Page 1
Group Members Portland State University Advisor
Fahad Aldakheel Dr. Dave Turcic
Chad Knutsen Portland State University Instructor
Melanie Ferguson Dr. Sung Yi
Hamid Tavazoie Industry Advisors
Evan Topinka Gregg Meyer, MME
Dieterich Steinmetz, M.D.
Amy Walker, MPT
Winter2014
PORTLAND STATE UNIVERSITY | Mechanical Engineering Dept.
Assistive
Exercise
Machine for
Post Stroke
Rehabilitation
Page 2
EXECUTIVE SUMMARY
Myoelectric Robotic Orthosis is a device created for Stroke Survivors. It senses the brain
signal to a muscle group to power a pulley system connected to the person to assist in therapeutic
activities. Our team designated a list of constraints to follow when creating the device, and have
since made modifications to that list. From research, interviews, and testing, we have made
changes to what our top priorities are.
This progress report discusses what our new priorities are, as well as comparing our
original goals with our new ones. We will evaluate our progress and delve deeper into our
internal and external research. Without a company to fund us or look up to for answers and
evaluation, we rely on the consumer to guide us through this process.
Page 3
Contents
INTRODUCTION ............................................................................................ 4
MISSION STATEMENT .................................................................................. 4
PROJECT PLAN ............................................................................................ 5
PRODUCT DESIGN SPECIFICATION SUMMARY ................................................... 6
EXTERNAL SEARCH ...................................................................................... 7
INTERNAL SEARCH ....................................................................................... 8
DESIGN EVALUATION & SELECTION ................................................................ 8
DETAILED DESIGN PROGRESS ....................................................................... 10
CONCLUSION ............................................................................................ 12
APPENDIX ................................................................................................ 13
REFERENCES ............................................................................................. 24
Page 4
INTRODUCTION According to the National Institute of Neurological Disorders and stroke, there are
approximately 4 million Americans living with the effects of stroke(1)
. Many stroke survivors
suffer from weakness (hemiparesis) or paralysis (hemiplegia) on one side of their body affecting
the use of their limbs. Therefore, Myoelectric Robotic Orthosis is medical device that will help
stroke survivors regain the ability of moving their limbs in a rapid amount of time compared with
current physical therapy methods. Basically, this medical device is an exercise machine that uses
advanced technology to detect the voltage signals via Biopotential electrode sensors in the
Electromyography (EMG) Amplifier. In other words, EMG measures muscle response or
electrical activity in response to a nerve’s stimulation of the muscle. Most medical researchers
use EMG to test if muscles and nerves are working correctly(2)
. However, in this project it’s
important to take advantage of the muscle electrical activity and use it as input for the motor.
Therefore, electrical signals will be amplified and used to function the device. Figure 1 shows
the five main processes in the device.
MISSION STATEMENT Designing this medical device will develop the method of integrating technology with physical
therapy. It will help stroke survivors relearn skills that are lost when part of the brain is damaged.
Also, it will help them to become as independent as possible in a rapid amount of time compared
to traditional physical therapy exercises. The ultimate goal is to deliver the final product by the
end of Spring 2014.
