20
Asbestos- related diseases Asian-Pacific Newsletter Volume 21, number 2, November 2014 ON OCCUPATIONAL HEALTH AND SAFETY
| Date post: | 21-Jul-2016 |
| Category: |
Documents |
| Upload: | tyoeterveyslaitos |
| View: | 214 times |
| Download: | 0 times |

Asbestos-related diseases
Asian-Pacific NewsletterVolume 21, number 2, November 2014
O N O C C U P A T I O N A L H E A L T H A N D S A F E T Y

Contents23 Editorial
Sang Gil Lee, Republic of Korea
24 The ticking time-bomb of asbestos consumption in the Asian region Matthew Soeberg, Nico van Zandwijk, Australia
28 Mesothelioma in Australia – monitoring disease incidence and past asbestos exposure with the Australian Mesothelioma Registry
Fleur E. Champion de Crespigny, Ewan MacFarlane, Paula Laws, Malcolm R. Sim, Australia
32 ICOH Statement: Global Asbestos Ban and the Elimination of Asbestos-Related Diseases (October 2013)
34 Outline for the Development of National Programmes for Elimination of Asbestos-Related Diseases
35 Eliminating asbestos hazards – Meeting report Suvi Lehtinen, Finland
36 The Helsinki Declaration on Management and Elimination of Asbestos-Related Diseases
39 Asian Asbestos Initiative Toolkit for the Elimination of Asbestos-Related Diseases
Asian-Pacific Newsletter ON OCCuPATIONAl HEAlTH AND SAfETy
Volume 21, number 2, November 2014 Asbestos-related diseases
Published by finnish Institute of Occupational Health Topeliuksenkatu 41 a A fI-00250 Helsinki, finland Editor-in-Chief Suvi lehtinen Editor Inkeri Haataja Linguistic Editing Alice lehtinen Layout Kirjapaino uusimaa, Studio
Printing Sly-lehtipainot Oy /Kirjapaino uusimaa The Editorial Board is listed (as of 1 September 2014) on the back page. This publication enjoys copyright under Protocol 2 of the universal Copyright Convention. Nevertheless, short excerpts of the articles may be reproduced without authorization, on condition that the source is indicated. for rights of reproduction or translation, application should be made to the finnish Institute of Occupational Health, International Affairs, Topeliuk-senkatu 41 a A, fI-00250 Helsinki, finland. The electronic version of the Asian-Pacific Newslet-ter on Occupational Health and Safety on the Inter-net can be accessed at the following address: http://www.ttl.fi/Asian-PacificNewsletter The issue 3/2014 of the Asian-Pacific Newsletter deals with occupational health services and primary health care.
Photographs on the cover page:Ken Takahashi, UOEH, Japan Korea Apparel Testing & Research Institute
Printed publication:ISSN 1237-0843On-line publication:ISSN 1458-5944 © finnish Institute of Occupational Health, 2014
The responsibility for opinions expressed in signed articles, studies and other contributions rests solely with their authors, and publi-cation does not constitute an endorsement by the International la-bour Office, the World Health Organization or the finnish Institute of Occupational Health of the opinions expressed in them.

Asbestos is a well-known occupational and environmentally hazardous substance. Humans have been using asbestos for a long time. Diseases associated with asbestos have also been re-ported since its use began, but especially so since asbestos began to be used in large quantities for industrial purposes. Most asbestos exposure comes from the use of asbestos for economic
purposes. Environmental exposure is closely related to the commercial use of asbestos.Asbestos is a carcinogen. According to studies, types of cancer related to asbestos continue to in-
crease. As our knowledge increases, so does the number of diseases related to asbestos. The relationship between asbestos and lung cancer, malignant mesothelioma, laryngeal cancer, and ovarian cancer has already been proven. Further research on stomach cancer and colorectal cancer is needed. Asbestos can also cause asbestosis, ventilator impairment, obstruction and chronic airway diseases. These diseases are closely related to patients’ quality of life and mortality.
Because asbestos is a well-known hazardous substance and so many studies have been carried out, some people think studies on asbestos exposure or the prevention of exposure are tedious and deriva-tive. But, at this moment many people are suffering from asbestos-related diseases and the number of patients is increasing globally. Thus we should not underestimate the importance of asbestos exposure prevention.
Asbestos exposure has caused global health problems. At first, the asbestos industry was mainly centered in Europe and North America. These industries moved to Asia, i.e. Japan, South Korea, Indo-nesia etc., and now, through unawareness or ignorance in the pursuit of economic benefit, the number of victims of asbestos-related disease are increasing in Asia. For example, asbestos textile machines op-erating in North America were moved to Japan, then the Republic of Korea. These machines now oper-ate in Indonesia. If we do not intervene, they will be moved to another country and take new victims.
Because the disease does not occur immediately after exposure, people still use asbestos. But the cost of using asbestos is a long-standing, fatal curse. The safe use of asbestos is impossible.
Through new effective diagnostic technology, we are able to reduce the number of deaths and pa-tients who suffer from severe disease caused by asbestos exposure. But we cannot rescue everybody. In addition, even though those exposed to asbestos may not yet have a disease, they have to live in fear and anxiety about becoming ill their whole lives.
For these reasons, the use of asbestos must be strictly regulated globally. We must know that the benefit of using asbestos now will have high costs through illness and death in the future. We also know that the best way to reduce the risk is to eliminate the risk factors. We already know how to save lives. It is now time to do the right thing. It is an ethical obligation.
Sang Gil Lee, MD/ Senior Researcher Occupational Health Research Team Center for Occupational Health Research Occupational Safety and Health Research Institute, KOSHA Republic of KoreaEmail [email protected]
Asian-Pacific Newslett on Occup Health and Safety 2014;21:23 • 23
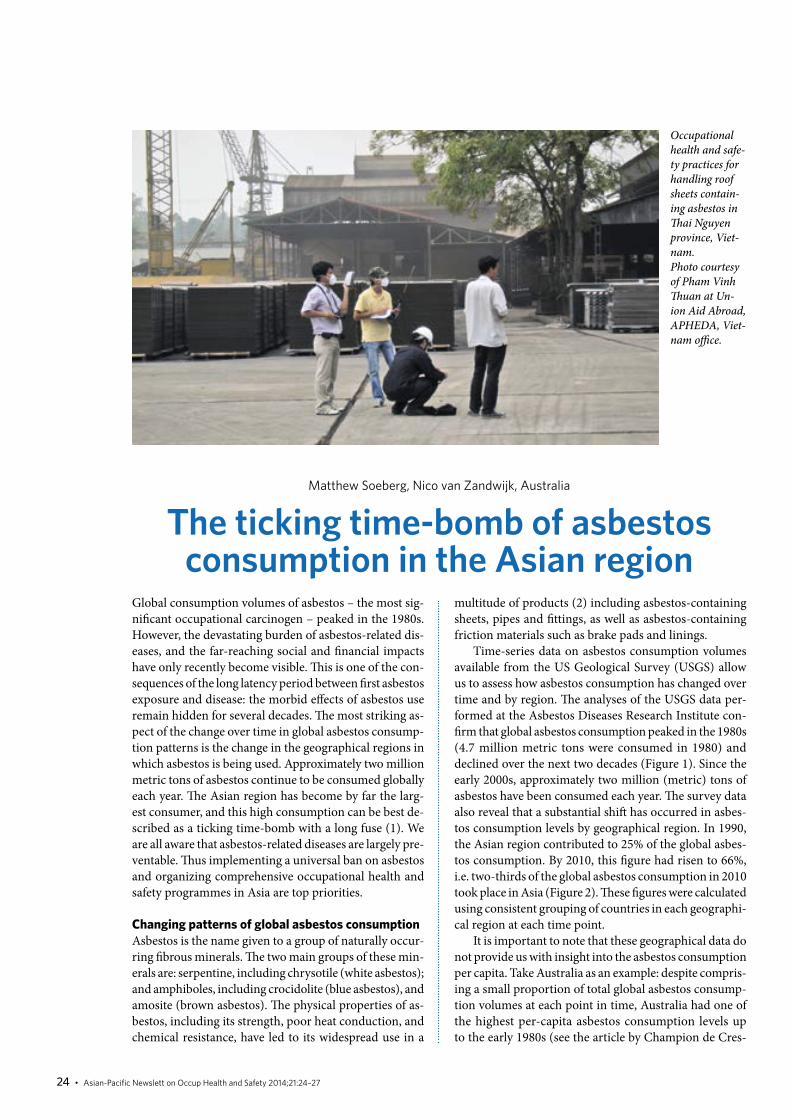
Global consumption volumes of asbestos – the most sig-nificant occupational carcinogen – peaked in the 1980s. However, the devastating burden of asbestos-related dis-eases, and the far-reaching social and financial impacts have only recently become visible. This is one of the con-sequences of the long latency period between first asbestos exposure and disease: the morbid effects of asbestos use remain hidden for several decades. The most striking as-pect of the change over time in global asbestos consump-tion patterns is the change in the geographical regions in which asbestos is being used. Approximately two million metric tons of asbestos continue to be consumed globally each year. The Asian region has become by far the larg-est consumer, and this high consumption can be best de-scribed as a ticking time-bomb with a long fuse (1). We are all aware that asbestos-related diseases are largely pre-ventable. Thus implementing a universal ban on asbestos and organizing comprehensive occupational health and safety programmes in Asia are top priorities.
Changing patterns of global asbestos consumptionAsbestos is the name given to a group of naturally occur-ring fibrous minerals. The two main groups of these min-erals are: serpentine, including chrysotile (white asbestos); and amphiboles, including crocidolite (blue asbestos), and amosite (brown asbestos). The physical properties of as-bestos, including its strength, poor heat conduction, and chemical resistance, have led to its widespread use in a
Matthew Soeberg, Nico van Zandwijk, Australia
The ticking time-bomb of asbestos consumption in the Asian region
multitude of products (2) including asbestos-containing sheets, pipes and fittings, as well as asbestos-containing friction materials such as brake pads and linings.
Time-series data on asbestos consumption volumes available from the US Geological Survey (USGS) allow us to assess how asbestos consumption has changed over time and by region. The analyses of the USGS data per-formed at the Asbestos Diseases Research Institute con-firm that global asbestos consumption peaked in the 1980s (4.7 million metric tons were consumed in 1980) and declined over the next two decades (Figure 1). Since the early 2000s, approximately two million (metric) tons of asbestos have been consumed each year. The survey data also reveal that a substantial shift has occurred in asbes-tos consumption levels by geographical region. In 1990, the Asian region contributed to 25% of the global asbes-tos consumption. By 2010, this figure had risen to 66%, i.e. two-thirds of the global asbestos consumption in 2010 took place in Asia (Figure 2). These figures were calculated using consistent grouping of countries in each geographi-cal region at each time point.
It is important to note that these geographical data do not provide us with insight into the asbestos consumption per capita. Take Australia as an example: despite compris-ing a small proportion of total global asbestos consump-tion volumes at each point in time, Australia had one of the highest per-capita asbestos consumption levels up to the early 1980s (see the article by Champion de Cres-
Occupational health and safe-ty practices for handling roof sheets contain-ing asbestos in Thai Nguyen province, Viet-nam. Photo courtesy of Pham Vinh Thuan at Un-ion Aid Abroad, APHEDA, Viet-nam office.
24 • Asian-Pacific Newslett on Occup Health and Safety 2014;21:24–27

