74
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | anwesha-manna |
| View: | 414 times |
| Download: | 5 times |


INTRODUCTION:
DEFINITION:
Strabismus is the condition when visual axis of two eyes do not meet at the point of fixation.

COMITANT: Although misaligned they retain relation in all direction of gaze
INCOMITANT: Deviation is different in all position of gaze
TROPIA: It is manifest ocular misalignment .
PHORIA: It is latent ocular deviation.
ALTERNATE : Fixation is retained by alternate eye
UNILATERAL: Only one eye habitually fixes
INTERMITTENT: when deviation remain only for some time

Contd..
Tropia Or Phoria can be,
Esotropia /phoria
Exotropia/phoria
Hypertropia/phoria
Hypotropia/phoria
Cyclotropia/phoria

ASSESSMENT:History
Visual Acuity
Examination:
1) Examination of motor status : a) Head posture
b) Ocular deviation
c) Ocular motility
d) Diplopia
2) Examination of sensory status & adaptation
Refraction & fundoscopy

HISTORY

The age of onset
Gradual or sudden (old photographs may sometime help)
Symptoms, i.e. diplopia/ discomfort/ blurring/ eye ache/ cosmetic
Whether the symptoms occur during fatigue / illness/ stress/inattentive condition etc.
Whether it occurs for near/ distant vision
Whether it is unilateral/ alternate or constant/ intermittent.
General health ( measles, whooping cough), birth history( LBW) & family history( high refractive error, strabismus)
Previous treatment if any, & type & improvement after it.

VISUAL ACUITY

TESTING IN < 1YR AGE:
OKN test
Catford drum test
Preferential looking test
Teller acuity card test
Visually evoked potential
Indirectly by, blinking & fixation( central, steady , maintained)

TESTING IN 1-3 YRS AGE:
Cardiff acuity card test
Marble game test
STYCAR graded ballsvision test
Coin test, Miniature toytest, etc.

TESTING 3-5 YRS AGE:
Lea symbol chart
Broken wheel acuity
Sheridan- gardiner test
Tumbling E test
TESTING IN PRE-SCHOOL AGE:
Can be done by snellen’s chart/ above tests
EXAMINATION OF MOTOR STATUS:
ABNORMAL HEAD POSTURE (AHP) :
Chin elevation/ depression (vertical).
Face turn to right/ left side ( horizontal).
Head tilt to right or left shoulder (torsional).
CAUSES:
Incomitant squints
A –V phenomenon
One eyed persons

OCULAR DEVIATION:
Is it a true squint/ pseudo or apparent squint?
Causes of pseudo strabismus:
Telecanthus
Epicanthus
Hypertelorism
Ptosis
Lid retraction
Large angle κ

ANGLE KAPPA:
It is the angle subtended by the visual and optical axis and is usually about 5° (positive).

Contd…
A large positive angle κ stimulate exotropiaas in high hyperopia
A negative one stimulate esotropiaas in high myopia

TESTS TO MEASURE & DETECT OCULAR DEVIATION:
1) Cover test2) Cover- uncover test3) Alternate cover test4) Prism bar cover test5) Maddox rod test6) Double maddox rod test7) Maddox wing test8) Hirschberg’s test 9) Krimsky test 10) Bruckner test 11) 4D prism test
corneal reflection test

COVER TEST:
Fixation of eyes
Cover the apparently fixating eye
Observe the deviation of the other eye
Movement confirms manifest or true
squint(Heterotropia)

COVER-UNCOVER TEST:
One of the eyes is covered 2-3 sec
Then cover removed
In heterophoria the eye behind cover deviates
Examiner observes the movement of the on removal of cover


ALTERNATE COVER TEST:
The right eye covered for several seconds
Occluder quickly shifted to the opposite eye for 2sec
It repeats for several times
Examiner notes the recovery of eye position
Compensated heterophoria will have straight eyes, but poor control patient may show manifest deviation

PRISM BAR COVER TEST:
Prism of increasing strength is placed in front of squinting eye
Cover & alternate cover test is performed
Until the movement stops

MADDOX ROD TEST:
ORTHOPHORIA: streak passes through white light.
If streak passes on the left to the light i.e. esophoria &, if to the right then exophoria

DOUBLE MADDOX ROD TEST:
A red maddox rod is put in front of suspected eye & white in front of other eye.
Now a 6D prism is put behind white rod
The rods are kept at 90° in trial frame

Result:
Orthophoria: 2 line will be parallel
Cyclodeviation : Not parallel, red line will be inclined.
Angle can be measured by rotating the rod

MADDOX DOUBLE PRISM:
Patient will see 3 horizontal line parallel to each other.
In cyclodeviation Intermediate line will be oblique.