Page 5
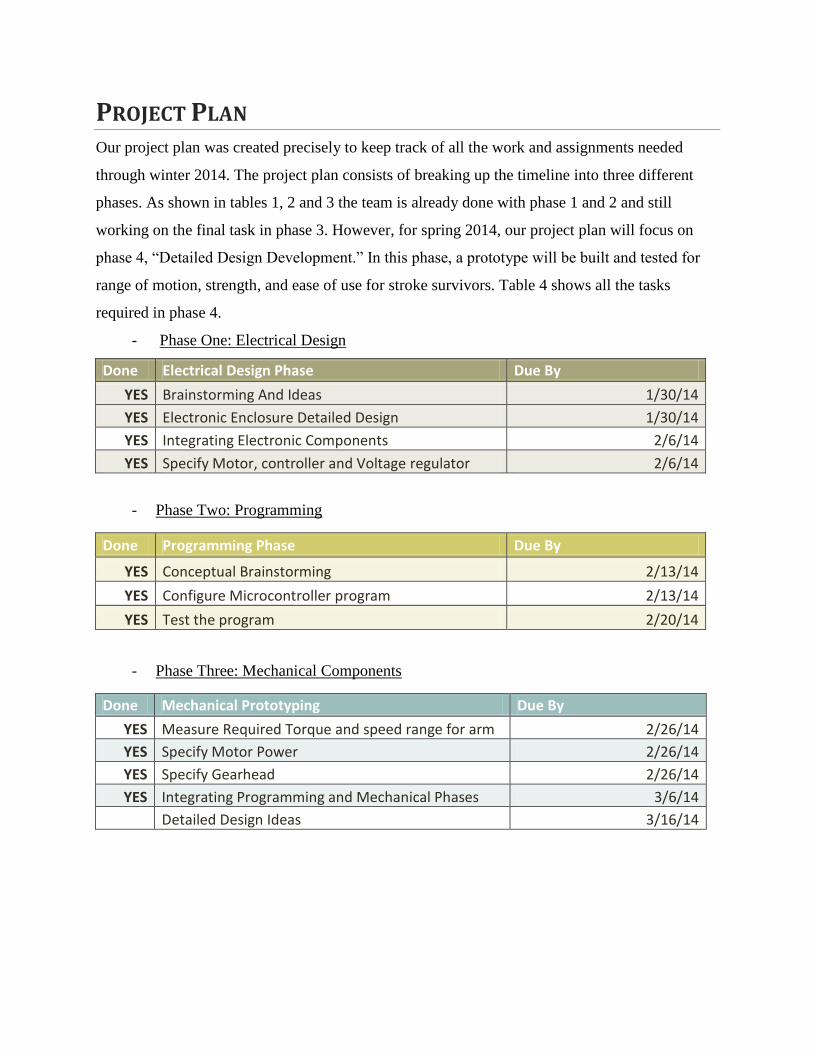
PROJECT PLAN Our project plan was created precisely to keep track of all the work and assignments needed
through winter 2014. The project plan consists of breaking up the timeline into three different
phases. As shown in tables 1, 2 and 3 the team is already done with phase 1 and 2 and still
working on the final task in phase 3. However, for spring 2014, our project plan will focus on
phase 4, “Detailed Design Development.” In this phase, a prototype will be built and tested for
range of motion, strength, and ease of use for stroke survivors. Table 4 shows all the tasks
required in phase 4.
- Phase One: Electrical Design
Done Electrical Design Phase Due By
YES Brainstorming And Ideas 1/30/14
YES Electronic Enclosure Detailed Design 1/30/14
YES Integrating Electronic Components 2/6/14
YES Specify Motor, controller and Voltage regulator 2/6/14
- Phase Two: Programming
Done Programming Phase Due By
YES Conceptual Brainstorming 2/13/14
YES Configure Microcontroller program 2/13/14
YES Test the program 2/20/14
- Phase Three: Mechanical Components
Done Mechanical Prototyping Due By
YES Measure Required Torque and speed range for arm 2/26/14
YES Specify Motor Power 2/26/14
YES Specify Gearhead 2/26/14
YES Integrating Programming and Mechanical Phases 3/6/14
Detailed Design Ideas 3/16/14
Page 6
- Phase four: Detailed Design Development
Done Final Mechanical Assembly Due By
Detailed design Discussion 4/3/14
CAD Model/Solidworks 4/10/14
Generating G-Code 4/17/14
CNC Machining of electronics enclosure 4/24/14
3D print and laser cutting 4/24/14
Machining Rigid Support Frame 5/2/12
Design thermoform mold 5/9/14
Sewing 5/16/14
3D Print thermoform mold 5/16/14
Thermoforming of cuffs 5/23/14
Assembly 5/30/14
Test Prototype 6/1/14 - Refer to Appendix-A for the detailed descriptions of all the tasks and the approximate
amount of time that is associated for each task.
PRODUCT DESIGN SPECIFICATION SUMMARY A Product Design Specification layout was created to act as a guide to design this product.
Electrical and programming designs is complete, therefore the mechanical design components
are the main focus of the updated PDS. From the research and interviews conducted since the
original PDS document, the following summary of the updated design specifications was created.
REQUIREMENTS
Survivor
- Comfort is a luxury, but should be integrated if possible.
