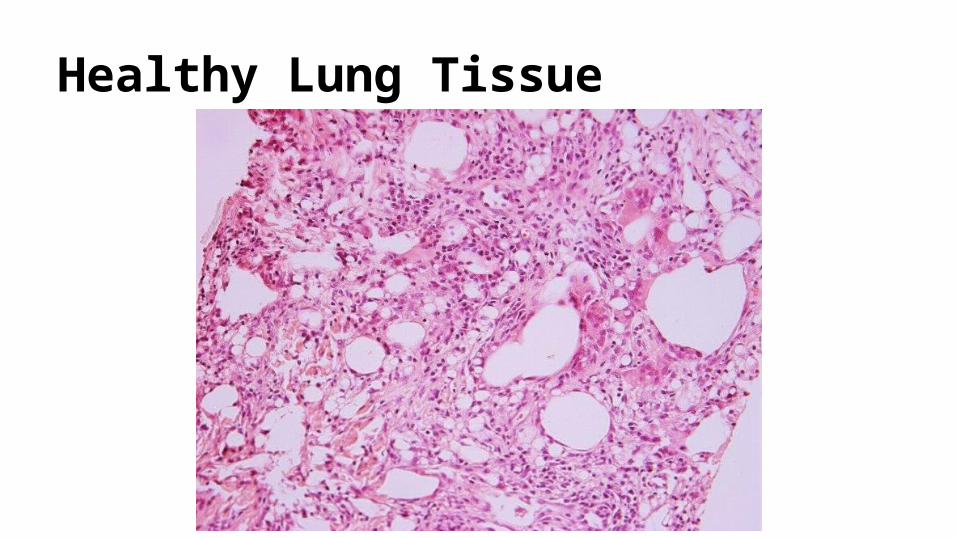
Healthy Lung Tissue
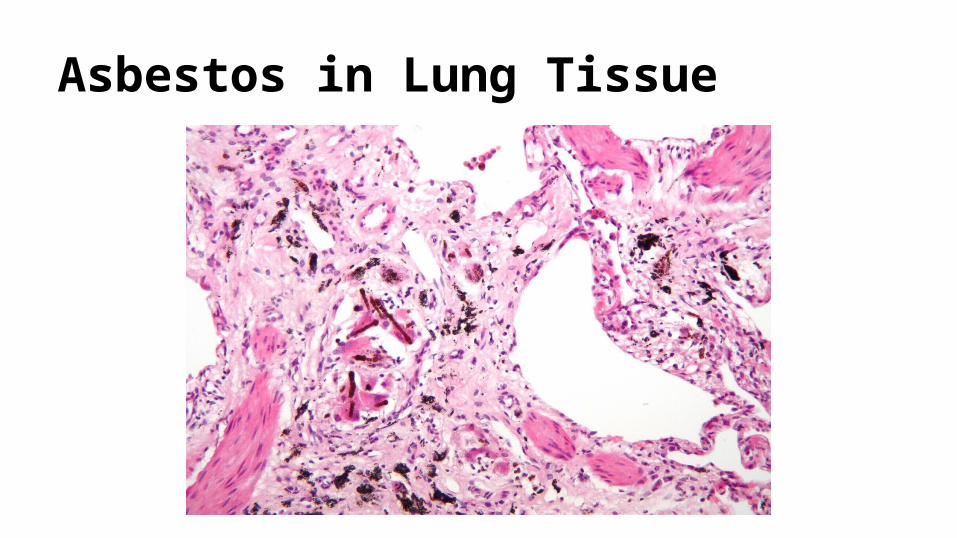
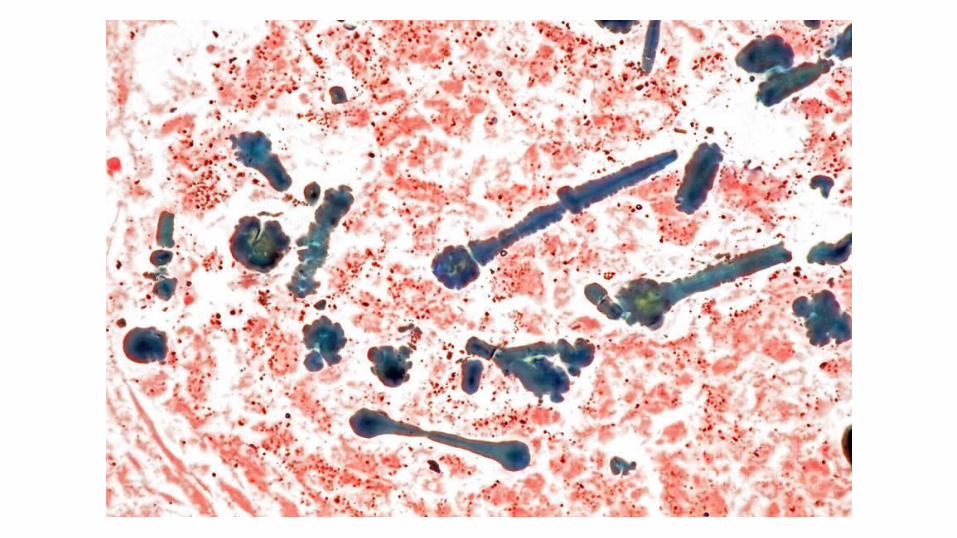
Asbestos in Lung Tissue

