92
ASSIGNING THE PRINCIPAL DIAGNOSIS Mary Ann P. Leonard, RHIA, RAC-CT AHIMA ICD-10-CM Approved Trainer/Ambassador Health Information Professionals 610-291-9210 [email protected]
ASSIGNING THE PRINCIPAL DIAGNOSIS
Mary Ann P. Leonard, RHIA, RAC-CTAHIMA ICD-10-CM Approved Trainer/AmbassadorHealth Information [email protected]

CONFLICT OF INTEREST
CONTINUING EDUCATION CONTACT HOURS
There is no conflict of interest in the
presentation of this program.
The certificate for the Continuing
Education contact hours will be
provided after completion of the
program evaluation tool.

Official Coding Guidelines
ICD-9-CM Official Guidelines for Coding & Reporting
Developed by: Centers for Medicare & Medicaid
Services (CMS) National Center for Health Statistics
(NCHS)
Approved by the Cooperating Parties
CMS NCHS American Health Information
Management Association (AHIMA) American Hospital Association
(AHA)
Published on Center for Disease Control & Prevention (CDC) web site
Must be followed per HIPAA Transaction &
Code Set (TCS) rule and per Section I
coding instructions in the RAI manual
Developed to assist in coding and reporting
situations where the ICD-9-CM code book
does not provide direction Instructions
published in code book take precedence
over any guidelines
Official Coding Guidelines

LTC PAYMENT SYSTEM
Skilled Nursing Facility Prospective Payment System (SNF PPS)
Per Diem Payment
Covering All Costs for Services Furnished to Medicare Beneficiaries under Part A
Including Routine, Ancillary and Capital Costs <BBA 1997>

Resource Utilization Groups
A case mix system in which payment is based on the resources expected to be used to care for the resident

How Payment Rates are Determined
Reimbursement is Determined by Resource Utilization Group (RUG) that Results from Coding of the MDS Assessment
MDS Assessment Coding Results from Medical Record Documentation of Resident Care Items
The RUG Level is Transferred to the Claim Form (UB-04)

RUG III Classification
Categories
Rehabilitation plus Extensive Services
Rehabilitation
Extensive Services
Special Care II
Special Care I
Clinically Complex
Impaired Cognition
Behavior
Reduced Physical Function
Resource Utilization Groups
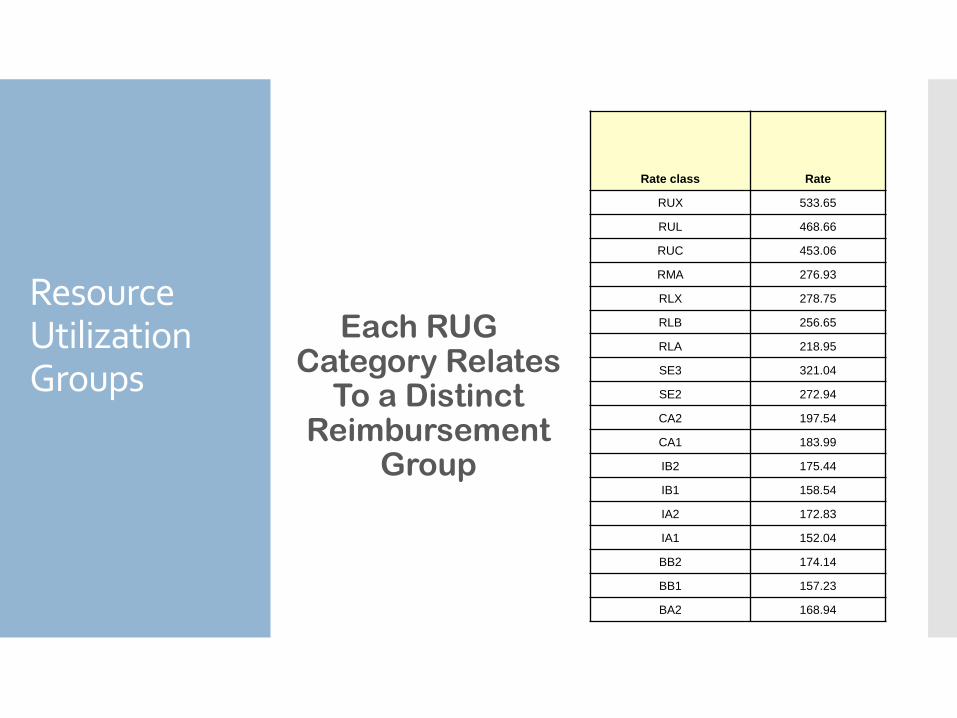
Each RUG Category Relates
To a Distinct Reimbursement
Group
Rate class Rate
RUX 533.65
RUL 468.66
RUC 453.06
RMA 276.93
RLX 278.75
RLB 256.65
RLA 218.95
SE3 321.04
SE2 272.94
CA2 197.54
CA1 183.99
IB2 175.44
IB1 158.54
IA2 172.83
IA1 152.04
BB2 174.14
BB1 157.23
BA2 168.94
Resource Utilization Groups
Per Diem Reimbursement
Rate
The Payment Rate Includes all Services Provided to a Resident during a Part A Stay for Medicare
Exception: Services Excluded Under Consolidated Billing