- There should be no safety concerns that distract the patient from their mental focus.
- Ease of use will also allow mental focus on the task at hand.
Therapist
- Target multiple muscle groups.
- Device needs to work as good, or better than current technology.
- It will save time and money by allowing patients to use it without assistance.
- The machine needs to be adjustable to perform multiple exercises.
Page 7
- A wall-mounted design is of preference.
- Exercises should target extension muscles, as well as contraction muscles.
- Level-plane motion (perpendicular to force of gravity) is of importance.
- Exercises should mimic everyday tasks.
- Repetition is a major component of success.
These are all things that are necessary for this product to function in a matter that will be
accepted by and purchased by the therapeutic industry.
EXTERNAL SEARCH There are many methods, devices, and machines being used in post stroke rehabilitation. The
devices and machines that appeared to be affective were too expensive and the affordable options
were already being offered to my grandma.
The existing devices are passive. Passive rehabilitation included devices and methods that assist
the patient through a task or motion without the patient initiating or controlling the movement.
An example of this is a simple range of motion exercise where the therapist holds the patients
arm and physically assists them. Another example is the parallel beams. These are used to assist
the patient in relearning how to walk.
After doing neurological research on the physiology of a stroke, and reading case studies relating
to stroke therapy, the idea for an active therapy device came about. An overview of the findings
from this research can be found in appendix A. An active therapy device means that the patient
initiates the movement and the machine or device assists. The case studies supported this
approach and confirmed that it is more effective in restoring function and greatly reduces overall
recovery time.
The next step was to search for existing active therapy devices. The mPower10003 was
discovered. It is a wearable robotic orthosis developed by MIT. This was the only active
therapy device found.
Page 8
INTERNAL SEARCH After the arm brace style device was found to be unviable due to patent protection, the capstone
team began brainstorming to generate alternative methods of limb actuation. Three main
concepts were initially explored for the actuation. The first concept involved moving affected
limbs in a similar manner to an adjustable hospital bed. The second was to initiate movement on
a Cartesian plane much like a CNC table. The third movement method was a device comparable
to an exercise machine, where instead of using weights to supply resistance to movement a motor
would be used to assist movement.
In addition to the general concept of movement, system layout was explored. The layout of the
machine is crucial in generating a detailed design. This led to the discovery of four possible
design layouts: wall mounted, table mounted, stationary free standing, and movable free
standing.
Another topic for brainstorming was the components and set up of the electrical system. The
ideas generated for powering the DC motor included an H-bridge and a linear amplifier. It was
found that both would power the motor with less of a delay. To track the movement of the motor,
both potentiometers and encoders were discussed.
After extensive brainstorming, it was necessary to evaluate the ideas produced and make a
selection based on the needs of the system.
DESIGN EVALUATION & SELECTION To evaluate the ideas produced during brainstorming, seven main criteria were used: versatility,
low weight and volume, simplicity, ease of use, low cost, low visibility, and safety.
First, the system needs to be versatile in order to be most useful for patients. If the machine can
perform more exercises and function with more degrees of freedom, then it can help patients to
regain the use of more limbs and joints.
Page 9
Second, the machine should not be excessively heavy or large. The more compact and
maneuverable the machine is, the more likely it is to appeal to rehabilitation facilities.
Third, the design for the machine should be relatively simple. If the design or manufacture of the
system is too complex, the machine will be less likely to be finished on time for this project,
more likely to have problems, and will probably be more expensive.
Fourth, the ease of use of the machine is crucial. Since the idea is to sell the device to physical
therapy and rehabilitation facilities, the machine will need to be intuitive and easy to use, or the
physical therapists will not want to use it for treatment. Customer satisfaction will also increase
sales. Therefore, this criterion reflects the opinion of the group on ease of use, as well as some
feedback from physical therapists and customers.
Fifth, the device must be low cost. This is important both for the feasibility of completion for this
Capstone project, and for the future manufacture and sale of these machines. The device must be
comparable to or less expensive than existing products, or it will not be useful for customers.
Sixth, the machine should not be too visible or bulky. The user should not feel that they are
hooked to a machine, but rather that they are simply going through the motions themselves. This
is important for the stroke survivors to restore their neurological pathways through the concept or
neuroplasticity.
