Standards for ectopic pregnancy and miscarriage: ultrasound for determining viable intrauterine
pregnancy clinical audit
Audit standard Guidance reference
Exceptions Definitions
Initial ultrasound scan
1. All women with pain and/or bleeding or atypical symptoms suggestive of early pregnancy problems are assessed by a healthcare professional before referral to an early pregnancy assessment service.
See data collection form, question 1.
1.2.3 A – Women who self-refer to an early pregnancy assessment service due to a recurrent miscarriage or a previous ectopic or molar pregnancy.
The healthcare professional may be a GP, accident and emergency (A&E) doctor, midwife or nurse.
Early pregnancy is defined as the first trimester.
Further details of the initial assessment can be found in section 1.3 of the guidance.
2. All women who attend an early pregnancy assessment service should be offered a transvaginal ultrasound scan.
See data collection form, question 2.
1.4.1 (key priority)
B – Women with an enlarged uterus or other pelvic pathology such as fibroids or an ovarian cyst who have a transabdominal ultrasound scan.
NICE recommends offering a transabdominal scan if a transvaginal ultrasound scan is unacceptable to the women.
Audit standard Guidance reference
Exceptions Definitions
Confirmed intrauterine pregnancy with no visible fetal heartbeat and a visible fetal pole – measuring crown–rump length
3a. All women with a confirmed intrauterine pregnancy, no visible fetal heartbeat and a visible fetal pole have crown–rump length measured.
See data collection form, questions 4, 5, 6 and 7.
1.4.5 None None
3b. Where the crown–rump length is less than 7.0 mm with a transvaginal ultrasound scan a second scan is performed a minimum of 7 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 7 and 8.
1.4.6 None None
3c. Where the crown–rump length is 7.0 mm or more with a transvaginal ultrasound scan a second opinion is sought on the viability of the pregnancy and/or a second scan is performed a minimum of 7 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 7 and 9.
1.4.7 None None
3d. Where crown–rump is measured with a transabdominal ultrasound scan the size of the crown–rump length is recorded and a second scan is performed a minimum of 14 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 7 and 10.
1.4.8 None None
Audit standard Guidance reference
Exceptions Definitions
Confirmed intrauterine pregnancy with no visible fetal heartbeat and no visible fetal pole – measuring mean gestational sac diameter
4a. All women with a confirmed intrauterine pregnancy with no visible fetal heartbeat and no visible fetal pole have mean gestational sac diameter measured.
See data collection form, questions 4, 5, 6 and 11.
1.4.5 None None
4b. If the mean gestational sac diameter is less than 25.0 mm using a transvaginal ultrasound scan, a second scan is performed a minimum of 7 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 11 and 12.
1.4.9 None None
4c. If the mean gestational sac diameter is 25.0 mm or more using transvaginal ultrasound scan, a second opinion is sought on the viability of the pregnancy and/or a second scan is performed a minimum of 7 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 11 and 13.
1.4.10 None None
4d. If the mean gestational sac diameter is measured using a transabdominal ultrasound scan, the size of the mean gestational sac diameter is recorded and a second scan is performed a minimum of 14 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 11 and 14.