Importance of Accurate Diagnosis Coding
Medicare Billing
Accuracy of MDS and RUG Category
Quality Measures

Diagnosis Code Reporting
Plays a Significant Role in the Completion of both the MDS Form and the UB-04.

Relationship
UB-04
Medical RecordMDS
Organization:Section I – ICD-9-CM
A. Conventions
B. General Coding Guidelines
C. Chapter-specific Guidelines
Applies to all care settings
Official Coding Guidelines
Official Coding Guidelines
Organization cont.:Section II - Selection of Principal
Diagnosis Applies to all inpatient care
settings including LTC. Principal diagnosis is defined in
Uniform Hospital Discharge Data Set (UHDDS) as the condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care.

Official Coding Guidelines
Organization cont.: In LTC where claims are submitted for
extended stays, the principal diagnosis listed may change to the reason for which the resident remains in the facility.
Following transfer to the hospital with an anticipated return to the facility, the principal diagnosis will be:
The “primary” reason that the resident is returning or remaining in the facility.
This may not be the reason for Medicare coverage.

Organization cont.: Section III - Reporting
Additional Diagnoses Applies to all inpatient
care settings including LTC.
The definition for “other diagnoses” is interpreted as additional conditions that affect patient care in terms of requiring: clinical evaluation; or therapeutic treatment; or diagnostic procedures; or extended length of hospital stay; or increased nursing care.
Official Coding Guidelines

Organization cont.:Section IV - Diagnostic Coding
and Reporting Guidelines for Outpatient Services
These guidelines are for use by hospital-based outpatient services and provider –based office visits.
These guidelines are not used in LTC
Official Coding Guidelines
Section I, General Coding Guidelines –Coding Signs & Symptoms
Use signs & symptoms codes when:
A related, definitive diagnosis has not been established
Symptoms are not routinely associated with a disease process
Do not code signs and symptoms that are part of the disease process
Official Coding Guidelines

Section I, General Coding Guidelines –Multiple Codes for Single Condition
Some diagnoses require more than one code number to correctly identify the condition
Instructions in the Alphabetical Index or Tabular List identify need for additional codes
Generally, the second code is listed in italics.
Examples:
Alzheimer’s Dementia 331.0 [294.11]UTI due to E. coli 599.0 [041.49]
Official Coding Guidelines
Section I, General Coding Guidelines -Combination Codes
A single, combination code can identify:
Two diagnoses
A diagnosis with an associated secondary process (manifestation)
A diagnosis with an associated complication
If the code fully identifies the conditions involved, assign only the combination code
Examples:Asthma with COPD 493.2Peptic ulcer with GI bleeding 533.40
Official Coding Guidelines
Section I, General Coding Guidelines –LATE EFFECT
Residual condition (sequela)
Condition that remains after acute phase of an illness
Sequenced first unless otherwise instructed
Cause of sequela listed second
Do not use code for the acute phase of illness
Example:Dysphasia following CVA 438.12
Official Coding Guidelines

