Page 1
•
•
•
•
.;
."
I I
, /
0994
C()O\,' 3 I,'
:iD JUN 1992
FAMI,-V IN""ORMATlON CENTRE
AUSTRA~I.~ I:;S:liUT~ Of rA;J~Y STUDICS 300 QUEEN STREET
MEL.BOUR~E vie. 3000
REPORT ON STAGE ONE OF THE EARLY CHILDHOOD CONTEXTS STUDY:
prel~nary findings
Gay Ochiltree and Don Edgar
This study is conducted in conjunction with the Children's Service
Office in South Australia, the Office of the Family in Western Australia
and with assistance'from the Commonwealth Department of Community
Services and Health.
The following staff provided research assistance and or advice on the
project: Peter Schmidt, Andrew Prolisko, Peter McDonald, Gillian
Hamerston, Violet Kolar, Vance Merrill, Sandra Marsden and Evelyn
Greenblatt. '--l
Page 2
- 2 -
CONTENTS
1. Introduction
2. Method and sample characteristics
3. Mother's work patterns and child care
arrangements
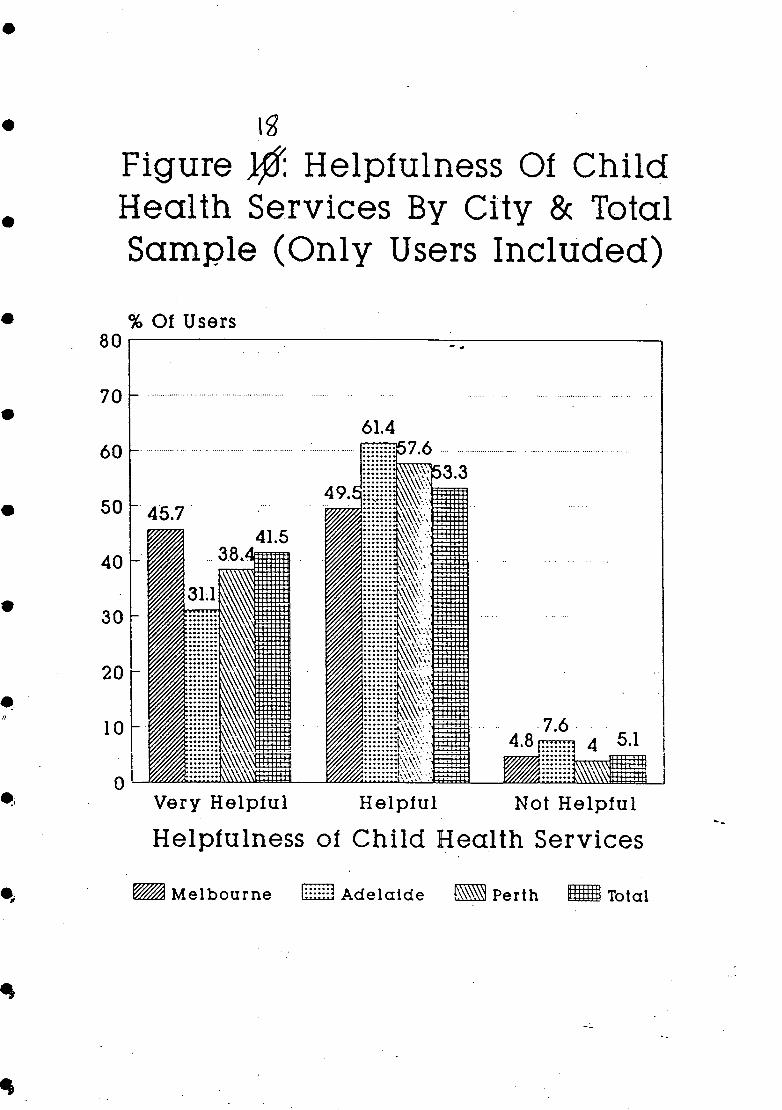
4. 'An ear to listen and a shoulder to cry
on': the use of child health services in
Melbourne, Adelaide and Perth.
5. The effects of non-maternal care in the
first twelve months of life on children
in the first year of school
Page
3 ..
13
24
49
76
•
•
•
•
•
•
•
•
•
•
•
Page 3
•
•
•
•
•
•
•
- 3 -
Introduction
until recently, most Australian children under the age of five years were
cared for at home by their mothers; these days, due to social and economic
changes in society, increasing numbers of mothers of pre-school children are
entering the paid work force and their children are in the care of others.
This trend is c~mmon to most Western countries, not just in Australia, as
married women return to work after bearing children. In 1954, only 13 per
cent of married women were in the ~aid workforce. By 1966 it was 29
per cent (Prosser, 1981). By June 1990, the rate of participation of
mothers with children in the 0 to 4 age group reached 46 per cent, of whom
27.9 per cent were working part-time, 14.4 per cent full-time and 4.0 per
cent were unemployed. However, as children get older, the maternal labour
force participation rate increases and stands at 69.5 per cent for mothers
of children in the 5 to 14 age group, with 30.3 per cent of mothers working
full-time, 34.9 per cent part-time and 4.3 per cent unemployed (ABS, 1990).
Mothers work outside the home for many reasons, but financial need is a
pressing incentive to many as the cost of bringing up children increases,
and the prices of homes and rents rise. Some mothers work for career
reasons, ensuring their skills do not become out-of-date and because they
like the mental stimulation and the independence associated with earning
their own money. Whatever the reasons that mothers of pre-school children
work outside the home may be, the result is that the early childhood
experiences of many children are different from those of previous
generations.
It is important to note that this trend to working mothers is not new
historically. Before the Industrial Revolution both men and women took care
of children as they went about their work at home or in the local area. In
the early days of the Industrial Revolution children of the working class
worked in the factories with their parents, until children's hours of work
were made shorter thus breaking up the family unit. Gradually children's
labour was no longer needed as machines improved (Harrison 1973). The
separation of home and work that occurred with industrialisation led to the
isolation of middle-class women in their homes and set the scene for the
idealisation of motherhood that occurred in the late nineteenth century
(Dally 1982; Zelizer 1985). Over time this pattern extended to working
class mothers, even though it was more difficult for them to live up to the
ideal.
Page 4
- 4 -
Early childhood is an important stage in child development; the progress
of children physically, intellectually, socially and emotionally is greatest
in the first five years of life. From birth on children are learning all
the time, and whether at home with mother or in the care of others, those
around them are involved in this learning process even if they are not aware
of it. It is in early childhood that children acquire language, and that
the foundations are laid for literacy, which is so important for success at
school, and later for employment. Whether children are cared for at home or
away from home, it is important that they receive care which not only keeps
them safe and healthy but enables them to participate in a modern society
which requires independent, literate and educa~ed citizens (~nkeles, 1965;
Clauscen, 1966; Smith, 1969; Edgar, 1971, 1974, 1975, 1980).
There is considerable debate concerning the care of children in the
period between birth and starting school. Central to this debate are
competing views on the effects of non-maternal care on young children, the
importance of the mother-child relationship and, with the increase in
mothers returning to the paid work-force, problems regarding the
availability of child care, and issues relating to the quality and cost of
that care. While many children whose mothers work are cared for in child
care centres or family daycare schemes, many others are.cared for informally
by relatives, neighbours or friends, either in their own homes or in the
homes of the care-giver; others again are cared for by privately employed
baby-sitters, housekeepers, or Nannies in their own home. Although child
care provision is often regarded largely as a women'.s issue, because
availability is closely linked with equal opportunities for ~omen, it is
also important that children should receive care which is appropriate to
their developmental needs and to the needs of society.
The Early Childhood Study was designed in response to these changes in
the care of pre-school children and arguments about the effects on children.
The major objectives of this study are:
(i) to provide a comprehensive picture of Australian mothers'
experiences of bringing up children in a variety of circumstances (in
metropolitan areas), from birth until the first year at school, (whether
mother was in the paid workforce for some of the time or whether she
remained at home with the child).
•
•
•
•
•
•
•
•
•
•
•
Page 5
•
•
•
•
• ~
•
•
•
- ~ -
(ii) to examine the relationship between differing contexts of child
care and the development of child competence by time of the first year
of school.
Australia today
,. The trend to increased participation of mothers in the paid work force is
only one of the changes in the social context in which young children are
now living. There are several-others. The trend is to small families;
between 1971 and 1982- the total fertility rat& dropped from 2.87 births per
woman to 1.94 births;, by 1988 it was 1.84 (ASS 1988). However, McDonald
(1.990) points out that despite the lower Total Fertility Rate for all women,
over a lifetime 32 per cent of all women would have three or more children.
Younger women are de~aying childbearing and older women are ending
childbearing at a younger age. Families are therefore not only smaller but
children are closer in age (Department of Immigration, 1988).
With the increase in divorce and separation in recent years more single
parents are bringing up children alone. Estimates are that about 3.9 per
cent of children have experienced the divorce of their parents by the time
they are five years old, and even more children in this age group have , experienced the separation of their parents (Carmichael and McDonald, 1988).
There is increased poverty, much of which is associated with living in a
female headed single parent family after divorce, however there has also
been an increase in ~he proportion of married couple families living in
poverty, usually related to unemployment (Maas, 1987). In the period
between 1972-73 and 1985-86, the number of children in poverty had risen
from 6 per cent to 21 per cent of all children (Brownlee and King., 1989).
Poverty is known to have a negative effect on child health, wellbeing, and
educational opportunities (Edgar, Keane and McDonald, 1989).
Where once Austr~lia_ was notable for the common British background of
its people, Australia's population has undergone a major cultural change
with the arrival 'of 3.5 million immigrants since World War 11, and is now a
country notable for its mixture of races and cultures. As a result of this
influx of migrants, one in every seven Australians speaks a l~nguage other
than English in the home (Department of Immigration, 1988). At the time of
Page 6
- 6 -
the 1986 Census just on 21 per cent of the population was born overseas
(Department of Immigration, 1988). Today migrants are encouraged to retain
their own cultural identity and government policy encourages multi
cu1turalism, unlike the earlier policy of assimilation, where migrants were
expected to discard their own language and cultural heritage and to adopt
Australian ways.
To sum up, the current context for bringing up young children in present
day Australia is very different from that of previous decades; mothers are
more likely to be working before the child goes to school, there are more
single parents rearing children alone, there rs increased poverty, many
children are growing up in different cultural contexts from the dominant
Anglo-Celtic culture, and more children are growing up with English as a
second language or with exposure to languages other than English.
Design of the Early childhood study
The Australian Early Childhood study was designed both to describe and to
examine the relationship between a broad range of family factors, child
characteristics, and different patterns of caring for children, including
non-maternal care, in the years between birth and starting school and a
range of child outcomes in the first year of school. The study design is of
two complementary stages; stage 1 consists of a mailed-out questionnaire to
mothers of children in the first year of school. Data collected in this
stage of the study includes information on the various forms of care used
for the child in the years before starting school, mother's current work
situation and average hours of paid work for each year since birth, average
hours that the child was in the care of others for each year from birth,
mother's use of and satisfaction with child health services, an indication
of the child's competence as measured by a modified form of the ACER Parent
Checklist, and basic social and economic information about the family. This
report is based on information from Stage 1 of the study only.
Although this report does not contain information from Stage 2 of the
Early Childhood study, it is useful to have some understanding of the links
between Stage 1 and Stage 2. Information collected in Stage One of the
study, on the different contexts of caring for children, enabled the precise
selection of the smaller Stage 2 sample. Mothers were selected on the basis
of the forms of care they had used for their children in the pre-school
years; the selected mothers were interviewed in depth about the particular
•
•
•
•
•
•
•
•
•
•
•
•
Page 7
•
•
•
•
•
•
•
•
•
• I
• I
- 7 -
child who was the focus of the study, their family, reasons for working or
not working and, if they worked, how they managed both home and work
responsibilities. Mother's reasons for the choice of different forms of
child care, and information on the health and wellbeing of mother and child
was also obtained. Table 1 shows aspects of information about the family
context which were collected in stages 1 and 2 of the study (information
collected in St~ge 1 is indicated by *). Table 2 shows information about
child care contexts which were collected in the two stages of the study.
INSERT TABLES 1 AND 2 HERE
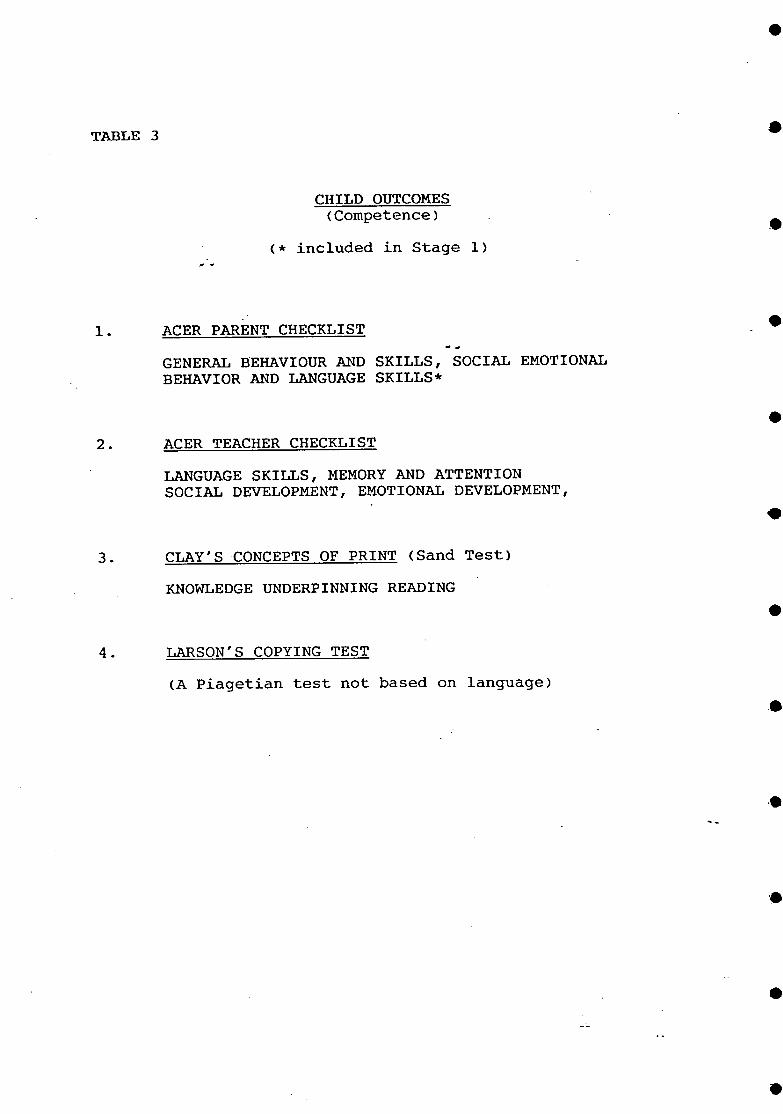
At stage 2 the competence of the target child. in the first year of
school was tested using several measures - Clay's concepts of print
(reading), Larson's copying test (a Piagetian non-language based test)
individually administered in the child's own home. In addition teachers
filled in the ACER teacher checklist (which includes teacher's perceptions
of the child's memory and attentio~, language skills, and social and
emotional development). Table 3 shows the competence outcome measures used
in the study (* indicates that the measure was used in Stage 1).
Information on Stage Two of the study will come out in a series of reports
and articles and will be available separately. The rest of this report
refers to Stage 1 only.
INSERT TABLE 3 HERE
Child competence
The overall concern of this study is the relationship between different
contexts of caring for children. in the pre-school years and child
competence. The focus is competence, rather than a narrow focus on
pathological behaviour, adjustment, or simply.educational achievement,
because the concept of competence stresses positive aspects of development
rather than deficits, and it encompasses a wide range of human functioning
(Wine, 1981). Competence is having the knowledge, skills and abilities
suitable for life in contemporary society, and includes also the intra
personal elements of control and efficacy. competence varies to some extent
according to the community and social group in which the individual lives,
but some basic abilities are necessary for people in all walks of life.
Page 8
TABLE 1
FAMILY CONTEXT
(* included in Stage 1)
SOCIAL BACKGROUND FAMILY INCO~E * EDUCATION bEVEL OF BOTH PARENTS * OCCUPATION OF BOTH PARENTS * FAMILY STRUCTURE (2 parents, 1 parent, remarried) * ETHNICITY *
FAMILY PROCESSES MOTHER-CHILD RELATIONSHIP (as perceived by mother) FATHER-CHILD RELATIONSHIP (as perceived by mother) DIVISION OF LABOUR IN THE FAMILY (as perceived by mother) MARITAL CONFLICT (as perceived by mother)
PARENTING MOTHER'S VALUES ASPIRATIONS FOR THE CHILD ENCOURAGEMENT OF EDUCATION PARENTING STYLE
MOTHER MOTHER'S HEALTH NOW AND AFTER BIRTH OF CHILD MOTHER'S WELLBEING LIFE SATISFACTION * LIFE EVENTS SCALE EMPLOYMENT HISTORY SINCE BIRTH OF CHILD
NEIGHBOURHOOD HOUSING QUALITY NEIGHBOURHOOD QUALITY PERCEPTION OF SERVICES MOBILITY
CHILD CHARACTERISTICS SEX * POSITION IN BIRTH ORDER * DISABILITY * HEALTH PERSONALITY NOW AND AS AN INFANT (mother's perception) CURRENT SITUATION AT SCHOOL
•
•
•
•
•
•
•
•
• ...
•
•
•
Page 9
•
•
•
•
•
•
•• . J
TABLE 2
CHILD CARE CONTEXTS
(* included in Stage 1)
AGE OF CHILD WHEN FIRST IN NON-MATERNAL CARE * .. ,.
CARE CONTEXT
FORMAL CARE
INFORMAL CARE
AT HOME (includes kindergarten) * HOME AND OTHER CARE *
.. KINDERGARTEN * CHILD CARE CENTRE (public/private) * FAMILY DAYCARE * WORK-BASED CHILD CARE *
R~LATIVES * FRIENDS * NEIGHBOURS * NANNY/BABYSITTER * HOUSEKEEPER * LEFT ALONE * SIBLINGS *
COMBINATIONS OF ABOVE CARE (over the pre-school years)*
MULTIPLE CONTEXTS * SIMPLE CONTEXTS * CONTINUITY/DISRUPTION STABILITY/INSTABILITY
MOTHER'S SATISFACTION WITH CARE SITUATIONS
CHOICE OF CARE
IN GENERAL * IN EACH PARTICULAR CARE SITUATION
QUALITIES LOOKED FOR ADVANTAGES/DISADVANTAGES ARRANGEMENTS FOR SICK CHILD ARRANGEMENTS FOR MORE THAN ONE CHILD
Page 10
TABLE 3
1.