Finally, safety is imperative. The exercise machine must be safe to use, including the ability to
contain programming and mechanical stops to keep the device from overextending limbs or
otherwise harming the patients. Safety is a high priority and must be addressed in any concept
that is chosen.
Each concept generated during brainstorming was rated in each of these seven criteria. The
rating is weighted and each concept is given a score out of the highest score possible for each
criteria. The total of the rating values was calculated for each concept. The concept with the
highest total was deemed to be most appropriate for the project and was selected. See Table 1 for
the ratings and totals.
Page 10
Table 1: Concept Evaluation Criteria and Ratings
After applying the evaluation criteria, a decision was made for each category based on the totals
for each concept. The final decision was to develop a pulley exercise machine that can be
mounted on a wall or stationary freestanding. Using these components, the detailed design
process could begin.
DETAILED DESIGN PROGRESS Detailed design encompasses three fundamental areas: electrical, programming, and mechanical.
The initial electrical system prototype used voltage sensors placed on the forearm, a differential
amplifier, an arduino microcontroller and a transistor circuit to drive a servo motor. A power
supply was used to power both the controller and the servo motor. This system proved the
possibility of controlling a motor by sensing muscle voltage changes. However, when the servo
motor was replaced with a DC motor that had sufficient power to move a limb, there was a
perceivable delay between sensory input to motor output. This problem was resolved by using
an H-bridge circuit to drive the motor. The H-bridge and motor are powered by a separate supply
from the Arduino microprocessor, due to electromagnetic interference (noise) issues. Currently
the prototype electrical system drives a geared DC motor without perceptible delay.
Page 11
Another consideration in the electrical system was position sensing and feedback. The design
options considered were to use an optical encoder to sense the rotational position of the armature
or using a potentiometer attached to either the output shaft of the actuating pulley, or on the
patient’s arm itself. Using a potentiometer to sense motor output shaft position was selected
mainly due to lower cost and simpler design. Using an encoder would add more complex code
and a lot of processing time to the circuit. Since the goal is to minimize the patients’ perceivable
delay, the potentiometer was the best option. Using a potentiometer, changes in position will
change the resistance, which can be measured as a voltage change in the circuit proportional to
angular position.
The microcontroller program currently receives voltage input and converts this signal to voltage
output normalized to the 24VDC input of the motor. Subsequent programming steps will
incorporate a calibration program that will set the resting muscle voltage to zero and set the
limits of motion for the motor. A graphic display will also be used to streamline the interface
between the user and the machine.
The mechanical system is supplied motive power from a 24V brushed DC gear motor. Body
segment mass data and limb movement speed were researched to determine the torque and
angular velocity specifications of the motor. While stepper motors and brushless motors were
initially considered, the brushed motor was selected due to price, simplicity of control, and no
need for fine angular positioning due to the reduction in angular speed through a gearbox. The
purchased motor provides a rated torque and rotational velocity of 31 in-lb and 167 rpm,
respectively, with a keyed shaft for pulley attachment.
Detailed design of the entire assembly which includes an adjustable frame structure, components,
and interface is in progress. The frame consists of a vertical square tube with attachments points
on the top and bottom that can accommodate free standing and wall mount operation. A housing
containing the motor and part of the electronics package will be attached to the tube allowing for
vertical adjustment for patient build and differing exercises. A counterweight system will be
employed to preclude the housing unit from falling to the floor if unclamped. Design of the
Page 12
EMG sensors and integrated limb attachment point are currently underway and will be the final
step of detailed design.
CONCLUSION The progress of the design is congruent with the goals set in place. A prototype of the
Myoelectric Robotic Orthosis device is complete, but is lacking full functional potential. Goals
were set based on three categories: Electrical, Programming, and Mechanical, and further design
will be addressed Spring 2014. The electrical system currently consists of many discrete and
disconnected parts. The next step in detailed design is to consolidate these separate elements
into an unobtrusive electronic package, and to create versatility in the exercises of the machine.