Section I, General Coding Guidelines
-Reporting Same Diagnosis Code More Than Once
Each unique ICD-9-CM diagnosis code may be reported only once for an encounter.
This applies to bilateral conditions or two different conditions classified to the same ICD-9-CM diagnosis code.
Official Coding Guidelines

Where To Find Diagnoses
The diagnosis is identified by the treating provider
Consultants may provide additional diagnoses but these must be reviewed/approved by the attending physician
If there is a conflict in diagnoses, the attending provider’s documentation supersedes consultants
If the attending provider is silent regarding the condition documented by another treating provider, it is NOT a conflict

Where To Find Diagnoses
Review clinical record, including but not limited to:
Discharge SummaryMD progress notesConsultationsH & POrders
NOTE: the diagnosis must originate with those authorized to diagnose (physician, physician extender) diagnoses cannot be interpreted or assumed
Coding Process in LTC
Create a listing of diagnoses and codes Select principal diagnosis and list
first
The “first listed diagnoses” is the diagnoses that is chiefly responsible for the admission to, or continued residence in, the nursing facility and should be sequenced first.
List additional diagnoses that reflect services provided or clinical conditions (treated, monitored or carry a risk of death)
Coding Process in LTC
Do not list diagnoses that are not pertinent to nursing facility stay
Do not list diagnoses that have been resolved or are historical unless clinically significant to staff
Do not code conditions documented as “suspected”, “rule out”, and/or “probable”
Only established diagnoses are coded in LTC

Coding Process in LTC
Subsequent Admissions (Readmits)
Following transfer to the hospital with anticipated return to the facility, the principal diagnosis will be:
The “primary” reason that the resident is returning or remaining in the facility.
This may not be the reason for Medicare Coverage
Coding Clinic, 4th quarter, 1999.

Coding Process in LTC
Example:
A nursing home resident is transferred to the hospital for treatment of pneumonia. She returns to the nursing home and is still receiving antibiotics for the pneumonia. However, the main reason she is returning to the nursing home is because this has been her residence since developing a CVA with residuals several years ago.
Which diagnosis should be listed first at the nursing home, the pneumonia or sequela of CVA?
LATE EFFECT of CVA

Code Sequencing Definitions in LTC
Secondary diagnoses for LTC:
Any and all conditions that co-exist when resident is admitted to the facility, or
Develop subsequently during a resident’s stay, or
Affect treatment the resident receives or the resident’s length of stay
Diagnoses that relate to an earlier episode which have no bearing on the current stay are to be excluded.
Coding Process in LTC
Review diagnosis list with clinical staff as applicable:
Nursing representative (MDS or other)
Therapy
Inclusion of therapy treatment and medical diagnoses
May want to label treatment diagnoses/ codes from therapy

Coding Process in LTC
Best practices for when to assign codes (or at least review them):
Long-term care residentsUpon admission &
readmissionWhen new diagnoses
ariseQuarterly (with MDS
schedule)
Coding Process in LTC
High acuity residents (i.e. Medicare, skilled or managed care)
Review codes monthly
Codes on MDS, billing claim forms (i.e.
UB04/837), and in medical record
need to support:
Medical necessity
Skilled services provided (may
include therapy treatment diagnosis)
Resource Utilization Group (RUG)
selection as applicable
Coding Process in LTC
Triggers for concurrent coding: Change, addition or
discontinuations of therapy services
Recent hospitalization
New diagnoses documented by the medical staff
Significant changes in condition
Resolved diagnoses
Changes in medication – new or discontinued