CHILD OUTCOMES (Competence)
(* included in Stage 1)
ACER PARENT CHECKLIST
GENERAL BEHAVIOUR AND SKILLS, SOCIAL EMOTIONAL BEHAVIOR AND LANGUAGE SKILLS*
2. ACER TEACHER CHECKLIST
LANGUAGE SKILLS, MEMORY AND ATTENTION SOCIAL DEVELOPMENT, EMOTIONAL DEVELOPMENT,
3. CLAY'S CONCEPTS OF PRINT (Sand Test)
KNOWLEDGE UNDERPINNING READING
4. LARSON'S COPYING TEST
(A Piagetian test not based on language)
•
•
•
•
•
•
•
•
•
•
•
Page 11
•
•
•
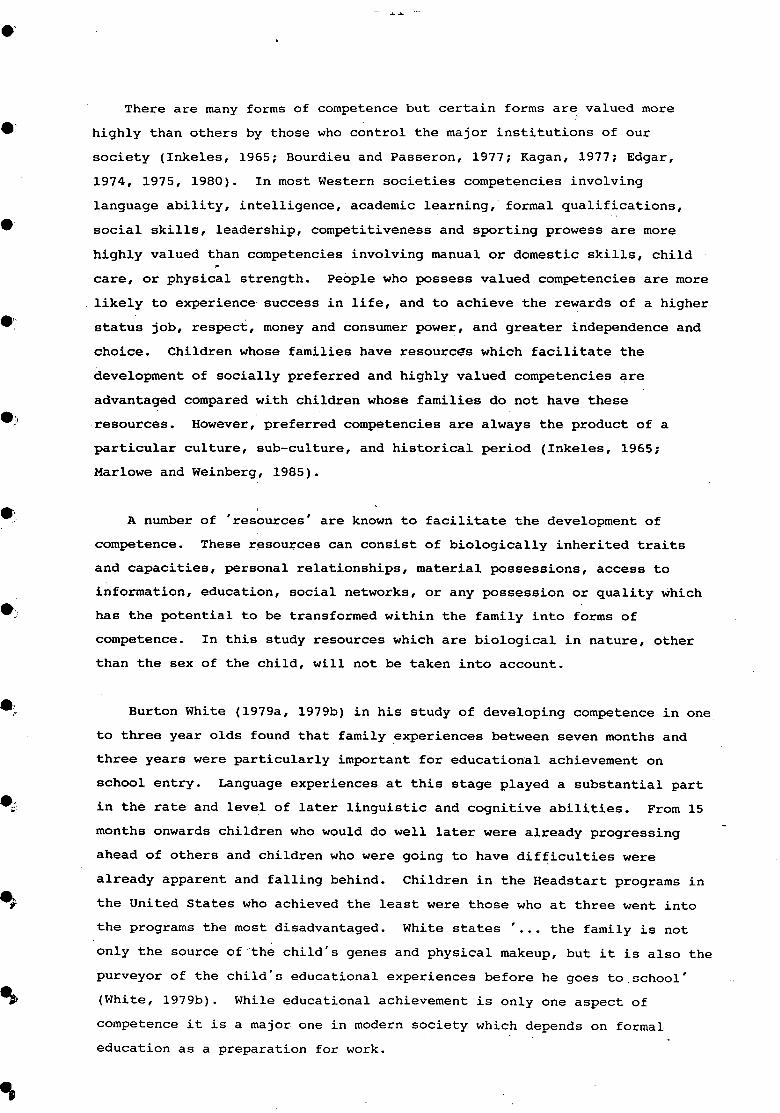
There are many forms of competence but certain forms are. valued more
highly than others by those who control the major institutions of our
society (Inkeles, 1965; Bourdieu and Passeron, 1977; Kagan, 1977; Edgar,
1974, 1975, 1980). In most western societies competencies involving
language ability, intelligence, academic learning, formal qualifications,
social skills, leadership, competitiveness and sporting prowess are more
highly valued than competencies involving manual or domestic skills, child
care, or physical strength. People who possess valued competencies are more
likely to experience success in life, and to achieve the rewards of a higher
status job, respect, money and consumer power, and greater independence and
choice. Children whose families have resourcGs which facilitate the
development of socially preferred and highly valued competencies are
advantaged compared with children whose families do not have these
resources. However, preferred competencies are always the product of a
particular culture, sub-culture, and historical period (Inkeles, 1965;
Marlowe and Weinberg, 1985).
, A number of 'resources' are known to facilitate the development of
competence. These resources can consist of biologically inherited traits
and capacities, personal relationships, material possessions, access to
information, education, social networks, or any possession or quality which
has the potential to be transformed within the family into forms of
competence. In this study resources which are biological in nature, other
than the sex of the child, will not be taken into account.
Burton White (1979a, 1979b) in his study of developing competence in one
to three year olds found that family experiences between seven months and
three years were particularly important for educational achievement on
school entry. Language experiences at this stage played a substantial part
in th~ rate and level of later linguistic and cognitive abilities. From 15
months onwards children who would do well later were already progressing
ahead of others and children who were going to have difficulties were
already apparent and falling behind. Children in the Headstart programs in
the United states who achieved the least were those who at three went into
the programs the most disadvantaged. White states' ••• the family is not
only the source of "the child's genes and physical makeup, but it is also the
purveyor of the child's educational experiences before he goes to school'
(White, 1979b). While educational achievement is only one aspect of
competence it is a major one in modern society which depends on formal
education as a preparation for work.
Page 12
- 12 -
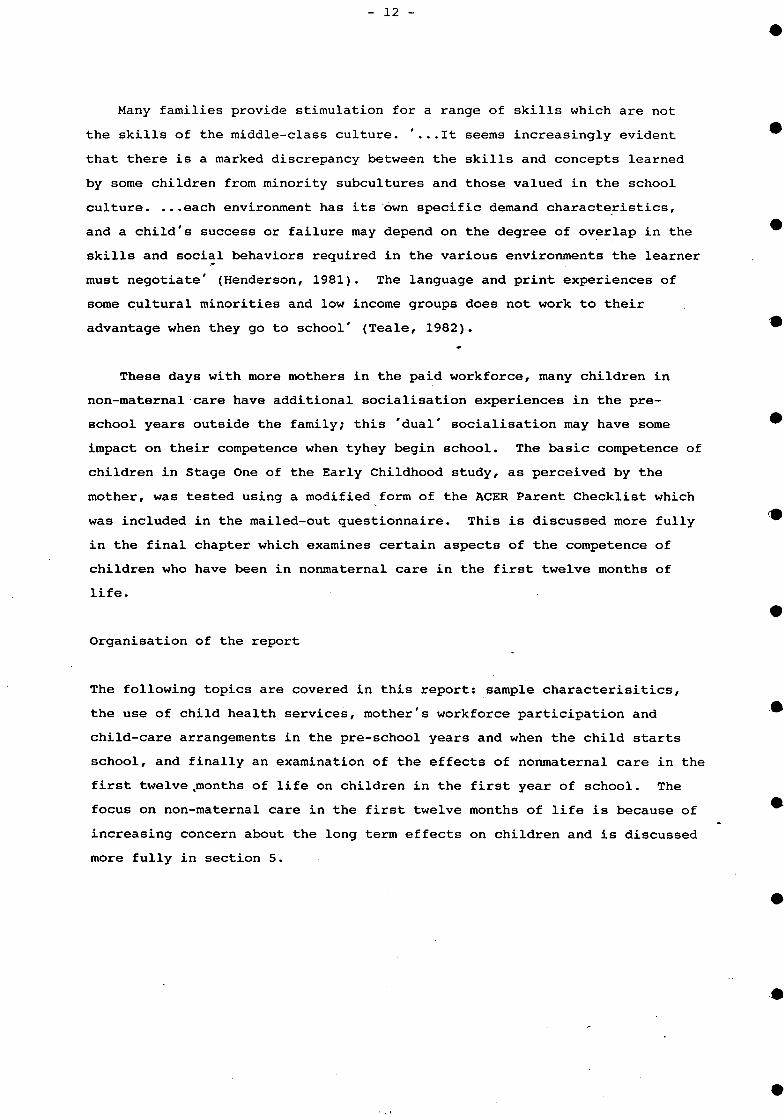
Many families provide stimulation for a range of skills which are not
the skills of the middle-class culture. ' ... It seems increasingly evident
that there is a marked discrepancy between the skills and concepts learned
by some children from minority subcultures and those valued in the school
culture •••• each environment has its own specific demand characteristics,
and a child's success or failure may depend on the degree of overlap in the
skills and social behaviors required in the various environments the learner
must negotiate' (Henderson, 1981). The language and print experiences of
some cultural minorities and low income groups does not work to their
advantage when they go to school' (Teale, 1982).
These days with more mothers in the paid workforce, many children in
non-maternal care have additional socialisation experiences in the pre
school years outside the family; this 'dual' socialisation may have some
impact on their competence when tyhey begin school. The basic competence of
children in Stage One of the Early Childhood study, as perceived by the
mother, was tested using a modified form of the ACER Parent Checklist which
was included in the mailed-out questionnaire. This is discussed more fully
in the final chapter which examines certain aspects of the competence of
children who have been in nonmaternal care in the first twelve months of
life.
Organisation of the report
The following topics are covered in this report: sample characterisitics,
the use of child health services, mother's work force participation and
child-care arrangements in the pre-school years and when the child starts
school, and finally an examination of the effects of nonmaternal care in the
first twelve.months of life on children in the first year of school. The
focus on non-maternal care in the first twelve months of life is because of
increasing concern about the long term effects on children and is discussed
more fully in section 5.
•
•
•
•
•
•
•
•
•
•
•
•
Page 13
e
•
e
e
e.
e,
e· J
e,i
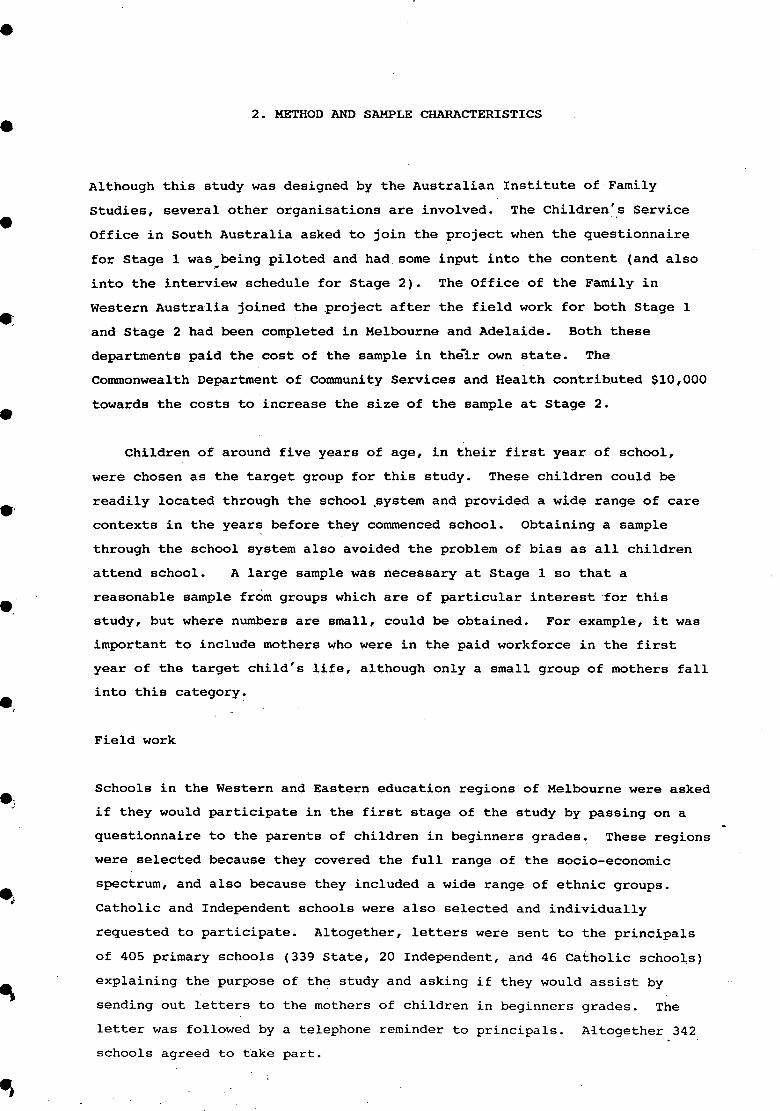
2. METHOD AND SAMPLE CHARACTERISTICS
Although this study was designed by the Australian Institute of Family
Studies, several other organisations are involved. The Children's Service
Office in South Australia asked to join the project when the questionnaire
for Stage 1 was being piloted and had. some input into the content (and also .~
into the interview schedule for Stage 2). The Office of the Family in
Western Australia joined the project after the field work for both Stage 1
and Stage 2 had been completed in Melbourne and Adelaide. Both these
departments paid the cost of the sample in their own state. The
Commonwealth Department of Community Services and Health contributed $10,000
towards the costs to increase the size of the sample at Stage 2.
Children of around five years of age, in their first year of school,
were chosen as the target group for this study. These children could be
readily located through the school .system and provided a wide range of care
contexts in the years before they commenced school. Obtaining a sample
through the school system also avoided the problem of bias as all children
attend school. A large sample was necessary at Stage 1 so that a
reasonable sample from groups which are of particular interest for this
study, but where numbers are small, could be obtained. For example, it was
important to include mothers who were in the paid workforce in the first
year of the target child's life, although only a small group of mothers fall
into this category~
Field work
Schools in the Western and Eastern education regions of Melbourne were asked
if they would participate in the first stage of the study by passing on a
questionnaire to the parents of children in beginners grades. These regions
were selected because they covered the full range of the socio-economic
spectrum, and also because they included a wide range of ethnic groups.
Catholic and Independent schools were also selected and individually
requested to participate. Altogether, letters were sent to the principals
of 405 primary schools (339 State, 20 Independent, and 46 Catholic schools)
explaining the purpose of the study and asking if they would assist by
sending out letters to the mothers of children in beginners grades. The
letter was followed by a telephone reminder to principals. Altogether 342
schools agreed to take part.
Page 14
- 14 -
Children's Services Office South Australia took a slightly different
approach to the selection of Adelaide schools. Invitations to participate
in the study were sent to 357 schools: 63 State Junior primary schools, 145
State Primary schools, 81 Independent and 68 catholic Parish schools. One
hundred and thirty-nine schools agreed to take part. The lower ~esponse of
Adelaide schools is probably because a draft copy of the questionnaire was
included with t~e ·letter to the principal; some principals objected to the
question about family income on the grounds that it was intrusive. Even so,
the schools willing to take part represented more children than the
Children's Services Office could afford to process. For this reason schools
in each of the four regional areas which had agreed to take part were ranked
on a scale of one to three, indicating need priorities and taking account
the numbers of children at each. Selection took into account socio-economic
status, ethnicity and newly developing areas. Ninety-four schools were
selected, 17 Junior Primary, 47 Primary, 15 Independent and 15 Catholic.
The Office of the Family in Pe~th followed a similar procedure to that
taken in Melbourne. Schools that were invited to take part in the study
covered the socio-economic range and included children of many ethnic
backgrounds. Some independent and Catholic schools were also invited to
take part. Altogether 59 schools in W.A. agreed to participate: 2
Independent, 9 Catholic, and 48 state schools.
Although the Office of the Family joined the study after the fieldwork
in Melbourne and Adelaide was complete, all fieldwork procedures were the
same. Questionnaires were sent to mothers of all children in beginners
grades in the schools which had agreed to take part. Included with the
questionnaire was a letter explaining the purpose of the study and asking
mothers to return the completed questionnaire to the Institute, in the
enclosed reply-paid envelope. A letter of explanation in the major
community languages was also included. Principals received a copy of all
information which the mothers received, and a letter explaining the
procedures. They also received envelopes containing two reminder letters
for parents which were to be sent out a week and a fortnight after the
questionnaire. The first reminder letter was accompanied by another in the
major community languages. All printed material included the names and
telephone numbers of people who could be contacted for assistance with
language problems or other difficulties.
•
•
•
•
•
•
•
•
•
•
•
•
Page 15
•
•
•
•
•
•
•
.,
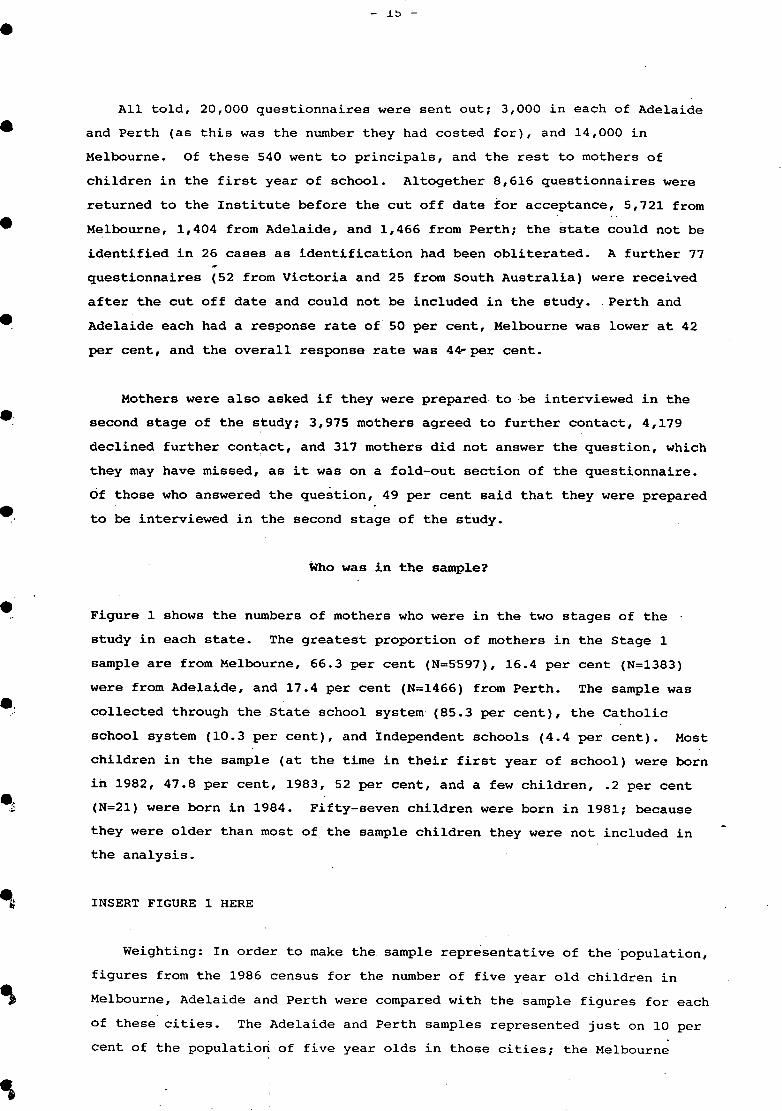
All told, 20,000 questionnaires were sent out; 3,000 in each of Adelaide
and Perth (as this was the number they had costed for), and 14,000 in
Melbourne. Of these 540 went to principals, and the rest to mothers of
children in the first year of school. Altogether 8,616 questionnaires were
returned to the Institute before the cut off date for acceptance, 5,721 from
Melbourne, 1,404 from Adelaide, and 1,466 from Perth; the state could not be
identified in 26 cases as identification had been obliterated. A further 77
questionnaires (52 from Victoria and 25 from South Australia) were received
after the cut off date and could not be included in the study. Perth and
Adelaide each had a response rate of 50 per cent, Melbourne was lower at 42
per cent, and the overall response rate was 4~per cent.
