Assault on the RV Impact of Pulmonary Hypertension on Heart-Lung Interactions John Greenwood, MD University of Pennsylvania Department of Emergency Medicine Department of Anesthesiology & Critical Care
Transcript
Assault on the RV
Impact of Pulmonary Hypertension on
Heart-Lung Interactions
John Greenwood, MDUniversity of Pennsylvania
Department of Emergency MedicineDepartment of Anesthesiology & Critical Care
DISCLOSURES
NONE.
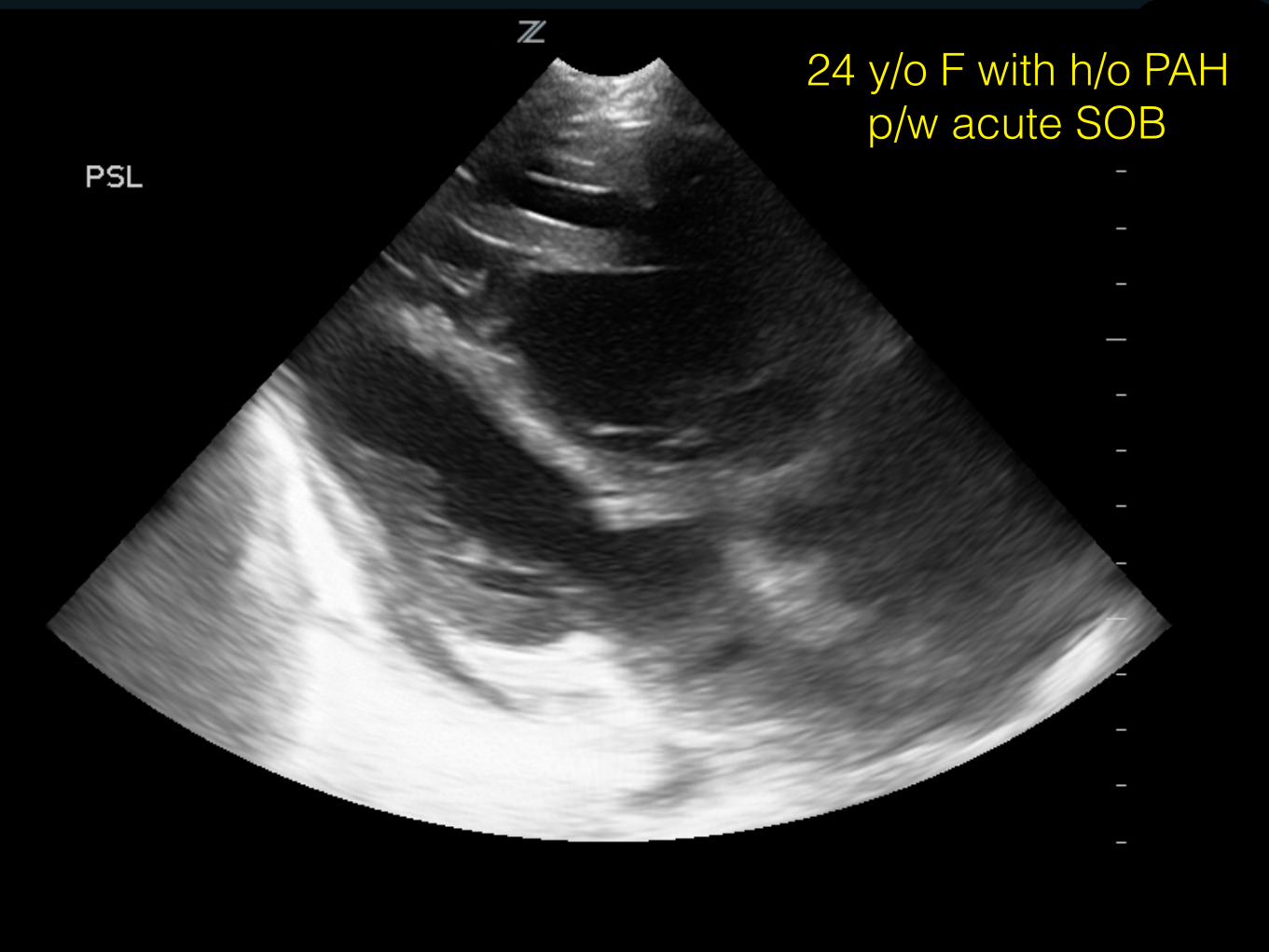
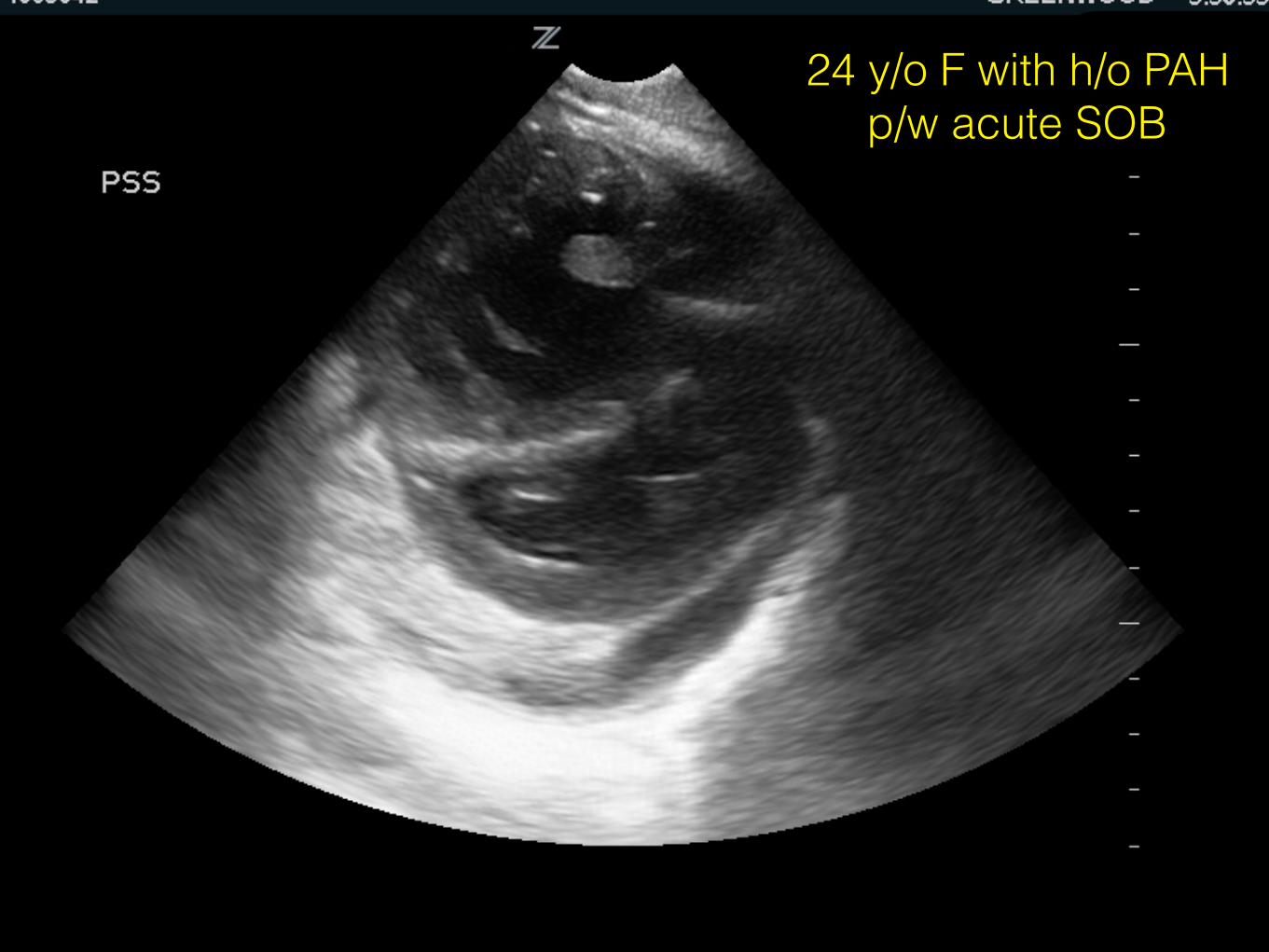
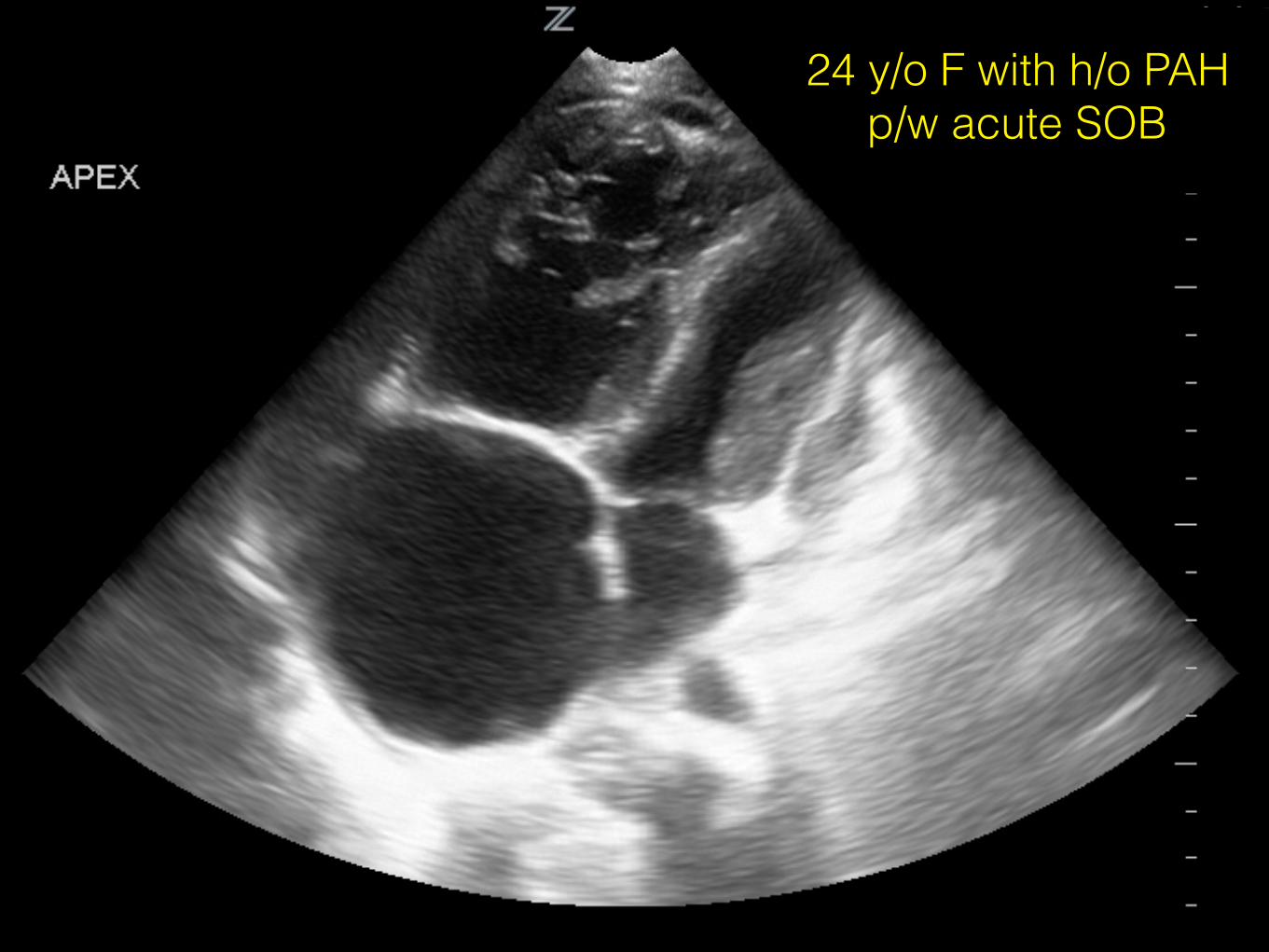