MADDOX WING TEST:
R/E : white arrow vertically And red arrow horizontally pointing left.
L/E :Horizontal row of figures in white and Vertical row in red

Contd…
White arrow measures horizontal tropia
Red arrow measures vertical tropia
In cyclophoria red scale is adjusted to appear parallel to horizontal scale.

HIRSCHBERG TEST:
Corneal reflections are usually symetricalin absence of squint
In esodeviationreflex fall on temporal cornea.
Roughly 1mm shift signifies 7° or 15 prism diopter.

KRIMSKY TEST:
A prism bar is placed in font of the fixating eye
The power increased
until the reflections get symmetrical.

BRUCKNER TEST:
Direct ophthalmoscope is used to obtain a red reflex simultaneously in both eyes.
In strabismus , the deviated eye will have a lighter and brighter reflex.

4 D PRISM TEST:
BIFOVEAL FIXATION:
Base-out prism placed in front R/E
For fixation B/E move to left
Then L/E move To right side to fuse image

IN LEFT MICROTROPIA:
When prism placed in front L/E no movement of either eye is seen
When moved to R/E , R/E adducts, Also the L/E Abducts
But L/E do not Adducts again to fuse image

OCULAR MOVEMENTS:
Ductions: Monocular movement
Versions: Binocular , simultaneous conjugate movement.
Vergences: Binocular, simultaneous, disjugate movement .

ACTION OF EXTRA-OCULAR MUSCLES:

9 POSITION OF GAZE:

Near point of convergence:
Nearest point on which eye can maintain binocular fixation.
Measured by RAF rule
It should be Less than 10 cm.
Near point of accommodation:
Nearest point on which eyes can maintain clear focus.
CONVERGENCE TEST:
Hold a pencil / a finger at distance of 30-40cm
Ask the patient to look at its tip
Bring it nearer to patient’s eyes.
kept at the eye level of patient till the eye develops
Diplopia or one eye Deviates

FUSIONAL AMPLITUDE:
It is the efficacy of vergence movements.
It is done by increasing prism dioptre.
Vertical fusional reserve: 1.5°-2.5°
Horizontal negative fusional reserve
(abduction range): 3°-5°
Horizontal positive fusional reserve
(adduction range) : 20°-40°

PRISM VERGENCE TEST:
Patient at 6m distance from light source
The highest Prism that permits single vision gives
Verging Power

TESTS FOR DIPLOPIA:
Diplopia charting
Hess screen test
Lees screen test
PARK’S 3 step test
Forced duction test

DIPLOPIA CHARTING:
Maximum separation is in the quadrant in which the muscle acts most
The level of 2 image
In which direction the image is deviated (image displaced toward the direction of action of the muscle)

LEFT LATERAL RECTUS PALSY:

HESS CHART:
Patient is asked to superimpose green light on the red light.
Procedure repeated with red filter in front of left eye.
The points are marked by examiner.
RESULT:
In orthophoria: both lights superimpose in 9 position of gaze.

Rt 6th nerve palsy:

R/E 4th nerve palsy:

LESS SCREEN:
Consists of two opalescent glass screens at right-angles to each other, bisected by a two-sided plane mirror which dissociates the two eyes
interpretation done as like hess chart

PARK’S 3 step test:
Use to identify cyclovertical muscle paralysis.
Performed by measuring the vertical alignment in
1)primary position,
2) In right and left gaze and
3) In head tilt to the right and to the left.