pigny and colleagues in this newsletter edition for their discussion on the Aus-tralian malignant mesothelioma epidem-ic). Per-capita asbestos consumption cal-culations provide important information about the association between asbestos consumption volumes and the level of as-bestos-related disease, and are discussed later in this article.
Asbestos as a carcinogenic agentScientific evidence on the carcinogenic effects of asbestos has been accumulat-ing over the last forty years and new data have recently become available. The most recent review was published by the In-ternational Agency for Research on Can-cer (IARC) in 2012 (3). IARC has used a standardized approach to evaluating the strength of the evidence for carcinogenic-ity, which is now being applied to a wide range of different agents. IARC assigns one of five possible classifications to a po-tential carcinogenic agent, with Group 1 representing the agents with sufficient (abundant) evidence for human carcino-genicity.
After re-evaluating the evidence ob-tained in human populations and in ex-perimental animals, IARC determined that asbestos is definitely carcinogenic to humans (one of the one hundred and fourteen human carcinogenic agents in-cluded in the Group 1 category). IARC confirms that there is well-established epi-demiological research showing that asbes-tos exposure causes malignant mesothe-lioma, and cancer of the lung, larynx and ovary. There is more limited evidence for the association of asbestos exposure and other cancer sites. In making their deter-mination, IARC has stated that the carci-nogenic risks of asbestos apply to all forms of asbestos (including chrysotile).
The asbestos industry and their pro-ponents continue to attempt to promote the so-called safe use of chrysotile asbes-tos. These assertions lack any scientific basis and in this context it is worthwhile mentioning that the very high incidenc-es of lung cancer in Eastern Europe and the Russian republics are closely associ-ated with the unrestricted use of chryso-tile and smoking. However, the asbestos industry tries to obscure the devastating human health impacts of asbestos expo-sure. Combined evidence clearly indicates
that there are no levels at which expo-sure to any form of asbestos is considered safe, and increased cancer risks have been observed in populations with a low level of asbestos exposure (4–9). All these re-cent reports confirm again that asbestos exposure (primarily chrysotile), leads to increased risks of malignant mesothelio-ma and lung cancer. These studies from a variety of countries include data from the Asian region.
Figure 1. Global asbestos consumption (metric tons), 1920–2010, by geographical region and calendar year (first year of each decade)
Figure 2. Global asbestos consumption (metric tons), 1920–2010, by geographical region and calendar year (first year of each decade)
2010
200
0
1990
1980
1970
1960
1950
1940
1930
1920Calendar year
Metric tons
5 000 000
4 000 000
3 000 000
2 000 000
1 000 000
0
-1 000 000
Africa Asia Central and North America Europe Oceania South America Unknown
Calendar year
100%
80%
60%
40%
20%
0%1920 1930 1940 1950 1960 1970 1980 1990 2000 2010
Asbestos consumption in the Asian region as a proportion of total global consumption
Asbestos-related diseases and the latency period
An international expert framework aim-ing to establish uniform diagnoses of as-bestos-related diseases and their causal relationship with asbestos exposure has presented the Helsinki Criteria (10). The Criteria, first published in 1997, represent the consensus views of a range of interna-tional experts in the field of asbestos-re-lated lung and pleural disease. The Crite-ria describe various aspects of asbestosis,
Asian-Pacific Newslett on Occup Health and Safety 2014;21:24–27 • 25