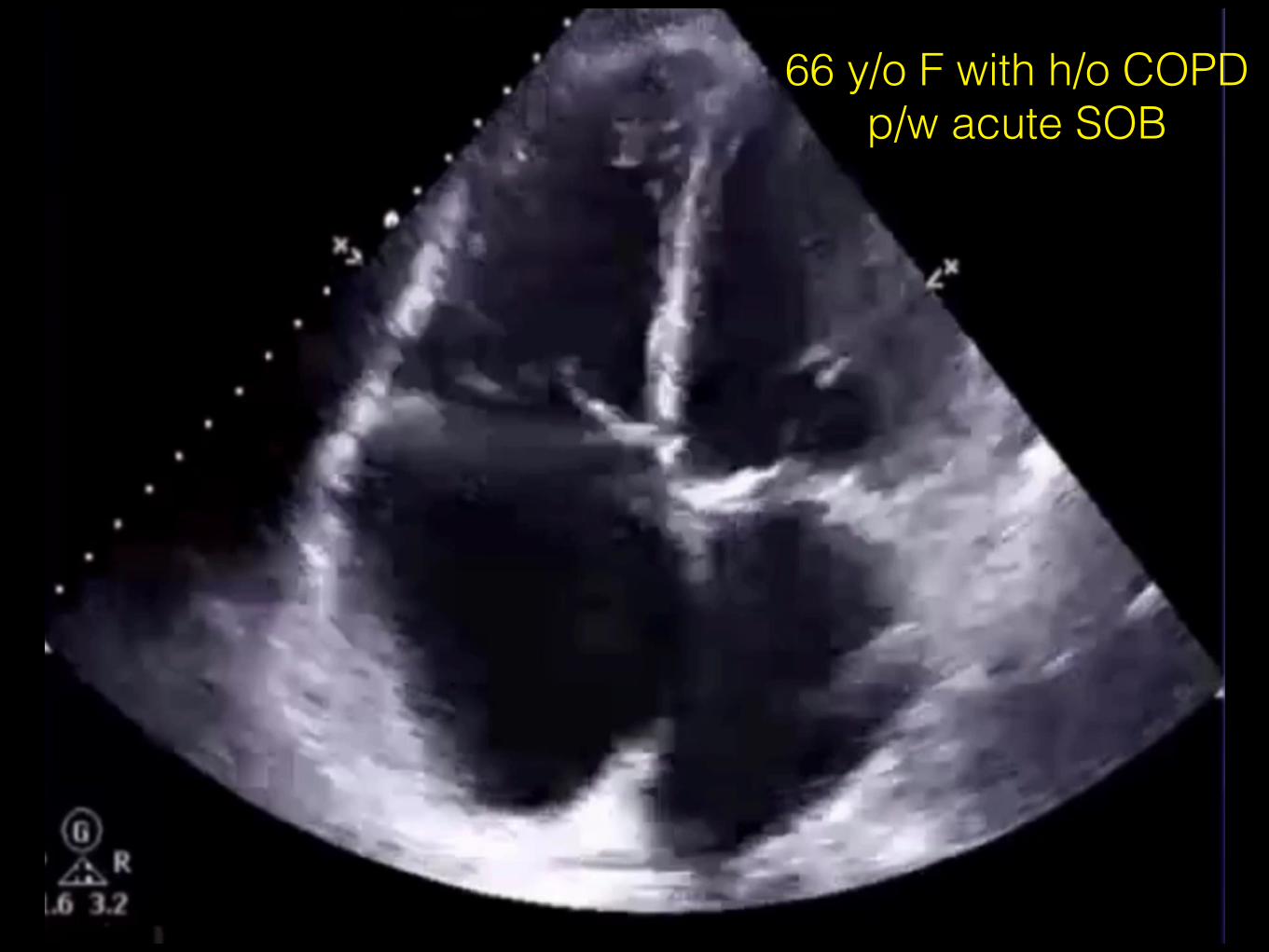
THE PATIENT
THE PATIENT
OBJECTIVES
• Understand clinical heart-lung interactions affected by pulmonary hypertension (PH)
• Identify patients at high risk for arrest from PH
• Discuss critical management strategies for the unstable patient with PH & RV dysfunction
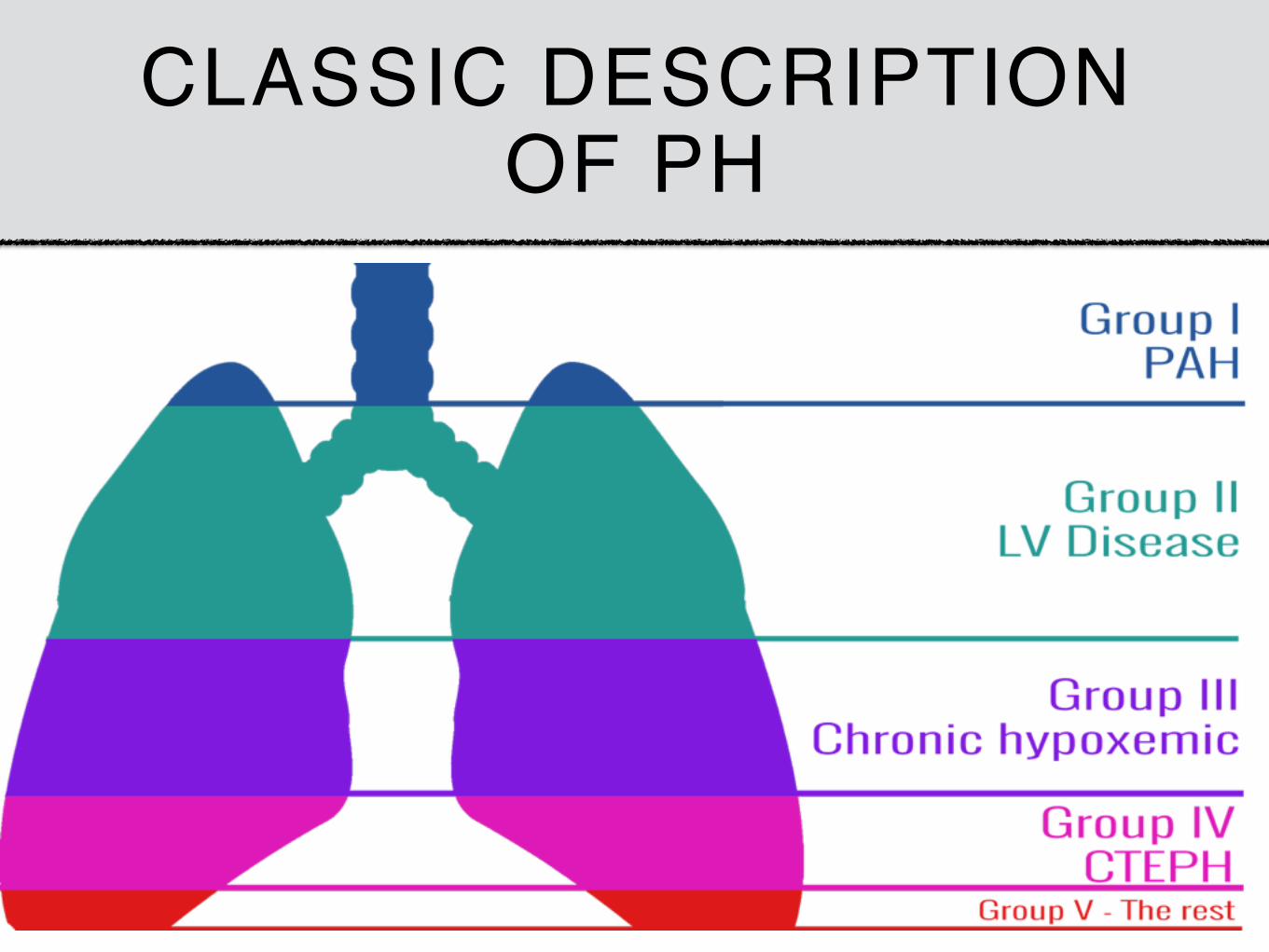
CLASSIC DESCRIPTION OF PH
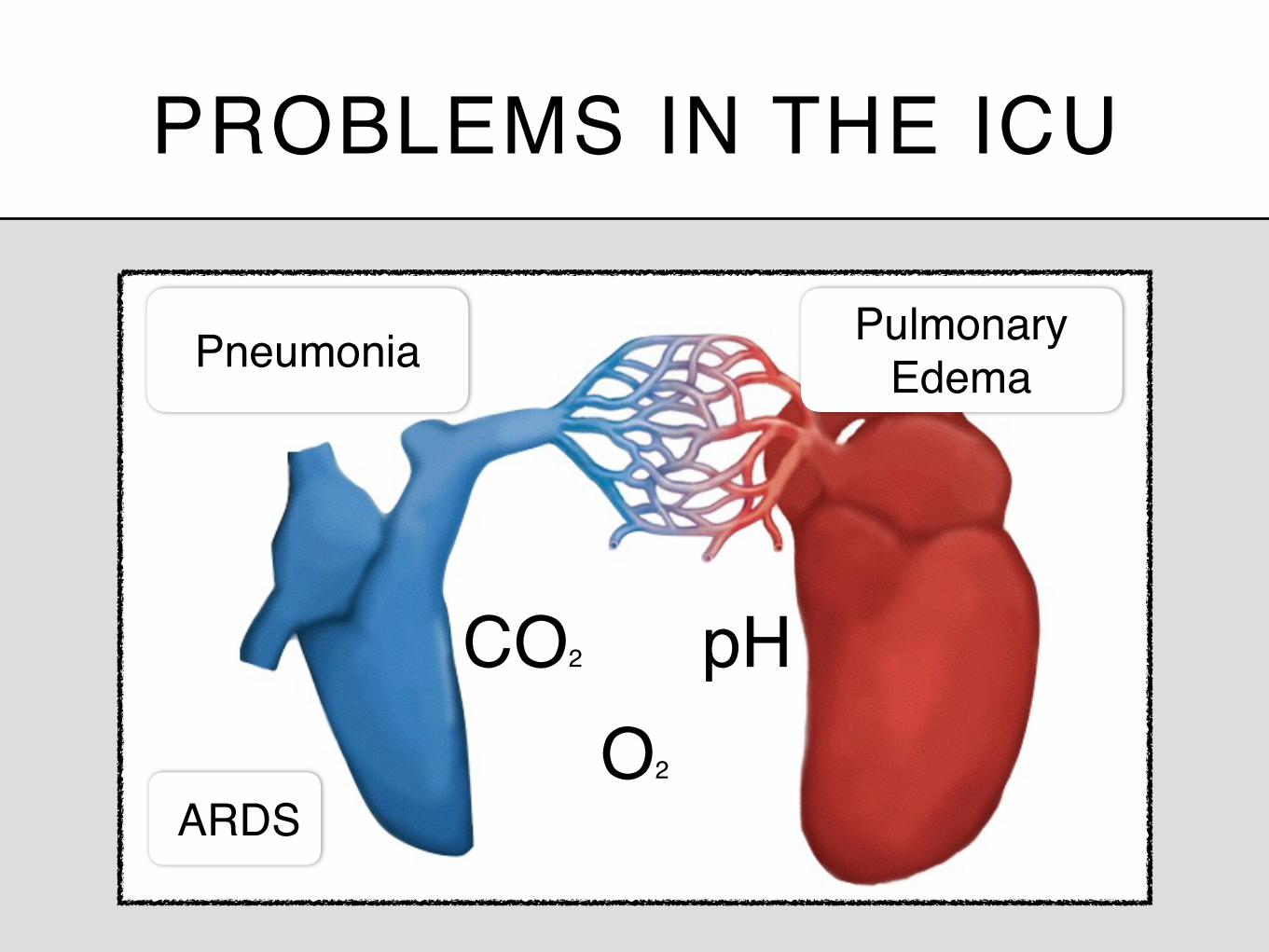
PROBLEMS IN THE ICU
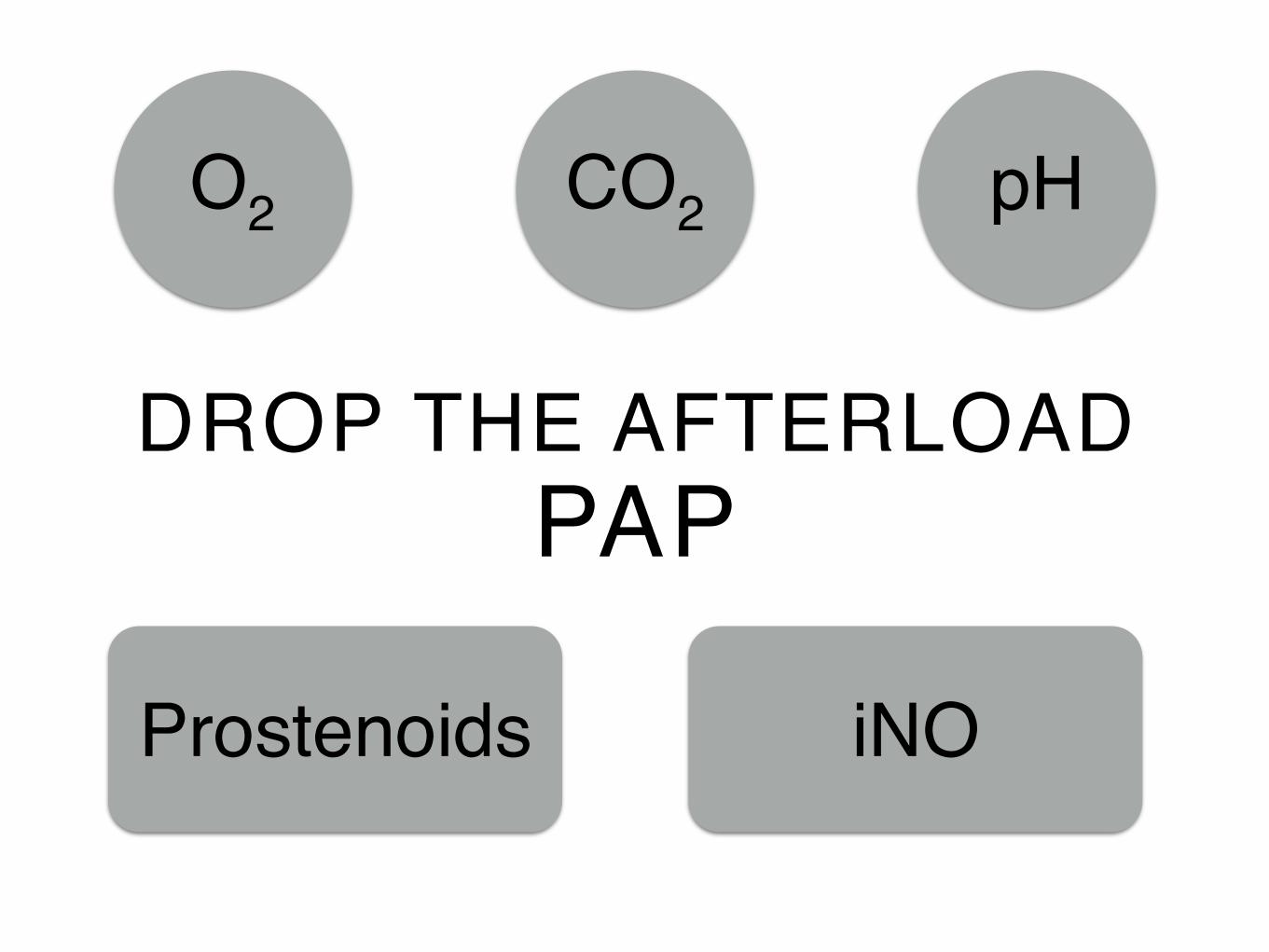
CO2
O2
pH
Pneumonia PulmonaryEdema
ARDS
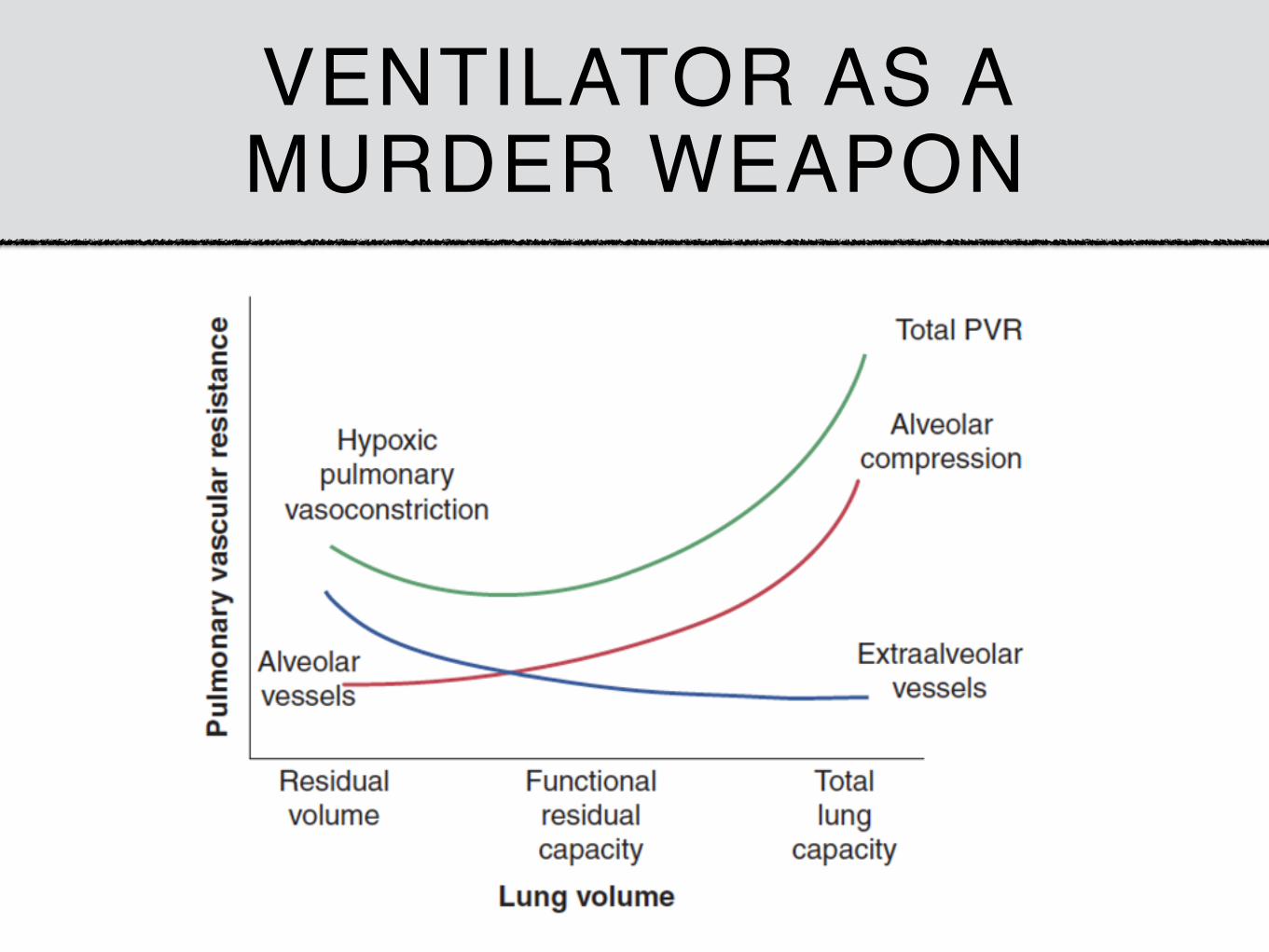