Mothers were also asked if they were prepared to be interviewed in the
second stage of the study; 3,975 mothers agreed to further contact, 4,179
declined further cont~ct, and 317 mothers did not answer the question, which
they may have missed, as it was on a fold-out section of the questionnaire.
Of those who answered the question, 49 per cent said that they were prepared
to be interviewed in the second stage of the study.
Who was in the sample?
Figure 1 shows the numbers of mothers who were in the two stages of the
study in each state. The greatest proportion of mothers in the Stage 1
sample are from Melbourne, 66.3 per cent (N=5597), 16.4 per cent (N=1383)
were from Adelaide, and 17.4 per cent (N=1466) from Perth. The sample was
collected through the State school system- (85.3 per cent), the Catholic
school system (10.3 per cent), and Independent schools (4.4 per cent). Most
children in the sample (at the time in their first year of school) were born
in 1982, 47.8 per cent, 1983, 52 per cent, and a few children, .2 per cent
(N=21) were born in 1984. Fifty-seven children were born in 1981; because
they were older than most of the sample children they were not included in
the analysis.
INSERT FIGURE 1 HERE
Weighting: In order to make the. sample representative of the population,
figures from the 1986 census for the number of five year old children in
Melbourne, Adelaide and Perth were compared with the sample figures for each
of these cities. The Adelaide and Perth samples represented just on 10 per
cent of the populatiort of five year olds in those cities; the Melbourne
Page 16
FIGURE 1: SAMPLES FOR STAGES I.AND 2 AUSTRALIAN EARLY CHILDHOOD ST.UDY
STAGE 1: MAILED QUESTIONNAIRE TO MOTHERS OF CHILDREN IN THE FIRST- YEAR OF SCHOOL
I I MELBOURNE ! 5{>19 I i I
ADELAIDE 1386
PERTH 1451
TOTAL 8456
STAGE 2: MOTHER INTERVIEWS & CHILD TESTING
MELBOURNE 446
ADELAIDE 182
PERTH 100
TOTAL 728
•
•
•
•
••
•
•
•
•
•
•
•
Page 17
•
•
•
•
•
•
•
eo
e~
- J../ -
sample was 14 per cent. of the population of five year olds. A weighting
factor was calculated for each city and the sample was weighted so that it
proportionally represents the population of five year olds in the three
cities combined.
As can be seen in Figure 2, for 44.2 per cent of the sample the target
child (who was in the first year of school) was the first born (this
category included only children), 37.8 per cent were the last born child,
and 18 per cent were middle children.
INSERT FIGURE 2 HERE
Because of the ethnic diversity of the Australian community, it was
important that the sample represented this range. Figure 3 shows that
almost a fifth of the sample (18.1 per cent) spoke a language other than
English in the home. Slightly more Melbourne mothers reported speaking a
language other than English in the home than Adelaide or Perth mothers.
Both parents were born in English speaking countries in approximately 74.1
per cent of families. In 13.2 per cent of families, one parent was born in
a non-English speaking country while the other was not. In another 12.7 per
cent of families, both parents were born in non-English speaking countries.
Melbourne had more families (14.9 per cent) where both parents were born in
non-English speaking countries in the sample, than Perth, 11.7 per cent, and
Adelaide had the least with 7.3 per cent (these percentages omit single
parent families and stepfamilies, and were confined to families where both
parents were present).
INSERT FIGURE 3 HERE
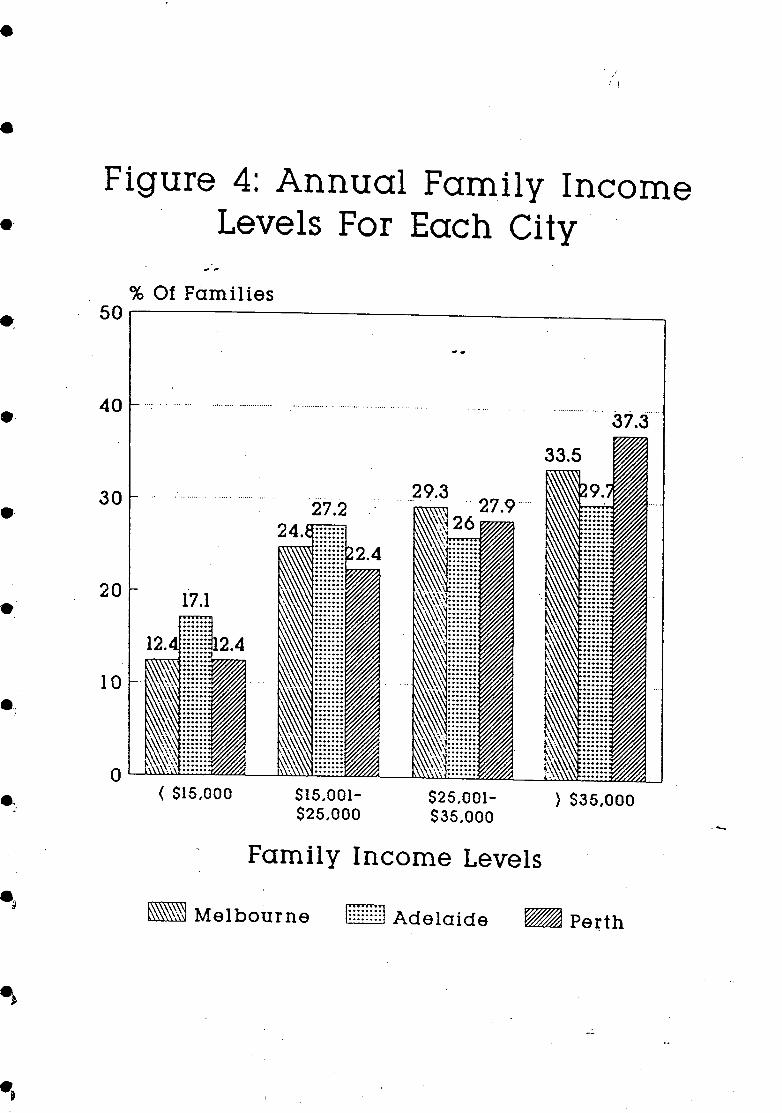
Figure 4 shows family income levels broken into four categories for each
city. As can be seen in Figure 4, a slightly higher percentage of the
Adelaide sample was in the two lowest income groups than for the other two
cities.
INSERT FIGURE 4 HERE
Page 18
.....
Figure 2: Birth. Order Of Children In Sample
% Of sample
Figure 3: Language Other Than English Spoken At Home By
City & Total
7. Of famllLet
lOO~--------------------------~
Melboarne Adelaido Perth TotAL
~ Only Enqlllh ~ Othor Lanqaaqe
•
•
•
•
•
•
•
•
•
•
•
•
Page 19
• i,
• Figure 4: Annual Family Income
e· Levels For Each Ci ty .
e·
e·
•
e.
.:J
. . .. .. % 01 Families
50~--------------------------------~
40 ....
30
20
10
< S15,000 SI5,001-$25,000
$25,001-$35,000
Family Income Levels
} $35,000
- Melbourne gmmn Adelaide ~ Pe~th
Page 20
- 20 -
Comparison of the sample with population
To examine the extent to which this sample represents the population it was
compared with the 1986 Census of Population on several important demographic
characteristics: birth place of mother and partner, mother's marital status,
the employment status of mother and partner, and annual family income. As
the census tape .does not identify the three cities used in this study, the
comparison was made with all metropolitan cities in Australia. Census
figures for families with children aged five (the age of most children in
the sample at the time of data collection) were appropriate when comparing
family income, marital status and the work status of the parents. However,
when comparing the birthplace of parents census figures for families with
children aged 2 or 3, the actual age of many children in the sample at the
time of the census, were more appropriate.
Table 4 compares the marital status of mothers in the sample with census
figures for mothers with children qf similar age. As can be seen there were
no significant differences between the sample and the population in terms of
marital status.
. INSERT TABLE 4 HERE
As already mentioned, Australia is now a country notable for its mixture
of many races and cultures. It was therefore important to ascertain the
extent to which this sample represents that diversity. When the sample was
compared with the population, as can be seen in Table 5, there was no
significant difference in the proportions of mothers and partners (usually
fathers) who were born in Australia or born overseas.
INSERT TABLE 5 HERE
Nevertheless, Table 6 indicates that there were significant differences
in the proportions of both mothers and partners born in different areas of
the world. Asians, both mothers and partners, were under-represented in the
sample, while both mothers and partners from the united Kingdom and Ireland
were over-represented. Thus, while there is a wide representation of
mothers and partners born in other countries, the proportions are different
from the population.
INSERT TABLE 6 HERE
•
•
•
•
•
•
•
•
•
•
•
•
Page 21
•
•
e·
e·
e·
-" . .;
.~
.,
TABLE 4 MOTHER'S MARITAL STATUS
Never married Married/Defacto Separated Divorced Widowed
SAMPLE
2.0 89.5 4.4 3.6
.6
CENSUS
4.5 85 .. 1
4.8 4.5 1.1
TABLE 5 AUSTRALIAN BORN OR NOT AUSTRALIAN BORN
Born in Australia
Not born in Australia
TABLE 6 PLACE OF BIRTH
Australia UK & Ireland Europe Asia Other
MOTHER Sample Census
71.1 71.5
28.9 28.5
MOTHER Sample Census
71.1 71.5 11.6 7.5
6.3 7.0 2.2 9.3 8.8 4.7
PARTNER Sample Census
65.8 66.7
34.2 33.3
PARTNER Sample Census
65.8 66.7 13.1 8.5 10.3 10.6 1.9 9.9 9.0 4.4
" . ,
Page 22
- 22 -
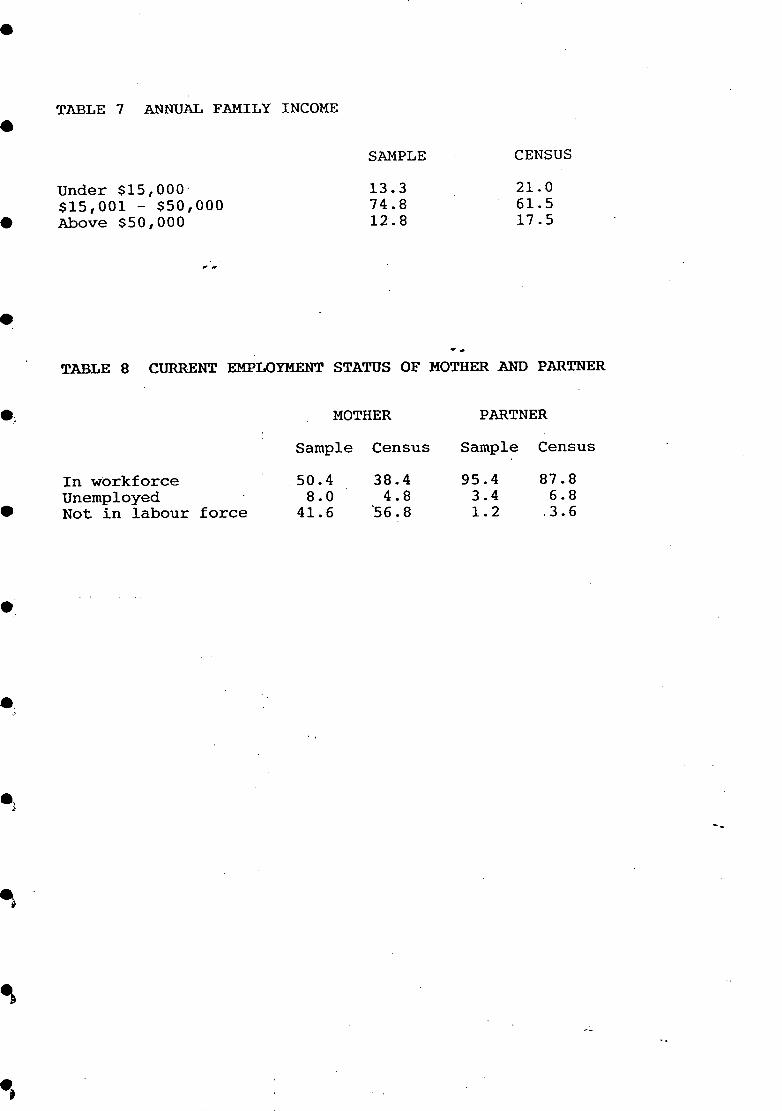
In comparing family income, significant differences were found between
the sample and the population (families with 5 year olds) as can be seen in
Table 7. The sample under-represents those in the lowest income bracket and
over-represents those in the middle-income bracket. Under-representation of
those in the lower income brackets is a problem often found in social
research. In this study, despite efforts to include low income mothers,
there were two aspects of stage 1 which may have turned them away: first,
the questionnaire required a reasonable level of literacy, and those with.
poorer literacy skills are often in the lower income groups; second, the
questionnaire had a rather official appearanca with the Commonwealth Crest
on the front, and may have been rejected as representing government
authority. The difference may also be related to the fact that there are
more two income families in the study than in the census.
INSERT TABLE 7 HERE
When the work status of mothers in the sample was compared with the
population (families with 5 year olds) there was a significant difference
between the two. Table 8 indicates that the sample over-represents the
proportion of mothers working for money, 50.4 per cent,. compared with 38.4
per cent in the population of mothers of five year olds in 1986. There are
two likely explanations for the greater proportion of mothers in the sample
who were in the paid workforce; first there has been an increase in the
number of mothers working since the 1986 Census, and secondly mothers who
were working may have seen the questionnaire from the Early Childhood study
as an opportunity to express their views. The employment status of partners
(usually fathers) in the sample did not differ significantly from that of
the population, as can be seen in Table 8.
INSERT TABLE 8 HERE
To sum up, the sample for Stage 1 of the study represents the population
in regard to the proportions born overseas and in Australia, in regards to
marital status and fathers' work status. However it under-represents
particular groups such as Asians, and those in the lowest family income
brackets. Families with mothers in the workforce are over-represented
however this is to our advantage as the study is particularly concerned with
the effects on children of non-maternal care, which is usualLy related to
mothers' work force participation.
•
•
•
•
•
•
•
•
•
•
•
•
Page 23
•
•
•
•
.~
•
e.
e. -'
.)
e.
TABLE 7 ANNUAL FAMILY INCOME
Under $15,000· $15,001 - $50,000 Above $50,000
..
""
SAMPLE
13.3 74.8 12.8
--
CENSUS
21.0 61.5 17.5
TABLE 8 CURRENT EMPLOYMENT STATUS OF MOTHER AND PARTNER
In workforce Unemployed Not in labour force
MOTHER
Sample Census
50.4 38.4 8.0 4.8
41.6 '56.8
PARTNER
Sample Census
95.4 87.8 3.4 6.8 1.2 ,3.6
--
Page 24
3. MOTHER'S WORK PATTERNS AND CHILD-CARE ARRANGEMENTS
As discussed in the introduction, a major trend in the 1980s has been the
increased participation of mothers in the paid workforce, partic~lar1y
mothers of pre-school children. Many women drop out of the workforce with
the birth of their first child and, if they return, often prefer part-time ~
work because it is easier to manage while caring for children. Most of the
increase in women's work has been in part-time and casual work. For
example, between 1974 and 1982, about four-fifths of the total increase in
jobs for women was in part-time and casual work, and over a third of all
women are in part-time employment compared with only 6.5 per cent of men
(Brennan and O'Donnell, 1986). Glezer, in the AIFS study of maternity
leave, found that although before the birth 62 per cent of women were
working full-time, 18 months after the birth, of those who returned to the
labour force, only 36 per cent were working full-time. She also found that
three-quarters of the women working full-time would prefer part-time work
(Glezer, 1988).
Mothers in this study were asked several questions about their work
history and care of the child since birth. They were asked the number of
hours per week, on average, that they were in paid work for each year since
the birth of the target child. These average hours, for purposes of the
analysis presented here, were recoded into three categories: not in paid
workforce; worked short hours - 1 to 19 hours; worked long hours - 20 hours
and more. The age of children for each year was calculated.from the child's
date of birth so that the work situation of mothers could be compared
although their children were born in different years. However, because of
the bias towards working women in the sample, caution should be exercised in
generalising from the findings presented here.
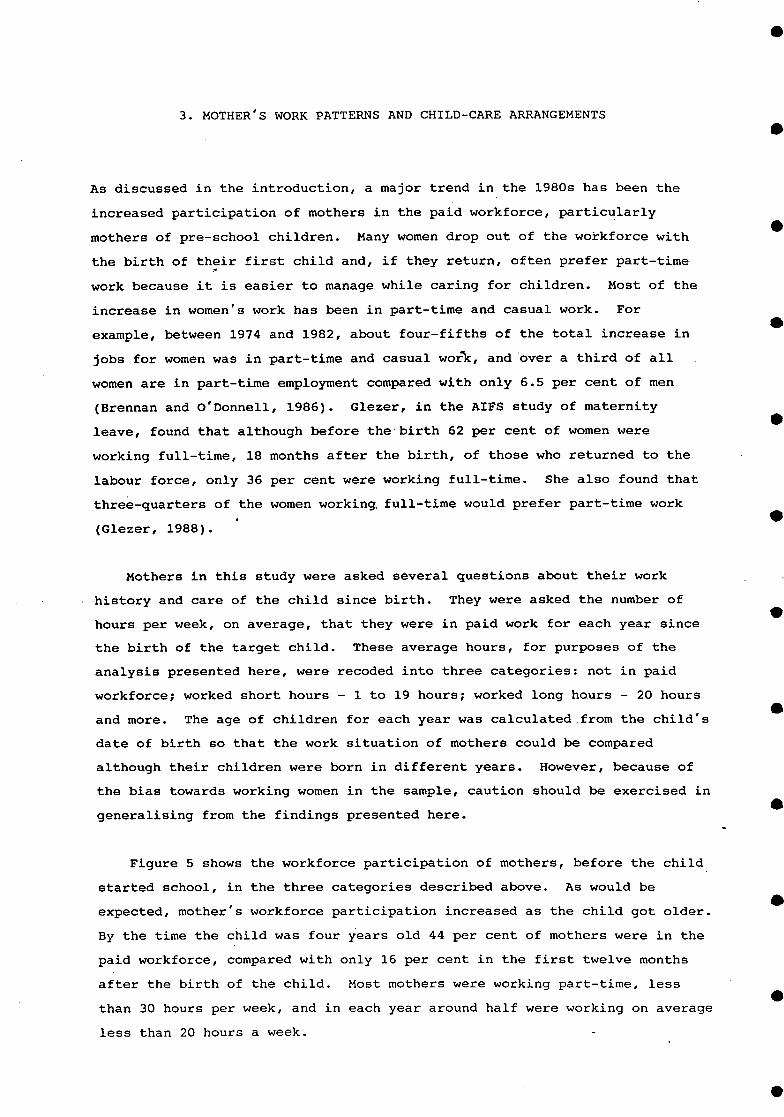
Figure 5 shows the workforce participation of mothers, before the child
started school, in the three categories described above. As would be
expected, mother's workforce participation increased as the child got older.