The Patient
69 year old man.
Retired construction contractor of 45 years.
Primarily installed insulation materials in high-rise apartment and office buildings.
Been retired for 4 years and began experiencing respiratory symptoms approximately 6 months ago.
Medical History
Appendectomy at age 13Osteoarthritis in left knee (high school football injury) x 30 yearsStatus post-cholecystectomy, 16 years agoBenign prostatic hyperplasia, transurethral resection 7 years agoHypertension x 7 yearsHyperlipidemia x 4 yearsGastroesophageal reflux disease x 4 years

Family History
Paternal history of coronary heart disease. Father died age 63 from “heart problems.”
Material history of cerebrovascular disease. Mother died at age 73 after a series of strokes.
Brother died in boating accident at age 17.
No other siblings.

Social History
Married with 3 grown children, aged 40, 45, and 49Smokes 1 pack per day x 45 yearsRarely exercisesHistory of heavy alcohol useVolunteers at community food pantryNo history of intravenous drug useKnown to unreliable in keeping follow up appointments, doesn’t like doctors
Review of Systems
Denies rash, nausea, vomiting, diarrhea, and constipationDenies headache, chest pain, bleeding episodes, dizziness, and tinnitusDenies loss of appetite and weight lossReports minor visual changes recently corrected with stronger prescription bifocal glasses.Complains of generalized joint pain, especially left knee painNever been diagnosed with chronic obstructive pulmonary disease or any other pulmonary disorderDenies paresthesias and muscle weaknessNegative for urinary frequency, dysuria, nocturia, hematuria, and erectile dysfunction
Medications
Acetaminophen 325 mg 2 tabs po Q 6H PRNRamipril 5 mg po BIDAtenolol 25 mg po QDPravastatin 20 mg po QDFamotidine 20 mg po Q HS
General
Pleasant but nervous, elderly white gentleman
Appears pale but is in no apparent distress
Looks his stated age
Strong Italian accent
Appears to be slightly overweight
Vital Signs
Blood pressure (sitting, both arms) = average 131/75 mm HgPulse = 69 beats per minuteRespiratory rate = 29 breaths per minute and slightly laboredTemperature = 98.6 °FPulse oximetry = 95% on room airHeight 5’9”Weight = 179 lb

Skin
Pallor noted
No lesions or rashes
Warm and dry with satisfactory turgor
Nail beds are pale
Head, Eyes, Ears, Nose, and ThroatExtra-ocular muscles intactPupils equal at 3mm with normal response to lightFunduscopy within normal limits (no hemorrhages or exudates)No strabismus, nystagmus, or conjunctivitisSclera anictericTympanic membranes within normal limits bilaterallyNare patentNo sinus tendernessOral pharyngeal mucosa clearMucous membranes moist but paleGood dentition

Neck and Lymph Nodes
Neck supple
Negative for jugular venous distension and carotid bruits
No lymphadenopathy or thyromegaly
Chest and Lungs
Breathing labored with tachypnea
Prominent end-inspiratory crackles in the posterior and lower lateral regions bilaterally
Subnormal chest expansion
Mild wheezing present

Heart
Regular rate and rhythm
Normal S1 and S2
Negative S3 and S4
No murmurs or rubs noted

Abdomen
Soft, non-tender to pressure, and non-distended
Normal bowel sounds
No masses of bruits
No hepatomegaly or splenomegaly

Genitalia and Rectum
Normal male genitalia, testes descended, circumcisedProstate normal in size and without nodulesNo masses of dischargeNegative for herniaNormal anal sphincter toneGuaiac-negative stool