RIGHT HYPERTROPIA:
1) Circle the muscles which pull R/E down or L/E up

2) Determine whether vertical deviation is more on left/ right gaze
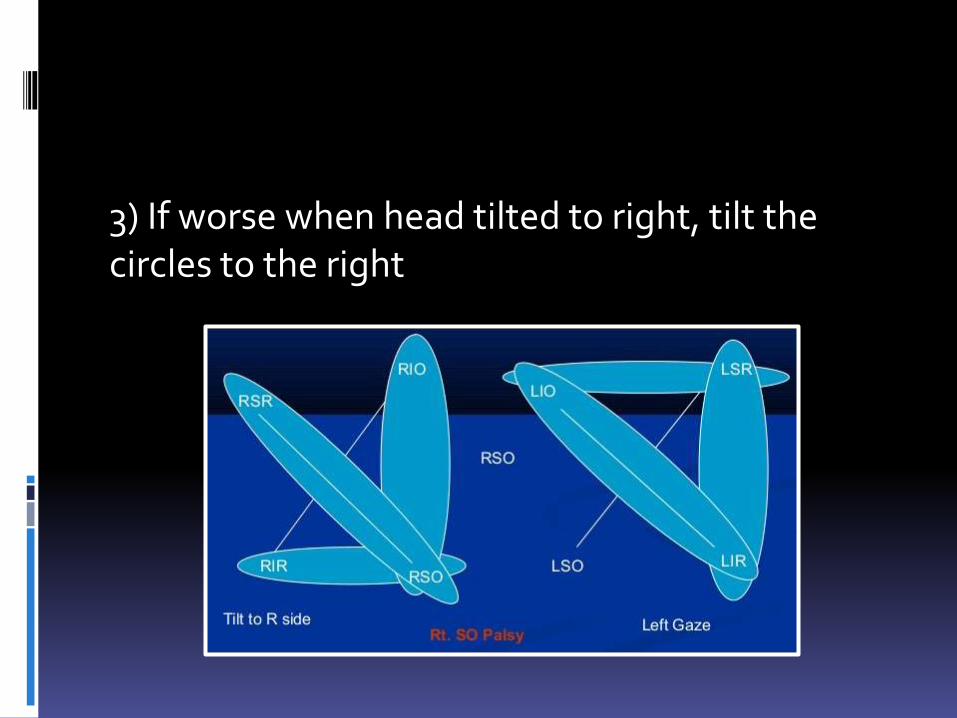
3) If worse when head tilted to right, tilt the circles to the right

FORCED DUCTION TEST:Anesthetize the eye
Lids retracted
Patient looks in the direction of
the muscle tested
Globe hold at the opposite limbuswith globe holding forceps
Eye is rotated at the direction of action of muscle

Contd..
RESULT:
If free movement is present then the test is negative
If restricted then the test is positive

EXAMINATION OF SENSORY STATUS:
Binocular vision & its grade
Type of Retinal correspondence
Suppression
It Determines prognosis in a case of squint.

GRADES OF BINOCULAR VISION:
1) First grade (simultaneous perception):
2) Second grade (Fusion):
3) Third grade (stereopsis)

SUPPRESSION:
It is active inhibition of image of one eye by the visual cortex, when both eyes are open.
Stimuli :
Diplopia
Confusion of image
Blurred image
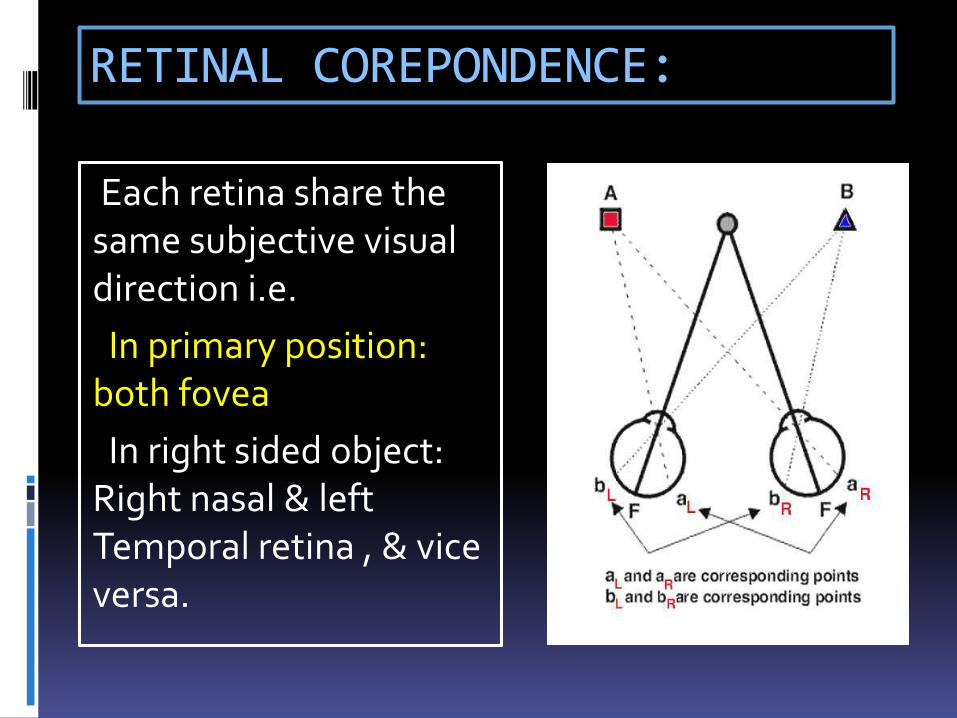
RETINAL COREPONDENCE:
Each retina share the same subjective visual direction i.e.
In primary position: both fovea
In right sided object: Right nasal & left Temporal retina , & vice versa.

