Association of adipokines with obesity in children and adolescents
Background: Childhood obesity is a global epidemic and is associated with a higher risk of chronic diseases such as hypertension, diabetes mellitus and other metabolic disorders. Several adipokines including resistin, visfatin, leptin and adiponectin are synthesized and secreted by adipocytes, which play an important role in obesity. Patients & methods: A total of 90 subjects (60 controls and 30 obese) between the ages of 5 and 18 years were selected. Serum visfatin, TNF-a, resistin, insulin and adiponectin were measured using ELISA and insulin resistance was calculated by the Homeostasis Model of Assessment–Insulin Resistance. Results: Mean ± standard deviation Homeostasis Model of Assessment–Insulin Resistance, serum TNF-a and visfatin levels were significantly higher in obese subjects (3.99 ± 0.94, 12.99 ± 3.42, 10.89 ± 2.72, respectively) compared with the control group (1.60 ± 0.34, 7.22 ± 2.22 and 4.97 ± 1.57, respectively). Mean ± standard deviation serum adiponectin levels were significantly lower in obese children (5.95 ± 1.02) compared with controls (9.07 ± 1.25). Binary logistic regression shows that adiponectin and visfatin are associated with obesity. Conclusion: Circulating levels of adipokines vary in obesity and adiponectin and visfatin are associated with obesity.
KEYWORDS: adiponectin n HOMA–IR n inflammation n insulin n resistin n TNF-a n visfatin
Obesity is an emerging global public health chal-lenge in developing as well as developed countries. According to the most recent National Health and Nutrition Examination Survey 2009–2010, almost 17% of youths and 37.5% of adults were obese in 2009–2010. There was no change in the prevalence of obesity among adults or children from 2007–2008 to 2009–2010 [1]. There is considerable concern among the public for adult obesity, but obesity in children is still a neglected area. The percentage of overweight children (>95th percentile) has reached approximately 14% among both boys and girls according to the National Health and Nutrition Examination Sur-vey III database [2]. Research shows that several environmental factors contribute to obesity, which is related to dietary intake of refined carbohy-drates and saturated fat, and limited consumption of fruit and vegetables. Moreover, an increasingly sedentary lifestyle and indoor activities such as computer and TV use limit the opportunities for physical activity. Genetic predisposition for obe-sity may be a contributing factor for the increasing prevalence of overweight children that needs to be explored [3].
Obesity is the leading preventable cause of death worldwide and a serious public health con-cern of the 21st century. It increases the risk of diabetes, hypertension, and high blood choles-terol and triglyceride levels, which can lead to
atherosclerosis [4,5]. Adipose tissue is a source of adipokines such as leptin, adiponectin and visfa-tin, which are secreted by adipocytes [6]. It is pro-posed that these adipokines produced by adipose tissue may be responsible for insulin resistance or insulin sensitivity in obesity. Indeed, the expres-sion or production of these adipokines was shown to be related to the degree of obesity of subjects and, thus, might be involved in inducing or pre-venting obesity-related insulin resistance [7]. The deleterious effect of TNF-a on insulin action has been presented in different experimental studies, which shows that phosphorylation of the insulin receptor substrate-1 on serine residues results in reduction of insulin signaling into the cell [8,9]. Studies on obese rodents and humans show higher expression of TNF-a mRNA in the subcutane-ous abdominal adipose tissue depot [9,10], which indicates that TNF-a may play a crucial role in obesity-related insulin resistance [11]. Contrary to this, the relationship between adipose-derived TNF-a and the in vivo insulin sensitivity in humans is under discussion, as some studies show nonsignificant release of TNF-a in vivo [7,12–14].
The objectives of this study were: to determine the levels of blood glucose, insulin, visfatin, resis-tin, adiponectin and TNF-a in nonobese controls and obese children and adolescents; and to deter-mine the correlation of adipokines with insulin resistance and obesity.