Although the mechanism works in the simplest form, the functionality of the system needs to be
altered to meet design requirements based on consumer feedback. An adjustable pulley system
will be integrated that allows patients to mimic everyday tasks. The last portion of the
mechanical design is refining the sensor attachment and being more specific about placement of
the electrode pads. A detailed CAD model will be complete by April 10. The final step of the
programming is adding ROM and baseline voltage calibration sequence into the program and
integrating a graphic interface. Furthermore, there have been three major stopping points in this
design process that called for creative decision-making. The necessary decisions made at these
crossroads were the following: Creating a machine that targets multiple body parts and body
motions—as opposed to an arm brace, switching from a servo motor to a DC motor with an H-
bridge to facilitate power, and to have a wall-mounted machine to harness leverage without
compromising floor space. With all these design components in place, the greatest compromise
made is in the optimization of time and money versus functionality. Instead of creating a
machine with a complex system that can do all intended exercises, time and money constraints
lead to a more simple and efficient machine that does most intended exercises.
Page 13
APPENDIX
Appendix-A [Timeline Schedule] - This table shows the detailed descriptions of all the tasks, and the approximate
amount of time that is associated to each one.
*Number inside boxes indicate number of team members for each task
Task Name Duration June
W1 W2 W3 W4 W5 W6 W7 W8 W9 W10 W11 W12 W13 W14 W15 W16 W17 W18 W19 W20 W21 W22
Electrical
Procurement Lead Time 20 days
Conceptual Brainstorming and Selection 16 hrs Group
Integrating Electronic Components 10 hrs 2
Electronic Enclosure Detailed Design 12 hrs Group
Specify motor controller and voltage regulator6 hrs 1
Total Work 44 hrs
Programming
Conceptual Brainstorming and Selection 10 hrs Group
Configure Microcontroller Program 6 hrs 1
Test the program 1 hr 1
Total Work 17 hrs
Mechanical Prototyping
Procurement Lead Time 15 days
Conceptual Brainstorming and Selection 20 hrs Group
Detailed design 20 hrs Group
Measure required torque range to assist arm30 min 2
Measure required speed range to assist arm 5 min 2
Specify motor power 3 hrs 1
Specify gearhead 3 hrs 1
CAD Model 10 hrs 1
3D print and laser cutting time 36 hrs 1
Assembley 5 hrs Group
Test 2 hrs Group
Design Refinement 10 hrs Group
Total Work 83 hrs
Final Mechanical Assembley
Procurement Lead Time 15 days
Detailed design 10 hrs Group
CAD Model 10 hrs 1
Generating G-Code 3 hrs 1
CNC Machining of electronics enclosure 12 hrs 1
Machining Rigid Support Frame 5 hrs 2
Design thermoform mold 2 hrs Group
Sewing 5 hrs 2
3D Print thermoform mold 10 hrs 1
Thermoforming of cuffs 1 hr 2
Assembley 10 hrs Group
Total Work 41 hrs
January February March April May
Page 14
Appendix-B [Product Design Specifications]
- This table shows the House Of Quality used in the Product Design Specification
Phase.
Customer Requirements Design Criteria
House of Quality
Ite
m #
Re
lati
ve
Im
po
rta
nce
(1-5
)
Mic
roco
ntr
oller
Sele
cti
on
Mo
tor
To
rqu
eM
oto
r Sp
eed
Ge
ar
Red
uct
ion
Bra
ce M
ate
rial Sele
ctio
nLe
ngth
of
mo
men
t a
rmFri
ctio
n r
ed
uct
ion
Ge
ar
rati
oM
echa
nic
al Fu
nct
ion w
ith
u
ser
Performance
1 Relatively Silent operation 4 +++ + + +++ + · · · · Level of Correlation
2 Brace weight 4 + ++ ++ · + +++ · + · · None
3 moving an average person's arm unassisted 4 ++ +++ · · . · + ++ . + Low
4 range of motion 4 ++ + ++ . + + + ++ + ++ Moderate
5 Calibration setup time 3 ++ + · · . · · ++ ++ +++ High
6 ambidextrous operation 5 · ++ · · . · . +++ ++
7 Intuitive User Interface 4 +
Cost
10 parts <$1000 1 + ++ + +++ + · + · ·
Design Life
10 NA 2 · ++ + ++ + + · · ·
Quality
11 Withstand small impacts 3 + . . +++ . + . . +
12 Operate at full capacity 4 +++ +++ +++ · +++ +++ ++ ++ +
Safety
14 Does not cause injury 5 +++ +++ +++ +++ +++ +++ +++ +++
Page 15
- This table consists of all the original Product Design Specifications such as:
Performance, Safety, Environment, Ergonomics, Manufacturing and Installation.