VENTILATOR AS A MURDER WEAPON
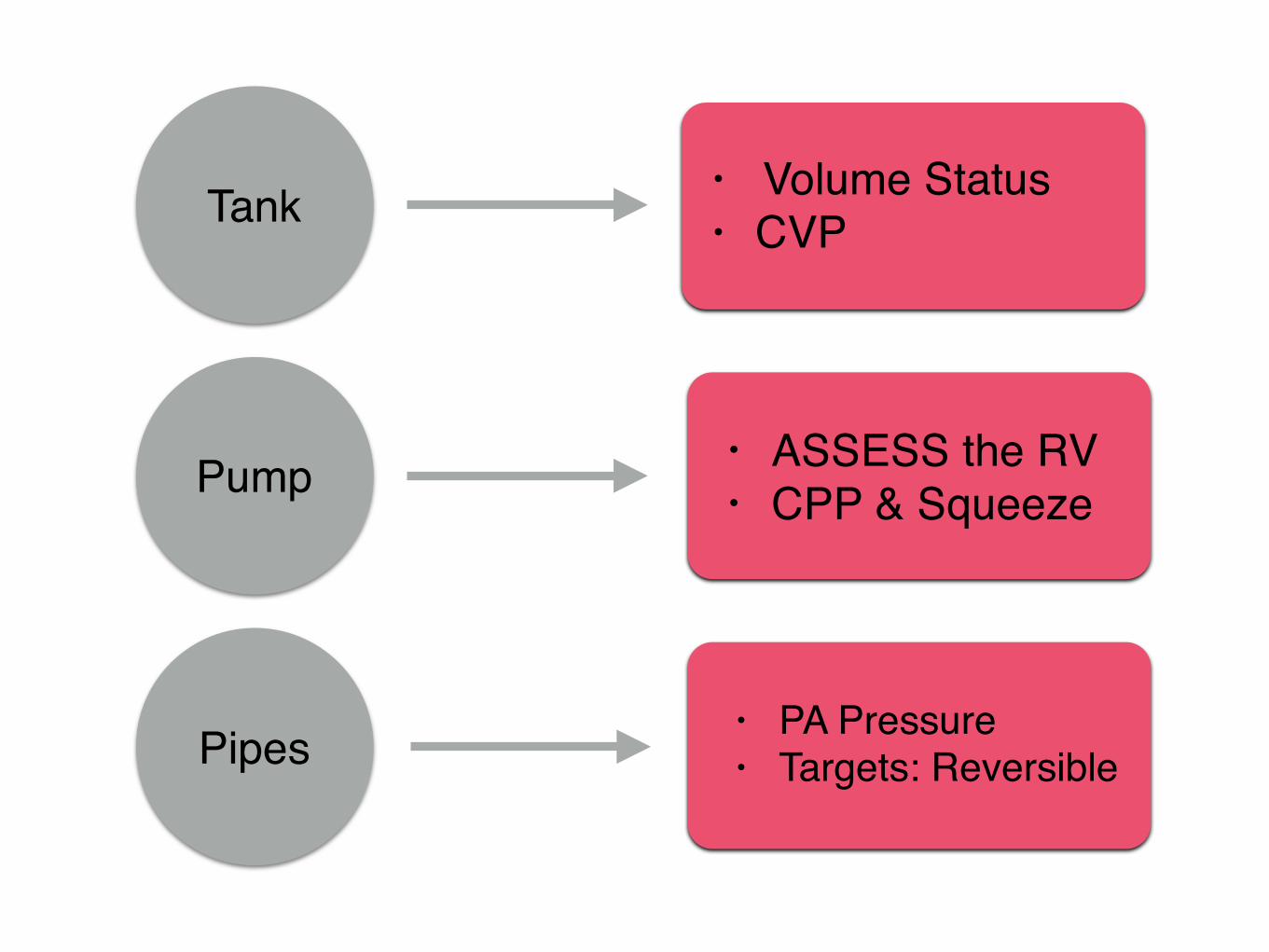
CARDIOVASCULAR CONSEQUENCES OF PH
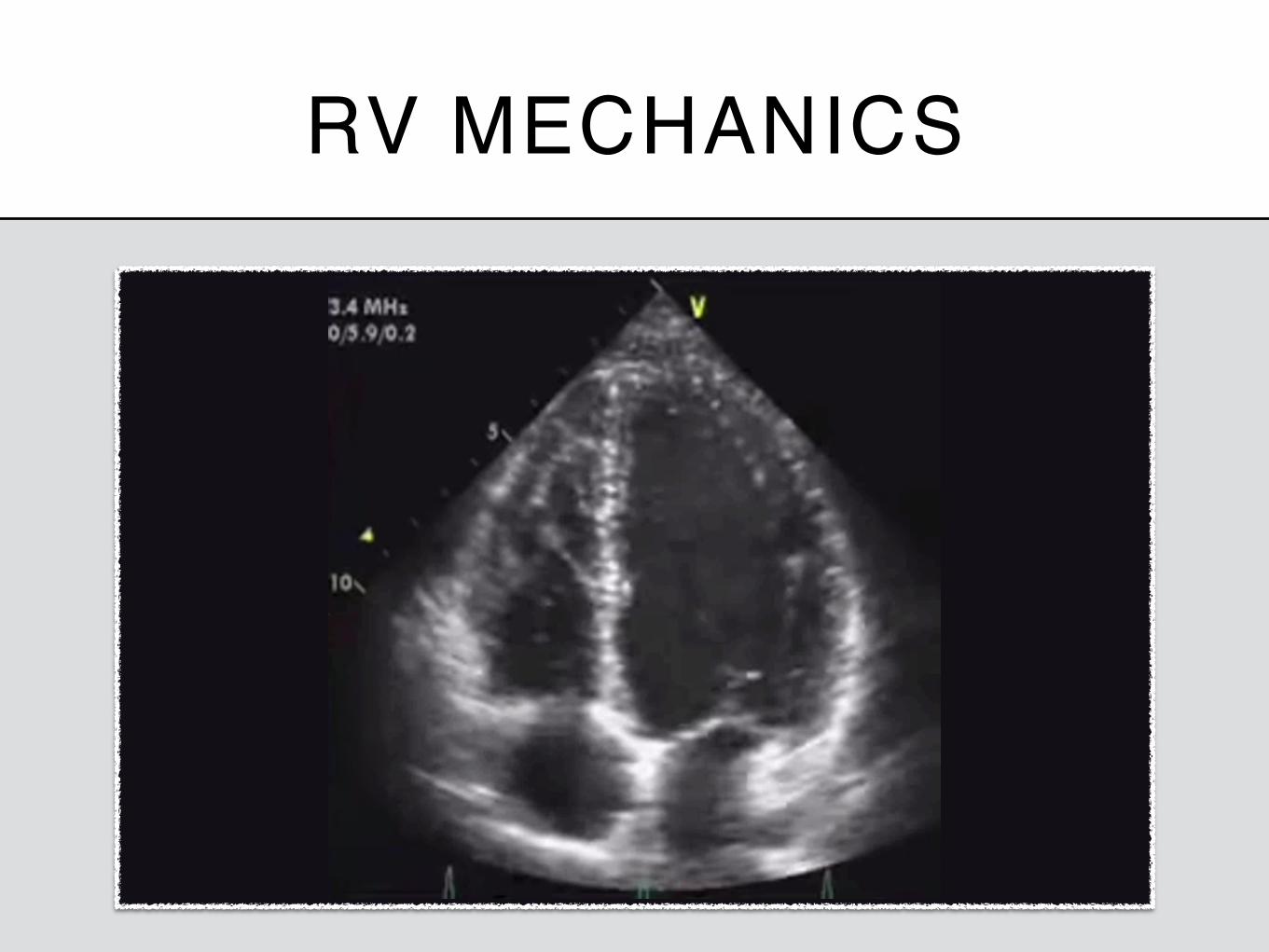
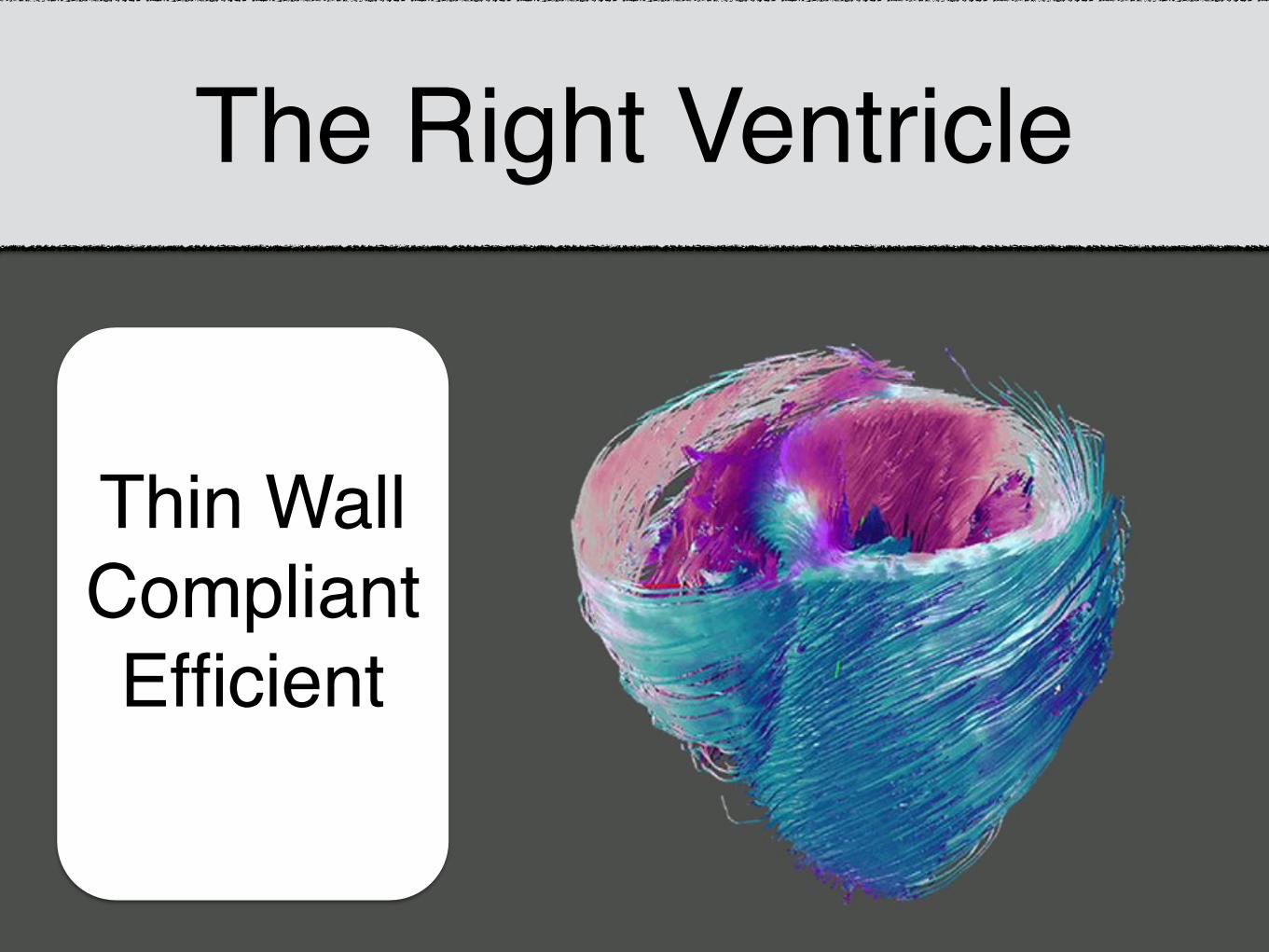
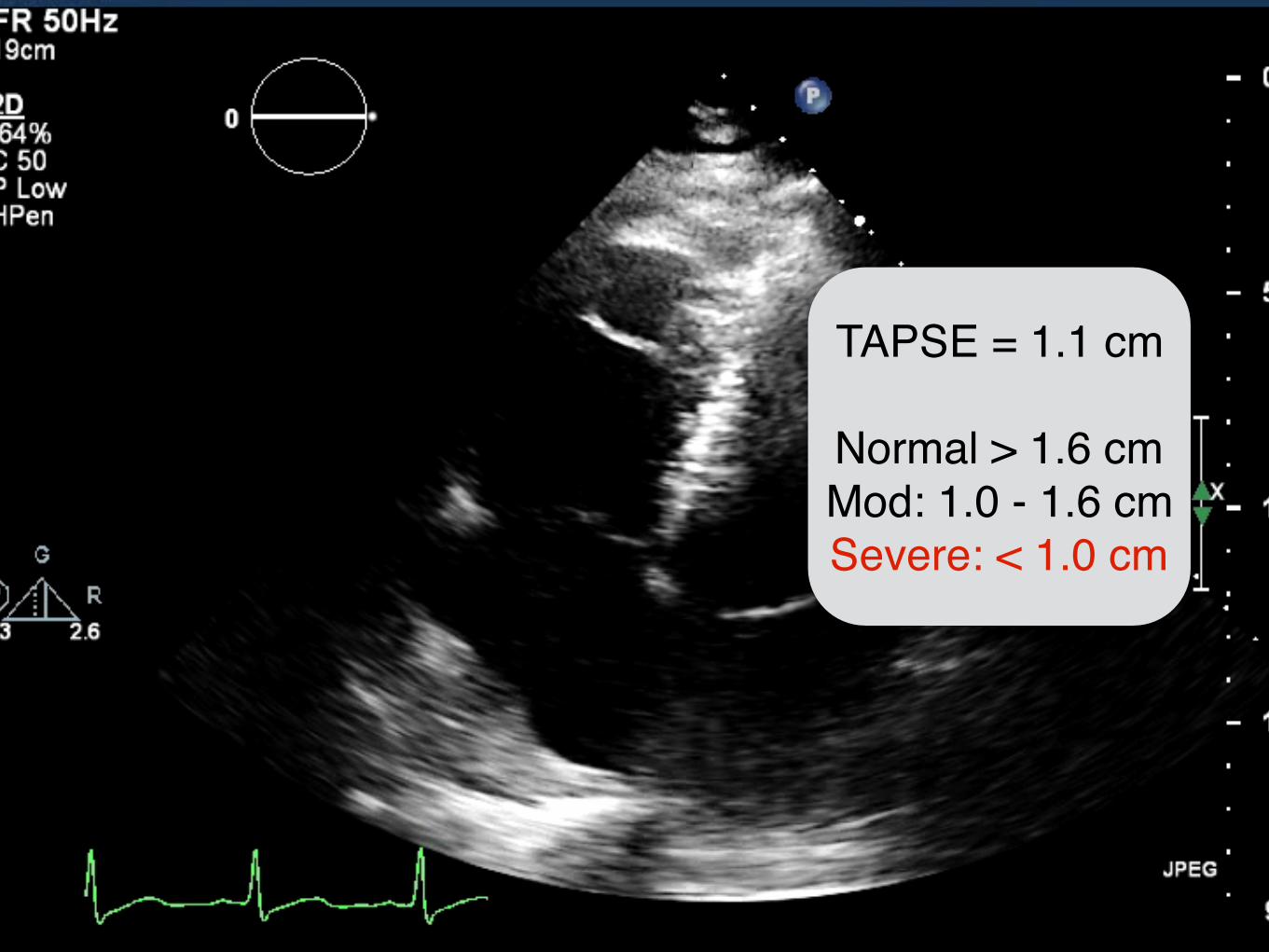
RV MECHANICS
The Right Ventricle
Thin WallCompliantEfficient
VerticalMotion
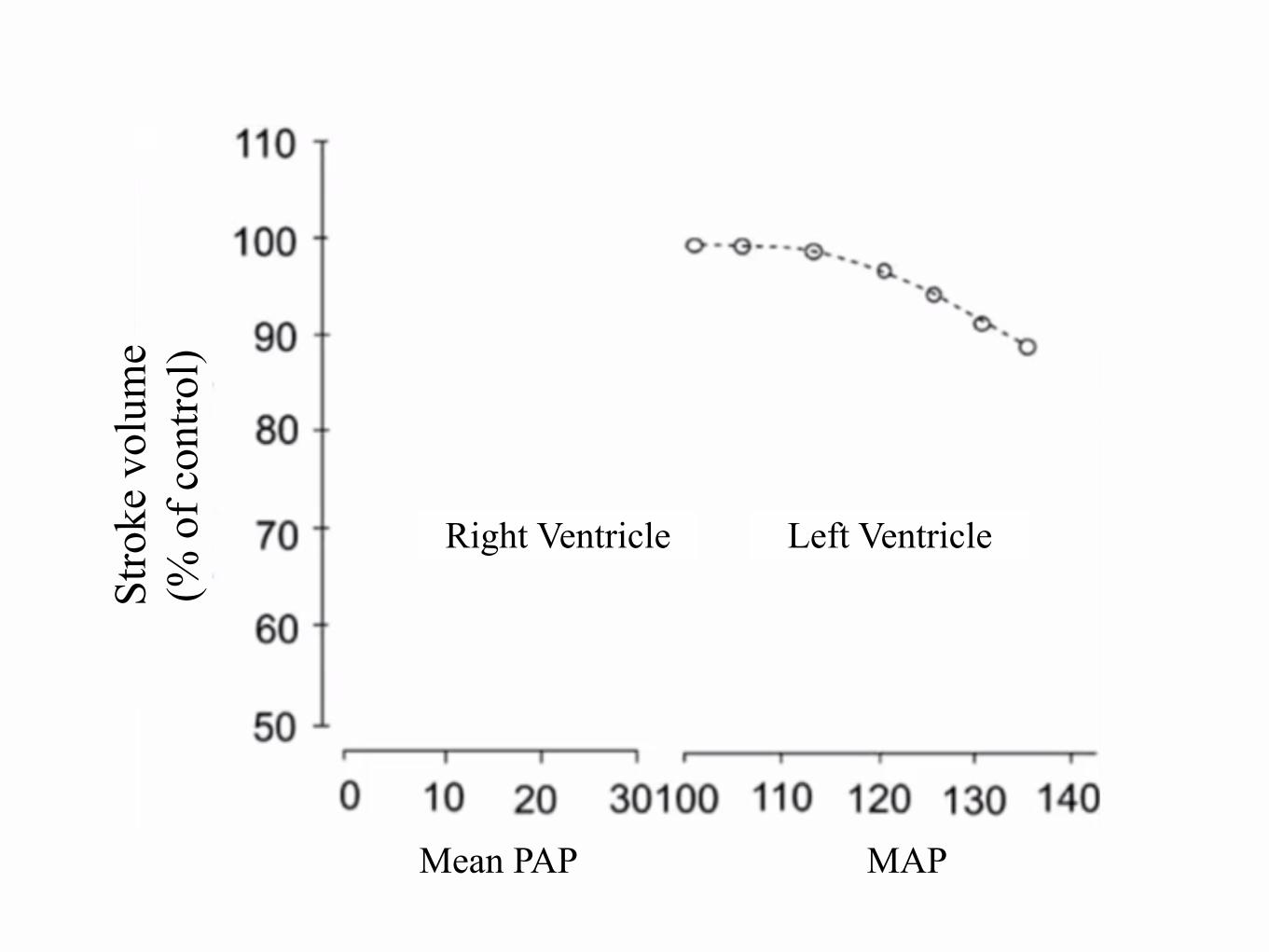
Adapts to VOLUME
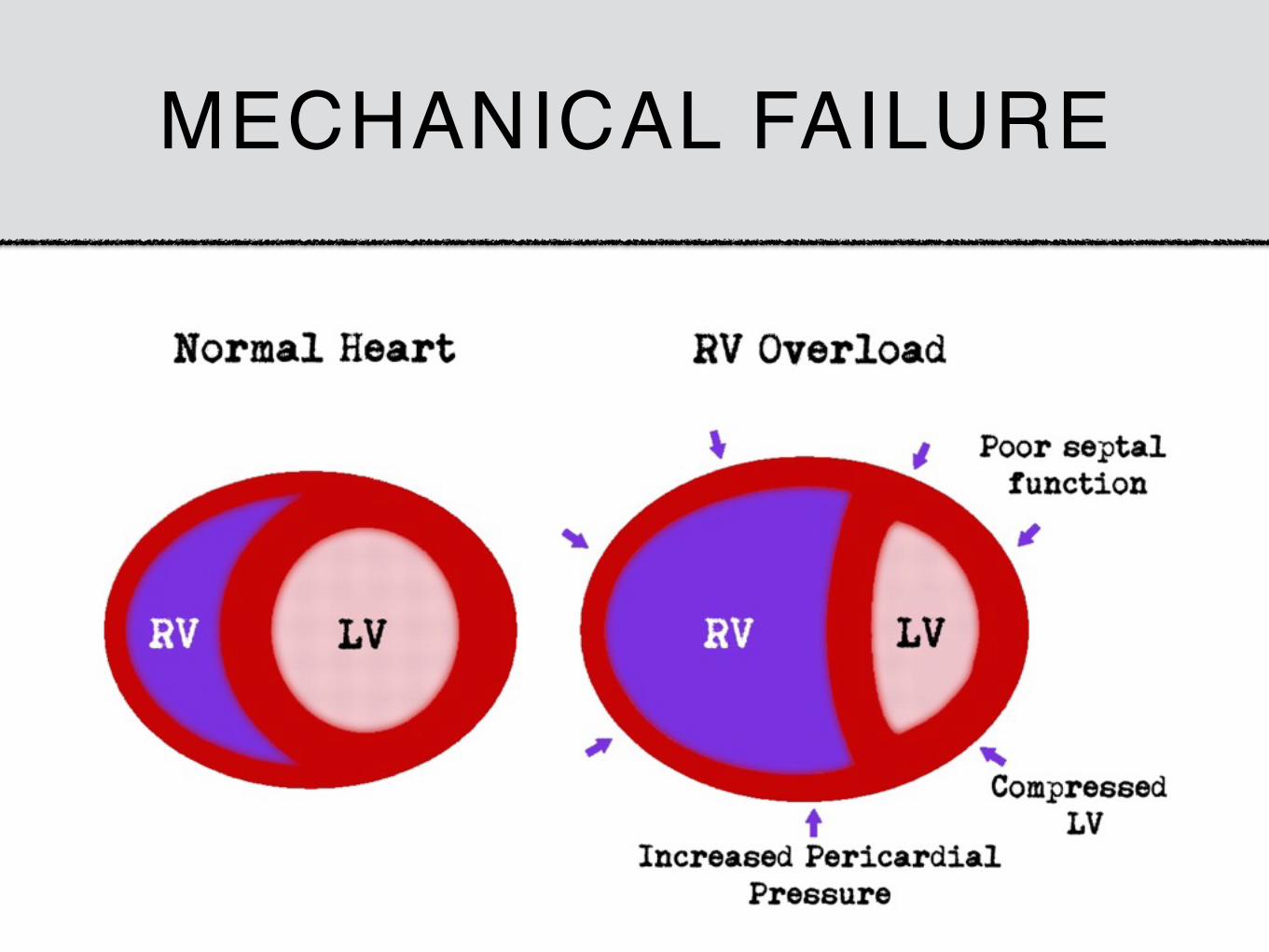
Fails under PRESSURE
MECHANICAL FAILURE
Mean PAP MAP
Right Ventricle Left Ventricle
Stro
ke v
olum
e (%
of c
ontro
l)