1Department of Biochemistry, Ziauddin University, 4/B, Shahrah-e-Ghalib, Block 6, Clifton, Karachi 75600, Pakistan 2Basic Health Sciences, Ziauddin University, Clifton, Karachi 75600, Pakistan 3Department of Pathology, Sheikh Zayed Bin Neyhan Medical College, University Avenue, New Muslim Town, Lahore 54600, Pakistan 4Department of Biochemistry, 2. Rawal Institute of Health Sciences, Islamabad, Pakistan 5Ziauddin University, Clifton, Karachi 75600, Pakistan *Author for correspondence: [email protected]
Biomarkers Med. (2013) 7(5)732 future science group
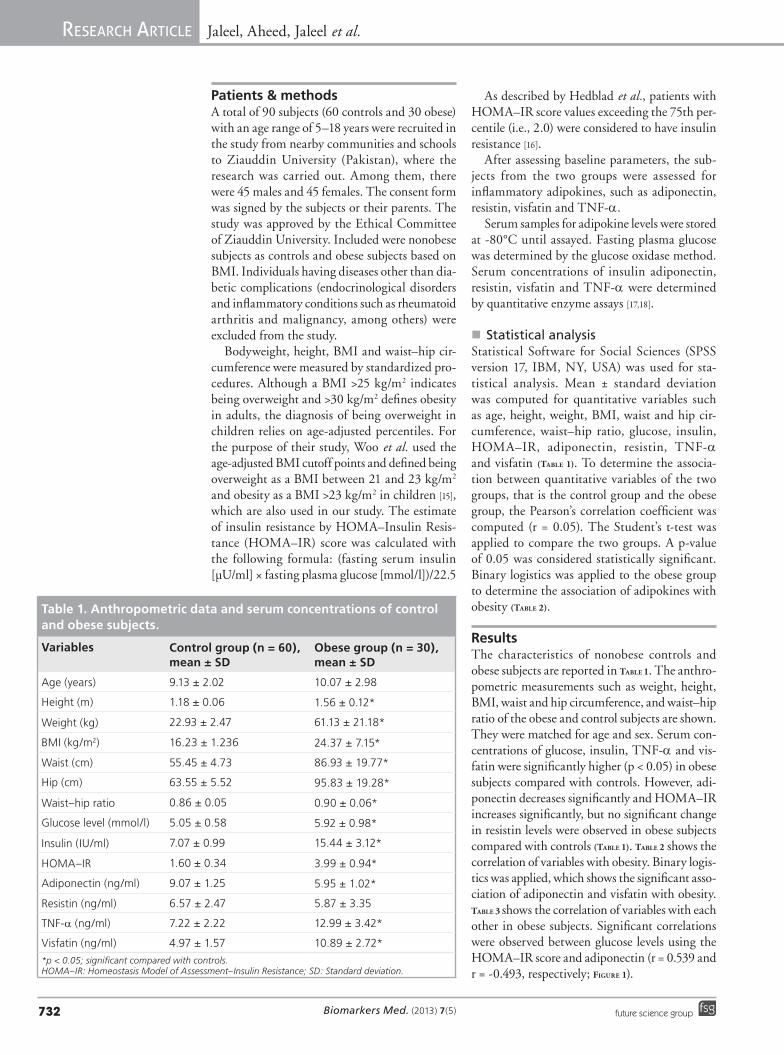
Patients & methodsA total of 90 subjects (60 controls and 30 obese) with an age range of 5–18 years were recruited in the study from nearby communities and schools to Ziauddin University (Pakistan), where the research was carried out. Among them, there were 45 males and 45 females. The consent form was signed by the subjects or their parents. The study was approved by the Ethical Committee of Ziauddin University. Included were nonobese subjects as controls and obese subjects based on BMI. Individuals having diseases other than dia-betic complications (endocrinological disorders and inflammatory conditions such as rheumatoid arthritis and malignancy, among others) were excluded from the study.
Bodyweight, height, BMI and waist–hip cir-cumference were measured by standardized pro-cedures. Although a BMI >25 kg/m2 indicates being overweight and >30 kg/m2 defines obesity in adults, the diagnosis of being overweight in children relies on age-adjusted percentiles. For the purpose of their study, Woo et al. used the age-adjusted BMI cutoff points and defined being overweight as a BMI between 21 and 23 kg/m2 and obesity as a BMI >23 kg/m2 in children [15], which are also used in our study. The estimate of insulin resistance by HOMA–Insulin Resis-tance (HOMA–IR) score was calculated with the following formula: (fasting serum insulin [µU/ml] × fasting plasma glucose [mmol/l])/22.5
As described by Hedblad et al., patients with HOMA–IR score values exceeding the 75th per-centile (i.e., 2.0) were considered to have insulin resistance [16].
After assessing baseline parameters, the sub-jects from the two groups were assessed for inflammatory adipokines, such as adiponectin, resistin, visfatin and TNF-a.