pleural disorders, malignant mesotheli-oma, and lung cancer. Focusing on ma-lignant mesothelioma, the consensus re-port states that the great majority of mes-otheliomas is due to asbestos exposure and that mesothelioma can occur in cases with relatively low asbestos exposure. The Criteria also state that a minimum of ten years from the first exposure is required to attribute the mesothelioma to asbestos exposure. However, in most cases, the la-tency period is much longer; in the range of 30–50 years.
It is an appropriate time to consid-er the Helsinki Criteria, as the consen-sus statement has recently been updat-ed and published by Wolff et al., 2014 (11). A number of areas of the Helsin-ki Criteria were updated: CT (comput-ed tomography) screening for asbestos-related lung cancer, follow-up of asbes-tos-exposed workers and the diagnosis of non-malignant asbestos diseases, new asbestos-related disease entities, and pa-thology and biomarkers. Each of these issues is succinctly addressed in the ar-ticle by Wolff et al. However, most of the original criteria published in 1997 have remained unchanged. The Helsinki Cri-teria, alongside the carcinogen reviews performed by the International Agency for Research on Cancer and the rapid-ly accumulating body of evidence on as-bestos-related disease, represent an im-portant international reference point for asbestos-related disease.
Global burden of asbestos-related diseaseUnderstanding the global burden of as-bestos-related disease is an important yet challenging task – both for countries in which asbestos use has been banned as well as countries and regions in which such bans are yet to be implemented. This is because asbestos exposure occurs not only when handling raw asbestos prod-ucts or asbestos-containing materials in occupational settings, but also through exposure in non-occupational settings due to in situ asbestos located in build-ings and other structures in the physical environment.
There is clear evidence of an increase over time in the number of people who have died due to occupational exposure to asbestos. A study published by Lim et al. (2012) on the global burden of disease attributable to a range of different risk fac-tors included analyses of the number of deaths due to occupational exposure to as-bestos in 1990 and 2010 (12). These anal-yses show that there was a 46% increase in the number of deaths due to occupa-tional asbestos exposure between 1990 and 2010. The investigators estimated that 23 057 people died from occupational as-bestos exposure in 1990, and that this rose to 33 610 in 2010, with men making up ap-proximately 75% of all estimated deaths. These data likely reflect deaths in coun-tries and regions in which occupational asbestos exposure occurred in previous
decades and in which asbestos bans are now likely to be in place. The global bur-den of deaths from occupational asbestos exposure in countries in which asbestos is still in use will not be felt for decades to come as the latency periods have not yet expired.
There is also international evidence for clear and plausible associations between deaths from asbestos-related disease and previous asbestos consumption, such that an increase of asbestos consumption is correlated with an increase in asbestos-related disease mortality rates. These data are presented in an ecological study in-vestigating the association between lev-els of per-capita asbestos consumption and deaths from asbestos-related disease published by Lin et al. (2007) (13). In this study, the investigators calculated age-ad-justed mortality rates for malignant mes-othelioma and asbestosis and per-capita asbestos consumption for 33 countries. The results of this study show that histor-ical asbestos consumption was a signifi-cant predictor of malignant mesothelioma deaths among both sexes and of asbestosis deaths among males. The study findings add important scientific weight to the calls for a complete international ban of asbes-tos use. Further analyses published by Ni-shikawa et al. (2008) assess changes over time in country-specific mortality rates from pleural mesothelioma according to when asbestos bans were introduced (14). This study showed that the change in as-bestos use during 1970–1985 was a sig-nificant predictor of changes over time in pleural mesothelioma mortality.
The global burden of asbestos-relat-ed disease can also be measured using incidence and mortality data. The Inter-national Agency for Research on Cancer and the World Health Organization pub-lish calendar period-specific, population-based data on the global incidence and mortality of malignant mesothelioma. These global data are recognized as be-ing high-quality, as stringent data qual-ity control and analysis procedures are applied centrally, and enable internation-al comparisons. However, it is important to note that the incidence and mortality data from low- and middle-income coun-tries are often incomplete due to limit-ed resources for collecting vital statistics and health information. These global in-
Managing roof sheeting containing asbestos in Thai Nguyen province, Vietnam. Photo courtesy of Pham Vinh Thuan at Union Aid Abroad, APHEDA, Vietnam office.
26 • Asian-Pacific Newslett on Occup Health and Safety 2014;21:24–27
References
1. LintonA,VardyJ,ClarkeS,vanZandwijkN.Thetickingtime-bombofasbestos:itsinsidiousroleinthedevelopmentofmalignantmesothelioma.Criticalreviewsinoncology/hematology2012;84(2):200–12.Epub2012/03/31.
2. DodsonR,HammarS.AsbestosRiskAssessment,Epidemiology,andHealthEffects.2nd.ed.UnitedStatesofAmerica:CRCPress2011.3. InternationalAgencyforResearchonCancer.Areviewofhumancarcinogens.PartC:Arsenic,metals,fibres,anddusts/IARCWorkingGroupontheEvaluation
ofCarcinogenicRiskstoHumans.Lyon,France.2012.4. KanarekMS.Mesotheliomafromchrysotileasbestos:update.Annalsofepidemiology2011;21(9):688–97.Epub2011/08/09.5. LacourtA,GramondC,RollandP,DucampS,AudignonS,AstoulP,etal.Occupationalandnon-occupationalattributableriskofasbestosexposureformalignant
pleuralmesothelioma.Thorax2014;69(6):532–9.Epub2014/02/11.6. LacourtA,LeffondreK,GramondC,DucampS,RollandP,GilgSoitIlgA,etal.Temporalpatternsofoccupationalasbestosexposureandriskofpleuralmesothe-
lioma.TheEuropeanrespiratoryjournal2012;39(6):1304–12.Epub2011/11/15.7. OffermansNS,VermeulenR,BurdorfA,GoldbohmRA,KauppinenT,KromhoutH,etal.Occupationalasbestosexposureandriskofpleuralmesothelioma,lung
cancer,andlaryngealcancerintheprospectiveNetherlandscohortstudy.Journalofoccupationalandenvironmentalmedicine/AmericanCollegeofOccupa-tionalandEnvironmentalMedicine2014;56(1):6–19.Epub2013/12/20.
8. vanderBijS,KoffijbergH,LentersV,PortengenL,MoonsKG,HeederikD,etal.Lungcancerriskatlowcumulativeasbestosexposure:meta-regressionoftheexposure-responserelationship.Cancercauses&control:CCC2013;24(1):1–12.Epub2012/11/29.
9. WangX,YanoE,QiuH,YuI,CourticeMN,TseLA,etal.A37-yearobservationofmortalityinChinesechrysotileasbestosworkers.Thorax2012;67(2):106–10.Epub2011/09/23.
10. Asbestos,asbestosis,andcancer:theHelsinkicriteriafordiagnosisandattribution.ScandinavianJournalofWork,Environment&Health1997;23(4):311–6.Epub1997/08/01.
11. WolffH,VehmasT,OksaP,RantanenJ,VainioH.Asbestos,asbestosis,andcancer,theHelsinkicriteriafordiagnosisandattribution2014:recommendations.ScandinavianJournalofWork,Environment&Health2014.Epub2014/10/10.
12. LimSS,VosT,FlaxmanAD,DanaeiG,ShibuyaK,Adair-RohaniH,etal.Acomparativeriskassessmentofburdenofdiseaseandinjuryattributableto67riskfac-torsandriskfactorclustersin21regions,1990–2010:asystematicanalysisfortheGlobalBurdenofDiseaseStudy2010.Lancet2012;380(9859):2224–60.Epub2012/12/19.
13. LinRT,TakahashiK,KarjalainenA,HoshuyamaT,WilsonD,KamedaT,etal.Ecologicalassociationbetweenasbestos-relateddiseasesandhistoricalasbestosconsumption:aninternationalanalysis.Lancet2007;369(9564):844–9.Epub2007/03/14.
14. NishikawaK,TakahashiK,KarjalainenA,WenCP,FuruyaS,HoshuyamaT,etal.Recentmortalityfrompleuralmesothelioma,historicalpatternsofasbestosuse,andadoptionofbans:aglobalassessment.Environmentalhealthperspectives2008;116(12):1675–80.Epub2008/12/17.
15. WattersonA,GormanT,MalcolmC,RobinsonM,BeckM.Theeconomiccostsofhealthservicetreatmentsforasbestos-relatedmesotheliomadeaths.AnnalsoftheNewYorkAcademyofSciences2006;1076:871–81.Epub2006/11/23.
16. WorldHealthOrganization.Eliminationofasbestos-relateddiseases.Geneva,Switzerland:2006.
cidence and mortality data frequently also fail to contain (individual and/or popu-lation) asbestos exposure data. The IARC incidence and mortality data sets are pub-licly available at http://www-dep.iarc.fr/.
Summary: Taking action against the ticking time bomb of asbestos in the Asian regionIn countries in which asbestos consump-tion levels peaked in the 1970s and 1980s, the full devastating effects of asbestos ex-posure are only now beginning to be fully understood. The enormous impacts on human health have major financial con-sequences in the form of health care costs (15), compensation costs for those who were exposed occupationally, careful re-moval of asbestos from the (built) en-vironment and remediation of asbestos factories and mines. The substantial de-crease of asbestos consumption in largely high-income countries during the 1980s has coincided with a dramatic increase in asbestos consumption in low- and mid-dle-income countries, particularly in the Asian region. Ongoing, and increasing as-
bestos consumption in the Asian region is a ticking time-bomb with a fuse of 20–50 years or more depending on the removal of asbestos from workplaces and the en-vironment.
Recent international agency efforts (16) have highlighted the fact that the elimination of asbestos-related disease is a top priority and can be achieved through a number of practical measures. The dev-astating effects of future asbestos-related disease in the Asian region can be large-ly eliminated by planning, collaborating, and implementing evidence-based ac-tions including:• recognizing that the only way to elimi- nate asbestos-related disease is to im- plement a universal ban on asbestos• providing information, incentives and mechanisms for solutions that replace asbestos with safer substitutes• implementing comprehensive preven- tive asbestos-related disease pro- grammes in workplaces and other set- tings in which asbestos exposure is likely; and • improving the capacity and capability
to effectively diagnose and treat asbes- tos-related disease at the local level.
Together, this framework of actions will help stop the asbestos time-bomb ticking in the Asian region.
Dr. Matthew Soeberg 1,2 Professor Nico van Zandwijk 1,2
1 Asbestos Diseases Research Institute, Sydney, Australia 2 The university of Sydney, Sydney, Australia
Corresponding authorDr. Matthew SoebergResearch fellowCancer Epidemiology and Services Research Group/Asbestos Diseases Research Institute level 6 North, The lifehouse (C39Z)Royal Prince Alfred Hospital, The university of Sydney NSW 2006 AustraliaEmail: [email protected]
Asian-Pacific Newslett on Occup Health and Safety 2014;21:24–27 • 27