By the time the child was four years old 44 per cent of mothers were in the
paid workforce, compared with only 16 per cent in the first twelve months
after the birth of the child. Most mothers were working part-time, less
than 30 hours per week, and in each year around half were working on average
less than 20 hours a week.
•
•
•
•
•
•
•
•
•
•
•
•
Page 25
•
•
.~
•. :'
- 25 -
INSERT FIGURE 5 HERE
Traditionally Australian children have been cared for by their mothers
at home in the pre-school years. However, with the increased participation
of mothers in the workforce, more pre-school children are in non-maternal
care or non-parental care, at least for some of the time. Figure 5 also
provides information about the number of hours the target children spent in ,. .
non-parental care in the pre-school years. The average hours per week spent
in non-parental care for each year are divided into three categories: 0 to 9
hours, 10 to 19 hours, .and .. 20 .hours'·and above. As can be seen, the
proportion of children cared for by others 'for a medium number of hours (10
- 19), or for long hours (20 or more) increases as the child gets older.
The sharp increase in medium hours of non-parental' care at 4 years is
probably due to the effect of kindergarten attendance.
Non-parental child care takes many forms and can be either formal
supervised care in a centre or family daycare home, or it can be informal
unsupervised care provided by relatives, friends, or neighbours, or a paid
employee such as a baby-sitter, nanny or housekeeper. Informal care can be
provided either in the child's own home, or in the home of the carer. It is
often difficult for mothers to find a place for their child in the formal
system of child care at a location that is convenient, where there is a
vacancy, where they can afford the costs, where they are happy with the
quality of the care p~ovided, and where the hours are suitable. Some
mothers may prefer to use informal care by-relatives or others, some must
use informal care because it is cheaper or there is no cost in some
circumstances, while other mothers may have no choice but to use informal
care if they cannot find a place in the formal system.
To obtain an overview of child care used by mothers in the sample they
were asked to fill in a grid which indicated all forms of child-care used in
the daytime for each year of their child's life; the grid included maternal
and paternal care. Although mothers were able to indicate if more than one
form of care was used in any year (multiple response), the limitation of
this information was that a particular form of care may have been used just
once or many times and this could not be indicated on the grid. However,
another questidn indicating the form of care most frequently used in each
year overcame this limitation to some extent. Careful checking of responses
on this grid with later interview responses (for mothers who participated in
Page 26
, "
• •
. ~
Figurel\!: % Of Mothers Working In First 4 Years & A:mount Of Ti:me Child Spent
In Non-Parental Care
% Of Mothers' \ \ lOO ...... -.--...... -........... -... - -----.--.. -.. _ .... -_ ........ -.- .. -- ... ----.-.... ---.-
Hrs Mother Worked
~@ At Home
~ 1 to 19 hrs
~ 20 & Above
80
60
--------------------------*- N o/Short(O-9)
-<r- Medlum(lO-19)
-&- Long(20+)
Hrs In Non-Parental
Child Care
• • •
40
20
84
0-12 1 Year 2 Years ; ~ Years 4 Years Months
Age Of Child
• • • • • • •
Page 27
•
•
•
•
•
•
•
- LI -
stage 2) to more detailed questioning revealed some discrepancies, but the
patterns of child care use reported are consistent and, on the whole,
accurate.
Responses to the grid on forms of child care used each year were grouped
into three categories: (i) parental care by mother or partner (mostly
mother), (ii) formal care (child care centre, creche, family daycare,
workbased child care), and (iii) informal care (care by relatives,
babysitters, nannies, siblings, friends and neighbours. As can be seen in
Figure 6, the use of formal care (i.e. child care centre, creche, family
daycare home, work-based child-care) increase~with the age of the child
(kindergarten attendance was not included). Informal care was generally
used more than formal care, probably because of availability, the range of
possible carers, and also because some parents used it in addition to formal
care. For example, before their infants were 12 months of age, 25.6 per
cent of mothers used informal care compared with 5 per cent who used formal
care. By the time children were three years of age 39.1 per cent of mothers
used informal care for' their children while only 21.6 per cent used formal
care. Some of the use of informal care may well have been for short periods
of occasional care (this may also be true of formal care although it is less
likely because formal occasional care is less available), and some mothers
were using both forms of care.
INSERT FIGURE 6 HERE
Mothers were also asked the daytime arrangements they used most for the
care of their children for each year since the birth of the child. They
were instructed that if they considered it was themselves who mostly looked
after the child during the daytime that they should indicate this. This
question was not a multiple response and only one answer could be given for
each year. Answers to this question were coded into the same categories as
above: parental care (mostly mother), formal care and informal care.
Superimposed on Figure 6 are lines representing the care arrangements which .
were most used each year. Although the use of both formal and informal care
increases as the child gets older, mothers' perception is that parents
(usually mother) play the biggest part in the daytime care of pre-school
children.
Page 28
: ...
I.
•
6 Figure t(: Child Care Arrangements Used
By. Mothers During Child's First Four Years And The One Used Most
% Of Mothers Mentioning 100~~--·---------------------------------~
60
60
40
20
0-12 Months
I Y~~r
2 Years
3 Years
Age 01 Child NB. • Mul ttple Response Graph. Mothers Can Appear More Than Once For Each Age
• • • • •
4 Years
•
\ ,.
rrangements Used •
~~ Mother/Prtnr
mHI Informal
~ Formal -----------------------x- Mother/Prtnr
~ In10rmal
-t~- Formal Arrangements Used Most
• • •
Page 29
•
•
•
e·
e·
e
.~
- 29 -
Satisfactory things about daytime child care arrangements
To obtain an overview of how mothers felt about the way in which their
children had been cared for in the pre-school years, all mothers were asked
the open-ended question: 'What do you believe were the satisfactory things
about these arrangements for caring for the child during the day?' (More
precise.information on mothers' views in relation to different forms of
child care will be available in Stage 2). More than a quarter, 28 per cent,
of mothers did not reply to this question, possibly because some did not
realise that it applied to mothers who had cared for their children at home,
or because it required a written reply. Nevertheless, it is worth examining
the responses of the mothers who did reply to obtain a very general picture
of what mothers 'in different circumstances felt was satisfactory about their
child care arrangements. In order to examine the major themes in these
replies, a coding frame was developed from a random selection of
questionnaires. Ten per cent of the sample which had been randomly selected
was coded for analysis of responses to this question (to code the whole
8,446 cases would have been too expensive and 10 per cent is sufficient to
represent the trends).
Mothers could refer to several aspects of care which they felt were
satisfactory (multiple response). The most satisfactory aspect of
arrangements, mentioned by 44 per cent of mothers (cases), was related to
the development of the child. The second aspect of child care arrangements
which 33 per cent of mothers felt was satisfactory, was a good environment;
this applied to both the child's own home and to other care environments.
The third aspect of arrangements which 19 per cent of mothers felt was
satisfactory was the feeling of personal satisfaction gained by mothers from
being the major provider of care for their children. Mothers also mentioned
time away from the child, that they were able to work, and the child's
contacts with other adults.
It is likely that mothers' satisfactions with arrangements for care
during the day will vary depending on whether they have remained at home
with the child or have been involved in the paid workforce. In order to
investigate these differences, a variable was created which shows mother's
workforce attachment during the pre-school years. This variable indicates
if mother had: (i) no workforce attachment and mother had remained at home
with the child,. (ii) some workforce attachment, mother had been in work force
but part-time and/or not continuously, and (iii) mostly worked, ie mother
Page 30
- 30 -
had worked virtually continuously, although there may have been some breaks,
and/or long hours, although not necessarily full-time. [This variable was
created by using the average weekly hours mothers had been in the paid
work force each year since the child was born, ,taking into account the extent
to which work was continuous]. Figure 7 shows the percentages of. mothers in
each category.
INSERT FIGURE 7 HERE
Using the attachment to workforce variable to examine what mothers felt
were the satisfactory things about daytime arrangements for caring for the
child in the pre-school years, indicated that while the main satisfactions
remain the same, the emphasis changes somewhat as can be seen in Table 9.
For example, not un~xpectedly, the personal satisfaction of mothering was
more important to mothers who had not been in the work force (31 per cent of
responses), than to those with some workforce attachment (11.4 per cent of
responses), and those who had mostly worked and were very attached to the
workforce (4.1 per cent of responses).
INSERT TABLE 9 HERE
The following is a selection of typical quotes about personal
satisfaction with mothering from mothers who were at home and not in the
paid workforce in the pre-school years:
I know my child was brought up with a lot of care, love and
understanding, and not by some stranger.
I believe in a child spending the first five years of its life with
mother at home. We are very close and learnt and experienced many
memorable and happy times together.
All his needs could be met adequately in his own home, (he was) able to
enjoy the company of his mother. The arrangements were in the mother
and child's best interests
I love being at home and looking after my children. I've always seen
this as my responsibility and because I didn't expect anything from
anyone, when I did get a break, I loved the change, but one should not
always expect others to do their job.
•
•
•
•
•
•
•
•
•
•
•
•
Page 31
e
e
•
e.
ejl
e.
1 Figure ~: Mothers In The· Work Force
During Child's First Four Years filii'· .
5nme \I\I'O~lr _. 11 . \". 1 l ....
1'")4 .-, . , .... '"' ..
--
At Home 45.4
M ostl y \fIlrked 19.7
Per Cent Of Respondents
Page 32
9 TABLE ~: SATISFACTORY THINGS ABOUT ARRANGEMENTS FOR CARING FOR
THIS CHILD DURING THE DAY BY MOTHERS' WORKFORCE ATTACHMENT
Per cent of responses
Development of the child .. ,.
Satisfaction of mothering
Time away· from child for sport, shopping, and social activities
Able to work
Child's contact with other adults
Good environment at home or child-care/kindergarten
Cost satisfactory: low, a relative and no cost, or subsidised
AT HOME
36.9
31.0
12.3
0.5
4.3
13.0
2.0
This is a multiple response question.
SOME WORK
29.0
11.4
5.0
12.0
33.1
2.0
MOSTLY WORKED
31.2
4.1
2 •. 9
17.3
12.3
29.3
2.9
•
•
•
•
•
•
•
•
•
•
•
•
Page 33
•
•
•
•
•
•
•
•
- 33 -
I was there to enjoy my child and guide her growing up.
Daytime care arrangements which enhanced or stimulated the development
of children were mentioned as one of the satisfactory things by a~l three
groups of mothers (37 per cent of responses for mothers at home, 29 per cent
for mothers wit~ some attachment to the workforce, and 31 per cent for
mothers who were very attached to the workforce). The following are quotes
about the development of children typical of mothers in each of the three
groups:
Child learns to become independent in a caring environment
(kindergarten), mixes with peers, learns tolerance etc. (mother at
home).
The child-care centre provided wonderful opportunities for my son's
physical, mental, and social d~velopment (mother had some attachment to
workforce).
In family daycare there was intimacy and closeness of contact between
caregivers and child because of small group situation. At the child
care centre there was social contact/interaction with other children and
a variety of activities for child development (mother had some
attachment to work force).
(Child was) exposed to different attitudes, etc. Greater freedom to
express herself in wider environment, greater exposure to other kids
(mother very attached to workforce).
A good care environment was mentioned more often by mothers in the paid
work force (some workforce attachment 33 per cent, and by mothers who mostly
worked 29 per cent), than by mothers who had remained at home with their
children (13 per cent), perhaps because mothers who remained at home took it
'for granted that the home provided a good environment. The following are
quotes in this category from mothers who worked in the pre-school years.
I can only leave my daughter with my mother because she looks after her
properly. Anywhere else they don't feed them properly and don't give
them enough attention because they have a lot of other children to look
after (mother had some work force attachment).
Page 34
- 34 -
My daughter has attended two child-care centres, one for 18 months, the
other for two months. The first centre was council run, subsidised by
the government to reduce fees for low income parents. (It) provided a
warm lunch, morning and afternoon tea, and when the child was ill, a
family daycare mother, at no extra cost to me, as I was a low, income
single parent at the time. The second centre had some stimulating
activities ~nd they were willing to change the sessions I had booked to
fit my changing work needs (mother had some attachment to workforce).
(Child-care was) provided at the worksite, therefore I was able to
breastfeed (both children fully breastfed ~ntil 6 months). Continuity
of care which was loving and affectionate was possible (mother had some
workforce attachment).
An amalgamation of 3 mothers working part-time, taking it in turns to
mind children was satisfactory. The kids thought of it as 'playing with
their friends' rather than being taken to child-care. I also used a
short weekly session (of child-care), which was based at a kindergarten
complex (mother had some attachment to workforce).
-Unsatisfactory things about daytime child-care arrangements
To obtain some preliminary insights into any unsatisfactory aspects of
caring for the child, all mothers were asked the open-ended question' What
do you believe were the unsatisfactory things about these arrangements for
caring for this child during the day?' Mothers could refer to several
aspects of care which they felt were unsatisfactory. A coding frame was
developed, which included all the major themes, from a random selection of
questionnaires. The same 10 per cent sample, which was used for the
previous question, was coded for analysis. However, almost two-thirds of
mothers did not reply to this question, perhaps because they felt nothing
was particularly unsatisfactory with their care arrangements, or perhaps
because they did not think the question applied to them. It is worth
examining responses from mothers who answered the question~ to explore the
range of reasons for dissatisfaction, although, this information should be
seen as exploratory only and not for generalisation. The mother's interview
at Stage 2 of the study will provide more precise information about
satisfaction or lack of it with particular care situations and in particular
circumstances.
•
•
•
•
•
•
•
•
•
•
•
•
Page 35
•
•
•
•
•
•
•
•
•
The most unsatisfactory aspect of care, as reported by 31 per cent of
those mothers (cases) who replied to the question, was difficulty with
finding appropriate care and/or preferred type of care, at suitable times
and reasonable costs. Seventeen per cent of mothers reported personal
dissatisfaction with being tied down by the child, another 14 per cent of
mothers reported daily problems, such as early rising and the long day,
coping with illness and other difficulties of everyday life with young
children. Fourteen per cent of mothers also reported feeling guilty leaving
the child in the care of others and not having enough time with the child.
Mothers' responses to this question are likely to vary depending on
whether they are in the paid workforce or not. In order to investigate any
differences, the variable indicating work force attachment, which was
described earlier, was used to differentiate responses. As expected, Table
10 shows some differences in the responses depending on whether mothers had
been in the paid workforce or remained at home with the child in the pre
school years. Guilt about leaving the child in the care of others was
expressed more often by mothers with some attachment to the workforce (15
per cent of responses) or who were very attached to the workforce (20 per
cent of responses), rather than by mothers who were not in the workforce (6
per cent of responses).
INSERT TABLE 10 HERE
The following are.typical responses from mothers in the workforce:
I only spent half the day with my daughter and I feel that wasn't
enough, but I had to work. (mother had some attachment to the workforce)
Worry, guilty feeling. Hated parting with them and disturbing their
routine. (mother had some attachment to workforce)
.Not being with the child to see the little things they do and say whilst
growing up prior to school age. (mother very attached to the
workforce).
Difficulties with certain aspects of care were mentioned by mothers
whether they were in the paid work force or remained at home with their
children (26 per cent of responses for mothers at home, 30 per cent of
responses for mother with some workforce attachment, 24 per cent of
Page 36
\0 . TABLE ~: UNSATISFACTORY THINGS ABOUT ARRANGMENTS FOR CARING FOR
THIS CHILD DURING THE DAY BY MOTHERS' WORKFORCE ATTACHMENT
Per cent of responses
Parent's guilt, not enough time with child ..
,,"
Daily problems:long day, driving, hurrying etc
Poor quality of care
Child affected by different social environment and carers
Difficulties with aspects of care: times, finding, cost,
AT HOME
5.8
3.6
1.7
4.3
inappropriateness 26.2
Personal dissatisfaction, tied down by child 35.2
Effect of other children: infection, different standards
Other
4.9
18.3
This is a multiple response question
--
SOME WORK
15.0
18.5
8.9
5.7
30.4
4.9
5.9
10.7
MOSTLY WORKED
20.1
12.8
12.7
11.1
23.3
0.0
7.4
12.4
•
•
•
•
•
•
•
•
•
•
•
•
Page 37
•
•
•
•
•
•
•
•
• J
- 37 -
responses for mothers who were very attached to the workforce and mostly
worked). However, the concerns of mothers in the workforce were somewhat
different from those of mothers who stayed at home, as can be seen in the
following quotes:
Family day care as such was not available to the average suburban mother
on a part-t~me basis - ie one day or one and a half days a week. (It
is) fully booked out by full-time single working mothers and is not
available to give full-time mothers a break!
child)
(mother at home with
. The only times I wanted a break was to go shopping alone (clothes etc).
I wish you could leave your child at an independent care centre and go
on your own. Sometimes, leaving your children with relatives leaves you
obligated. (mother at home with child).
It was difficult to find facilities where my child could be put in care
while I attended to necessary business tasks. The local government
funded day-care centre would not consider putting my child in care
unless I was in paid employment, but gave priority to working parents,
regardless of marital status or combined income. I found this policy
most unsatisfactory, especially where circumstances of special needs
were not even considered. (mother at home with child)
Child care at home is very expensive, but I needed it for my other two
children after school as well (as this child).
workforce attachment)
Work did not have any child care facilities.
attachment)
(mother had some
(mother had some workforce
Expense factor - good child care centres are very expensive, and if
subsidised, they are constantly under threat of funding cutbacks which
in turn affects morale of staff. (mother had some workforce attachment)
It is unsatisfactory that child care costs so very much. After spending
$90 to $100 per week on child care you certainly are not left with very
much. Why are we b~ing penalised just because we want and need to go to
work!! Is this equal opportunity?
workforce)
(mother very attached to the
Page 38
- 38 -
The burden on my parents (of child care). The cost of formal child
care. Long hours of separation during the day.
to workforce)
(mother very attached
Personal dissatisfaction with being tied down by the child wa~ expressed
more by mothers who were at home with their child and not in the work force
(35 per cent of~responses) than by those who were in the p~id work force (5
per cent of responses for mothers with some work force attachment and not
mentioned at all by mothers who were very attached to the workforce). The
following are typical responses from mothers who were not in. the paid
work force and who expressed personal dissatisfaction:
The only unsatisfactory thing is selfish - very little space for mum to
do her own thing. But I would never change the situation if I did it
all over again.
Mothers are tied down and rarely can achieve any personal satisfaction
apart from child raising. Too long at home can make one less aware of
one's worth.
That I had no freedom, that is, complete freedom from him when things
got too much. It was always a battle on shopping days.
I needed 'time out' to be a person, other than a survival kit to a
child.
More mothers who were attached to the work force expressed
dissatisfaction with daily problems in caring for children (19 per cent of
responses of those with some workforce attachment and 13 per cent of
responses of those who were very attached to the workforce) than mothers who
were at home (4 per cent of responses). The following are typical responses
from mothers in the paid workforce.
Long absences from the family. (mother had some attachment to workforce)
(Child care was) not always reliable, i.e. last minute arrangements
sometimes necessary. Occasionally I was reluctant to ask for help
because I felt it was an imposition. (mother had some attachment to
workforce)
•
•
•
•
•
•
•
•
•
•
•
•
Page 39
•
•
•
•
•
•
•
•
- 39 -
Picking her up after working late. (mother had some attachment to
workforce)
The constant rush from home to grandmother's, interrupted sleeps.