Serum samples for adipokine levels were stored at -80°C until assayed. Fasting plasma glucose was determined by the glucose oxidase method. Serum concentrations of insulin adiponectin, resistin, visfatin and TNF-a were determined by quantitative enzyme assays [17,18].
�n Statistical ana lysisStatistical Software for Social Sciences (SPSS version 17, IBM, NY, USA) was used for sta-tistical ana lysis. Mean ± standard deviation was computed for quantitative variables such as age, height, weight, BMI, waist and hip cir-cumference, waist–hip ratio, glucose, insulin, HOMA–IR, adiponectin, resistin, TNF-a and visfatin (Table 1). To determine the associa-tion between quantitative variables of the two groups, that is the control group and the obese group, the Pearson’s correlation coefficient was computed (r = 0.05). The Student’s t-test was applied to compare the two groups. A p-value of 0.05 was considered statistically significant. Binary logistics was applied to the obese group to determine the association of adipokines with obesity (Table 2).
ResultsThe characteristics of nonobese controls and obese subjects are reported in Table 1. The anthro-pometric measurements such as weight, height, BMI, waist and hip circumference, and waist–hip ratio of the obese and control subjects are shown. They were matched for age and sex. Serum con-centrations of glucose, insulin, TNF-a and vis-fatin were significantly higher (p < 0.05) in obese subjects compared with controls. However, adi-ponectin decreases significantly and HOMA–IR increases significantly, but no significant change in resistin levels were observed in obese subjects compared with controls (Table 1). Table 2 shows the correlation of variables with obesity. Binary logis-tics was applied, which shows the significant asso-ciation of adiponectin and visfatin with obesity. Table 3 shows the correlation of variables with each other in obese subjects. Significant correlations were observed between glucose levels using the HOMA–IR score and adiponectin (r = 0.539 and r = -0.493, respectively; Figure 1).
Table 1. Anthropometric data and serum concentrations of control and obese subjects.
Variables Control group (n = 60), mean ± SD
Obese group (n = 30), mean ± SD
Age (years) 9.13 ± 2.02 10.07 ± 2.98
Height (m) 1.18 ± 0.06 1.56 ± 0.12*
Weight (kg) 22.93 ± 2.47 61.13 ± 21.18*
BMI (kg/m2) 16.23 ± 1.236 24.37 ± 7.15*
Waist (cm) 55.45 ± 4.73 86.93 ± 19.77*
Hip (cm) 63.55 ± 5.52 95.83 ± 19.28*
Waist–hip ratio 0.86 ± 0.05 0.90 ± 0.06*
Glucose level (mmol/l) 5.05 ± 0.58 5.92 ± 0.98*
Insulin (IU/ml) 7.07 ± 0.99 15.44 ± 3.12*
HOMA–IR 1.60 ± 0.34 3.99 ± 0.94*
Adiponectin (ng/ml) 9.07 ± 1.25 5.95 ± 1.02*
Resistin (ng/ml) 6.57 ± 2.47 5.87 ± 3.35
TNF-a (ng/ml) 7.22 ± 2.22 12.99 ± 3.42*
Visfatin (ng/ml) 4.97 ± 1.57 10.89 ± 2.72*
*p < 0.05; significant compared with controls. HOMA–IR: Homeostasis Model of Assessment–Insulin Resistance; SD: Standard deviation.
Association of adipokines with obesity in children & adolescents ReseaRch aRticle
www.futuremedicine.com 733future science group
DiscussionThe increase in prevalence in obesity is an alarm-ing condition, especially in developing countries where there is scarcity of resources. Lifestyle has played an important role in the pandemic of obesity, which leads to insulin resistance, diabe-tes mellitus and cardiovascular complications. Efforts to understand the link between obesity and insulin resistance has led to the identification of several adipocyte-derived adipokines, which are both proinflammatory and anti-inflammatory, and are secreted from immune cells that infiltrate the adipocytes of the obese individuals [19].
In this study, we measured four adipokines, that is, adiponectin, resistin, visfatin and TNF-a, and their relationship with insulin and HOMA–IR score in obese subjects. Adiponectin was found to be significantly lower and visfatin, TNF-a, glucose, insulin and HOMA–IR score were sig-nificantly higher in obese children compared with controls; however, no significant change was observed in resistin levels among the two groups. Adiponectin shows a positive correlation with insu-lin and visfatin shows a negative correlation with insulin in obese children. No significant correla-tion of these adipokines was found with anthro-pometric measurements: waist–hip ratio and BMI, as well as glucose, insulin and HOMA–IR score.