28 • Asian-Pacific Newslett on Occup Health and Safety 2014;21:28–32
Introduction
Australia’s long-term production and use of asbestos has resulted in one of the highest rates of mesothelioma per capita in the world [1] and presents ongoing challenges for policy-makers, occupational health and safety and the general health and safety of Australians today. By 1954, Australia was ranked fourth in the Western world in terms of gross consumption of asbestos cement products and was clearly the highest consumer per capita [1]. Most of the asbestos was used in the asbestos cement manufacturing industry and much of the output of this industry remains present in the built environment today – in houses and in sewerage and water piping – representing a continuous potential source of exposure to asbestos for the Australian community in the future.
fleur E. Champion de Crespigny, Ewan Macfarlane, Paula laws, Malcolm R. Sim, Australia
Mesothelioma in Australia – monitoring disease incidence
and past asbestos exposure with the Australian Mesothelioma Registry
The use of asbestos has been regulated in Australia since the late 1970s, initially by imposing occupational exposure limits for the different types of asbestos [1]. By the mid-1980s most uses of asbestos had been phased out and in 2003 the use (or re-use), importation, transport, sale, storage and manufacturing of all forms of asbestos and asbestos containing products was formally prohibited across Australia. The prohibition banned all new uses of asbestos but did not require removal of asbestos products that were in situ on 31 December 2003.
The long latency between exposure to asbestos and diagnosis of mesothelioma (20 to >40 years) [2, 3] means that Australia may not yet have seen the peak in mesothe-lioma diagnoses. However, models suggest that the peak is likely to occur between 2014 and 2017 [4]. Data from the Australian Institute of Health and Welfare (AIHW) have shown an apparent potential plateau in the number of new diagnoses between 2007 and 2010 at around 670 cases per year [5]. Recent Australian Mesothelioma Reg-istry (AMR) data for 2011 to 2013 suggest the beginning of a decline in the number of new cases, but because these numbers are likely to be revised upwards due to late reg-istrations with the AMR, it is too early to determine the ongoing trend [6].
Mesothelioma diagnoses in Australia have historically been concentrated among those who worked in the min-ing, manufacturing and installation of asbestos contain-ing products up until the 1980s [1]. However, because of in situ asbestos still found in Australian houses and in-frastructure, it is expected that future mesothelioma cases may be increasingly associated with exposures outside the traditional asbestos-related occupations, for example non-occupational exposures associated with “Do It Yourself ” (DIY) home renovation [7]. These new groups of people diagnosed with mesothelioma are sometimes referred to as the ‘third wave’ and there is concern that exposures from in situ asbestos may keep the incidence of mesothelioma from falling as fast as it might following the phasing out of the use of new asbestos products. However, current evi-
PhotosbyCarolineReid
White asbestos in rock, as mined at Barraba, NSW, Australia

information flowMesothelioma notifications from states/territories
NSW/VIC/QLD/WA/SATAS/ACT/NT
Contact DoctorObtain Doctor’s advice to
contact mesothelioma patient
Patient consentObtain patient consent for collection of
asbestos exposure information
Asbestosexposure
informationcollection
information flow
information flow
information flow
information flow
Asian-Pacific Newslett on Occup Health and Safety 2014;21:28–32 • 29
dence on the nature of asbestos exposures that give rise to mesothelioma is limited, making it imperative that assessments of asbestos exposure associated with new cases of mesothelioma are undertaken in the future.
The Australian Mesothelioma RegistryAustralia first began monitoring mesothe-lioma in 1980 with the Australian Meso-thelioma Surveillance Program, which actively sought voluntary notification of cases from a wide variety of sources and took a full occupational and environmen-tal history from patients or their next of kin [8]. From 1986, the programme mor-phed into the Australian Mesothelioma Register (the Register), which had a less detailed notification system and a short section seeking occupational/exposure history. By 2004 it had been clear for sev-eral years that the number of mesothelio-ma cases notified to the Register was well below the number of cases diagnosed and notified, as is mandatory, to the state and territory cancer registries. Furthermore, the quality of information collected about the cases’ asbestos exposure was low [9]. For this reason, report publication ceased in 2004 and the Register was suspended in 2007.
The demise of the Register meant the end of any national information on meso-thelioma cases’ asbestos exposure. Con-siderable effort was made by Safe Work Australia and its predecessor, the Aus-tralian Safety and Compensation Coun-cil to search for and propose viable op-tions for continuing mesothelioma sur-veillance and collecting asbestos expo-sure information. In February 2009, Safe Work Australia held a forum including mesothelioma experts as well as repre-sentatives from regulators, industry, un-ions, cancer registries and asbestos disease support groups to discuss the best way to improve the collection of information on asbestos. The forum’s consensus was to use the mandatory notification of mesotheli-oma to the state and territory cancer reg-istries, and to combine this with a timely follow-up of consenting patients to collect asbestos exposure information. In 2010, Safe Work Australia, in conjunction with a consortium led by the Cancer Institute NSW, established the Australian Meso-
thelioma Registry (AMR), which became operational in 2011.
Aims of the AMRThe AMR collects information about all new cases of mesothelioma diagnosed in Australia since 1 July 2010 in order to:• provide a timely and accurate meas- ure of the incidence of mesothelioma in Australia and to track changes in the incidence of mesothelioma over time• determine whether changes in medi- cal treatment for mesothelioma result in measurable improvements in sur- vival after diagnosis• better understand the relationship be- tween asbestos exposure and mesothe- lioma, including understanding the nature and levels of asbestos exposure associated with mesothelioma• identify changes in work-related asbes- tos exposure among mesothelioma cases and asbestos exposure patterns in non-occupational contexts• identify the groups of workers with the highest risk of exposure to asbestos
that results in mesothelioma, and• provide a resource for policy-makers dealing with the control of asbestos still present in Australia’s built environ- ment and for people undertaking re- search related to mesothelioma.
How does the AMR work?Mesothelioma notificationsMesothelioma is a notifiable disease in Australia. This means that it is manda-tory to notify state and territory cancer registries of all new cases of mesothelio-ma upon diagnosis. The AMR has an ar-rangement with each state and territory cancer registry that mesothelioma notifi-cations are ‘fast tracked’ and are thereby processed and coded as quickly as possi-ble. The state and territory cancer regis-tries submit notifications to the AMR on a regular basis and these notifications con-tain demographic and diagnosis informa-tion and also details about the deaths of mesothelioma sufferers. Patients are also able to self-notify, but these people are not included in the AMR unless a notifi-
Figure 1. AMR data flow

Asbestos remains in the built environ-ment, in-cluding in telecom-munica-tion pits
Asbestos remains in the built environ-ment – asbestos cement sheeting
Chrysotile asbestos, photographed using polarized light
30 • Asian-Pacific Newslett on Occup Health and Safety 2014;21:28–32
cation from the relevant state or territory cancer registry is also received, confirm-ing the diagnosis of mesothelioma. Fig-ure 1 shows the process of obtaining both mesothelioma notifications and asbestos exposure data by the AMR.
Asbestos exposure assessmentOnce a mesothelioma notification has been confirmed, the state and territory cancer registries contact the relevant cli-nician to determine whether or not the mesothelioma patient meets the eligibil-ity criteria for participation in the asbestos exposure assessment component of the AMR. Apart from the requirement that the diagnosis was made on or after 1 July 2010, the patient must be alive, aware of their diagnosis and well enough to partici-pate in the research. If these criteria are met, the patient is contacted by the cancer registry and asked for their consent to par-ticipate in the exposure research. At the same time they are provided with a postal questionnaire that collects information relevant to asbestos exposure, including residential, school and occupational his-tories and family history of mesothelioma.
Monash University, through the Monash Centre for Occupational and En-vironmental Health (MonCOEH) has led the design, implementation and analysis of the asbestos exposure component of the AMR. Their approach is unique among mesothelioma registries internationally in that it uses a Job Specific Module (JSM) questionnaire approach with algorithm-based analysis to estimate asbestos expo-sure in occupational and non-occupation-al spheres.
MonCOEH uses information from the postal questionnaire to design a tailored telephone interview for each patient us-ing a web application called OccIDEAS (Occupational Integrated Database Expo-sure Assessment System). OccIDEAS also provides a platform for systematic expo-sure estimation using algorithms based on published exposure data and expert input [10]. A comprehensive overview of the use of OccIDEAS in the AMR context is provided in MacFarlane et al. 2012 [10].
The telephone interview is then con-ducted with the patient and their respons-es to the JSM questions are recorded in OccIDEAS. Exposure assessment algo-rithms programmed into OccIDEAS es-