(mother had some attachment to workforce)
When the ch;ld was ill it caused a dilemma. (mother very attached to
workforce)
Difficulties when child was sick. Some days the child was tired by the -end of the day. (mother very attached to the workforce)
Mothers who had been in the paid workforce in their child's pre-school
years were also more likely to report problems with poor quality of care (13
per cent of mothers who were very attached to the workforce, 9 per cent of
mothers with some attachment to the workforce compared with 2 per cent of
mothers who were not in the paid workforce.) The following responses are
typical of mothers with work force attachment in the pre-school years.
Child-care centre - too many children under the care of few care-takers.
and we the parents had little say in who was employed to look after the
children. (mother with some workforce attachment)
Her creche did not seem to have many structured activities. She came
home quite bored and not wanting to return. (mother with some workforce
attachment)
I now feel he would have been better off with more young children his
own age. The lady who looked after him was very busy and I feel he
missed out on attention. (mother with some work force attachment)
Being cared for by friends and baby-sitters limited my son's activities
and learning ability. (mother very attached to the workforce)
Missing out on child's development, lack of care given by minders, very
hard to cope under these conditions. (mother very attached to workforce)
Page 40
- 40 -
Who paid for child-care?
Child care is often very expensive although it may cost nothing or very
little if the child is cared for informally by a relative or if the mother
is eligible for a government subsidy and the child is in formal care of some
kind. All mothers were asked 'Who mainly covered the costs involved in
child care?' H9wever, as mothers with no workforce attachment in the pre
school years had used child care very little, usually only for occasional
care, they were omitted from analysis.
Figure 8 shows the distribution of costs for-mothers in the labour force
divided into two groups: those with some workforce attachment and those who
mostly worked and were very attached to the workforce. A high proportion
of mothers with some work force attachment as well as those who had mostly
worked had costs associated with child care.
INSERT FIGURE 8 HERE
Mothers with some work force attachment were more likely to have no costs
associated with child care than those who mostly worked and were very
attached to the workforce. This is probably because the hours they required
child care were shorter, and for some mothers child care was required for
intermittent periods only. In addition, child care for short time spans can
sometimes be provided by the parents themselves (by shift work and fitting
their work times around child care), or by relatives. Mothers who were very
attached to the workforce,- on the other hand, required care that was
continuous over the years and usually for longer hours. It was therefore
probably more difficult for them to manage care without cost involved. As
can be seen, fathers rarely covered the costs of child care alone, although
mothers frequently did, but the most common arrangement was that both
parents covered the costs.
Now the child is at school
The previous section was concerned with mothers' work and child care
arrangements in the pre-school years. At the time of data collection the
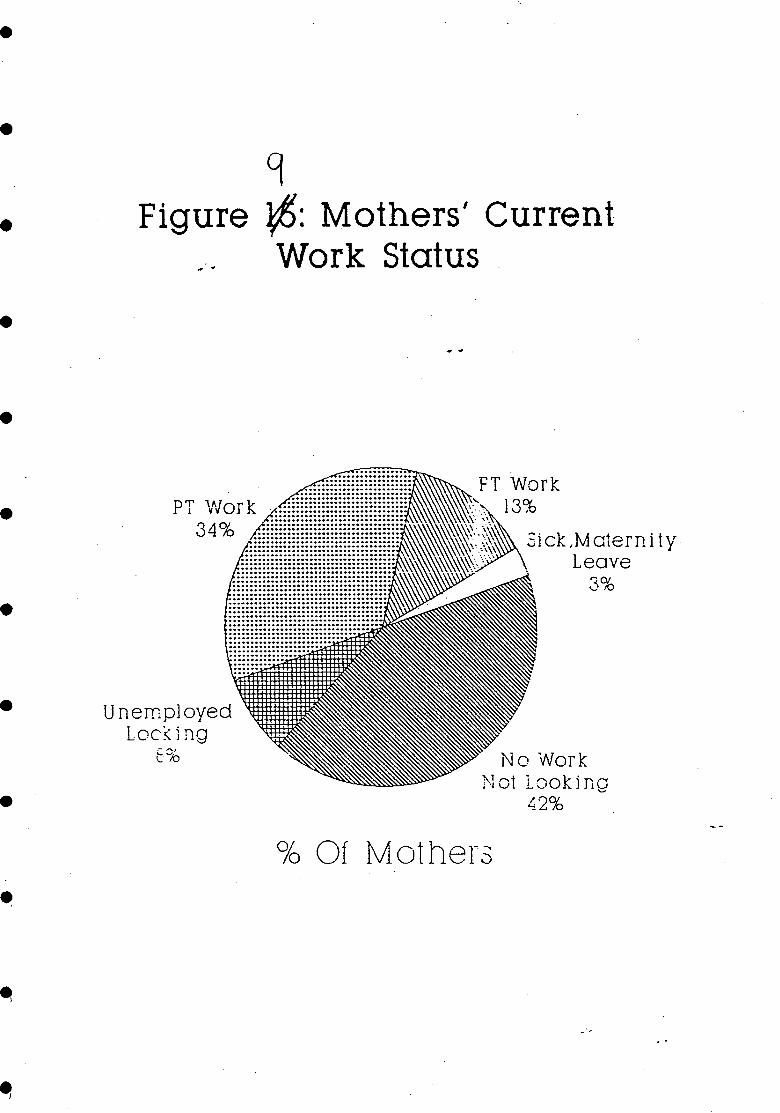
target children were in their first year of school. By this time (see
Figure 9) more than half the mothers in the sample were in the paid
workforce, although 3 per cent of mothers were temporarily out of the
workforce (1 per cent on workcare or sickness benefits and 2 per cent on
•
•
•
•
•
•
•
•
•
•
•
•
Page 41
. ~. .'. •
• g Figure ~: Persons Covering Child.care
• 'Costs For Mothers In The Worklorce At Any T"irne In Child's Pre-school Years
• . % Of Mothers .. 60~------------------~------------~
• 50 49.7
• 40
30 28.3·
• 22.2
20
• 10
• o Some Work Mostly Worked
Degree 01 Attachment To Workforce
~ No Costs mj~m Partner ~ Self ~ Both
Page 42
- 42 -
maternity leave). Less than half the mothers were not in the paid workforce
and were not looking for work. Seventy-nine per cent of those mothers who
were in the paid workforce were working for someone outside the home; 9 per
cent worked in a family business and 9 per cent were self employed. Only 4
per cent of mothers worked from their home for someone else.
INSERT FIGURE 9 .~HERE
All mothers were asked what their work preference would be if they had
their choice (this question applied both to mothers in the workforce and
those at home not looking for work). The majority of mothers, as can be
seen in Figure 10, indicated that they would like to work part-time. Only
11 per cent indicated that they would like to work full-time, and the
remaining 12 per cent of mothers would prefer not to be in the labour force.
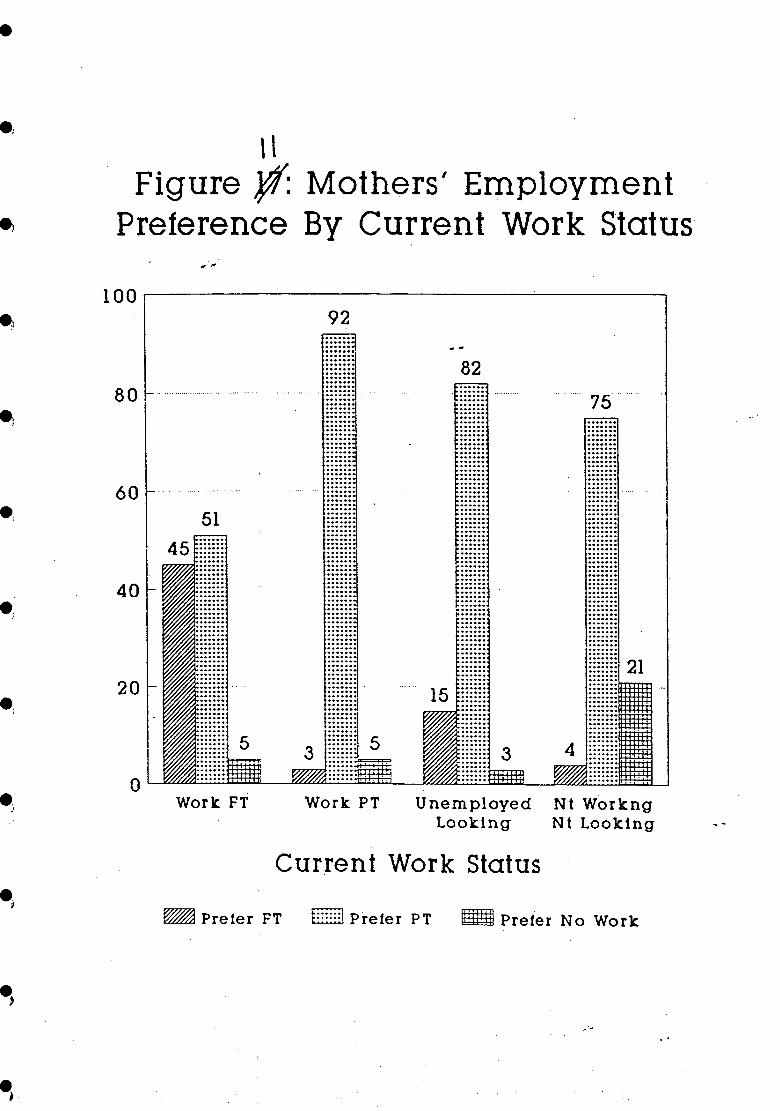
Figure 11 shows the work preferences of mothers in relation to their current
employment status. Part-time work was favoured by most mothers regardless
of their current work situation. Hore than half the mothers who were
working full-time would have preferred part-time work. Most mothers who
were actually working part-time preferred this situation. Most mothers who
were unemployed but looking for work would prefer part-time work. The
preferences of mothers not in the paid workforce are also of interest: only
about a fifth, would prefer to remain outside the workforce; most would like
part-time work, and only 5 per cent would like full-time work. Quite
clearly, part-time work is preferred by mothers with children who have just
commenced school. Glezer (1988) in the AIFS study of maternity leave found
a similar strong preference for part-time work by mothers of~young children.
INSERT FIGURES 10 AND 11 HERE
After school care is sometimes a problem for mothers in the paid
workforce. All mothers were asked who cares for the child after school.
Figure 12 shows the way in which the child who was the focus of the study
was cared for after school and whether the mother was in employment or not.
The majority of children were cared for by their mothers. As can be seen
partners (fathers) took a very small part in after school care, probably
because they were unavailable due to work force participation. A very small
. percentage of families used an after school care centre, the rest relied on
relatives, older children, neighbours, and paid babysitters to care for the
child after school.
•
•
•
•
•
•
•
•
•
•
•
•
Page 43
•
•
•
•
•
•
•
•
•
9 Figure ~: Mothers' Current
Work Status
PT V/ark 34%
........................... .......................... ..................................... -"."' "" '''' ............................. ................................ ................................ ................................ ................................ .............................
Unemployed Loc!( i ng
............................ ............................. ............................. ............................. ............................... ............................... .................................. .................................. .................................. ..................................
Of Mother:)
13%
Sick ,Matern i ty Leave
Lookino '-
42%
Page 44
10 Figure ~: Mothers' Employment
Preferences
............................. ............................. ................................ ................................ ................................ ................................
Full Time Work 1]%
!'''Io Paid 'Nark 11%
••
•
•
•
•
•
.............................. :: :::::::::: ::::: :::: :::::::: ::::: . ~~~~~~~~~~~~~~~~~~~;;1~~~;~~;;;;;;::::::::::~~~~;~~;;~~~~~;;~;~~;~E~~;i -:::::::: ::: ::::: ::: :::::::::::: ::: ::::::::: ::::::::::::::: :::::::: ::: ~ . ...................................................................... ~ ::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::, ...................................................................... , .... ::::::::::::::::::::::::::::: ::::::::::::::::::::::::: ::::::::::: ::~
:::::::: ::::::::::::: :::::: :::: ::::::: ::::::::::::::::::::::::: ::::!
'll\\lllllllllllillllllllillllilllllilllilillilil!llli11111' • Part Ti me Wort
78%
..................................................
0;0 Of tv10thers
•
•
•
•
Page 45
•
•• ,
.;
.)
• J
\ \ Figure ~ Mothers' Employment
Preference By Current Work Status .. ..
100~------------------------~--------,
92
--80···
60
40
20
Work FT Work PT Unemployed Nt Workng Looking Nt Looking
Current Work Status
~ Prefer FT [g~~1 Prefer PT IlmWl Prefer No Work
Page 46
- 46 -
INSERT FIGURE 12 HERE
As can be seen in Table 11 further analysis indicated, not unexpectedly,
that it was the group of mothers who were working full-time who mostly used
people other than themselves and their partners to care for their children.
Even so, 42 per cent of the children whose mothers worked full-time were
cared for after school by their parents. Relatives cared for 19 per cent,
while the rest of these children were cared for by other people. Most part
time workers, 88 per cent, cared for their children themselves after school.
Part-time work is less likely to make after school care a problem for
mothers.
INSERT TABLE 11 HERE
Conclusions
The analysis reported here indi~ates that many pre-school children whose
mothers are in the work force experience non-parental care, but more c~ildren
at each age level examined are in informal care than are in formal care.
Nevertheless, mothers still ~erceive themselves or their partner as taking
the major role in the daytime care of their children. As children get older
mothers' work force participation increases and children's experience of non
parental care also increases. Most families have costs associated with
child care, but families where mothers were less attached to the workforce
had no child care costs more often than those where mother mostly worked.
The majority of mothers, including those working full-time in the child's
first year of school and those not working at all, would prefer to work
part-time.
•
•
•
•
•
•
•
•
•
•
•
•
Page 47
•
•
••
•
•
•
• ,
\J-Figure ~: Person Who Usually Cares
For Child Alter School - Mothers Employed And· Not Employed
Sel1 .9
Partner
Both
Older Child
Othr Relative
Neighbour
Paid Si tter
Care Cntr
Varies
Other
o 10 20 30 40 50 60 70 80 90 100
_ Employed ~ Not Employed
Page 48
•
\ \ TABLE J{&: CARE OF THE CHILD AFTER SCHOOL • CARER FIT WORK PIT WORK AT HOME ALL
% % % %
Self (mother) 27.0 79.2 94.9 80.8 • Partner (usually father) 8.3 .9 .4 1.6 -Both parents, different days 6.2 7.3 2.2 4.5 • Older sibling 5.1 .5 .1 .9 -Other relatives 14.0 1.8 .2 2.5
Neighbours 2.1 .5 .0 .5 • Paid babysitter 13.2 1.9 .1 2.4
After school centre 12.5 1.4 .4 2.3
Arrangements vary 7.3 5.6 1.2 3.5 • Child left alone .1 .0
Someone else 4.2 .8 .5 1.1
TOTAL 12.9 34.4 52.8 100.0 •
•
•
•
•
•
Page 49
•
•
••
•
•
•
.'
•. :
4. • AN EAR TO LISTEN AND A SHOULDER TO CRY ON':
THE USE OF CHILD HEALTH SERVICES IN MELBOURNE, ADELAIDE AND PERTH
Child health services are the only service which is free and universally
available to mothers and infants. Stage one of the Institute's Early
Childhood study provided the opportunity to examine current use of child ,. health services in Melbourne, Adelaide and Perth, and also to make some
assessment of the extent to which these services are meeting the needs of
modern-day mothers of infants and young children. Mothers were asked three
questions about their use of child health serVices for the particular child:
how often they used the service, how helpful it was, and what they thought
about the child health service in their state. Before examining the use and
helpfulness of child health services in recent times, these services in
Victoria, South Australia and Western Australia are described and their
development placed in historical context.
Child health services today
Child health services aim at improving the health and wellbeing of infants
and. young children so that optimal physical, emotional and social
development is possible. They began early this century when infant
mortality was high due to gastric infections, poor hygiene and poor living
conditions (Gandevia, 1978).
Unlike Britain, which has a health visitor scheme and home visiting is
usual (Mayall and Foster, 1989), child health services in Australia provide
support for mothers and children essentially through locally based centres,
although the first visit may be in the home and arrangements can be made for
home visits, on request, in special circumstances. Nurses in child health
services are fully qualified and. have training and/or relevant experience in
maternal and child health. (Victorian and Western Australian child health
nurses are triple certificated, South Australian nurses are required to have
basic nursing training, but it is regarded as highly desirable that they
also have further specialist qualifications and/or experience).
In Victoria hospitals notify nurses in the local government area of
births. Child health nurses make the first contact with mothers either by
hospital or home visit. South Australia has a video about the service which
is shown to mothers while still in hospital. The service provides advice on
Page 50
e
•
•
e
e·
•
•
• I
- 50 -
feeding and on the general day-to-day care of the baby; health checks of
such things as vision, hearing, language and general development are also
routinely provided. Information about immunisation and health needs is
given, and mothers are put in touch with other relevant services. Some
centres run parenting education sessions, particularly for parents of first
babies; there are also play groups for young children and toddlers in some
centres. Services differ somewhat from one area to the other, often due to
differences between the nurses in charge and their ideas about the scope of
their role. South Australia differs from the other States because it
combines child, adolescent and family health services; however, services for
babies and pre-school children, which are provided through Child Health
Centres, are essentially the same as in the other states (Information
brochures from child health services in Victoria, Western Australia, and
South Australia.)
Child health services in each state provide mothers with a booklet in
which to keep a record of their child's development, immunisation, and
health. South Australia provides the most comprehensive of these with the
Personal Health Records book which is issued in the hospital on the birth of
a child and includes details of the birth. This booklet is designed as a
complete health record of the individual child and is held first by parents
and then passed on to the children when they reach an age of responsibility.
The booklet, which contains the telephone numbers of emergency services and
of local Child Health and Adolescent Centres, is divided into sections to
record all aspects of the child's health and development; it includes also a
section on family events as well as simple advice on caring for a new baby.
Each state has brochures explaining to new parents the functions of
child health services and encouraging their use; these are distributed by
the hospitals and other centres and are also available in the major
community languages. The following quote from the Victorian Maternal and
Child Health Service brochure shows how an attempt is made to go beyond the
bounds of basic child health, nutrition and developmental issues, and into
the realms of parenting and family support.
Becoming a parent means learning lots of new things and you can't be
expected to know it all at once. Feel free to ask your nurse all those
questions that probably didn't even occur to you before the baby arrived
or just talk about your concerns. Each baby has its own personality and
it takes time for you to know your baby and your baby to know you.
Page 51
- 51 -
A brief history of child health services
This section contains a brief description of the beginnings of child health
services in Australia. An understanding of the development of child health
services helps put current services into context.