Page 16
Appendix-C [External Search Information]
- An overview of the physiology of a stroke and background on case studies supporting
active therapy.
Physiology of a stroke
Stroke victims suffering from hemiplegia or hemiparesis show functional deficits in voluntary
motor control. All voluntary motor control originates in the brain and the motor cortex is the
area of the brain most involved with voluntary movement.
Even the simplest tasks require many complex sequential and concurrent processes. When you
take a drink of water from a glass, it involves reaching out towards the glass and positioning your
hand so it can grab the glass. Your prefrontal cortex immediately begins preparation for this
movement and transmits the information through a large number of axons projecting from the
parietal cortex, a region involved with spatial perception. Its analysis of the position of your
body and limbs relative to the glass is essential in preparing for the movement. The basal
ganglia are another set of brain structures involved in this part of the process.
The premotor cortex and supplementary motor area work with the cerebellum to specify the
precise sequence of contractions of the various muscles that will be required to carry out the
selected motor action, in this case, raising your arm and extending it forward to grab the
glass. To do this your brain will need to convert the glasses location in the external environment
into a set of intrinsic coordinates allowing precise adjustment of the angles of the joints involved
in the movement.
The primary motor cortex, the brain stem, and the spinal cord produce the contractions of all the
muscles needed for the chosen movement. The primary motor cortex determines how much force
each muscle group must exert, and then sends this information to the spinal motor neurons and
interneurons that generate the movement itself, as well as the postural adjustments that
accompany it.
Page 17
Neuroplasticity
Neuroplasticity refers to the brains ability to change in response to stimuli from the external and
internal environments. The changes involve individual neurons—for example, synthesis of
different proteins or sprouting of new dendrites—as well as changes in the strengths of synaptic
connections including the neuromuscular junction.
The areas of the brain known to have this capability include the association areas of the frontal,
parietal, occipital, and temporal lobes, and the primary somatosensory and primary motor areas
in the brain.
If a particular body part is used more intensively or in a newly learned activity, such as reading
Braille, the cortical areas of the brain devoted to that body part gradually expand. Memory
occurs in stages over a period of time. Immediate memory is the ability to recall ongoing
experiences for a few seconds. It provides a perspective to the present time that allows us to
know where we are and what we are doing it is related to. Short-term memory is the temporary
ability to recall a few pieces of information for seconds to minutes. One example is when you
look up an unfamiliar telephone number, cross the room to the phone, and then dial the new
number. If the number has no special significance, it is usually forgotten within a few seconds.
Brain areas involved in immediate and short-term memory include the two nuclei of the thalamus
(anterior and medial nuclei). Some evidence supports the notion that short-term memory
depends more on electrical and chemical events in the brain than on structural changes, such as
the formation of new synapses. Information in short-term memory may later be transformed into
a more permanent type of memory, called long-term memory, which lasts from days to years. If
you use that new telephone number often enough, it becomes part of long-term
memory. Information in long-term memory usually can be retrieved for use whenever needed.
The reinforcement that results from the frequent retrieval of a piece a piece of information is
called memory consolidation. Long-term memories for information that can be expressed by
language, such as a telephone number, apparently are stored in wide regions of the cerebral
cortex.
Page 18
Anatomical changes occur in neurons when they are stimulated. For example, electron
micrographs of neurons subjected to prolonged, intense activity reveal an increase in the number
of presynaptic terminals and enlargement of synaptic end bulbs in presynaptic neurons, as well
as an increase in the number of dendritic branches in postsynaptic neurons. Moreover, neurons
grow new synaptic end bulbs with increasing age, presumably because of increased use.