References
1. LeighJ,DavidsonP,HendrieL,BerryD.MalignantmesotheliomainAustralia,1945–2000.AmericanJournalofIndustrialMedicine2002;41:188–201.
2. BianchiC,BianchiT.Malignantmesothelioma:globalincidenceandrelationshipwithasbestos.Indus-trialHealth2007;45:379–87.
3. MarinaccioA,BinazziA,CauzilloG,CavoneD,DeZottiR,FerranteP,GennaroV,GoriniG,MenegozzoM,MensiC,MerlerE,MirabelliD,MontanaroF,MustiM,PannelliF,RomanelliA,ScarselliA,TuminoR,andItalianMesotheliomaRegister(ReNaM)WorkingGroup.Analysisoflatencytimeanditsdeter-minantsinasbestosrelatedmalignantmesotheliomacasesoftheItalianregister.EuropeanJournalofCancer2007;43:2722–8.
4. ClementsM,BerryG,ShiJ,WareS,YatesD,JohnsonA.ProjectedmesotheliomaincidenceinmeninNewSouthWales.OccupationalandEnvironmentalMedicine2007;64:747–52.
5. SWA.Asbestos-RelatedDiseaseIndicators.Canberra:SafeWorkAustralia,2014.6. AMR.3rdAnnualReport:MesotheliomainAustralia2013.Sydney:AustralianMesotheliomaRegistry,
CancerInstituteNSW,2014.7. OlsenN,FranklinPJ,ReidA,deKlerkNH,ThrelfallTJ,ShilkinK,MuskB.Increasingincidenceofma-
lignantmesotheliomaafterexposuretoasbestosduringhomemaintenanceandrenovation.MedicalJournalofAustralia2011;5:271–4.
8. NOHSC.TheIncidenceofMesotheliomainAustralia1994to1996:AustralianMesotheliomaRegisterReport,1999.Canberra:NationalOccupationalHealthandSafetyCommission,1999.
9. ASCC.PreparinganEstimateoftheNationalPatternofExposuretoAsbestosinCasesofMalignantMesothelioma.Canberra:AustralianSafetyandCompensationCouncil,2008.
10. MacFarlaneE,BenkeG,SimMR,FritschiL.OccIDEAS:AninnovativetooltoassesspastasbestosexposureintheAustralianMesotheliomaRegistry.SafetyandHealthatWork2012;3:71–6.
11. GoldbergM,ImbernonE,RollandP,GilgSoitIlgA,SavesM,deQuillacqA,FrenayC,Chamming’sS,ArveuxP,BoutinC,LaunoyG,PaironJC,AstoulP,Galateau-SalleF,BrochardP.TheFrenchnationalmesotheliomasurveillanceprogram.OccupationalandEnvironmentalMedicine2006;63:390–5.
12. MarinaccioA,BinazziA,DiMarzioD,ScarselliA,VerardoM,MirabelliD,GennaroV,MensiC,RiboldiL,MerlerE,DeZottiR,RomanelliA,ChelliniE,SilvestriS,PascucciC,RomeoE,MenegozzoS,MustiM,CavoneD,CauzilloG,TuminoR,NicitaC,MelisM,LavicoliS,andR.W.Group.Pleuralmalignantmesotheliomaepidemic:incidence,modalitiesofasbestosexposureandoccupationsinvolvedfromtheItalianNationalRegister.InternationalJournalofCancer2012;130:2146–54.
13. FazzoL,MinelliG,DeSantisM,BrunoC,ZonaA,MarinaccioA,ContiS,PirastuR,CombaP.Meso-theliomamortalitysurveillanceandasbestosexposuretrackinginItaly.Annalidell’IstitutoSuperiorediSanita2012;48(3):300–10.
14. McElvennyDM,DarntonAJ,PriceMJ,HodgsonJT.MesotheliomamortalityinGreatBritainfrom1968to2001.OccupationalMedicine2005;55:79–87.
15. HSE.MesotheliomainGreatBritain2013:MesotheliomaMortalityinGreatBritain1968–2011.London:HealthandSafetyExecutive,2014.
16. NeumannV,RuttenA,ScharmachM,MullerK-M,FischerM.Factorsinfluencinglong-termsurvivalinmesotheliomapatients–resultsoftheGermanmesotheliomaregister.InternationalArchivesofOc-cupationalandEnvironmentalHealth2004;77:191–9.
Asian-Pacific Newslett on Occup Health and Safety 2014;21:28–32 • 31
timate asbestos exposure for each par-ticipant based on his/her JSM responses [10]. Importantly, as part of the telephone interview, all participants, irrespective of job history, also receive a questionnaire module specific to non-occupational as-bestos exposure. This non-occupational module includes questions about ‘third-wave’-type exposures, for example expo-sures associated with DIY activities.
Challenges for the AMRThe main challenge for the AMR is in-creasing patient participation rates in the asbestos exposure research. Only around 18% of those diagnosed with mesothelio-ma during 2011–2013 have participated fully (both questionnaire and interview) in the asbestos exposure component. This relatively small proportion may be due to lags between diagnosis of mesothelioma and notification to registries, or delays with, or lack of approval from, the pa-tient’s clinician to contact the patient (up to 4 weeks in most jurisdictions). Given that mean survival after diagnosis is on-ly nine months, a proportion of patients become too unwell to participate by the time they receive the postal questionnaire.
The AMR is working with cancer reg-istries and clinicians to hasten notifica-tions, reduce patient recruitment time lags and raise awareness amongst clini-cians about the importance of asbestos exposure research. One of the initiatives employed to improve patient recruitment is the adoption of a passive consent model whereby clinician consent is assumed if the clinician has not responded regard-ing patient eligibility within 3-4 weeks. This has resulted in an increased pro-portion of patients contacted within the states and territories in which the pas-sive consent model operates. However, further improvements are needed for the AMR to fulfil its most unique function – namely documenting the likely asbes-tos exposure history for a representative proportion of Australians diagnosed with mesothelioma.
Future directions for the AMRA number of mesothelioma registries or surveillance programmes similar to the AMR exist worldwide. For example, the French National Mesothelioma Surveil-lance Programme was established in 1998
and includes an assessment of lifetime as-bestos exposure by industrial and envi-ronmental hygiene experts [11]. Other ex-amples include the Italian National Mes-othelioma Register [12, 13], the British Mesothelioma Register [14, 15] and the German Mesothelioma Register [16], all of which approach mesothelioma surveil-lance in slightly different ways. A chal-lenge for the AMR as it develops is to learn from and work closely with registries such as these and to share information and doc-ument worldwide patterns of diseases and asbestos exposure scenarios that result in mesothelioma. This information is poten-tially a valuable resource, particularly for developing countries, including those in
Asia where asbestos use continues and/or in situ asbestos remains a potential expo-sure source. Like some of the registries, the AMR also has the potential to evalu-ate the impact of quality of care and treat-ments on life expectancy following diag-nosis, to develop robust estimates of as-bestos exposure risks and possibly other causes of mesothelioma.
Further information on the AMRReports and data accessMore information on the AMR, includ-ing the latest statistical reports (e.g. AMR 2014) [6] can be found at http://www.mesothelioma-australia.com
Data from the AMR are made avail-

There is sufficient evidence in humans for the carcinogenicity of all forms of asbes-tos (chrysotile, crocidolite, amosite, trem-olite, actinolite and anthophyllite). Ma-lignant asbestos-related diseases include lung cancer, mesothelioma and cancers of the ovary and larynx. (1). Non-malignant asbestos-related diseases include asbes-tosis and pleural abnormalities such as pleural thickening, pleural calcification and pleural effusion. (2)
International consensus has recom-mended that a total ban on production and use of all forms of asbestos is the best way to eliminate the occurrence of asbes-tos-related diseases. In 2006 WHO stated that the most efficient way to eliminate asbestos-related diseases is to stop using all types of asbestos. (3) The ILO Reso-lution on Asbestos, 2006, calls for elimi-nating the use of asbestos and identify-
ICOH Statement: Global Asbestos Ban and
the Elimination of Asbestos-Related Diseases
(October 2013)
ing and properly managing asbestos cur-rently in place as the most effective means to protect workers from asbestos and to prevent future asbestos-related diseases and deaths. (4) By government decision, a number of countries have already adopt-ed a universal ban on all types of asbestos based on recognition of the substantial human and economic burden of diseases caused by asbestos. Some other countries have banned the use of amphibole asbes-tos, predominantly crocidolite, but have not banned the use of chrysotile. As there is sufficient evidence by the International Agency for Research on Cancer (IARC 2012) of the carcinogenicity in humans for all forms of asbestos, amphibole-only bans are inadequate; asbestos bans need to include chrysotile as well.
Some countries have banned the pro-duction and/or use of asbestos-containing
The International Commission on Occupational Health (ICOH) calls for a global ban on the mining, sale and use of all forms of asbestos and for the elimination of asbestos-related diseases. To accomplish the elimination of asbestos-related diseases, we urge each and every individual country to implement a total ban on production and use of asbestos. We also urge complementary efforts aimed at primary, secondary and tertiary prevention of asbestos-related diseases through country-specific “National Programmes for Elimination of Asbestos-Related Diseases” in line with IlO and WHO guidelines.
32 • Asian-Pacific Newslett on Occup Health and Safety 2014;21:28–32
able to researchers upon request, at the discretion of the data custodian and sub-ject to relevant ethics and administrative approval(s). The process for applying for access to data is outlined in the Data Ac-cess Policy on the AMR website.
Funding and management arrangements of the AMRThe AMR is funded by Safe Work Austral-ia – the national policy agency for work health and safety and workers’ compen-sation in Australia, and Comcare - the Australian Government work health and safety regulator for federal workplaces. The AMR is managed by the Cancer Insti-tute NSW in collaboration with the AMR Management Committee. The Commit-tee consists of a range of stakeholders and experts in the field of asbestos and mesothelioma, including representatives from Safe Work Australia, Comcare, Can-cer Institute NSW, MonCOEH (Monash University), Asbestos Diseases Research Institute, School of Public Health of the University of Sydney, the University of Western Australia, and state and territory cancer registries.
Fleur E. Champion de Crespigny1, Ewan MacFarlane2, Paula Laws3, Malcolm R. Sim2 1 Safe Work Australia2 Monash Centre for Occupational and Environmental Health, Monash univer- sity3 Cancer Institute NSW
Dr. Fleur de CrespignySafe Work AustraliaData and Analysis | DirectorPolicy and Services Branch GPO Box 641Canberra ACT 2601location code: C220 NB2Email: [email protected]