Use of Diagnoses on the RAI/MDS
Use of Diagnoses on the MDS
Diagnosis information captured on the Minimum Data Set (MDS) in Section I - Disease Diagnoses
Diseases: check-off list of common diagnoses
Infections: check-off list of common infections
Other Current or More Detailed Diagnoses and ICD-9 Codes – text area for listing diagnoses with ICD-9-CM codes
Use of Diagnoses on the MDS
Instructions for completing MDS Section I are found in Chapter 3, Long Term Care Resident Assessment Instrument User’s Manual, Version 3.0
Manual available for download from:
http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/NursingHomeQualityInits/MDS30RAIManual.html
Use of Diagnoses on the MDS

Use of Diagnoses on the MDS
Review clinical record for current, physician-documented diagnoses
Transfer documentation, including hospital progress notes and discharge summary
Physician medication and treatment orders
Follow Official Guidelines for Coding and Reporting

CURRENT within the look back period
Documented within the past 60 days
Active within the last 7 days
Have a CURRENT relationship to:
Activities of Daily Living (ADL) status
Cognitive status
Mood and Behavior status
Medical Treatments
Nursing Monitoring - includes clinical monitoring by a licensed nurse (e.g., serial blood pressure evaluations, medication management, etc.)
Risk of Death
Use of Diagnoses on the MDS

Do NOT list
Conditions that have RESOLVED or
INACTIVE diagnoses that no longer affect the resident’s function or care plan
Examples:
Resolved pneumonia
History of appendectomy
Use of Diagnoses on the MDS
When diagnosis is more specific than item description in Section I:
Check the more general diagnosis in Section I and
Enter more detailed diagnosis, with ICD-9-CM code, in I8000 if space available
Example:Gouty Arthritis:
I3700 - Check item I1l, arthritis
I8000 - Enter “Gouty Arthritis
Use of Diagnoses on the MDS

Process for Question I2 - Infections Using a 30-day look back for UTIs,
and a 7-day look back period for all other items
Check all infections that apply in I2300
Watch for very specific criteria for UTIs
Code more specific diagnoses in I8000 if space available
Use of Diagnoses on the MDS
DO NOT report procedure codes in Section I
Procedure codes not used in LTC
Results in “fatal error” (record rejection) when submitting an MDS
DO NOT report code on Section I if already captured in other sections of the MDS (Therapies, g-tube, etc.) – do code them as they would appear on the UB-04 form
Use of Diagnoses on the MDS

Section I and RUGs Classification Diagnoses reported in Section I can affect
classification in Resource Utilization Groups (RUGs) used to determine Medicare and/or Medicaid payment rates
I2000 – Pneumonia
I2100- Septicemia
I2900 – Diabetes mellitus
I4400 - Cerebral palsy
I4900– Hemiplegia/hemiparesis
I5200- Multiple sclerosis
I5300 – Parkinson's Disease
I5100– Quadriplegia
I6200 – Asthma & COPD
I6300 – Respiratory Failure
Use of Diagnoses on the MDS

Use of Diagnoses on the MDS
Section I and MDS Assessments Completed for Medicare PPS
Diagnoses and conditions entered on the Medicare PPS assessments should be reflective of ICD-9-CM codes on the UB04/837 for the same time period
Medicare PPS Assessments:
5-day
30-day
90-day
14-day
60-day
OMRA
Medicare Readmission/Return
Section I and quarterly MDS Assessments Each state determines which of the
MDS assessment forms are required for the quarterly assessment
MDS Full Assessment Form
Medicare PPS Assessment Form (MPAF)
MDS Quarterly Assessment Form
MDS Quarterly Assessment Form (Optional Version for RUG IV)
MDS Quarterly Assessment Form (Optional Version for RUG IV)
Use of Diagnoses on the MDS

Section I and the Quarterly MDS Assessment
Report diagnoses based on instructions printed at Section I
Some quarterly MDS forms have the following instruction for Section I "Include only those diseases documented in the last 60 days and active in the last 7 days that have a relationship to current ADL status, cognitive status, mood or behavior status, medical treatments, nursing monitoring, or risk of death".
Use of Diagnoses on the MDS
Use of Diagnoses on the MDS
Section I and Quality Measures Diagnoses in Section I affect
inclusion, exclusion, and risk adjustment of residents in Quality Measures
I6000 – Schizophrenia
I5350 – Tourette’s Syndrome
I5250 – Huntingdon’s Disease
I2300 – UTI within the last 30 days