Mirror Neurons
Scientists studying Area F5 in the ventral premotor cortex of monkeys found that certain neurons
in this area sent out action potentials not only when the monkeys were moving their hands or
mouths, but also when they were simply watching another animal or a human being who was
making such a gesture. These neurons were dubbed mirror neurons because of the way that a
visually observed movement seemed to be reflected in the motor representation of the same
movement in the observer.
In addition to mirror neurons, which are activated both when you perform an action yourself and
when you see someone else performing it, another kind of neurons, called canonical neurons,
become activated when you merely see an object that can be grasped by the prehensile
movement of the hand whose movements they encode—as if your brain were foreseeing a
possible interaction with this object and preparing itself accordingly.
What these two types of neurons have in common is that they are both activated by an action
regardless of whether you are carrying that action out, anticipating carrying it out, or watching
someone else carrying it out.
Many subsequent studies have tended to confirm that mirror neurons exist in the human brain as
well. For example, in a study published in the December 2004 on-line edition of Cerebral Cortex,
a group of professional ballet dancers and a group of dancers of capoeira (a Brazilian
dance/martial arts form) were asked to watch short videos of dancers performing brief ballet and
capoeira moves, while a functional magnetic resonance imaging (fMRI) scanner detected
changes in their brain activity. A control group of non-dancers also participated.
Page 19
The fMRI results showed that the areas of the dancers’ brains associated with this “mirror neuron
system” were more active when they were watching movements of the kind that they were
trained in than when they were watching the other kind. The non-dancers in the control group
showed even less mirror-neuron activity than the ballet dancers watching capoeira or the
capoeira dancers watching ballet, and this lower level of activity was the same regardless of
which of the two types of dance they were watching.
This study thus not only supports the idea that there is a mirror neuron system in the human
brain, but also shows that this system’s activity level increases with the degree of training that
the individual has in certain particular types of movements. And, it should be stressed, this
increased activity occurs not in the visual centers of the occipital cortex, but in the motor area
where the brain plans complex movements, as well as in the intraparietal sulcus, a brain area
responsible for visual-motor integration.
Action Potential
“Action potential” is the technical term used to describe a nerve impulse. It consists of a brief,
reversible polarization that propagates along an axon. It differs from a receptor potential
(synaptic potential) in several respects.
First of all, an action potential does not propagate passively, but actively, by means of special
voltage-sensitive ion channels in the axon. In addition, mammals have a particular mechanism
that accelerates the propagation of the action potential.
This process also requires energy from the neuron, which must maintain the activity of the ion
pumps that rebalance the charges on either side of the membrane after an action potential has
passed.
Action potentials do not vary in amplitude or intensity. If the intensity of a stimulus falls below
the neuron’s excitation threshold, nothing happens. If the intensity of this stimulus exceeds this
threshold, it does not matter whether it does so by a small or a large amount. Either way, an
action potential will be triggered, and its amplitude and frequency will always be the same for
Page 20
any given cell. Consequently, the only way a neuron can transmit information is by varying the
frequency of its action potentials. The action potential creates a voltage potential that is
proportional to the force of the contraction and this voltage potential can be measure at the
surface of the skin above the muscle and observed used an EMG.
Evidence Based Rehabilitation Studies
There are several types of post stroke rehabilitation that can be divided into three categories;
pharmacological, behavioral, and cognitive. Behavioral and cognitive are shown to have the
greatest impact in facilitating neuroplasticity.
Behavioral Therapy: Exercise is one of the best behavioral therapies because it has one of the
most significant effects on neuroplasticity. Studies have shown that exercise can have substantial
benefits for brain reorganization, because it stimulates the connections in the central nervous
system. Rehabilitating exercise improves motor skills after a stroke which helps the brain forge
new neural pathways and connections. This facilitates the processes involved in neural plasticity.
Cognitive Therapy: Cognitive rehabilitation focuses on the recovery of functions such as
memory, attention, motor skills, as well as other functions. Depending on the patients care
needs, it can be the most important. It’s the most effective form of therapy for stimulating the
neuroplasticity processes in post-stroke patients due to its direct effects on the cognitive areas in
the brain.