industrial products, but have continued to mine, sell and export asbestos. This is an unacceptable policy and should be recon-sidered by those countries. In order to be effective, a total ban on production, use and export of all forms of asbestos should be achieved in every country.
Even after a total ban on production and use of asbestos is achieved, occupa-tional exposure to asbestos will persist due to the continued presence of asbestos from prior use in building materials and durable machinery/equipment. Workers who carry out maintenance, demolition and removal of asbestos-containing mate-rials will thus continue to be at risk. There-fore a set of protective measures must be implemented to optimize effective pre-vention. The adoption of a total ban on all use of asbestos and products, equipment and materials containing asbestos implies a need to follow up the implementation of the ban with supplementary regulations and national programmes for ensuring the elimination of all use of asbestos and the required protection from exposure to asbestos. This includes, as appropriate, the review of legislation and regulatory sys-tems regarding trade and the protection of consumers and the external environment.
Primary prevention involves ensuring control of exposures to airborne asbestos fibres, monitoring concentrations accord-ing to established standards and reporting exposure levels to appropriate authorities. There is no exposure level below which asbestos-related disease risk can be to-tally eliminated. A global ban represents the best form of primary prevention. Ad-ditionally, for those countries that have already adopted a ban on the production and use of asbestos, environmental de-contamination required for buildings, in-dustrial facilities and infrastructures can represent a further form of primary pre-vention with beneficial impacts both on the people working in contaminated sites and on the general population. To mini-mize asbestos exposure, reference expo-sure limits (i.e., occupational exposure limits) should adhere to international standards. Complying with these limits will reduce, but not totally eliminate, the risk of asbestos-related diseases. Exposed workers should be informed about their working conditions and associated haz-ards, and provided with appropriate res-
pirators. While respirators should not be relied upon as the sole means of routinely limiting exposure to asbestos fibres, work-ers provided with them should be trained for their proper use, and encouraged to wear them when warranted. Adequate fit-ting, changing of filters, sanitary storage and maintenance of respirators are also required for optimal protection. Licens-ing or authorization procedures need to be considered to ensure safe handling, re-pair, maintenance and demolishing oper-ations. Ambient air levels at the boundary of demolition sites adjacent to residential areas should be strictly monitored and kept below exposure limits. Proper and safe handling of asbestos-contaminated waste is essential. Finally, in view of the synergistic effect of smoking and asbes-tos exposure on lung cancer risk, access to smoking cessation programmes is es-sential for all workers currently and pre-viously exposed to asbestos.
Secondary prevention includes medi-cal monitoring of exposed workers, early diagnosis and individual case manage-ment to prevent disease progression. Sec-ondary prevention is not effective for mes-othelioma and is not yet proven to be ef-fective for lung cancer among asbestos exposed individuals, but individuals iden-tified with early asbestosis can be trans-ferred away or protected from further exposure with the intent of slowing pro-gression of their disease. Malignant and non-malignant asbestos-related diseases can be diagnosed according to established guidelines. (2, 5)
Tertiary prevention includes medical intervention and public health services to limit disease-related disability and help workers affected by asbestos-related dis-eases to cope with chronic effects of their disease. Appropriate medical care and re-habilitation for the diseases and their po-tential complications, including immu-nization against pulmonary infections, should be provided. After disability and impairment evaluation, just compensa-tion and disability benefits should also be provided, as warranted.
Individuals with asbestos-related dis-eases should be reported to authorities and public health registries. Public health surveillance of asbestos-related diseases, in particular malignant mesothelioma, as-bestosis and pleural abnormalities, can
help track progress towards eliminating asbestos-related diseases and may identify where further primary prevention efforts are needed. Public health surveillance of reported exposure levels can also be used to target enhanced primary prevention.
Achieving a worldwide ban on the mining, sale and use of all forms of as-bestos and the elimination of asbestos-related diseases will require that physi-cians and occupational health personnel responsibly and persistently express their concerns, raise awareness and take nec-essary action regarding the need to pre-vent asbestos-related diseases. Recogniz-ing the urgent need for coordinated ac-tions, ICOH will continue to foster global and national collaboration in this endeav-our, promoting the engagement of ICOH members in training occupational medi-cine and health professionals in compe-tencies needed to support comprehensive national efforts to eliminate asbestos-re-lated diseases.
http://www.icohweb.org/site_new/multi-media/news/pdf/2013_ICOH%20State-ment%20on%20global%20asbestos%20ban.pdf
References
l. IARC,WHO.Asbestos(Chrysotile,Amosite,Crocidolite,Tremolite,ActinoliteandAnthophyllite).IARCMonographs,Volume100C,2012.
http://monographs.iarc.fr/ENG/Mono-graphs/vol100C/mono100C-11.pdf
2. AmericanThoracicSociety.Diagnosisandinitialmanagementofnonmalignantdiseasesrelatedtoasbestos.AmJRespirCritCareMed2004;170:691–715.
http://ajrccm.atsjournals.org/con-tent/170/6/691.full.pdf+html
3. WorldHealthOrganization.Eliminationofasbestos-relateddiseases.WHO/SDE/OEH/06.03.September2006.
http://www.who.int/occupational_health/publications/asbestosrelateddiseases.pdf
4. InternationalLabourOrganization. Resolutionconcerningasbestos,2006. http://www.ilo.org/safework/info/stand-
ards-and-instruments/WCMS_108556/lang--en/index.htm
5. Asbestos,asbestosis,andcancer: theHelsinkicriteriafordiagnosisandat-
tribution[consensusreport].ScandJWorkEnvironHealth1997;23:311–316.
http://www.sjweh.fi/show_abstract.php?abstract_id=226
Asian-Pacific Newslett on Occup Health and Safety 2014;21:32–33 • 33