Musculoskeletal and Extremities
No clubbing, cyanosis, or edema
Muscle strength 5/5 throughout
Peripheral pulses 2+ throughout
Decreased range of motion, left knee
No inguinal or axillary lymphadenopathy

Neurological
Alert and oriented x 3
Cranial nerves II-XII intact
Sensory and proprioception intact
Normal gait
Deep tendon reflexes 2+ bilaterally

Laboratory Blood Test Results
Na………………………..142 meq/LK…………………………..4.9 meq/LCl………………………....105 meq/LHCO3…………………… ...22 meq/LBUN………………………..12 mg/dLCr………………………….0.9 mg/dLGlu, fasting………………..97 mg/dLCa………………………….9.1 mg/dLHb…………………………..15.9 g/dLHct……………………………….41%
WBC………………….9,200/mm^3plt…………………..430,000/mm^3pH……………………………...7.35PaO2…………………….83 mm HgPaCO2…………………..47 mm Hg

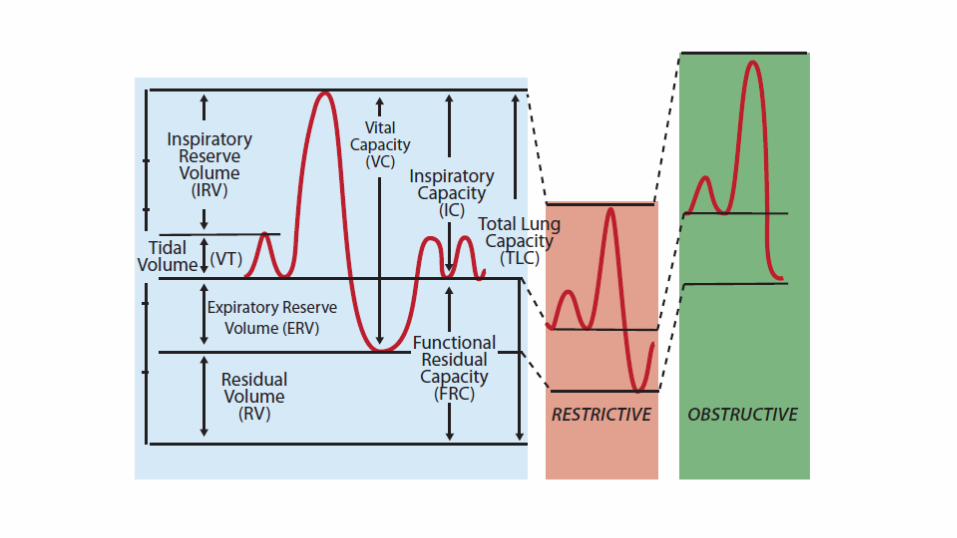
Pulmonary Function Tests (Spirometry)
Vital capacity, 3200 ccInspiratory reserve volume, 1700 ccExpiratory reserve volume, 1000 ccTidal volume, 500 ccTotal lung capacity, 4500 cc
Chest X-Ray
Posterior anterior radiograph showed coarse linear opacities at the base of each lung, more prominent on the left.
Cardiac borders and diaphragm obscured.
Consistent with findings of asbestosis cases.


High-Resolution CT Scan
Thickened septal lines and small, rounded, subpleural, intralobular opacities in the lower lung zone bilaterally- suggests fibrosis.
Ground-glass appearance involving air spaces in the upper lung zone bilaterally suggests alveolitis.
Small, calcified diaphragmatic pleural plaques and mild “honeycomb” changes with cystic spaces less than 1 cm were seen bilaterally and are consistent with asbestosis.
Discussion of Treatment
No cure for asbestosis.Treatments are all supportive.Management of disease by prevention of further injury or inhalation of asbestos.Cease smoking highly recommended.Prompt attention to possible respiratory infections.Supplemental oxygen given if patient is hypoxemic.Other supportive treatments to remove secretions from the lungs.Patient is monitored for development of lung and pleural cancers.Hospice care is given if disease progresses to terminal phase.

Conclusion
Exposure to asbestos can cause lung cancer, pleural cancer, and pulmonary fibrosis.
Complications of pulmonary fibrosis include pulmonary hypertension, heart failure, and progressive respiratory insufficiency.
Both the severity of the disease and prognosis are directly related to the history of exposure to asbestos fibers.
Patients that develop lung cancer have a very poor prognosis.
Questions?

Thank you for your attention.

