1.4.11 None None
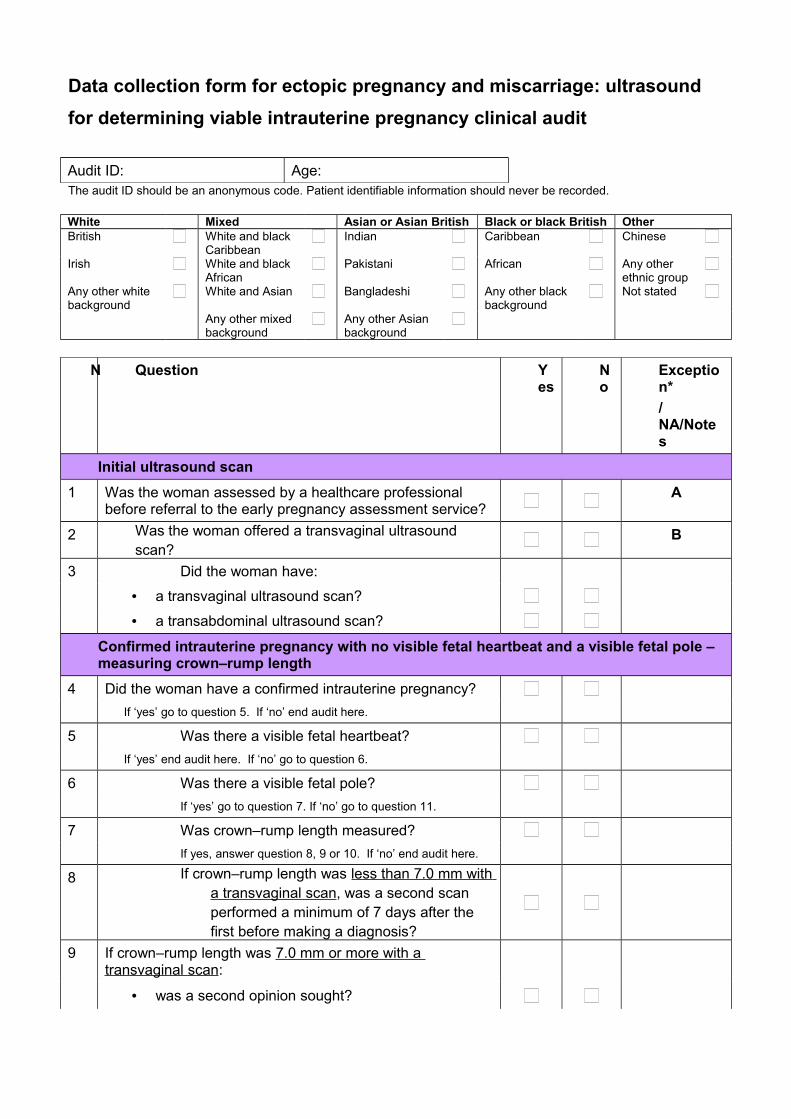
Data collection form for ectopic pregnancy and miscarriage: ultrasound
for determining viable intrauterine pregnancy clinical audit
Audit ID: Age:The audit ID should be an anonymous code. Patient identifiable information should never be recorded.
White Mixed Asian or Asian British Black or black British OtherBritish White and black
CaribbeanIndian Caribbean Chinese
Irish White and black African
Pakistani African Any other ethnic group
Any other white background
White and Asian Bangladeshi Any other black background
Not stated
Any other mixed background
Any other Asian background
N Question Yes
No
Exception*
/NA/Notes
Initial ultrasound scan
1 Was the woman assessed by a healthcare professional before referral to the early pregnancy assessment service?
A
2 Was the woman offered a transvaginal ultrasound scan?
B
3 Did the woman have:
• a transvaginal ultrasound scan?
• a transabdominal ultrasound scan?
Confirmed intrauterine pregnancy with no visible fetal heartbeat and a visible fetal pole – measuring crown–rump length
4 Did the woman have a confirmed intrauterine pregnancy?
If ‘yes’ go to question 5. If ‘no’ end audit here.
5 Was there a visible fetal heartbeat?
If ‘yes’ end audit here. If ‘no’ go to question 6.
6 Was there a visible fetal pole?
If ‘yes’ go to question 7. If ‘no’ go to question 11.
7 Was crown–rump length measured?
If yes, answer question 8, 9 or 10. If ‘no’ end audit here.
8 If crown–rump length was less than 7.0 mm with a transvaginal scan, was a second scan performed a minimum of 7 days after the first before making a diagnosis?
9 If crown–rump length was 7.0 mm or more with a transvaginal scan:
• was a second opinion sought?
N Question Yes
No
Exception*
/NA/Notes
• was a second scan performed a minimum of 7 days after the first before making a diagnosis?
10 If crown–rump length was measured using a transabdominal scan:
• was the size of the crown–rump length recorded?
• was a second scan performed a minimum of 14 days after the first before making a diagnosis?
End audit here.
Confirmed intrauterine pregnancy with no visible fetal heartbeat and no visible fetal pole – measuring mean gestational sac diameter
11 Was mean gestational sac diameter measured?
If yes, answer question 12, 13 or 14. If ‘no’ end audit here.
12 If mean gestational sac diameter was less than 25.0 mm using a transvaginal scan, was a second scan performed a minimum of 7 days after the first before making a diagnosis?
13 If mean gestational sac diameter was 25.0 mm or more using a transvaginal scan:
• was a second opinion sought on the viability of the
pregnancy?• was a second scan performed a minimum of 7 days
after the first before making a diagnosis?
14 If mean gestational sac diameter was measured using a transabdominal scan:
• was the size of the mean gestational sac diameter recorded?
• was a second scan performed a minimum of 14 days after the first before making a diagnosis?
End audit here.
*Circle exception codes as appropriate.
Exception codes
A – Women who self refer to a dedicated early pregnancy assessment service due to a previous ectopic or molar pregnancy.
B – Women with an enlarged uterus or other pelvic pathology such as fibroids or an ovarian cyst who have a transabdominal ultrasound scan.