In order to eliminate asbestos-related dis-eases, countries need political, operational and information tools as described below.
The National Programme for the Elimination of Asbestos-Related Diseas-es (NPEAD) is a consensus policy docu-ment that outlines the magnitude of the problem and the strategies for elimination of asbestos-related diseases. It also defines long-term objectives and targets, as well as the institutional framework for action and the directions for awareness raising and ca-pacity building. The NPEAD defines the elimination of asbestos-related diseases as a priority in protection of workers’ health, public health and the environment. There-fore, it should be based on a formal gov-ernmental decision. Ideally, such a deci-sion should be made by the government cabinet, as it involves different ministries. The governmental decision about establish-ing a NPEAD should spell out the political commitment towards elimination of asbes-tos-related diseases, should define the main elements of NPEAD, such as strategic ob-jectives and targets, mechanism for devel-opment, implementation and evaluation, leadership, role of different ministries and periodic reporting on the progress made. The outline for a NPEAD, containing sug-gestions for the key areas to be addressed under each section, is described below.
The National Asbestos Profile is an instrument for information. It defines the baseline situation with regard to consump-tion of the various types of asbestos, popu-lations at risk from current and past expo-
sures (taking into consideration the fact that some uses may have already been restricted or banned and some not), asbestos-related diseases etc.. It is updated periodically and serves as an instrument to measure the pro-gress made towards the objectives and tar-gets set by the NPEAD.
The National Asbestos Workplan is an operational tool to put in place meas-ures to achieve the objectives and targets of the NPEAD. As such, it is developed, im-plemented and evaluated on a step by step basis, taking into consideration progress made in dealing with the various forms of asbestos, available resources, and specific conditions. The Workplan should be fea-sible and adapted to the national situation, it should include time-sensitive objectives and necessary mechanisms for accountabil-ity, monitoring and evaluation. This docu-ment should also incorporate provisions for committed national support and sufficient resources for planned activities to be car-ried out, ensure sustained action, and assign responsibilities. The Workplan needs to be updated periodically to reflect progress in achieving objectives and targets set up by NPEAD and changes in use regulations.
The implementation of a NPEAD re-quires an intersectoral mechanism such as a steering committee or a task force. This mechanism should have a clearly defined mandate, responsibilities and accountabil-ity to manage the development, implemen-tation and evaluation of NPEAD. It should include representatives of the responsible governmental agencies, such as ministries
of labour, health, environment, industry, construction, trade, finance and others. It may also include academic experts, repre-sentatives of civil society, national insur-ance and compensation boards and other stakeholders. Depending on the national institutional framework, ministry of health, or other ministries may provide political leadership to the work of the intersectoral mechanism on elimination of asbestos-re-lated diseases.
All these elements require prior con-sultation between governmental agencies concerned, industry, trade unions and other interested parties on the feasibility of ob-jectives and targets, prevention strategies and responsibilities with a due considera-tion of local conditions and national situ-ation. Countries may need to organize dif-ferent forms of consultations in order to build a consensus for the establishment of the NPEAD, such as national workshops, information campaigns, and formal inter-agency consultations. In such consultations, priority should be given to protection of health and primary prevention of asbestos-related hazards over economic considera-tions. However, a consensus can only be reached when protection of health is backed up with political, legal, economic and so-cial arguments.
http://www.who.int/occupational_health/publications/asbestosdoc/enhttp://www.ilo.org/safework/areasofwork/oc-cupational-health/WCMS_108554/lang--en/index.htm
Outline for the Development of National Programmes for Elimination
of Asbestos-Related DiseasesThe IlO/WHO document entitled Outline for the Development of National Programmes for Elimination of Asbestos-Related Diseases is intented to facilitate countries, particularly those that still use chrysotile asbestos, in establishing their national programmes for elimination of asbestos-related diseases. Part of the document is published on this page. The whole text is available on the website of IlO and WHO.
34 • Asian-Pacific Newslett on Occup Health and Safety 2014;21:34
Asian-Pacific Newslett on Occup Health and Safety 2014;21:35–36 • 35
A total of 140 experts from 24 countries from Australia, Asia, Europe and North America gathered in Espoo, Finland in February 2014, to update the most recent research information concerning the ad-verse health effects of exposure to asbes-tos. The Conference was organized in col-laboration between the Finnish Institute of Occupational Health, FIOH, and the International Commission on Occupa-tional Health, ICOH.
In addition to the scientific conference on Monitoring and Surveillance of Asbes-tos-Related Diseases (ARD), the Helsin-ki Criteria, a consensus report first pub-lished in 1997, were also updated on the basis of 1.5 years of work by four Expert Groups.
Asbestos-related diseases continue to be a topical problem, despite the use of as-bestos being banned in 55 industrialized countries. As much as 2 million tons of as-bestos are still produced in the world, and about 125 million workers are exposed to it. The use of asbestos is being transferred to developing countries who lack the ca-pacities to control and manage its hazards.
Due to wide-scale use of asbestos in the last century, hundreds of thousands of workers in industrialized countries have contracted asbestos-related diseases. The ARDs often have a fatal course. Accord-ing to WHO, 107 000 people die annu-ally from ARDs, cancers or pulmonary fibrosis. In addition to the major health burden, if all the long-term health and social costs are taken into account, the significant financial impact of asbestos is clearly negative, for companies and na-tional economies alike.
The participants of the International Conference on Monitoring and Surveil-lance of Asbestos-Related Diseases ap-proved a Declaration, which you can find also on the website of the Finnish Insti-tute of Occupational Health: www.ttl.fi/helsinkiasbestos2014.
Suvi lehtinen, finland
Eliminating asbestos hazards – Meeting report
The Expert Meeting organized in 1997 produced The Consensus Report: Asbes-tos, Asbestosis, and Cancer: Helsinki Criteria for Diagnosis and Attribution. It was published in Scand J Work Environ Health 1997;23(4):311–6 (http://www.sjweh.fi/show_abstract.php?abstract_
PhotosbySuviLehtinen
id=226). The publication containing the background papers, published by FIOH, is available as a printed publication from FIOH. The results of the most recent re-search, as discussed by the four Expert Groups in 2013–2014, and commented on by the Conference participants, will

Declaration
We, the participants of the International Conference on Monitor-ing and Surveillance of Asbestos-Related Diseases (ARDs), declare: 1. The Consensus Report: Asbestos, Asbestosis, and Cancer: Helsinki Criteria for Diagnosis and Attribution 2014, updated by an International Expert Group in a two-year preparation process, and a final meeting in Espoo, Finland, on 10–13 Feb- ruary 2014, summarizes the up-to-date information on the methods for management and elimination of ARDs. The Re- port is recommended for use in the programmes and prac- tices for detection, diagnosis and attribution of ARDs.
Primary prevention 2. Primary prevention is the only effective way to eliminate ARDs. We confirm our support for the global ban of asbes- tos mining, processing, manufacturing, inclusion in any ma- terials or products, use and trade, as well as the circulation of all kinds of existing asbestos. We call for joint international actions for the implementation of the global ban. Informa- tion on the availability and feasibility of safe substitute mate- rials for asbestos should be made accessible for all in need. 3. We call for policies, regulations and practices for the preven- tion of risks and for effective protection of workers in removal
The Helsinki Declaration on Management and Elimination of Asbestos-Related Diseases
Adopted by the International Conference on Monitoring and Surveillance of Asbestos-Related Diseases, 10–13 February 2014, Espoo, Finland
36 • Asian-Pacific Newslett on Occup Health and Safety 2014;21:35–36
be integrated into the Helsinki 1997 Cri-teria. The updated Asbestos, Asbestosis, and Cancer: Helsinki Criteria for Diagno-sis and Attribution 2014 is available at the
following adress: www.ttl.fi/hcuasbestos.
”Asbestos-related deaths are prevent-able: by banning the use of asbestos, as WHO recommends,” says Professor Ken Takahashi from the University of Occu-pational and Environmental Health, Ja-pan.
”It is painful to see how developing countries are making the same mistakes that we have made in the past. It is partly a question of ignorance; and partly the case that developing countries have not experi-enced the hazards of asbestos, because of the latency time of 20–50 years between exposure and illness”, he says.
Suvi Lehtinen Chief of International Affairs finnish Institute of Occupational Health Topeliuksenkatu 41 a A fI-00250 Helsinki, finlandEmail: [email protected]
This leaflet (16 pages) is available free of charge from FIOH. Please contact Ms. Sal-mensaari, email: [email protected]

and waste handling of asbestos from existing structures (con- struction and industrial) and community infrastructures. Pre- paredness should also be ensured for the protection of work- ers, populations and communities against occupational and environmental exposures to asbestos in major hazard events, such as industrial, environmental and natural disasters. 4. Training on prevention, recognition and diagnosis of ARDs should be provided for all involved experts in health services and occupational safety and health. The competent authori- ties, employers and workers, as well as building owners and the public at large should be adequately informed and trained on asbestos hazards, of the risks of ARDs and their preven- tion and elimination.
Regulation 5. Monitoring of potential asbestos exposures should be organ- ized for identification of workers exposed to asbestos in cur- rent or previous occupations. Competent authorities should ensure the systematic registration of asbestos-exposed work- ers, their occupations, sectors of employment and exposure histories. Appropriate regulations and good practices for reg- istration of personal data and record keeping should be fol- lowed.6. In many countries health surveillance of asbestos-exposed workers is stipulated by law. In view of the lengthy latency periods of ARDs (some even beyond 50 years), health moni- toring should continue after exposure has ceased, and among workers who may have changed jobs or retired. Exposed work- ers need to be fully informed of the nature, purpose and re- sults of the monitoring. It must not result in any cost or loss of earnings for the workers. Records of the health monitor- ing data should be organized according to regulations and guidelines for good data protection practice, and kept for ap- propriate lengths of time.
Health surveillance and diagnosis 7. For medical, legal, and social reasons ARDs should be diag- nosed at the earliest possible stage of disease development. This is important for the appropriate use of available preven- tive and therapeutic opportunities, such as immunization against influenza and pneumococcus infections, and for min- imizing the adverse health effects of asbestos, as well as for compensation of disease and disability. Ongoing advances in biomedical research and technology provide good opportu- nities for more sensitive and reliable methods for early dis- ease detection and management.8. New scientific evidence provides support for the health ben- efits of screening people with a high risk of smoking-related lung cancer. Such screening programmes are also recom- mended for workers with a history of asbestos exposure who are at high risk of lung cancer. Screening should be carried out in organized screening programmes with ongoing qual- ity control, allowing assessment of lung cancer mortality.
Registration9. Systematic collection of data on ARDs is important for well- informed occupational and environmental health policies, prevention and treatment practices, and for compensation for ARDs. Diagnosed ARDs should be notified and registered according to national law and practice, based on international guidance (ILO Code of Practice, ICD10 and 11). Research and collaboration10. Further research is still needed on distribution and levels of asbestos exposures, epidemiological research on occurrence of asbestos-related cancers, further developments of methods for early diagnosis, and economic appraisal of asbestos-relat- ed diseases. International collaboration in research for follow- up, screening of asbestos-related diseases, and prevention and management of the global asbestos epidemic is recommended.
In order to prevent the epidemic of asbestos-related diseases from being repeated among workers and communities in the develop-ing world, ceasing the use of new asbestos is essential. We commit ourselves and invite all scientific and professional communities in occupational health and safety, environmental and public health, intergovernmental and nongovernmental organizations to join forces, for extension and implementation of the global ban of asbestos in all countries and protection of workers being currently exposed, as guided by the World Health Organization (WHO), International Labour Office (ILO) and the International Commis-sion on Occupational Health (ICOH).
Harri Vainio Kazutaka KogiChair of the Organizing Committee PresidentInternational Conference on Monitoring and International Commission on Occupational Health Surveillance of Asbestos-Related Diseases
Asian-Pacific Newslett on Occup Health and Safety 2014;21:36–38 • 37