Abnormal retinal correspondence:
Abnormal retinalcorrespondence is acondition in which non-corresponding retinalelements acquire commonsubjective visual direction.

TESTS FOR SENSORY STATUS:
1) Bagolini’s striated glass test
2) Worth four dot test
3) After-image test
4) Synoptophore
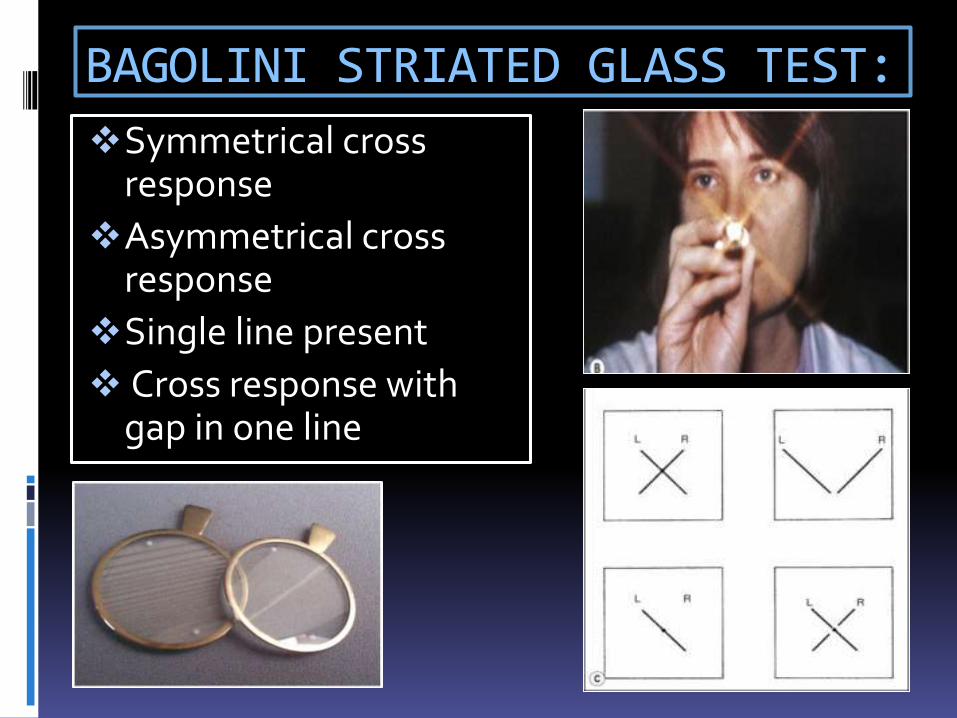
BAGOLINI STRIATED GLASS TEST:
Symmetrical cross response
Asymmetrical cross response
Single line present
Cross response with gap in one line

WORTH FOUR DOT TEST:
All 4 lights seen –NRC/ Harmonious ARC
Left suppression – 2 red light
Right suppression – 3 green light
Diplopia – 3 green & 2 red light
Alternating suppression –Alternate green & red light.