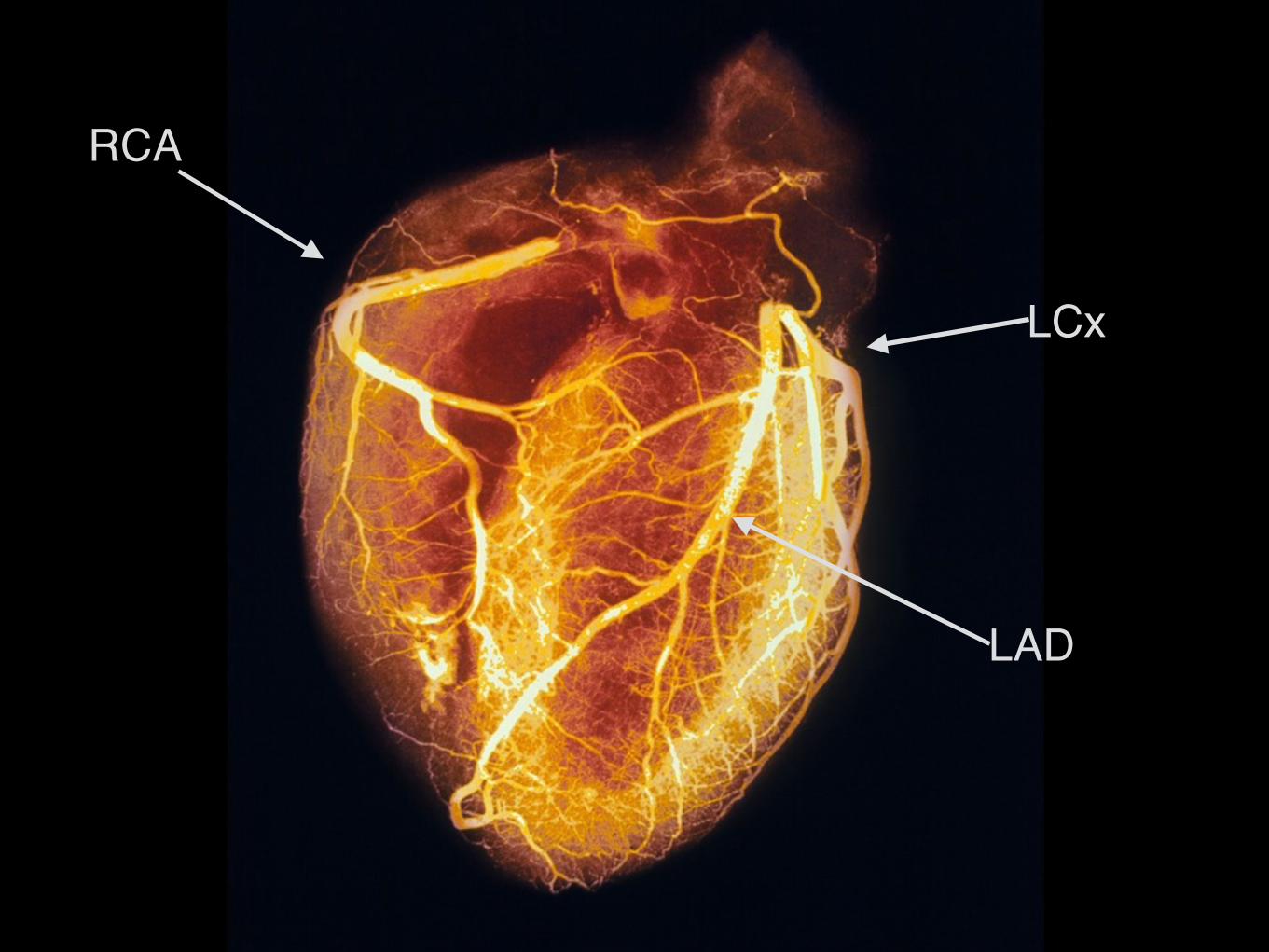
RCA
LCx
LAD
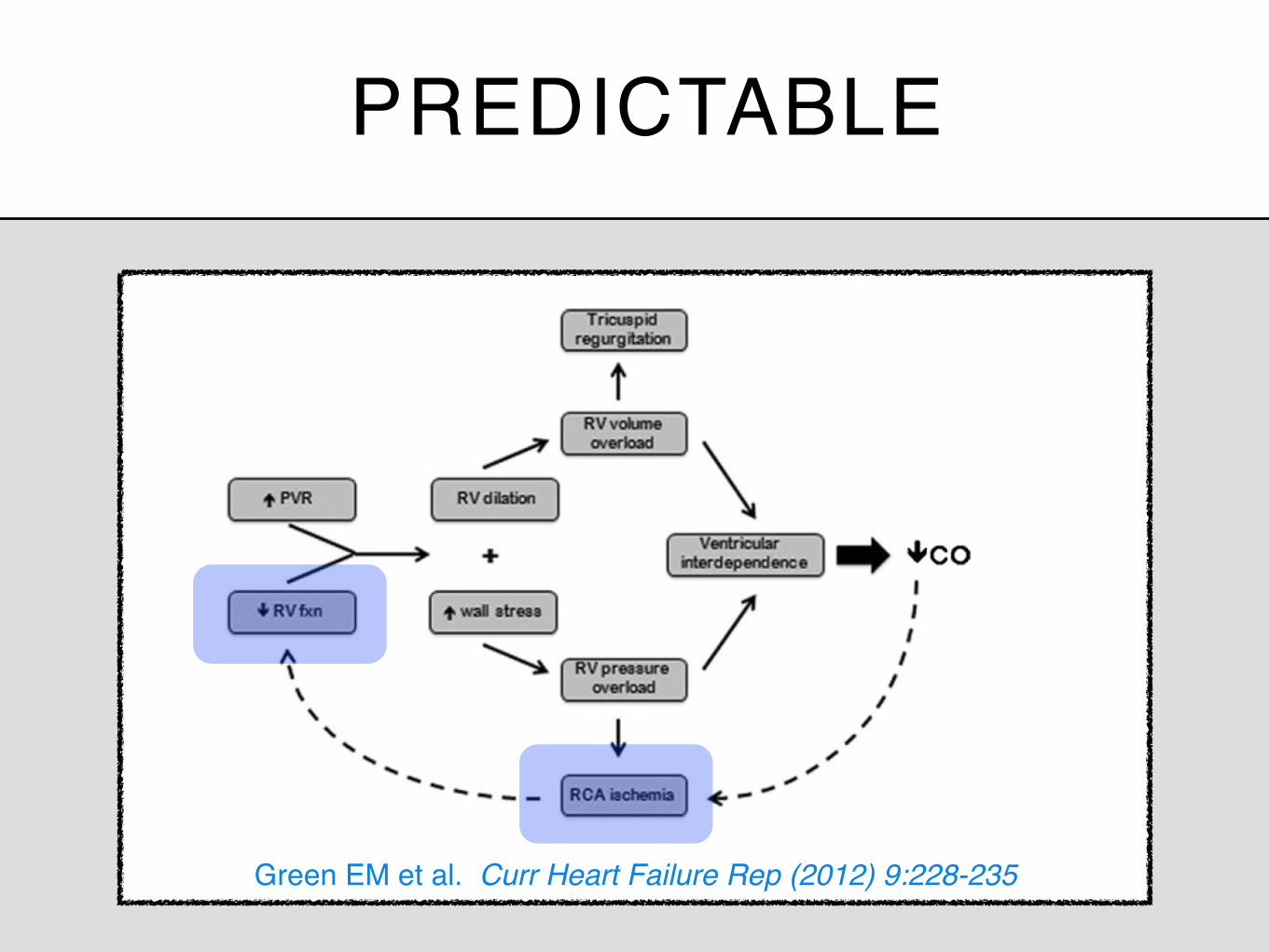
PREDICTABLE
Green EM et al. Curr Heart Failure Rep (2012) 9:228-235
1. Barbosa EJ, Jr., Gupta NK, Torigian DA, Gefter WB. Current role of imaging in the diagnosis and management of pulmonary hypertension. AJR American journal of roentgenology 2012;198:1320-31.
2. Barst RJ, Gibbs JS, Ghofrani HA, et al. Updated evidence-based treatment algorithm in pulmonary arterial hypertension. Journal of the American College of Cardiology 2009;54:S78-84.