Background
Over two million tonnes of asbestos are still produced, marketed, exported and used annually in some parts of the world, mainly in construction materials, asbestos cement, insulation and fire protec-tion. The production and use of asbestos has moved steadily from industrialized countries to the developing world and to countries in rapid industrialization. A total of 125 million workers are esti-mated to be exposed to asbestos in the world.
There is convincing evidence that asbestos in all its forms, even at low doses, is a proven human carcinogen. It is associated with an increased risk of cancers of lung, larynx, ovary and mes-othelioma (cancer of the pleura) among exposed workers. Other adverse health effects, pulmonary fibrosis (asbestosis), pleural changes (thickening), and related respiratory dysfunction are al-so caused by asbestos exposure. In a high proportion of cases, the diagnosis of asbestos-related diseases (ARDs) takes place at an advanced stage of the disease, with limited possibilities for effec-tive cure. New diagnostic and therapeutic methods are continu-ally being developed, thus permitting better and earlier diagnosis.
Due to wide-scale use of asbestos in the last century, hundreds of thousands of workers in industrialized countries have contract-ed ARDs. ARDs often have a fatal course. According to WHO, 107 000 people die annually from ARDs, cancers or pulmonary fibrosis. In addition to the major health burden, if all the long-term health and social costs are taken into account, the signifi-
The Helsinki Declaration on Management and Elimination of Asbestos-Related Diseases
cant financial impact of asbestos is found to be clearly negative, for companies and national economies alike.
Fifty-five countries have banned the use of new asbestos and undertaken regulatory and practical measures for the protection of workers and implementation of the ban. Notwithstanding, the adverse health effects from exposures in the past will be seen for many decades to come. The management and disposal of asbes-tos waste from existing buildings, community infrastructures and industrial facilities still constitute a risk and stringent legislation must be provided for workers’ protection.
Countries which have not yet undertaken to ban the use of new asbestos nor instituted other necessary measures for pre-vention will face the burden of ARDs for even longer periods. Thus, the global epidemic of ARDs is expected to continue well into the second half of the 21st century. Successful asbestos risk management and elimination of ARDs requires implementation of the global ban of the use of new asbestos and effective preven-tive and protective policies and practices for the management of risks from existing asbestos.
http://www.icohweb.org/site_new/ico_news_detail.asp?id=83
38 • Asian-Pacific Newslett on Occup Health and Safety 2014;21:36–38
Give your feedback!We value your opinion of the Asian-Pacific News-letter. We are in the process of analysing the reading habits of our readers.
Please visit the newsletter website and answer our questionnaire: www.ttl.fi/Asian-PacificNewsletter
Your comments are very much appreciated.
Five prizes will be raffled among the respondents.

Asian-Pacific Newslett on Occup Health and Safety 2014;21:39 • 39
We are pleased to hereby deliver the “Toolkit for the Elimination of Asbestos-Related Diseases”. This toolkit has been developed to serve as a concise and easy-to-use reference source of knowledge, technologies and information that merit attention for the purpose of eliminating asbestos-related diseases (ARDs). As such, the traditional public health approach, i.e., to address the three levels of prevention, was considered to be the basic means to tackle ARDs. Today it is a sad reality that many countries, especially those which are rapidly developing, continue to use asbestos at alarming levels. The de-veloping countries in Asia are at the forefront of this trait, so we intended the administrators, practitioners and researchers therein to be the primary beneficiaries. But our hope is that any party with concern on ARDs can have something to benefit from this toolkit. Whoever the party, a core principle to bear in mind, while referencing this toolkit, is that the most effective means to prevent ARDs is to stop using asbestos.
On behalf of all Contributors and the Secretariat, Ken Takahashi, MD, PhD, MPH Professor and Chair of Environmental Epidemiology, IIES Director of the International Center University of Occupational and Environmental Health, Japan
Asian Asbestos InitiativeAsia has recently become the world’s cent-er of asbestos consumption. Many Asian countries, particularly those in the midst of rapid industrialization, are increasingly
Toolkit for the Elimination of Asbestos-Related Diseases
using asbestos at substantial levels. Some-how the burden of asbestos-related dis-eases has not become apparent in many of these countries, mainly because the la-
tency time has not been reached yet and also because the recognition of these diseases is poor. However, the experiences of industrialized coun-tries that have extensively used as-bestos in the past show that an epi-demic of asbestos-related diseases is predictable in the region.
The Asian Initiative for the Elimination of ARDs (i.e. the Asian Asbestos Initiative or AAI) aims to develop an academic platform on which researchers and administrators from differ-ent countries can share relevant core technologies. The ultimate goal of this project is consistent with the efforts of the WHO and the International Labour Organization, to eliminate
ARDs. Proponents agree that the most effective means to prevent ARDs is to discontinue the use of asbestos; however, they acknowledge that the process will re-quire a gradual transition involving pro-gressive steps.
The AAI considers the tradition-al public health approach as the central pillar on which to develop intervention strategies as this model addresses all three levels of prevention. Thus, clinical tech-nologies (i.e. including the diagnosis and treatment of ARDs) are as important as technologies at the primary level of pre-vention (i.e. reducing or eliminating ex-posure). These efforts will focus on Asian countries, while attempting to formulate a regional model from which other parts of the world may benefit. The time is ripe for technology sharing.
http://envepi.med.uoeh-u.ac.jp/aai/aboutaai.html
The Toolkit can be accessed at the following address: http://envepi.med.uoeh-u.ac.jp/toolkit/index.html

Editorial Boardas of 1 September 2014
Nancy Leppink Chief of lABADMIN/OSH International labour Office 4, route des Morillons CH-1211 Geneva 22SWITZERlAND
Evelyn Kortum Technical Officer, Occupational Health Interventions for Healthy Environments Department of Public Health and Environment World Health Organization 20, avenue Appia CH-1211 Geneva 27 SWITZERlAND
Jorma Rantanen ICOH, Past President fINlAND
Harri Vainio Director General finnish Institute of Occupational Health Topeliuksenkatu 41 a A fI-00250 Helsinki fINlAND
Chimi Dorji licencing/Monitoring Industries Division Ministry of Trade and Industry Thimphu BHuTAN
N.B.P. BalallaHeadOccupational Health DivisionBlock 2 G5-03Jalan Ong Sum PingBandar Seri Begawan BA 1311 BSBBRuNEI DARuSSAlAM
Yang Nailian National IlO/CIS Centre for China China Academy of Safety Sciences and Technology 17 Huixin Xijie Chaoyang District Beijing 100029 PEOPlE’S REPuBlIC Of CHINA
Ho Ho-leung Deputy Chief Occupational Safety Officer Development unit Occupational Safety and Health Branch labour Department 14/f, Harbour Building 38 Pier Road, Centrum HONG KONG, CHINA
K. Chandramouli Joint Secretary Ministry of labour Room No. 115 Shram Shakti Bhawan Rafi Marg New Delhi-110001 INDIA
Lee Hock Siang DirectorOSH Specialist DepartmentOccupational Safety and Health Division#04-02, Ministry of Manpower Services Centre1500 Bendemeer RoadSingapore 339946SINGAPORE
John Foteliwale Deputy Commissioner of labour (Ag) labour Division P.O. Box G26 Honiara SOlOMON ISlANDS
Le Van TrinhDirectorNational Institute of labour Protection99 Tran Quoc Toan Str.Hoankiem, HanoiVIETNAM

