Diagnosis Codes on the UB-04 /837
Support reimbursement of claims
Serve as a means of communication between the provider & payer
Describe the conditions that qualify for reimbursement
Support medical necessity
Diagnosis Codes on the UB-04 /837

MYTH
The 1500 claim form (aka- HCFA 1500 or CMS 1500 form) is developed by the federal government
FACT
The 1500 form is developed and maintained by the National Universal Claim Committee (NUCC)
The form is in the public domain
The form is used by federal payer programs, e.g. Medicare, Tricare, Black Lung, etc.
Diagnosis Codes on the UB-04 /837
The NUCC was formed in 1995 taking over for the Uniform Claim Form Task Force that initially developed the standard professional claim form
NUCC assumed responsibility for the development and maintenance of the 1500 claim form
Its members represent a broad base of payers, providers, standards developers, data content committees, public health organizations and vendors
The AMA is the Secretariat of the NUCC
The website is www.nucc.org
Diagnosis Codes on the UB-04 /837

Some of the changes to the form:
Added 8 more diagnoses
Added ICD indicators and two dotted lines for 1-byte indicator
Can use either ICD-9-CM or ICD-10-CM (not both) on the form
Changed labels of the diagnosis code lines to alpha characters (A-L)
Removed the period within the diagnosis code lines
Diagnosis Codes on the UB-04 /837
CMS -1500 Claim FormRecently revised (version2/12)
Replaces version 8/05
New form accepted 1/6/14
Medicare will accept only the new form 4/1/14
Allows providers to indicate whether using ICD-9 or ICD-10 codes
Additional diagnoses\is codes from 4 to 12
Diagnosis Codes on the UB-04 /837

List diagnosis codes that support services provided during claim dates of service
Items/services billed on the UB-04/837 should be supported by a diagnosis code
Follow Official Guidelines for Coding and Reporting and instructions within the code book to sequence and report diagnoses codes as necessary.
Diagnosis Codes on the UB-04 /837

Diagnosis Codes on the UB-04/837: CMS Transmittal 437
Chapter 6, Section 30 of the Medicare Claims processing manual includes the following:
Principal Diagnosis Code- Code must be reported according to Official ICD-9-CM Guidelines
Other Diagnosis Codes Required-Enter 8 additional diagnoses - CMS does not have additional requirements regarding reporting or sequencing of codes other than those in the guidelines

Diagnosis Codes on the UB-04/837
Recommendations: Create a list of diagnoses and codes
upon admit, readmit and as needed (condition change, MDS schedule, billing cycle)
HIM review diagnoses list with nursing and therapy as applicable
Discuss diagnoses in Medicare or other appropriate meeting, finalize diagnosis sequencing
Diagnosis Codes on the UB-04/837
Recommendations:Communicate diagnoses
selected/sequenced to:
Business office – for inclusion on billing claim form (i.e. UB-04/837)
Medical record – for continuity of care
Others as appropriate for your facility

Diagnosis Codes on the UB-04/837
Sample Coding Sequencing & Communication Form

Accurately Reporting ICD-9-CM Codes
Accurate reporting of ICD-9-CM codes affects:
Accurate claim submission (e.g. Medicare)
Quality Measures
Data collected for long term care residents
Overall accuracy of your MDS/RUG categories

Accurately Reporting ICD-9-CM Codes
Report correct & complete diagnosis code numbers
Report correct number of digits Assign 4th, 5th, 6th or 7th digits as
required
NEVER add zeros or nines as “fillers” to an ICD-9-CM code
Changes the meaning of diagnosis
NEVER use a code because it ‘goes through the system’

Accurately Reporting ICD-9-CM Codes: MDS vs Billing Claim Forms
Not all diagnoses reported on MDS are appropriate for billing claim forms (i.e. UB-04/837)
Some diagnosis codes on MDS do not relate to reasons for claim coverage
Keep in mind time frame of MDS vs. billing claim form
Accurately Reporting ICD-9-CM Codes: Billing Claim Forms
Inaccurate and/or incomplete codes can prompt a suspension or rejection of a claim
Inaccurate codes can cause denials or medical reviews
Each FI determines diagnoses to be targeted
Remember the RACs, etc. also use codes to determine audits