Visfatin is identified as being secreted from vis-ceral adipocytes and was found to be significantly correlated with visceral fat in a study by Fukuhara et al. [20]. Previous studies reported elevated vis-fatin concentration in obesity [21–24], but Pagano et al. reported lower plasma visfatin concentration in obese subjects [25]. Studies by Chen et al. [26] and Zahorska-Markiewicz et al. [27] reported no cor-relation between serum concentrations of visfatin and anthropometric measurements in obese sub-jects, which supports the data in our study. This may be due to ethnicity, population characteristics and confounding factors such as gender, which result in conflicting reports. Similarly weak nega-tive correlations exist among visfatin and insulin (r = -0.355) and HOMA–IR score (r = -0.329) in our study, which is similar to the results reported by Araki et al. [23] and Berndt et al. [22], which show no correlation among them.
Our study shows significantly lower plasma adi-ponectin concentrations in obese children, which shows decreased protective effects of anti-inflam-matory adipokines in these subjects. A study by Oh et al. showed lower adiponectin levels in obese and nonobese subjects with a family history of Type 2 diabetes [28]. Similarly, studies by Kad-owaki et al. [29] and Hara et al. [30] reported lower concentration of adiponectin in insulin resistance
Table 2. Association of adiponectin and visfatin with obesity: binary logistics (obese group).
Variables b SE Wald DF Sig. Exp[B] 95% CI for Exp[B]
Constant 0.109 4.636 0.001 1 0.981 1.116 –The final logistic regression model includes adiponectin and visfatin after adjusting for the effect of other variables in the model and taking the option ‘obesity’ as the reference category. The model equation is now: obesity = 0.109 + 0.011(visfatin) + (-1.220)(adiponectin). Nagelkerke R2 shows that 65–90% of the variation in the outcome variable (obesity) is explained by this logistic model. The Hosmer–Lenshow test for the final model is c2 = 0.874 (p = 0.99), which shows that the model is fitted well for the data and the model predicts 94% correct data. The contribution of visfatin (Wald = 7.645) is more than adiponectin (Wald = 6.30) in the model. Both adiponectin and visfatin are associated with obesity (p-values of 0.012 and 0.006, respectively). Exp[B] tells the odds ratio. Both are quantitative variables. An increase in 1 unit (ng/ml) in adiponectin is associated with a 0.295-fold decrease in the odds that a child will be obese and an increase in 1 unit (ng/ml) in visfatin is associated with a 1.01-fold increase in the odds that a child will be obese.DF: Degrees of freedom; SE: Standard error; Sig.: Significance; Wald: Contribution of variable in model after being statistically significant.
Table 3. Correlation of variables in the obese group.
Visfatin (ng/ml) -0.329 0.013 -0.355 -0.175 0.190 -08.00 –Variables are expressed as r-values. *Significant at the p = 0.01 level. HOMA–IR: Homeostasis Model Assessment–Insulin Resistance.
ReseaRch aRticle Jaleel, Aheed, Jaleel et al.
Biomarkers Med. (2013) 7(5)734 future science group
and obesity, which confirms our results. However, no significant correlation exists with the anthro-pometric measurements, glucose and HOMA–IR score, in our study. However, a weak correlation between adiponectin and insulin (r = 0.339) exists in our study.
Resistin levels do not increase significantly in obese children compared with controls, nor do they show any correlation with the anthropo-metric measurements, glucose, insulin or HOMA–IR score. A study by Lee et al. showed no association of resistin with obesity, which is consistent with our study [31]. However, Degawa-Yamauchi et al. showed its concentration to be higher in obesity [32]. Contrasting data that do not confirm the possible role of resistin in obesity exist.
TNF-a concentration increases in obese children compared with controls. However, no significant correlation of TNF-a exists with the anthropometric measurements, glucose or HOMA–IR score in our study. Studies by Hota-misligil et al. [33] and Borst [34] confirmed the role of TNF-a in obesity, which is consistent with our
results. It is secreted by white adipose tissue and plays an important role in the pathophysiology of insulin signaling. Moreover, it also influences the secretion of other adipocyte-secreting peptides. This suggests that TNF-a secreted by adipocytes in turn leads to higher concentrations of visfa-tin and lower concentrations of adiponectin in our study.
This study has certain limitations, which include: cross-sectional design of the study; small sample size (due to limited budget); and large age range. Dietary and physical activity of the subjects were also not considered in the study.