3. Bogaard HJ, Abe K, Vonk Noordegraaf A, Voelkel NF. The right ventricle under pressure: cellular and molecular mechanisms of right-heart failure in pulmonary hypertension. Chest 2009;135:794-804.
4. Chin KM, Rubin LJ. Pulmonary arterial hypertension. Journal of the American College of Cardiology 2008;51:1527-38. 5. Goldstein JA. Pathophysiology and management of right heart ischemia. Journal of the American College of Cardiology 2002;40:841-53. 6. Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance,
and management of right ventricular failure. Circulation 2008;117:1717-31. 7. Hoeper MM, Granton J. Intensive care unit management of patients with severe pulmonary hypertension and right heart failure. Am J
Respir Crit Care Med 2011;184:1114-24. 8. Kopec G, Tyrka A, Miszalski-Jamka T, et al. Electrocardiogram for the diagnosis of right ventricular hypertrophy and dilation in idiopathic
pulmonary arterial hypertension. Circulation journal : official journal of the Japanese Circulation Society 2012;76:1744-9. 9. Ling Y, Johnson MK, Kiely DG, et al. Changing demographics, epidemiology, and survival of incident pulmonary arterial hypertension:
results from the pulmonary hypertension registry of the United kingdom and ireland. Am J Respir Crit Care Med 2012;186:790-6. 10. McGoon M, Gutterman D, Steen V, et al. Screening, early detection, and diagnosis of pulmonary arterial hypertension: ACCP evidence-
based clinical practice guidelines. Chest 2004;126:14S- 34S. 11. McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the
American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation 2009;119:2250-94.
12. Segers VF, Brutsaert DL, De Keulenaer GW. Pulmonary hypertension and right heart failure in heart failure with preserved left ventricular ejection fraction: pathophysiology and natural history. Current opinion in cardiology 2012;27:273-80.
13. van Wolferen SA, Marcus JT, Westerhof N, et al. Right coronary artery flow impairment in patients with pulmonary hypertension. European heart journal 2008;29:120-7.
14. Williams L, Frenneaux M. Diastolic ventricular interaction: from physiology to clinical practice. Nature clinical practice Cardiovascular medicine 2006;3:368-76.