Action plan for ectopic pregnancy and miscarriage: ultrasound for determining a viable intrauterine
pregnancy clinical audit
Action plan lead
Name: Title: Contact:
The ‘Actions required’ should specifically state what needs to be done to achieve the recommendation. All updates to the action plan should be included in the ‘Comments’ section.
Recommendation Actions required (specify ‘None’, if none required)
Action by date
Person responsible
Comments/action status(Provide examples of action in progress, changes in practices, problems encountered in facilitating change, reasons why recommendation has not been actioned etc)
Change stage
(see Key)
When making improvements to practice, organisations may like to use the tools developed by NICE to help implement the clinical guideline on ectopic pregnancy and miscarriage.
KEY (Change status)1 Recommendation agreed but not yet actioned2 Action in progress3 Recommendation fully implemented4 Recommendation never actioned (please state reasons)5 Other (please provide supporting information)
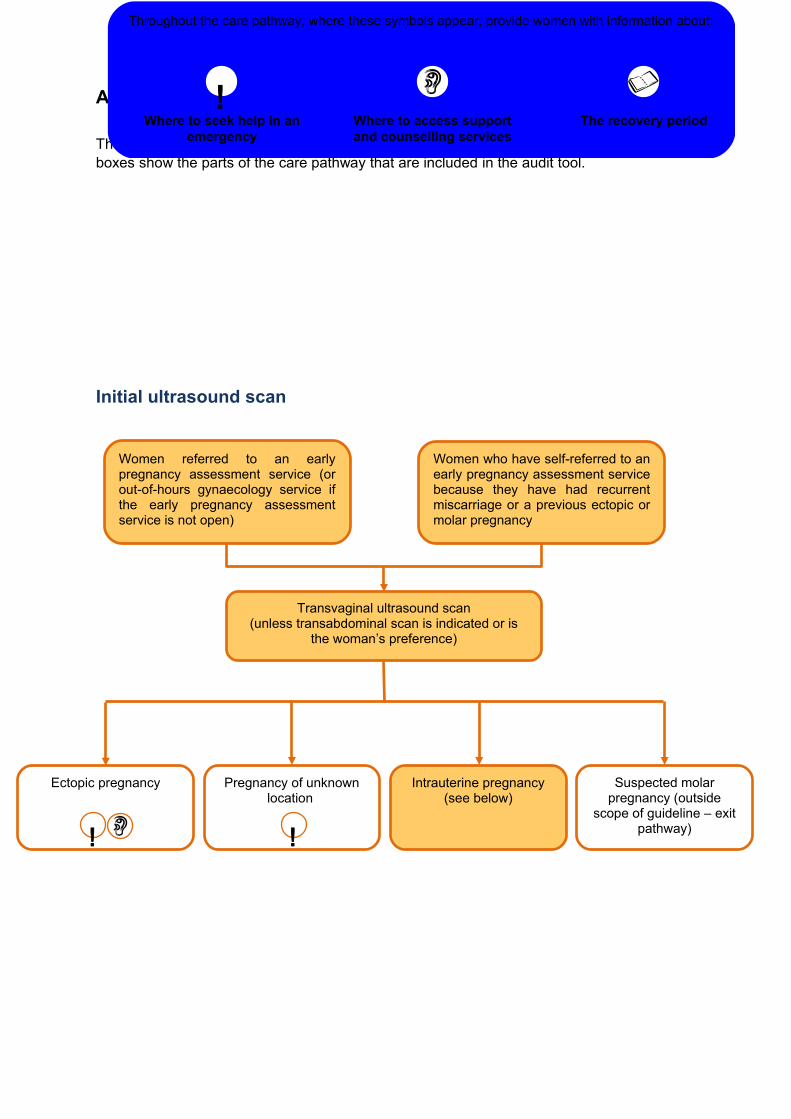
These extracts from the care pathway has been taken from the full guideline. The shaded boxes show the parts of the care pathway that are included in the audit tool.
Initial ultrasound scan
Throughout the care pathway, where these symbols appear, provide women with information about:
Where to seek help in an emergency
Where to access support and counselling services
The recovery period!
Ectopic pregnancy Pregnancy of unknown location
Transvaginal ultrasound scan(unless transabdominal scan is indicated or is
the woman’s preference)
Suspected molar pregnancy (outside
scope of guideline – exit pathway)
Intrauterine pregnancy (see below)
Women referred to an early pregnancy assessment service (or out-of-hours gynaecology service if the early pregnancy assessment service is not open)
Women who have self-referred to an early pregnancy assessment service because they have had recurrent miscarriage or a previous ectopic or molar pregnancy