ConclusionProinflammatory adipokines increase and anti-inflammatory adipokines decrease in obesity. Adiponectin and visfatin concentrations show significant associations with obesity.
Future perspectiveLarge-scale studies on adipokines will reveal interesting associations with obesity, which can lead to diabetes and ischemic heart disease. More-over, gene polymorphisms of adipokine receptors will help in establishing the missing link in the development of obesity
Financial & competing interests disclosureThe authors thank the Higher Education Commission for funding the project (Project No 20-RES-1357). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research The authors state that they have obtained appropriate insti-tutional review board approval or have followed the princi-ples outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investi gations involving human subjects, informed consent has been obtained from the participants involved.
Executive summary
� Obesity is on the rise not only in developed but also in developing countries. � This article addresses the association of adipokines with obesity in children and adolescents. � A total of 90 subjects were recruited, which were age- and sex-matched and divided into obese and nonobese groups. � Circulating levels of adipokines, such as adiponectin, resistin and visfatin, along with insulin and TNF-a, were measured by the ELISA technique, and fasting blood glucose by the glucose oxidase method.
� Serum adiponectin and visfatin levels were found to be associated with obesity in children and adolescents. No significant change in resistin level was observed in this study.
� Obese children can develop diabetes in the future so these adipokines may be helpful in the early detection of obesity in children and could lead to early prevention of complications.
Glu
cose
(m
mo
l/l)
Adiponectin (ng/ml)
r = -0.493p < 0.001
4.20
4.25 5.15 6.05 6.95 7.85
5.20
6.20
7.20
8.20
Figure 1. Correlation between glucose and adiponectin in the obese group.
Association of adipokines with obesity in children & adolescents ReseaRch aRticle
www.futuremedicine.com 735future science group
ReferencesPapers of special note have been highlighted as:n of interestnn of considerable interest
1 Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of Obesity in the United States, 2009–2010. NCHS Data Brief. CDC, GA, USA (2012).
n� Current trends in obesity and its prevalence among youths and adults.
2 Jafar TH, Qadri Z, Islam M, Hatcher J, Bhutta ZA, Chaturvedi N. Rise in childhood obesity with persistently high rates of under-nutrition among urban school-aged Indo-Asian children. Arch. Dis. Child. 93, 373–378 (2008).
3 Bray GA. Medical consequences of obesity. J. Clin. Endocrinol. Metab. 89(6), 2583–2589 (2004).
4 Allison DB, Fontaine KR, Manson JE, Stevens J, Van Itallie TB. Annual deaths attributable to obesity in the United States. JAMA 284, 1530–1538 (1999).
5 Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW Jr. Body-mass index and mortality in a prospective cohort of US adults. N. Engl. J. Med. 341, 1097–1105(1999).
7 Ahima RS, Flier JS. Adipose tissue as an endocrine organ. Trends Endocrinol. Metab. 11, 332–337 (2000).
8 Fernàndez-Real JM, Ricart W. Insulin resistance and inflammation in an evolutionary perspective: the contribution of cytokine genotype/phenotype to thriftiness. Diabetologia 42, 1367–1374 (1999).
9 Hotamisligil GS, Spiegelman BM. Tumor necrosis factor: a key component of the obesity-diabetes link. Diabetes 43, 1271–1278 (1994).
10 Kern PA, Saghizadeh M, Ong JM, Bosch RJ, Deem R, Simsolo RB. The expression of tumor necrosis factor in human adipose tissue. Regulation by obesity, weight loss, and relationship to lipoprotein lipase. J. Clin. Invest. 95, 2111–2119 (1995).
11 Hotamisligil GS, Arner P, Caro JF, Atkinson RL, Spiegelman BM. Higher adipose tissue expression of tumor necrosis factor-a in human obesity and insulin resistance. J. Clin. Invest. 95, 2409–2415 (1995).
12 Peraldi P, Spiegelman B. TNF-alpha and insulin resistance: summary and future
13 Ofei F, Hurel S, Newkirk J, Sopwith M, Taylor R. Effects of an engineered human anti-TNF-alpha antibody [CDP571] on insulin sensitivity and glycaemic control in patients with NIDDM. Diabetes 45, 881–885 (1996).
14 Frittitta L, Youngren JF, Sbraccia P et al. Higher adipose tissue PC-1 protein content, but not tumour necrosis factor-alpha gene expression, is associated with a reduction of both whole body insulin sensitivity and insulin receptor tyrosine-kinase activity. Diabetologia 40, 282–289 (1997).