Accurately Reporting ICD-9-CM Codes: Billing Claim Forms
Examples of diagnoses targeted for medical review in the past:
Bowel Obstruction
Dementia
Best defense is accuracy in the ICD-9-CM code assignment
ICD-9-CM in Long Term Care is Dynamic
Diagnosis Codes in the Long Term Care Facility are Dynamic. Diagnosis codes
listed depended upon the point in time of the resident’s stay when the coding is done.
Many Facilities Fail to Update the Resident’s List of “Active” Diagnoses
What Diagnosis Codes to List?
Create a List of Diagnoses and codes when appropriate
Upon:
Admission
Readmission
Change in Patient Status
MDS Schedule
Billing Cycle

Report Correct and Complete Codes
Code to the Highest Level of Specificity
Do Not Add Filler Numbers
Report Appropriate ICD-9-CM codes on the UB-04
Not All Diagnoses on the MDS Form are Appropriate to the UB-04.

Listed Diagnoses Codes
List Codes that Support Services Provided during the Dates of Service Reported
Items/Services Billed Should be Related to a Diagnosis Code

Finding the Diagnoses
The Clinical Record is Reviewed for Current Physician (Physician Extender)-Documented Diagnoses.
Transfer Documentation
Physician Medication and Treatment Orders

Current Diagnosis
The Disease or Condition is CURRENT within the Look Back Period
Diagnoses must be documented within the previous 60 days (based on the ARD)
Diagnoses must be ACTIVE within the past 7 days (based on the ARD)
Current Diagnosis
A Current Relationship Must Exist the Diagnoses/Conditions and:
Activities of Daily Living
Cognitive Status
Mood and Behavior Status
Medical Treatments between
Nurse Monitoring
Risk of Death

Disease Conditions
Do Not Report:Conditions That Have Been Resolved
Inactive Conditions:
Those that No Longer Affect:
the Resident’s Functioning
The Resident’s Care Plan

Importance of Communication
Communicate Final Diagnosis Listing/Sequencing with the Business Office, Medical Records and Others as Appropriate
V57.89
438.20V54.89
Diagnosis Coding and the UB-04
Importance: Support Reimbursement
Communication Between Payer and Provider
Describe Conditions and Disease
Support Medical Necessity

ICD-9-CM Reporting GuidelinesCMS Transmittal 437
First Listed Diagnosis Code –Reported According to the Official ICD-9-CM Guidelines
CMS Does Not have Additional Requirements for Reporting or Sequencing other Diagnosis Codes

ICD-9-CM CodesMDS and the Claim
A Correlation Should ExistHowever, Not all Diagnoses Entered on the MDS are Reported on the UB-04
Is the Condition Related to Medicare Coverage?

Acute Care Codes and LTC
Acute Care Codes are Not to be Used in the Long Term Care Setting Unless the Condition or Disease Manifests or is Treated while the Resident is in the Facility
Common Errors Pulling Acute Fracture or
Dehydration Diagnoses from Transfer Documentation

Reporting Fracture Codes
Only Report Fracture Codes (800.XX-829.X) if the Fracture Occurs in Your Facility!
The Fracture Must be Stabilized and Treated in Your Facility
If a Resident is Admitted for Rehab following the Fracture an Aftercare Code is Reported
Determine whether the Fracture is Traumatic or Pathologic to Assign the Correct Code
Consult Physician Documentation to Make the Determination

V-Codes and Long Term Care
Supplementary Classification of Factors Influencing Health Status and Contact with Health Services
Guidance for the Use of V-Codes Section I General Coding
Guidelines
AHA Coding Clinic, 4th Quarter 1999, 4th Quarter 2003
Coding Guidelines for Long Term Care
Medicare Claims Processing Manual, Transmittal 437