Awareness of. community responsibility for the maintenance of health ~
occurred increasingly, in developed countries, in the period between 1890
and 1920. It was a time of advances in scientific knowledge and the
implementation of measures to promote public health; there was recognition
that disease and accidents could be prevented or controlled through human
efforts and that illness and death of children did not have to be passively
accepted as "God's will" (Gandevia, 1978; Zelizer, 1985). In the early part
of this century legislation was enacted concerning sanitation, water
supplies and the notification of infectious diseases. Medical and
scientific advances led to safer milk supplies with effective supervision of
dairy herds to eliminate tubercular,cattle. Ironically it was around the
time that safe milk supplies became available that it was recognised that
breast fed infants suffered less from gastric infections (Gandevia, 1978);
it was also around this time that interest -in promoting the health of 'well'
babies developed.
Overseas knowledge and developments had a direct bearing on the
development of infant health services in Australia. The first International
Child Health Conference was held in 1905 in Paris, the city in which Infant
Welfare work had begun in 1880. The first English speaking Child Welfare
conference was held in I.ondon in 1913 (CAFHS, c.1989). Various approaches
were taken in Australia to improve child health and organisations were
formed to ensure that mothers were educated in the care of infants and
children. As a result of both education and public health measures infant
mortality declined in the early part of this century. Nevertheless,
services to mothers and babies were seen initially as a threat by some
medical practitioners.
The development of infant welfare organisations, usually initiated by
voluntary action but ultimately government sponsored or controlled, in
the first two decades of the present century was an inevitable step.
The advisory clinics established by these groups did meet with some
opposition on the grounds that they constituted an intrusion into
private medical practice, which indeed they were. However, as with
•
•
•
•
•
•
•
•
•
•
•
•
Page 52
•
•
•
•
•
•
•
•
•
- 52 -
other state medical services, such as compulsory immunisation, they
filled a need not adequately covered by conventional medical practice,
and they were led, or supported, by prominent physicians, such as Wood,
Turner and Vera Scantlebury Brown, concerned with paediatrics, whose
integrity and dedication were unquestioned. The risk that trained
nurses might replace the doctor in a significant segment of child care
did not eventuate, although in more recent years some problems arose ~
with the suggestion that infant welfare teaching in the centres had
become too rigid, ritualistic and authoritarian. For the most part, the
principle that the clinic nursing staff should refer sick children to
medical practitioners was followed~ •• (Ganaevia, 1978, 125).
The first person to organise support for infant welfare in Australia was
W.G. Armstrong, medical officer of health for Sydney, who had studied
problems of infant mortality and child welfare in England and France. He
saw the need to educate mothers in the care of infants and young children as
imperative and recognised the benefits of breast feeding rather than
improving the supply of sterilised milk. In 1904 Armstrong employed a
health visitor to go to the homes of all mothers of newborn babies. Child
mortality in Sydney, which was already in decline due to public health
measures, continued to decline over the next decade, from 116 per 1,000
births to 68 per 1,000 births, while the proportion of mothers breast
feeding increased from 72 per cent to 94 per cent by 1914 (MacOonald, 1975;
Gandevia, 1978). other states followed similar processes in developing
their infant health services. A brief description of the development of
these services in the three states which took part in the Institute's Early
Childhood Study follows in chronological order.
South Australia (Child, Adolescent and Family Health Service): Thomas
Borthwick, in Adelaide, introduced a system similar to that-operating in
Sydney in 1907, although it was short lived; it was Or Helen Mayo, who had
studied paediatrics in London, who had a more substantial impact. She
founded the School for Mothers in 1909, which in 1927 became the Mothers and
Babies Health Association. The first baby health train began operating in
country areas in 1931 and in 1934 a highly successful baby health centre was
conducted at the Royal Adelaide Show. A correspondence section was
introduced to the service in 1935 to help mothers in areas where there were
no clinics; work in country areas was extended in 1936. South Australia had
the lowest infant mortality rate in the world by 1937.
Page 53
- 53 -
In 1979-80 a report on the South Australian Child Health .Services, which
pointed out the importance of integrated services, led to the amalgamation
of the Mothers and Babies Health Association, the School Health Service and
the Child Adolescent and Family Psychiatric Service into the present Child
Adolescent and Family Health Service (C.A.F.H.S.).
Victoria (Maternal and Child Health Service): No organised service for the ~
welfare of children existed in Victoria before 1917; medical attention was
for sick infants and children only. Voluntary welfare a~sociations
developed between 1917 and 1926. The first service for the welfare of
normal babies was set up by Or Isabel Younger ~oss in a small: shop in
Richmond in 1917; Or Ross was influenced by work on the welfare of well
infants which she had seen in England. Advice at this centre was free and
the service was popular; other centres were set up and public interest grew.
In 1918 the Victorian Baby Health Centres Association was formed. A
deputation by this association to the Minister for Health resulted in a
government subsidy of 125 pounds pe~ annum for the employment of full-time
nurses, on the condition that local councils made an equal contribution to
the costs. Nevertheless, a great deal of money still had to be raised by
centre auxiliaries to fund operations. The Association also set up a school
in South Melbourne to train double certificated nurses to take charge of
centres (Campbell, 1976).
In 1926, as the result of a government Royal Commission into the welfare
of women and children in Victoria, the Infant Welfare Section of the
Department of Health was created with Or Vera Scantlebury Brown as the first
Director of Infant Welfare. Notification of births to local municipal
offices within 24 hours was made mandatory and these notifications were
passed on to Infant Welfare sisters. As had been recommended in the report
of the Royal Commission, Infant Welfare Centres were subsidised by state
government while municipal councils provided premises and part payment of
nurses. Efforts were made to reach every infant in the state; in 1935,
using a grant from the Victorian Centenary Council, a caravan which provided
roadside services to country mothers and babies was set up. A
correspondence service for mothers was also created; this service sent out
leaflets on child management and mothers could also write for advice on
their particular needs (Campbell, 1976; Poulter, 1976).
In 1976, a Jubilee Conference on Maternal and Child Health was held to
mark the 50th anniversary of the establishment of the Infant Welfare Section
•
•
•
•
•
•
•
•
•
•
•
Page 54
•
•
•
•
•
•
• e ..
- ~4 -
of the Department of Health, Victoria. The Infant Welfare section moved
from the Department of Health to Community Services Victoria in 1985. Soon
after, when staff changed their titles from Infant Welfare nurses to
Maternal and Child Health nurses, the service followed suit and became the
Maternal and Child Health Service. Maternal and Child Health Service is
jointly funded by state and local government.
Western Australia (Child Health Services): The Infant Health movement in
Western Australia commenced in 1923 when three clinics staffed by Infant
Health nurses opened in Perth. At thetime·infant mortality in western
Australia was higher·than in the other-states;· this was largely due to the
influx of people and poor living conditions in gold rush towns where fresh
water was in short supply (MacDonald, 1975; C.A.F.H.S, c.1989). Although
much of the drop in i:nfant mortality in the goldfields could be attributed
to the building of a water pipeline from Perth to Kalgoorlie, the work of
the infant health clinics contributed to the all round fall in infant deaths
from gastro-enteritis and to improvement in infant health (MacDonald,
1975) •
By 1926 there were 10 clinics in Western Australia; in 1932 Municipal
Councils were given the power to subsidise Infant Health Centres. In the
same year a correspondence section was established which communicated with
mothers in the outback through pedal wireless or letter. Later nurses from
this section also travelled twice a year to visit these outback mothers. In
1954 families on the Nullabor Plain were provided with health services via
the "Tea and Sugar" train (a. train which carried stores to people in that
area) (Child Health Services, c.1972). Infant health services in western
Australia were reorganised into the Infant Pre-school Health Service in 1952
in recognition of the fact that there was continued risk to children's
health.in the second and third years of life. This service was changed in
1972 to the current Child Health Services.
I
Present use of child health services in Melbourne, Adelaide and Perth
Conditions in Australia are now very different from when.child health
services commenced. Infant mortality has improved considerably; in 1988
infant mortality was 8.7 per thousand live births (ABS, 1988). Infectious
diseases and nutritional deficiencies are no longer major problems and most
.. women these days are better educated than when child health services began.
Page 55
- 55 -
However, as indicated in the introduction, there are many other changes
which may affect the care of young children and which have changed the
social context in which they are reared.
Modern mothers often experience great anxiety about their capacity to
parent. Whereas parents earlier this century were likely to have real
concerns about the physical health of the child, modern parents are often -\ more concerned about the emotional health of the child. This is part of a
trend of parental anxiety, but particularly maternal anxiety, throughout the
western world. This anxiety about parenting capacity has developed over the
twentieth century with greater knowledge of cHild development and the
importance of environment, higher expectations of parents and of children,
and as a result of conflicting theories of child rearing in self help books
and the media. All of this is related to the fact that humans learn how to
be parents from others, and that unlike animals, they do not instinctively
know the correct things to do with their babies (Ochiltree, 1990).
Child health services are used by most mothers; the majority of mothers
in the sample, 87.3 per cent, had used the infant health service in their
state for the selected child. Figure 13 shows the frequency of use of
services for each city and the total sample: a greater percentage of
Melbourne mothers, 90.2 per cent, had been users than had Adelaide mothers,
81.2 per cent, and Perth mothers 8S.1 per cent. A recent South Australian
study of the first year of parenting reported 94 per cent of mothers in the
sample used child health services, however there were only 49 mothers in
their sample (Southern Community Health Services, 1990).
INSERT FIGURE 13 HERE
In order to obtain more precise information about which mothers did not
use child health services or used them very little, the following
characteristics of families were examined in relation to the question on
frequency of use: position of child in the birth order, whether a language
other than English was spoken in the home, family income, and workforce
participation of mothers in the first twelve months of the child's life.
Just over a tenth of mothers in the total sample, 12.6 per cent had not
used child health services for the child involved in the study (ie the child
who had started primary school that year); they may have used-it for other
children, if they had any but this information was not collected. There
•
•
•
•
•
•
•
•
•
•
•
•
Page 56
•
•
•
•
•
•
•
•
•
..
13 Figure $: Use Of Child Health
Services By Ci ty & Total Sample
% 01 Mothers 60~·----------------------------------~
50 .............. .
Never Used
1 to 5 Times
················48
6 to 20 Times
More Than 20 Times
Use 01 Child -Health Services
~ Melbourne' I:~gm Adelaide ~ Perth ~ Total
Page 57
- ~I -
were some differences between the states as can be seen in Figure 13; more
Adelaide (18.8 per cent) and Perth (14.9 per cent) mothers had not used the
service than Melbourne mothers (9.8 per cent), and Melbourne mothers appear
to be the most frequent users.
The child's position in the family was coded to reflect whether the
child was the first born (a category which also included only children), ~
last born, or a middle child. Figure 14 shows the use of child health
services by the position of the target child in the family birth order. As
might be expected, mothers of first born children were more frequent users
than mothers of later born children; 43.7 per cent of mothers of first born
children used child health services more than twenty times, compared with
32.5 per cent of mothers of middle children, and 26.4 per cent of mothers of
last born children. Mothers of last born children were more often non-users
of child health services or used the services only a few times compared with
mothers of first born children. It is not surprising that mothers of last
born children make somewhat less use of child health services than mothers
of first born children, as these mothers are more experienced and may not
feel the same need for advice as do first-time less experienced mothers.
However, many mothers of later born children do use child health services
notwithstandin9 their previous experience.
INSERT FIGURE 14 HERE
As Australia has so many migrants, some of whom speak a language other
than English in the home, it is important to examine the extent to which
child health services were used by these mothers in the sample. Figure 15
shows the frequency of use of services by mothers from families where a
language other than English is spoken in the home compared with use by
mothers who came from English speaking homes. As can be seen, almost three
times as many mothers who come from families where a language other than
English is spoken, have not used child health services compared with mothers
from English speaking homes. These mothers generally made less use of child
health services than other mothers with only 26.3 per cent using the service
more than 20 times compared with 37.1 per cent of mothers from English
speaking homes.
INSERT FIGURE 15 HERE
•
•
•
•
•
•
•
•
•
•
•
•
Page 58
•
•
.'
."
•
.' e,
... .'
.\ ,
••
i :
. Figure ~ Use 01 Child Health Services By Position Ot Child
In Birth Order
% 01 Children 60r---------------------------~
60 43.7
40
30
20
10
~~~~L-~~~~~~=-~~~~
Never 1 to 6 6 to 20 ) 20 tried TlmOl Tlmel TimOl
Use Of Child Health Services
~ Pin' aa.a g 10(1441. CIl1l4 IZi2 La' aa ...
16 Figure f. Use Of Child Health Service
By Whether Non-English Language Spoken In The Home
To Of Motbora 60
1
26.8
"I 30[
::f .~ IIIII~ \ ... . , ... .
o , .. :. Never tried
16
12.4 :::: :\ ....
~~ :::: ~::::
1 to 5 TlmOl
6 to 20 Tlmel
)20 TlmOl
Use 01 Child Health Services
~ Ocly ECQ'llJb G otbor LacQ'U<Iqo
...
Page 59
- 59 -
Low income may affect the use of services even where there is no cost
involved. Figure 16 indicates that the lower the family income the less
likely mothers were to use child health services. The higher income groups
generally used child health services more frequently. However, it must be
noted that the measure of income used here is family income at the time of
data collection (when the child was in the first year of school) and will
only give a rou9h indication of family income in past years; family income
is also closely connected to mother's current work situation as it includes
mother's income ~s well as father's income. However, the assumption is made
that in general income levels now are relative to those when the child was
an infant.
INSERT FIGURE 16 HERE
As already discussed, mothers of pre-school children are increasingly
entering the work force before their children start school. Of the 8,446
mothers in the sample used in analysis, 1210 (14.3 per cent) returned to
work in the first year of their child's life.
Mothers were asked in the questionnaire to indicate the average numbers
of hours per week in the paid workforce for each year since the birth of the
target child. This information, along with information on the birth data
of the child, was used to create a variable that indicated mother's work
pattern for each year of the child's life. Figure 17 is based on the
average hours worked by mothers when their children were under twelve months
of age. As can be seen, Figure 17 indicates that a greater percentage of
mothers working medium (20 to 29 hours per week) or long hours (more than 30
per week) did not use child health services at all, or used them only a few
times, compared with mothers who did not work at all or who worked shorter
hours. Mothers who did not work outside the home or those who worked
shorter hours in the child's first year used child health services more
often than mothers who were working longer hours.
INSERT FIGURE 17 HERE
No analysis could be carried out to find if family type.influenced the
use of child health services when the child was an infant, as information
about family structure referred only to when the child was in the first year
of school and did not necessarily indicate the family situation when the
child was under twelve months of age.
•
•
•
•
•
•
•
•
•
•
•
•
Page 60
•
•
•
•
eo
e'
e.
.~
Ib Figure /. Use 01 Child Health
Services By Annual Family Income
'I. or famlllet 60r-------------------------______ -.
40
30
20
lO
I - Ii Tlm ••
Use Of ChUd Health Services
~ ($Ui.OOO
~ 126.001-$36.000
\1
~ $16.001-$25.000
B ) $35.000
Figure f: Use Of Child Health Services By Average Weekly Hours In Paid Work
During Child's First Year Of Life
'I. or Mothers 50r---------------------__________ ~
40
30
20
lO
I - Ii Tlm ••
Wo .. TbaD 20 Tlm ••
Use Of Child Health Services
~ Dlc1D'" Wort:
~ 20-29 Bouro
G 1-19 Boan
g ) 30 Boan
\
Page 61
- 61 -
In summary, the characteristics associated with non-use or little use of
child health services were: use of a language other than English in the
home, low family income, the child's later position in the birth order and
whether mother worked medium to long hours in the first year of the child's
life. However, it must be kept in mind that these mothers may have used
child health se;vices for another child, particularly in the case of mothers
of later born children.
Multi-variate analysis was used to further examine the relationship
between the four independent variables - income, language other than English
spoken at home, child's position in the birth order and mother's work
pattern in the first year of the child's life - and the dependent variable,
use of child health services. Because the dependent variable was nominal
and only 12 per cent of the sample was in the non-use category, while the
other 88 per cent of the sample had used child health services, log linear
modelling was chosen as a suitable ~ulti-variate technique. In this
analysis the dependent variable 'use of child health services' was recoded
into two categories only, 'use' and , , non-use •
. Log. linear analysis, using a saturated model, indicated that all second
order associations, that is associations between two of the variables while
controlling for the effects of the others, were significant, with the
exception of the association between language and position in the birth
order. Third order associations were not significant (that is associations
between three of the variables while controlling for the effects of the
others). The separate associations between each of the independent
variables - family income, position in the birth order, language other than
English spoken in the home, mother's work pattern in the first year of the
child's life and the dependent variable' use of child health services, can be
seen in Table 12. All associations were significant at .01, with the
exception of that between mother's work and use of child health services,
which was significant at .04.
INSERT TABLE 12 HERE
The partial Chi-squares and degrees of freedom indicated that income and
language used in the home had stronger associations with use of child health
services than either the position of the child in the family Gr the mother's
work pattern in the child's first year which had the weakest relationship
•
•
•
•
•
'. •
•
•
•
•
•
Page 62
•
• TABLE 12: TESTS OF PARTIAL ASSOCIATION (second order. effects only>
•
•
•
•
Effect name
Language*position in birth order
Language*mothe~'s work
DF
2
in first year 1
Position in birth order *mother's work in first year 2
Language*family income 3
Position in the birth order*family income
Mother's work in first
6
year*family income 3
Language*child health service use
Position in birth order *child health service use
1
2
.' Mother's work in first year*child health service use 1
Family income*child health service use 3
Partial ChiSq. Probe
4.795 .09
11.376 .01
36.555 .01
167.192 .01
39.071 .01
88.287 .01
180.681 .01
25.110 .01
4.435 .04
92.791 .01
Page 63
- 63 -
with use of child health services. However, it is worth noting that
although family income and language other than English spoken in the home
each individually have an association with use of child health services, the
effect of each is independent of the other. The association between the
two, and use of child health services is not significant (that is the third
order effects); in other words they represent separate groups.
Mothers' views of child health services
Mothers were also asked the open-ended question 'What do you think about the
Child Health Service?' (the appropriate name ~or the service in each state
was used). To examine underlying patterns in these responses a coding frame
was developed from a random selection of questionnaires. The randomly
selected ten per cent of the sample, mentioned in the last section, was
coded for analysis.
Table 13 shows the themes which,emerged from the responses and the
percentage of responses in each category; Table 13 also shows the percentage
of mothers who made particular comments. As some mothers made more than one
comment the percent of cases (mothers) in the table totals to more than 100
per. cent in this table.
INSERT TABLE 13 HERE
Three major themes (or categories) emerged from the coded responses of
mothers. As can be seen in Table 13, just under a quarter; 23.1 per cent,
of responses referred to the usage of child health services by first time
mothers, and/or for young babies. Another 23.1 per cent of responses
mentioned the quality of advice and staff training or a description of the
service they had received. The social value of child health· service, what
it provides (or does not provide) for mothers and the community in general
was the third major theme and was referred to in 23.2 per cent of responses.
However, within all categories the responses could have both positive and
negative elements, although most were positive. To examine mothers'
responses to child health services more critically it is useful to look at
these responses from the perpective of mothers who found the services
helpful compared with those who were not helped.