AFTER-IMAGE TEST(HERING-BIELSCHOWSKY ):
A bright linear light is used
Patient views the target with one eye and the light is flashed
For R/E flash held vertically & for L/E horizontally
Patient appreciate a plus sign.

Contd…
a) is consistent with normal retinal correspondence (NRC), (b) shows uncrossed after-image(diplopia) and anomalous retinal correspondence (ARC) and (c) shows left supression

SYNOPTOPHORE:
It is an instrument ,used for potential for binocular function in presence of manifest squint, & tests SP, FUSION, STEREOPSIS

TESTS FOR STEREOPSIS:
1) TNO TEST
2) FRISBY TEST
3) LANG TEST
4) TITMUS TEST

TNO RANDOM DOT TEST:
Consists of seven plates of randomly distributed paired red-green dots.
Test targets are only visible to individuals who have stereopsis .

FRISBY TEST:
Consists of 3 transparent plates of, each printed with 4 squares.
1 of the squares contains a hidden circle, & the random shapes are printed on the reverse side.
Patient needs to find out the hidden circle.
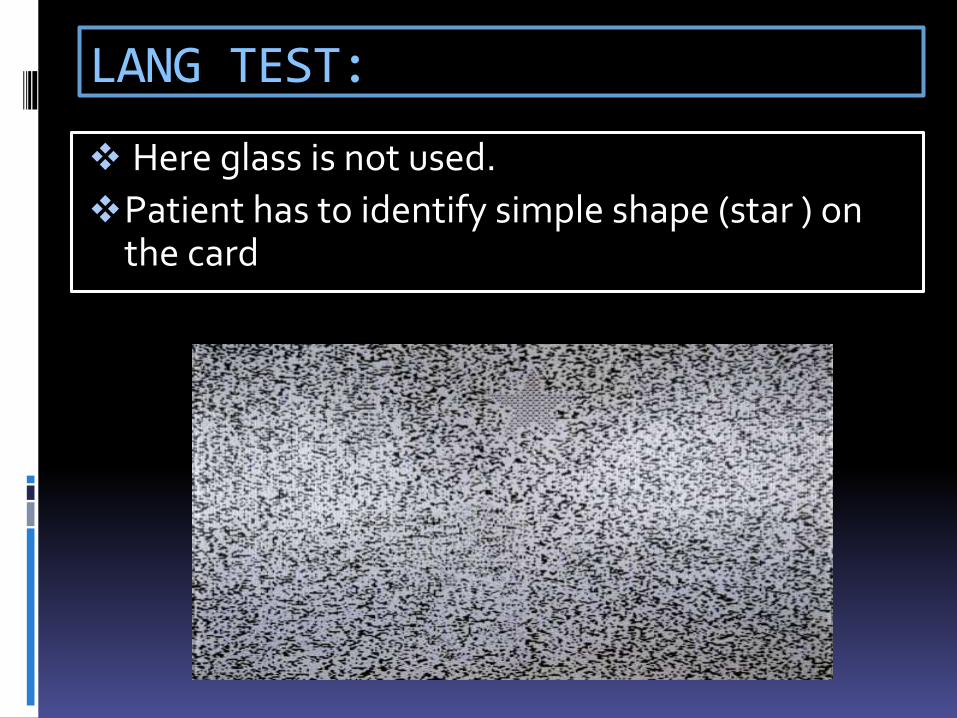
LANG TEST:
Here glass is not used.
Patient has to identify simple shape (star ) on the card

TITMUS TEST:
Viewed through polaroid spectacle
Right plate contains a picture of fly
Left contains 9 squares, each containing 4 circles, of which 1 has disparity
test done at 40cm distance

Contd…
FLY: Appears to stand out from page
CIRCLES: 1 circle form disparity & appear forward.
THE ANIMALS : 3 rows of animal ,one of which appear forward.

Fundoscopy & refraction:
Dilated fundoscopy is mandatory.
To exclude any underlying ocular pathology such as macular scarring, optic disc hypoplasia or retinoblastoma.
Proper Refractive correction should be given by retinoscopy
CONCLUSION
It is a common childhood & adult problem.
It is extremely difficult to examine a child and a tactful examination is to be done.
Quantification of the angle of deviation, binocular vision, ocular movement, refraction is important for diagnosis & proper treatment purpose.


