Page 21
Mental practice is the term given to practicing activities and movements ‘in the mind’, and it has
been used in athletes. Recent studies have shown that it can also be used on stroke patients, who
visualize motor movements through mental imagery, alongside other cognitive-based
treatments. It has been suggested that patients should visualize and practice an activity mentally
in conjunction with other conventional treatments in order to improve motor functions,
especially arm movement. Virtual reality has also been used to improve motor movements
alongside balance.
With regards to fine motor skills, repetition of the same activities every day such as putting on
make-up, picking up and putting down a coin helps to produce new neural pathways in order to
compensate for the damaged pathways, and these exercises can help promote neuroplasticity in
post-stroke patients.
With more strenuous motor movements such as with arm movement, studies have shown that it’s
more beneficial to conduct bimanual exercises opposed to merely exercising the affected arm
alone. Bimanual exercises have also been shown to have a direct effect on promoting cortical
neural plasticity in various ways: motor cortex disinhibition that allows increased use of the
spared pathways of the damaged hemisphere, increased recruitment of the ipsilateral pathways
from the contralateral hemisphere supplementing the damaged corticospinal pathways, and up
regulation of descending premotor neuron commands onto propriospinal neurons.
Conclusion from Research Analysis
Not all of the research data was presented in this report. The following conclusions are
presented in the same order as the sections of data presented. In some cases, conclusions will be
made based on correlations found between sections with an emphasis on neuroplasticity.
• The specific functional deficits observed in someone who has suffered a stroke can be
correlated with the functions of the cortical regions damaged by the stroke.
• The interdependencies that exist between the areas of the brain responsible for the
initiating, coordinating, learning, and remembering voluntary movement in conjunction with
neuroplasticity mean that stimulation of at any point in the loop is an effective way to innervate
new neural growth resulting in healthy brain function in stroke victims.
Page 22
• The cerebellum uses visual signals associated with movement of limbs to store
information that will improve the coordination of muscle tension and relaxation resulting in
more precise and accurate voluntary movement of that limb.
• The brain releases dopamine during a rewarding experience. The motor cortex
contains dopamine receptors which can form positive associative memories that reinforce the
neuro connections used in the corresponding movement.
• Neuroplasticity is the most important process that should be stimulated in the affected
areas of the brain.
• Visualizing a movement associated with an affected limb is an effective way to stimulate
the areas affected by the stroke thereby initiating the reparative effects of neuroplasticity.
• Cognitive therapy is the most effective form of therapy because it stimulates the
activation of neuroplasticity.
• Neuroplasticity can heal the neural connections damaged by a stroke and restore lost
functionality.
• When the patient initiates a voluntary movement, an action potential in the form of a
voltage differential is created across the appropriate muscle. This voltage change only exists
when the patient initiates movement. The voltage potential is created by sodium and potassium
ions and can be measured quantitatively.
• The threshold of an action potential is dynamic and influenced by the brains
interpretation of visual, tactile, pressure, and force signals from sensory receptors associated
with the movement.
Recommendations
It is our recommendation that the use of EMG activated motorized exercise machine be
implemented and used during all cognitive therapy sessions. When used on the affected limb it
will have a direct impact on the corresponding areas of the cortical region affected by the
stroke. The machine works by sensing the intent to move by measuring and monitoring the
action potential created during a muscle contraction. An EMG amplifier and sensors are used to
take these measurements in real time. At the instant the action potential is sensed, the motor
which is located on the exercise machine above the joint of the affected limb begins to
rotate. The motor spools a cable with an appropriate handle or strap that connects to the affected
Page 23
limb. The assisted motion can be incremental or continuous through the range of motion. The
visual feedback will stimulate the cerebellum reinforcing the creation of new neuro pathways for
the motion. The result is an increase in restored function compared to passive rehabilitation.
This versatility of this device makes it appropriate for use on the upper and lower extremities of
all stroke victims. The cost of the device is relatively low compared to passive therapy devices
such as electrical stimulation.
Page 24
REFERENCES
[1] Stroke rehabilitation information. (2013, June 19). Retrieved from
http://www.ninds.nih.gov/disorders/stroke/stroke_rehabilitation.htm
[2] Rash, G. (n.d.). Electromyography fundamentals. Retrieved from
http://people.stfx.ca/smackenz/Courses/HK474/Labs/EMG
Lab/EMGfundamentals.pdf
[3] http://www.myopro.com