Using V Code in Long Term Care
Reason for the Resident’s Stay
Rehab Services (V57)
Orthopedic Aftercare (V54)
Surgical Aftercare (V58)
Assign the Appropriate V-Code as the First Listed Diagnosis

V Codes In Long Term Care
Other V Codes can be used as a “First Listed” Diagnosis
The Following are Generally Used as Secondary Diagnoses in LTC
Attention and Management of Artificial Openings (V55)
Acquired Absence of Organ (V45.7X)
Monitoring Therapeutic Drug Uses (V58.83)
V Codes In Long Term Care
In Extremely Rare Circumstances the Following Could be used as a “First-Listed” Diagnoses:
“Status Post” or “History” V Codes
Must Impact the Resident’s Care
Family History (V16-V19)
Personal History Codes (V10-V13)

V Codes In Long Term Care
Only to be Listed as Secondary Diagnosis:
Amputation Status (V49.6X or V49.7X)
Drug Resistance Present (V09)
Hospice (V66.7)
Long Term (Current) Drug Use (V58.6X)
Organ Replacement Status (V42 or V43)
Personal History Codes (V14-V15)
V Codes and the Alphabetic Index
Look for Key Words
Absence
Aftercare
History of
Resistance
When Coding Scenarios
Determine a List of Diagnosis Codes
Utilize Transfer Documentation
Physician Treatment and Medication Orders

Coding Scenarios
What’s the correct principal or primary diagnosis?
Patient admitted from hospital following an elective total Right hip replacement for DJD. During the hospital stay the patient was transfused with 2 units of blood for acute blood loss anemia and continued to be anemic on iron supplements. Following surgery, the patient was placed on Coumadin until such time the patient was ambulatory for DVT prophylaxis. Patient was sent with orders for PT and OT, check PT/INR 2 x week, and CBC in 2 weeks.
Aftercare following joint replacement

Coding Scenarios
What’s the correct principal or primary diagnosis?
Patient admitted to hospital with slurred speech, facial droop, cognitive loss and dysphagia which was diagnosed as a result of an acute embolic CVA. Patient has ongoing diagnosis of HTN and hyperlipidemia. Prior to discharge from hospital a PEG tube was placed as speech therapy identified oropharyngeal dysphagia. It was noted that rather than placing the patient on Coumadin the patient was placed on Plavix due to history of falls with multiple fractures in the recent past. Patient will be treated with PT, OT, SLP and swallowing therapy at the nursing home.
Late effect CVA, cognitive loss

Coding Scenarios
What’s the correct principal or primary diagnosis?
Resident with PVD secondary to Type I diabetes mellitus with diabetic ulcers of right ankle and calf. Focus of care is on the ulcers.
Diabetes Mellitus Type I with
vascular

Coding Scenarios
What’s the correct principal or primary diagnosis?
Patient was hospitalized for a below-the-knee amputation of the left leg. Following surgery, he developed an infection of the amputation stump which was treated during the hospitalization and the antibiotics were complete at the time of discharge. The patient is now admitted to the nursing facility for dressing changes.
Orthopedic aftercare, following
amputation
Coding Scenarios
What’s the correct principal or primary diagnosis?
Resident admitted to SNF following right lobectomy and excision of sentinel lymph node with metastasis to lymph node. Resident will return in 2 weeks to surgeon for tumor clinic findings to start chemo and radiation therapy.
Aftercare following neoplasm
surgery
RESOURCES
Coding Guidelines; http://www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm#guidelines
http://www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm#guidelines
MDS 3.0 Manual; http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/MDS30RAIManual.html
http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/NHQIMDS30-ArchivedRAIManuals.html
RESOURCES
Medicare Policy Manuals
http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS050111.html?DLPage=1&DLSort=0&DLSortDir=ascending
http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS012673.html?DLPage=1&DLSort=0&DLSortDir=ascending
http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS018912.html?DLPage=1&DLSort=0&DLSortDir=ascending
http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS019017.html?DLPage=1&DLSort=0&DLSortDir=ascending

