•
•
•
•
•
•
•
•
•
•
•
Page 64
•
•
•
•
•
•
••
TABLE 13: COMMENTS ON CHILD HEALTH SERVICES
CATEGORY
First mothers, young babies useful, good
Staff personal qualities, age,~ motherhood requirements of staff
Quality of advice , and of training, description of service received
Social contact, referral point
Social value, service needed, description of what service does (or does not) provide
Positive and negative comment in one response
Particular situation described 'one-off'
Basic short comment
Other
PER CENT OF RESPONSES
23.1
9.4
23.1
2.6
23.2
5.0
1.4
10.6
1.6
100.0
PER CENT OF CASES
29.8
12.0
29.7
3.4
29.8
6.5
1.8
13.6
2.0
128.7
(This is a multiple reponse question. Mothers could make more than one comment.)
Page 65
- 65 -
Mothers who were helped
Ninety-five per cent of mothers who had used child health services found
them helpful; 41.5 per cent found them very helpful, and 53.3 per cent
helpful. Figure 18 shows how mothers in the three cities ranked the
helpfulness of child health services in their city.
INSERT FIGURE 18 HERE
For mothers who felt that they had been helped, responses to the
question 'What do you think about child healt~ service?' fell. into the same
three major categories reported above, but in larger proportions: 31 per
cent referred to the usage of the service for first time mothers and for
young babies, 31 per cent referred to the social value of child health
service and what it provides or does not provide for mothers and the
community in general, 29 per cent mentioned the quality of the advice, the
quality of staff training and/or a ?escription of the service received by
the respondent. The other 9 per cent of mothers who felt they had been
helped made a variety of responses falling into several of the other
categories (the categories can be seen in Table 13 above).
The following are typical examples of responses from the 31 per cent of
mothers who felt that they had been helped and who, in their comments,
referred to the use of the service by first time mothers and/or for young
babies. (However, as can be seen, mothers often made comments which fitted
into more than one category). It is also worth noting that while these
mothers were generally positive about child health services some also had
criticisms to make.
* Most impressed, very useful service especially for new mothers who
don't know what they are doing. Only one complaint, they tend to go by
the book instead of treating each baby as an individual.
* Very necessary service for mothers with their first child. I have
found many mothers feel very 'housebound' and lacking in confidence with
no positive feedback until they visit CAFHS (child health service)
clinics. I feel CAFHS needs to choose their clinic sisters much more
carefully and to publicise their wider range of services more.
•
•
•
•
•
•
•
•
•
•
•
•
Page 66
•
•
•
•
•
\~
Figure ,l;0: Helpfulness Of Child Heal th Services By City & Total Sample (Only Users Included)
% Of Users 80~--------------------.----------~
70
61.4 60
• 50 45.7·
40
• 30
20
••• o 10 5.1
• .f Very Helpful Helpful Not Helpful
Helpfulness at Child Health Services
•. ~ Melbourne 1::mB Adelaide ~ Perth ~ Total "
Page 67
- 01 -
* Very helpful for first child. Not as necessary for second child as
mother has some previous experience. Nevertheless, helpful for·
reassurance with specific problems. Generally, Maternal and Child
Health Service was helpful in terms of social contact (particularly
other mothers), as well as for health care.
* The service for me was more useful for my first child - more
experienced next time - and is indispensable for mothers lacking
confidence, suffering depression, etc. The recent cuts are to be
deplored, the sister should be present as much as possible, the service
is essential.
The following quotes are typical of those made by the 31 per cent of
mothers who had been helped by the service, and who referred to the social
value of child health service, what it provides (or does not provide) for
mothers and the community in general.
* An essential service that can provide support and understanding for
the infant and mother •
. * I think that it is an essential service that should be expanded, not
depleted. It is a God send for new mothers, and very supportive to
mothers of additional children. I believe that an after hours service
would be invaluable to some mothers who need assistance; after all, most
problems occur in the evening and there are many mums without family or
neighbour help. NB Although there are many services available (ie
emergency lines), being able to ring someone who is familiar is far more
appealing than a stranger. I believe that assurance for mother is dealt
with too lightly. A small amount of assurance can go a long way.
* I think it is a very important link with the mother and the community.
I think it is a service which should never lose any funding but be given
extra funds and extra workers.
* Excellent support and resource for all mothers and families especially
for the first born and those without extended families. It is also a
great service because it is FREE and accessible to mothers without
transport. It is less threatening than hospital and doctor's clinics.
It is also an advantage to have home-visits. Important fqr mothers to
be able to relate to other women and other mothers.
•
•
•
•
•
•
•
•
•
•
•
•
Page 68
•
•
•
•
•
•
The following quotes are typical of those made by the 29 per cent of the
mothers who found these services helpful and mentioned the quality of advice
and staff training and/or a description of the service received by the
respondent.
* I think the Maternal and Child Health Services are wonderful, without
my infant welfare sister I would have had trouble coping with my baby.
Not only are they a great help with the baby, they care greatly for the
mother and her individual problems, giving confidence, which is
important.
* I feel it was a great help in raising my first and continuing growing
family and feel that with the cut backs of late that it must put a great
strain on the unsure new mum, and remove the security of knowing that an
understanding, informative, trained person is a phone call away. I can
now only visit the centre by appointment and when I first came home
couldn't contact the centre for more than a week with several small
problems I had. You don't feel it necessary to go to a doctor or return
to the hospital although they suggest it, so I feel the health service
needs to be looked over again with the view to returning more permanent
staff.
* A positive service. Improved as younger better trained (usually
mothers) women replaced the old guard (often unmarried). I wonder if it
nets (is visited by) the really needy. Impressed that a representative
visited my home.to check on.mother and.child within a week of hospital
discharge.
* An invaluable service, offering sensible advice. The phone service is
also good, especially with a first child, when 'to go to the doctor or
not' can be a problem.
Analysis reported earlier in this paper indicated that one of the groups
associated with non-use of child health services was that where a language
other than English was spoken in the home. As migrants make up a large
proportion of the Australian population it is important to hear the views of
mothers from homes where a language other than English was spoken who had
used child health services. The following comments from these mothers are
typical of those who found the service helpful and very simil~r to those
from mothers in English speaking homes reported above.
Page 69
- 69 -
* It's a great help for mothers like me. (both parents born in the
Philippines)
* I found it very beneficial because it taught me different aspects of
child care. (Both parents born in Yugoslavia)
* I think t~e.centres are indispensable in meeting the needs of new
mothers. These can range from the need for information and guidance
when small as well as large problems arise, to contact with other
mothers (or fathers) with shared concerns. The centres seem to be
ideally placed to cater for the wide ranging nature of these needs.
(mother born in Italy, father in Australia)
Mothers who were not helped
A small minority of mothers, 5 per cent, who had used child health
services for the child in the study, said that they found the service was
not helpful. There were slight differences between the cities as can be
seen in Figure 18. Although this group of dissatisfied users is small,
information about such mothers and the reasons for their dissatisfaction is
important for service providers if they are to improve service provision.
Analysis indicated that these mothers showed no clear characteristics as a
group. However, not surprisingly, they tended to use the service less than
mothers who found it helpful. More than half of this group, 53 per cent,
had used the service as little as 1 to 5 times, whereas the larger group of
mothers who found the service 'helpful' or 'very helpful' tended to use the
service much more frequently and only 16.2 per cent and 6.3 Per cent
respectively of these groups had used it only 1 to 5 times.
When asked the question 'What do you think about the child health
service?', nearly half, 46 per cent, the group of mothers who felt that they
had not been helped by child health services, referred to the quality of
advice, the quality of staff training and/or a description of the service
received. The following responses are typical and give some indication of
why these mothers felt they were not helped.
•
•
•
•
•
•
•
•
•
•
•
•
Page 70
•
•
•
•
. : •
- IV -
* I thought that the Infant Welfare sisters relied too much on
statistics and not enough on the fact that every child is an individual
and advances at his own pace. Too many graphs are used which only
confuses matters. After having one child, the second child's visits
were completely unnecessary.
* Too pushy. Not all children are textbook cases.
* They do things out of a book written in the eighteenth century.
* They are not up to date with problems (health) of new born children.
They are only familiar with text book problems. I found them terribly
lacking in my area •
* Insistence on continuation of breast feeding was detrimental to the
early development of the baby. Also the particular difficulties of
working mothers were not addressed.
The comments of another 28 per cent of mothers who had not found child
health services helpful referred to personal qualities of the staff, their
age.group, and whether they were mothers themselves. The following are
typical replies from mothers in this category. It is worth noting that the
comments are not entirely negative.
* Good to weigh babies, but the women (health sisters) are usually
spinsters (childless) and .were not at. all knowledgeable with breast
feeding and its problems, .and were very discouraging and did nothing for
one's confidence in this area. They try to run babies to a clock.
* I never used. the service for my second and third child. I found the
sister whom I saw with my first child was too busy telling me, she never
listened to me.
* I think it depends on the individual centre. The principle is good,
but some of the staff may not be as good as others, therefore the
service is then affected. The centre I went to was not very good.
* They are a good idea BUT more often than not they have never had
children themselves and try to force ideas onto mothers. On paper these
ideas sound good but they don't always work in practice.
Page 71
- 71 -
* Depends largely on the wisdom and experience of the sister in charge.
With my children 1, 2 and 3, she was excellent. With number 4 the
sister was not at all helpful.
The other 25 per cent of mothers who felt that they had not been helped
by child health services made comments that fell into all the remaining
categories sho~ in Table 13; there were no clear patterns.
It is also important to examine the views of mothers in homes where a
language other than English is spoken, who have not found child health
services helpful, to see if their experience ~s the same as other mothers
who have not found the services helpful or if they have any special reasons
for feeling that they were not helped. The following are typical responses
from these mothers. It is interesting to note that with the exception of
the comment about English speaking these mothers are critical of child
health services for the same sort of things as mothers who speak English at
home.
* The nurse was not very helpful and although my English is quite good
she treated me as if I did not understand anything. I left the place
without being any less worried about my child's health. (Both parents
born in Hungary)
* Waste of time! (Both parents born in Greece)
* Most of the Health Centre sisters I have dealt with have never had
children of their own and when you have a problem child I don't think
they have the practical experience. I also felt that they thought I was
the 'dumb' mother who didn't know anything and they did know it all.
(Mother born in Greece, father born in Yugoslavia)
* I think that it is a waste of time, the things that they told me I
already knew them all. The only thing I thought was good about it was
that they weigh them! (Both parents born in Italy)
* Are fantastic for those mothers that don't know anything about health
and how to stimulate their children. (both parents born in Chile)
•
•
•
•
•
•
•
•
•
•
•
•
Page 72
•
•
•
•
•
•
•
- 72 -
Conclusions
Child health services in Melbourne, Adelaide and Perth were used and
appreciated by most mothers in the sample. Many mothers pointed out how
important the service was to first-time mothers, others pointed out how
essential the service is to mothers, children and the community as a whole.
Many mothers me9tioned the quality of the advice and the training of the
staff. Some mothers found that visiting the child health centre and
meeting other mothers prevented feelings of isolation.
Only a small group of mothers· (5 per cent'- who had used child health
services found they were not helpful. Many of these mothers referred to the
quality of the staff and their training. They objected to the rigidity and
narrowness of some advice and attitudes. Many of the mothers who felt they
were not helped alsol referred to personal qualities of the staff: that they
had no children of their own and lacked personal experience of motherhood~
that they had their own ideas about what was right and did not respond to
the particular circumstances of mother and child, and that they were too
'bossy'. A theme which came through, particularly among mothers who were
not helped, but also to some extent with mothers who were helped, was the
fact that much depended on the particular sister and centre, and that the
service could vary a great deal.
Over the period of time that Australian child health services have been
operating there have been reviews and reorganisation of the various services
at different times, but essentially they have remained educative and
supportive services available to all mothers with infants and/or young
children, rather than being intrusive and supervisory. Child health
services are available to those who want to use them and attempts are made
to reach all mothers; however, mothers can choose to use what is provided or
to stay away, the choice is theirs to make. It was quite clear from the
comments of some mothers that they appreciated the element of choice because
they did not have to attend if they felt confident with later born children
or did not like the sister at their centre.
It is interesting to compare this element of choice in Australian child
health services with the British system of health visitors where the element
of choice is less available. Mayall and Foster (1989) found that health
visitors in Britain, who can call on mothers in their homes unannounced,
perceived themselves and were perceived by parents as having the 'dual role
Page 73
- 73 -
of "policer" and "friendly advisor"'. Foster contrasted the English system
with the French, which is closer to that operating in Australia; the role of
the French 'puericultrice' is to promote the health of pre-school children
in a variety of settings, but in particular in the child health clinic
(Foster, 1988-89). Like the Australian child health nurse, the French
puericultrice visits homes only through arranged visits, but the main
service offered~is centred on the clinic. Foster (1989) argues that these
basic differences in operation lead to different ideas about parents and
their role, with the British health visitor having a more negative view of
parents than their French counterparts who view parents as responsible
adults who can make decisions for themselves about the care of their
children. Foster points o~t the strain placed on the English health
visitor, who tends to visit certain houses more often than others in their
effort to watch over their charges.
They (health visitors) have a caseload and are expected to 'keep an eye'
on all households in that caseload. They are accountable to society for
the wellbeing of these children. For example, they have been blamed by
official reports on cases of child abuse and in the press for failing to
oversee a family if a case of undetected child abuse occurred (Foster,
·1989, 326).
In the Australian system, like the French system, parents retain the
major responsibility for children. No evidence was found in the comments
made that Australian mothers who used child health services see nurses as
having a 'policing' role with families and children; mothers·~·who did not
like child health services could choose not to attend without" fear that
their decision could be over-ridden. Although this choice means that some
mothers do not attend centres, it appears that most mothers do so and the
.majority find them helpful.
Nevertheless, providers of child health services should, not rest on
their laurels. The group of non-users tended to come from particular
sections of society: those on lower incomes, those where a language other
than English was spoken in the home, those where the child was later born
and a slight tendency to non-use by mothers working long hours. However, it
must be remembered that some of the mothers who did not use the services for
the particular child in the study may have used them for other children.
The non-use by mothers of later-born children is not so worrying as the non
use by mothers in the other categories. On the other .hand, the children in
•
•
•
•
•
•
•
•
•
•
•
•
Page 74
•
•
•
•
•
•
•
•
•
•
- J4 -
this study were born in 1982, '83 and '84 and there have been some changes
in service provision since then. For example, hours have been extended on
some nights at some centres, health checks are carried out in some child
care centres and so on. At the same time some of the major trends in
society have intensified: there are now more mothers in the workforce,
particularly mothers of infants and pre-school children, poverty is
increasing due ;0 unemployment, and there has been continuing immigration
including people from non-English speaking backgrounds.
In the past, child health services. have been innovative and inventive in
servicing the needs of mothers and. infants in bard to reach circumstances;
for example, using the 'Tea and sugar train' in Western Australia to reach
mothers in far off regions, providing travelling caravans and correspondence
sections. Some modern day mothers in city locations, rather than the
country, may need services which are just as inventive and which make use of
locations other than clinics. Consultation with ethnic community groups,
and low income support groups, may ~dentify new approaches to meeting their
needs. Provision of more flexible opening hours for centres so that working
mothers can visit at convenient hours may be necessary to meet the
increasing needs of busy working mothers.
Child health service providers should also take note of the criticisms
of some of the users. Some nurses appear to be too rigid and to operate 'by
the book'. To what extent do these nurses understand the problems of
families in modern society where increasingly mothers of very young children
are entering the work force and leaving' their children in the care of others,
where many families come from very different cultures with different values
and ways of doing things, and where many speak a language other than English
at home? Some child health nurses may be more suited to some people and
some areas than others. Refresher courses which keep nurses up to date not
only on health matters but also on what is happening in families and society
are essential. Australian society has changed, and Australian families have
changed. Trying to balance work and family demands is a problem for many
parents, trying to adapt to a new and often strange society is a problem for
others, while low income places pressures on parents and is linked with low
self esteem. Child health services and individual nurses must be sensitive
to these difficulties.
Child health services are used by most mothers and most believe it is an
important and worthwhile support. Nevertheless, the needs of the mothers
Page 75
- 75 -
who felt that they had not been helped must not be forgotten as their views
indicate some areas which need improvement. Perhaps the final comment
should come from a mother whose experience was close to ideal.
The sisters gave help, advice, support, lent items (eg breast. pump) and
there was always an ear to listen and a shoulder to cry on.
•
•
•
•
•
•
•
•
•
•
•
•
Page 76
•
•
•
•
•
•
•
•
•
5. THE EFFECTS OF NON-MATERNAL CARE IN THE FIRST TWELVE MONTHS OF LIFE ON
CHILDREN IN THE FIRST YEAR OF SCHOOL
There has been considerable debate for many years about the effects of non
maternal care on children in the pre-school years. Current concern in
Australia and many other Western countries focuses on the effects of long
hours of non-maternal care on infants, particularly those under 12 months of
age. This concern is partly related to the increasing number of mothers who
are returning to work while their children are very young, partly to
difficulty in finding satisfactory child-care, particularly for very young
children, but also to publicity given to rese~rch by Belsky et al (1988), in
the United States, which indicates a greater degree of insecure attachment
in infants who had been in long hours of non-maternal care.
This study was designed to examine some of the long-term impacts of
varying child care contexts on Australian children and ,their developing
competence. Although' most of this ~nalysiB will be based on data in Stage 2
of the study, the larger sample at stage 1 gives us an opportunity to look
at some effects on children who experienced long day care away from their
mothers in the first 'twelve months of life.
Much of the fear about the possible negative effects of non-maternal
care on pre-school children stems from interpretations of John Bowlby's
research in the 1950s which emphasised the importance of mother-infant
bonding ahd attachment, and the detrimental effects of separation from
mother. Bowlby's work was actually concerned with the effects of maternal
deprivation on infants and young children brought up in hospitals and
institutions and who had suffered severe deprivation; however findings have
been generalised to' children living with their own mothers and fathers.
Bowlby claimed that young children could suffer psychological damage if
separated from mother or mother substitute in the first five years of life;
he also claimed that this is one of the principal causes of delinquency.
However, this claim has not been borne out by research in the thirty or
forty years since; separation from mother has not been found to have long
term effects on children in families, rather delinquency and behaviour
problems have been linked with ongoing conflict in the family (Rutter; 1976;
Rutter, 1981, 1984, 1989; Tizard, 1986).
Although Bowlby claimed it was not harmful for mothers to_leave their
babies and young children occasionally with their own mother or a known
Page 77
- 77 -
dependable adult, he also stated that' ••. to start nursery school much
before. the third birthday is for most children an undesirably stressful
experience' (Bowlby, 1973, 54). It became generally accepted that children
were at risk if mothers went out to work before they were 3 or even 5, and
that work should be part time only. Oakley (1981, 217) argues that: 'The
reason why Bowlbyism caught on was that his message fitted the spirit of the
times: the 1950s. were a reactionary time for women ••• '.