15 Woo KS, Chook P, Yu CW et al. Effects of diet and exercise on obesity-related vascular dysfunction in children. Circulation 109, 1981–1986 (2004).
16 Hedblad B, Nilsson P, Janzon L, Berglund G. Relation between insulin resistance and carotid intima–media thickness and stenosis in non-diabetic subjects: results from a cross-sectional study in Malmo, Sweden. Diabet. Med. 17(4), 299–307 (2000).
17 Flier JS, Kahn CR, Roth J. Receptor, antireceptor antibodies and mechanism of insulin resistance. N. Eng. J. Med. 300(8), 413–419 (1979).
18 Postman T, Kiessig ST. Enzyme immunoassay techniques: an overview. Immunol. Methods 150, 5–21 (1992).
19 Bouhours-Nouet N, Gatelias P, Boux C F, Rouleau S, Coutant R. The insulin like growth factor 1 response to growth hormone is higher in prepubertal children with obesity and tall stature. J. Clin. Endocrin. Metab. 92(2), 629–635 (2007).
20 Fukuhara A, Matsuda M, NishizawaM et al. Visfatin: apoprotein secreted by visceral fat that mimics the effect of insulin. Science 307(5708), 426–430 (2005).
21 Haider DG, Holzer G, Schaller G et al. The adipokine visfatin is markedly elevated in obese children. J. Pediatr. Gastroenterol. Nutr. 43(4), 548–549 (2006).
22 Berndt J, Klöting N, Kralisch S et al. Plasma visfatin concentrations and fat depot-specific mRNA expression in humans. Diabetes 54(10), 2911–2916 (2005).
23 Araki S, Dobashi K, Kubo K et al. Plasma visfatin concentration as a surrogate marker for visceral fat accumulation in obese children. Obesity 16(2), 384–388 (2008).
24 Davutoglu M, Ozkaya M, Guler E et al. Plasma visfatin concentrations in childhood
obesity: relationships to insulin resistance and anthropometric indices. Swiss Med. Weekly 139(1–2), 22–27 (2009).
25 Pagano C, Pilon C, Olivieri M et al. Reduced plasma visfatin/pre-B cell colony-enhancing factor in obesity is not related to insulin resistance in humans. J. Clin. Endocrinol. Metab. 91(8), 3165–3170 (2006).
26 Chen MP, Chung FM, Chang DM et al. Elevated plasma level of visfatin/pre-B cell colony-enhancing factor in patients with Type 2 diabetes mellitus. J. Clin. Endocrinol. Metab. 91(1), 295–299 (2006).
27 Zahorska-Markiewicz B, Olszanecka-Glinianowicz M, Janowska J et al. Serum concentration of visfatin in obese women. Metabolism 56(8), 1131–1134 (2007).
28 Oh YJ, Nam HK, Rhie YJ, Park SH, Lee KH. Low serum adiponectin levels in Korean children with a family history of Type 2 diabetes mellitus. Horm. Res. Paediatr. 77, 382–387 (2012).
nn� Association of adipokines with insulin resistance, obesity, and diabetes and its complications.
29 Kadowaki T, Yamaushi T, Kubota N, Hara K, Ueki K, Tobi K. Adiponectin and adiponectin receptors in insulin resistance, diabetes and metabolic syndrome. J. Clin. Inves. 116, 1784–1792 (2006).
30 Hara K, Yamaushi T, Imei Y, Manabi I, Nagai R, Kadowaki T. Reduced adiponectin level is associated with severity of coronary artery disease. Int. Heart J. 48, 149–153 (2007).
31 Lee JH, Chan JL, Yiannakouris N et al. Circulating resistin levels are not associated with obesity or insulin resistance in humans and are not regulated by fasting or leptin administration: cross-sectional and interventional studies in normal, insulin-resistant, and diabetic subjects. J. Clin. Endocrinol. Metab. 88, 4848–4856 (2003).
32 Degawa-Yamauchi M, Bovenkerk JE, Juliar BE et al. Serum resistin FIZZ3 protein is higher in obese humans. J. Clin. Endocrinol. Metab. 88, 5452–5455 (2003).
33 Hotamisligil GS, Shargill NS, Spiegelman BM. Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science 259, 87–91 (1993).
34 Borst SE. The role of TNF-alpha in insulin resistance. Endocrine 23, 177–182 (2004).