Bowlby also argued that there is a tendency for children to. attach to
one figure and that attachment to mother is qualitatively different from
other attachments. However this argument has ~lso been challenged by
research which indicated that some children are more attached to father,
although he may not be the primary caregiver, and some are attached to
several people; attachment is not dependent on the amount of time spent with
the child but rather the quality of the relationship (Rutter, 1981; Tizard,
1986). Studies have also indicated that father's role was both more
important and more direct than prev~ously realised (Lamb, 1976, 1977;
Clarke-Stewart, 1980; Pederson, 1980; Chibucos and Kail, 1981; Parke, 1981) •
. A survey of non-industrialised countries in the late 1970sfound that
child rearing is usually shared with other members of the extended family
and it is rare for mothers to be exclusively responsible for children
(Weisner and Gallimond, 1977, cited in McCartney and Galanopoulos, 1988).
For example, the care of young Maori children is seen as the pleasure and
the responsibility of the family group. In Pacific Island cultures there is
no word for mother; mothers and aunts share the same name and
responsibilities (Meade, 1988). In these societies mother care is not seen
as something unique, a fact that serves as a warning against assuming too
readily that one form of child care is necessarily superior to other forms.
During the 1960s Western researchers were concerned with the quality of
mother-child attachment and whether child care in centres was bad for
children. They found however that children in child care were just as
attached to mother as children cared for only by mother. Although there was
no difference in intellectual development, children in child-care centres
were found to be a little more 'aggressive' and 'independent' (McCartney and
Galanapoulos, 1988). Nevertheless, this research was criticised because the
children studied were cared for in high quality centres, often on university
campuses, whereas many children are cared for in centres with lower
•
•
•
•
•
•
•
•
•
•
•
•
Page 78
•
•
•
•
•
•
•
- 78 -
standards. This led Jay Belsky, who, in a review of the literature had come
to the conclusion that children were not harmed by child care (Belsky and
Steinberg 1978), to look once more at the effects of non-maternal care.
Belsky recently reversed his original stance and in an extensive review of
the research (1989) argues that there is substantial evidence of a link
between early placement in day care and later attachment and social
development proglems in children (Tizard 1986; Karen 1990).
While Bowlby argued that attachment to mother was essentially different
from attachment to any other person, Belsky, in line with more recent
research on the importance of the father, considered attachment to father an
important factor also, and in this sense is not as rigid in his definition
of attachment as were the earlier attachment theorists. Belsky's research
(Belsky and Rovine, 1988), found higher rates of insecure attachment in
babies (under 12 months) who had been in long hours of non-maternal care or
non-parental care. Belsky also reports several other studies with similar
findings. Belsky's research and other research on infant attachment rests
largely on the credibility of the. 'Strange Situation Technique' which was
developed by Mary Ainsworth to observe attachment behavior in mothers and
infants (Tizard 1986; Karen 1990).
Ainsworth believed that mothers' sensitivity to the signal of their
infants was a key factor in attachment, and that attachment in infancy was a
good predictor of later emotional and social behavior (Rutter, 1981; Tizard,
1986; Karen, 1990). The Strange Situation observation technique, a series
of eight episodes of combinations of mother, baby and stranger in a room,
has been criticised on several grounds, including validity. It is an
artificial situation in which mother and child are observed, and does not
take into account many other factors influencing the child's behaviour,
including child temperament and family factors. Babies do differ in their
ways and experience. Babies who. have been in child care may appear detached
not because they are insecure but because they are more independent, more
accustomed to the care and presence of strangers and used to coming and
going (Scarr and Dunn, 1987; McCartney and Galanopoulos, 1988).
Clarke-stewart (1988) questions the assumption that the Strange ,,'
Situation technique when used with children accustomed to non-maternal care
is psychologically equivalent to its use with home reared children. She
points out that the Strange Situation technique' ••• is premised on cr~ating
a situation in which the infant feels moderately stressed and therefore
Page 79
- 79 -
displays proximity seeking behavior to the object of his or her attachment' .
The strange Situation, therefore, may not be as stressful for infants
accustomed to non-maternal care as for home 'reared infants, as familiarity
may affect their responses. Clarke-Stewart (1988) also points out that
there are cultural variations in response to the strange Situation
technique, with some cultures having a high proportion of infants classified
as· insecurely a~tached; the artificially created situation is obviously not
stressful to infants from all cultures.
Research has also indicated that babies with several attachments are
less distressed if mother works outside the home than those with only one
attachment (Scarr and Dunn, 1987). Studies have shown that babies in child
care protest just as much at separation from mother as those at home with
mother; both groups showed a preference for mothers rather than care-givers.
No studies of day-care children have shown them to be more emotionally or
socially maladjusted (Tizard, 1986), although Belsky is doubtful about this
claim (Belsky, 1988).
The most valuable aspect of Belsky's recent review of the effects of
infant day care is the discussion of the broader issues involved in non
maternal care of children with reference to previous research. He looks
further than mere attachment theory and quality-of-care arguments, and
discusses the broader ecological circumstances of the family. Although
Belsky is concerned about increased rates of insecure attachment in children
in long hours of care in the first 12 months, he also points out that there
were some children in long hours of care who did not show insecure
attachment, and that it is therefore important to look for factors in the
family environment or in children themselves which are protective (Belsky
and Rovine, 1988; Belsky, 1988).
Nevertheless, Belsky's claim that insecure attachment at the end of the
first year is a risk factor which is associated with later aggression and
noncompliance is questionable (Fein and Fox 1988; Clarke-Stewart, 1988).
Aggression and non-compliance may also be interpreted as assertiveness and
independence. As Clarke-Stewart (1988) argues 'day care children may be
more "bratty" than home care children; they may want their own way and do
not have the skills to get it. This does not mean they are maladjusted.
More clinically sensitive measures of maladjustment are needed to prove that ,
case .
•
•
•
•
•
•
•
•
•
•
•
•
Page 80
•
•
•
•
•
•
•
•
•
•• ,
- bU ~
Fein and Fox (1988, 230) point out that some attachment theorists are
rethinking the meaning of attachment in the first year of life and' ••• now
argue for naturally occurring transformations in the quality of attachment
during the second and third years of life. Secure and insecure attachment
measured at the end of the first year is not viewed as a critical factor in
subsequent personality formation, but rather as one component in a
probabilistic model, along with continuity and stability of home ~
environment, life stress events, and the like'.
Family factors affecting-children
King and MacKinnon (1988), who reviewed research over the 1980s on the
relationship between day care and child development, assert that the
important question in regard to non-maternal care of children is how
qualities of the home interact with qualities of the day care environment to
affect child outcomes. Both Bronfenbrenner (1986) and Belsky (1988) suggest
that researchers should take an ecological approach, which includes family
factors, to the effects of non-maternal care on child development.
Although research taking into account both family and day care factors
has so far been limited methodologically, both in scope and sample size, a
number of family factors have been suggested as mediating the effects of day
care on infants and also influencing the choice of non-maternal care
(Hoffman, 1983; Belsky, 1988; Clarke-Stewart, 1988; King and MacKinnon,
1988; McCartney and Galanopoulos, 1988; Richters and Zahn-Waxler, 1988).
Richters and Zahn~Waxler' (1988)' suggest that family factors may not merely
mediate or buffer the effects of non-maternal care, but may account for
child outcomes independently. Family characteristics such as SES, and
family structure (single or two-parent) are likely to have both direct and
indirect effects on child outcomes, and also to influence the choice of non-
parental care (Belsky, 1988; Schachere, 1990; King and Mackinnon, 1988). We
know from other research that family conflict has a negative effect on
children's competence (Ochiltree and Amato 1984; Amato 1987; Ochiltree
1990).
Children from birth are part of a family system which influences the
developing child as a whole, and also through dyadic relationships with
individual members of the family (Minuchin, 1977). 'Both parents influence
their children's development and which parent is more importa~t varies with
the child's age, sex, temperament and environmental circumstances.
Page 81
- 81 -
Furthermore, it is not always meaningful to regard the influence of each
parent as separate and independent. The mental health of one parent may
influence that of the other and may also influence the marital relationship.
The family consists of individuals and pairs of individuals, but it is also
a social group of its own and needs to be considered as such' (Rutter,
1981). Nevertheless, there are indications that child-specific
relationships may be more important than overall family relationships ~
(Rutter, 1989)
Characteristics of the mother, such as her emotional state (King and
MacKinnon, 1988; Schachere, 1990; Lancaster, ~rior and Adler,. 1986),
quantity and quality of the mother-child relationship (Hoffman, 1983;
Clarke-Stewart, 1988; Mccartney and Galanopoulos, 1988; Schachere, 1990),
the father-child relationship (Hoffman, 1983; Belsky, 1988; Schachere,
1990), parenting skills (King and MacKinnon, 1988; Belsky, 1988; Richters
and Zahn-Waxler, 1988), family processes such as conflict and stress
(Rutter, 1976, 1981; Ochiltree and Amato 1984; Amato 1987; Belsky, 1988;
Fine and Fox, 1988; Ochiltree 1990), the marital relationship (Belsky, 1988;
Richters and Zahn-Waxler, 1988; Schachere, 1990), and job stress (Belsky,
1988; Clarke-Stewart, 1988) may affect child outcomes. with older children
the. negative effects of family conflict on adjustment and self ·esteem have
been well documented (Nye, 1957; Raschke and Raschke, 1979; Ellison, 1983;
Ochiltree and Amato, 1984).
Schachere (1990) suggests that the marital relationship affects how both
husband and wife function as parents and that a good relationship may act as
a parent support system. Clarke-Stewart (1988) paints out that employment
in the work force is hard on mothers and that this stress may affect their
relationships within the family, including those with their children.
Belsky (1988) cites research by Pederson and colleagues (1983) which found
that employed mothers of infants attempt to compensate for being absent by
spending more time with them and may displace father's time. He infers from
findings in studies which found that mothers of anxious-resistant infants
stimulated them and/or were more affectionate than mothers of secure
infants, that this behavior may inadvertently lead boys to have less secure
relationships with their fathers. However, there is no direct evidence for
his claim (Clarke-Stewart, 1988).
•
•
•
•
•
•
•
•
•
•
•
•
Page 82
•
•
•
•
•
•
•
•
..
- 82 -
Child Characteristics
There is both theoretical and empirical evidence that children are active
participants in the socialisation process. The theories of the cognitive
psychologists, Jean Piaget, Noam Chomsky and others, are based on the
premise that children have a built in tendency to explore and master the
environment, an~ to learn the unstated rules of .the world about them
(Ginsberg and Opper, 1979; Wine, 1981; Skolnick, 1981). Research over the
last couple of decades has indicated that babies, although limited in their
physical development, actively' attempt··to· master their environments very
early in life (Rheingold, 1971; Schaffer and Crook, 1978; Bell, 1979). The
environment in this sense is both physical and human, with the infant
attempting to predict and control both (Donaldson, 1978). Research has also
indicated that alert, responsive babies get more attention from mothers than
less responsive babies, that difficult new babies are more easily stressed
than others, and that mothers talk less to irritable babies (Tizard, 1986).
Children take an active role in relationships not just within the family but
in all settings. For example Zinsser, (1988) found family daycare minders
liked to care for children who were "good" and not demanding •
. While there is some evidence that boys are more affected by non-maternal
care than girls (Hoffman, 1983; Belsky, 1988; Schachere, 1990), Clarke
Stewart (1988) points out that the evidence is not strong. Child
temperament is also likely to affect child outcomes (Tizard, 1986; Clarke
Stewart, 1988; Richters and Zahn-Waxler, 1988). For example, Belsky (1988)
found that insecurely attached infants' of working mothers had more difficult
temperaments. Clarke-Stewart (1988) suggests that mothers' perceptions of
infant temperament are more important than objective tests. Siblings,
particularly older siblings, may also have an influence on children's
development and response to non-maternal care (Tizard, 1986).
The long term effects of early experience
There is a strong belief among parents and the public in general, arising
from the influence of Freud, Bowlby and others, that events which occur in
infancy and early childhood have a significant influence on later happiness
as an adult (Kagan, 1984). This belief makes mothers in particular, and
parents in general, disturbed when they are informed that infants in non
maternal care in the first twelve months of life are at risk of insecure
attachment and possibly later psychological problems. However, as Rutter
Page 83
- 83 -
(1989), in a comprehensive examination of the issues and related research
argues, this belief has been challenged by findings from research over the
last three decades. 'It became clear that people changed a good deal over
the course of development and that the outcome following early adversities
was quite diverse, with long-term effects heavily dependent on the nature of
subsequent life experiences (Clarke and Clarke, 1976). Even markedly
adverse experiences in infancy carry few risks for later development if the
subsequent rearing environment is a good one (Rutter, 1981)'.
Fien and Fox (1988, 233) in the introduction to the Early childhood
research quarterly. Special issue: infant da~care, sum up the issues: '
it seems clear that current studies, even those set within attachment
theory, have too many methodological problems and constraints to serve as
the basis for alarm or negative conclusions about the consequences of early
non-parental care. In the near future, the aim of systematic research will
be to devise measures of important attributes of parents, children,
caregivers, and settings; to devis~ procedures for identifying research
populations; and to devise strategies for building needed control conditions
into our group comparisons' •
. In addition to the methodological problems mentioned above, most
research on non-maternal (and non-parental) care and its effects has been
carried out in the United States, a country which is different in many ways
from Australia. In the light of changing patterns of child rearing, renewed
interest in the effects of child-care on children, and particularly on
infants, Australian research is necessary to provide a basis::.~for informed
policy and planning, and to assist mothers making decisions about the care
of pre-school children.
The Australian Early Child care Contexts study
A major concern of the Australian Early Child care Contexts study is the
relationship between a broad range of family factors, child characteristics,
and different patterns of caring for children, including non-maternal care,
in the years between birth and starting school (at approximately 5 years of
age), and child competence in the first year of school. This section of the
report examines some of the effects of non-maternal care in the first twelve
months of life on child outcomes, using data from Stage 1 of the. study.
•
•
•
•
•
•
•
•
•
•
•
•
Page 84
•
•
•
•
•
•
•
,
- b4 -
Hoffman (1983) criticised research examining the effects of maternal
employment on young children for small and biased samples, and indicated the
need for longitudinal or retrospective studies with less biased samples. In
order to obtain a representative sample of mothers of young children in the
present study, the sample was selected from children in their first year of
school; a retrospective approach was thus taken to care of children in the
pre-school years. Besides obtaining a random sample, this method had the
advantage of providing urgently needed information much faster than by
beginning with a birth cohort of children. Nevertheless, it is planned to
make thi~ a longitudin~l study.and to return to the children in the stage 2
sample at a later date, (perhaps when_the_child~en are 9 or 10 years of age).
As discussed in the introduction this study is theoretically based on an
understanding of the development of competence in children. The concept of
competence stresses the positive aspects of development rather than only
deficits, and encompasses a wide range of human functioning both social
emotional and cognitive and educatiQnal (Smith, 1969; Connolly and Bruner,
1974; Edgar, 1980; Wine, 1981; Amato, 1987; Ochiltree, 1990).
Family factors and child characteristics which are included in the
design of the study can be seen in Table 1 (see introduction). Many were
suggested in the earlier discussion of research in this area, but others,
such as mother and child health and the life events scale, are included as
possible stressors in the family system. Mother's perception of the quality
of the neighbourhood and the services provided are also included, as they
may have an impact on child outcomes through effects on the family (Rutter,
1981); but much of this analysis must wait until Stage 2 and is not
available in this stage 1 report.
Table 2 (see introduction) shows the various ch~ld care contexts
included in the design and indicates what is included at Stage 1. At Stage
2 of the study analysis need not be limited to simple comparisons of one
form of care with another; comparisons can be made of multiple forms of care
with simple contexts of care, continuity of care with discontinuity, and
mother's satisfaction with the care situation can be taken into account
also. Table 3 (see Introduction) shows the measures of child outcomes
(competence) used in the study; included are indicators of the social
emotional and the cognitive-educational status of children. However, as
indicated earlier, analysis in this report is limited to data_collected in
Stage 1 of the study.
Page 85
- 85 -
The effects on children of non-maternal care.
In the light of current concern with the effects of early non-maternal care
on infants, analysis in this section of the report focuses on children who
'were in non-maternal care in the first year of life (and who were in the
first year of school at the time of data collection). Any analysis from
this stage of the study can only be preliminary because of the limited
nature of the data and the lack of full information on the family.
In particular this analysis will examine the Stage 1 data·, for any
evidence which would support Belsky's argumen~, based on attachment theory,
that long hours of non-maternal care of children in the first year of life
is a risk factor in the later development of psychological problems. This
analysis will therefore examine the relationship between the hours children
were in non-maternal care in the first year of life and socio-emotional or
behaviour difficulties in their first year of school which are likely to be
in combination indications of psych~iogical problems. The current study
does not use the usual 'Strange Situation' technique, but includes other
measures which bear on the question of children's adjustment.
The. stage 1 Measure of Social Emotional Difficulty
In order to obtain some information on the general competence of children
whose mothers took part in Stage 1 of the study a checklist was included in
the questionnaire. This checklist, which was adapted from the ACER Parent
Checklist (with permission from ACER), consists of a number of skills and
behaviours which children are expected to have developed by the time they go
to school in Australia. The checklist was originally designed to be filled
in by parents (usually mother) and given to the teacher when their child
commenced school so that the teacher would have some idea of the child's
skill level or general competence. Mothers' perceptions of children's
behavior and development is the most viable way of obtaining information in
a questionnaire, but mothers also have the most opportunity to observe their
children over a long period of time. Objective observations by others are
usually for short time periods only and therefore are less accurate (Carey,
1982).
The ACER checklist was somewhat out of date and sexist. The wording was
changed to make it non-sexist, it was up-dated and new items about language
and emotional development were added. The checklist was trial led in three
•
•
•
•
•
•
•
•
•
•
•
•
Page 86
e
e
•
•
•
•
•
••
e,
- 86 -
pilots of the questionnaire before the main study commenced. It was
expected that the scale would be positively skewed (as it proved to be)
because the items are ones which most children should have achieved before
commencing school. However, the more important issue was to find which
children had not achieved this desired level of competence, as perceived by
their mothers.
The full checklist as set out in the questionnaire was in a simple 'tick
the box if the item applies to your child' format. Some ite~s were reversed
to prevent set expectations. The checklist included items such as 'Knows
full name', 'Talks -in· sentences', 'Dresses'him·self/herself most of the
time', 'can use scissors' and other items which are more concerned with
social and emotional behaviour such as 'Seems to worry a great deal', 'Likes
to play with other children', and so on.
The items from this scale which discriminated (i.e. frequency was less
than 90 per cent), 14 items in all,. were selected for further analysis.
These 14 items were subjected to principal components factor analysis from
which one main factor emerged (Alpha Coefficient .68); it includes 7 items
relating to socio-emotional behaviour patterns in children. This 'Social
Emotional Difficulty' factor consisted of the following·items 'Seems to
worry a great deal', 'Cries very easily when upset', 'Often has temper
tantrums when upset or corrected',' 'Is very restless or active, never stays
still for a moment', 'Inattentive, doesn't notice what is happening', 'Is
aggressive with other children', and 'Appears miserable, unhappy, tearful or
distressed'. Children could score" from "0 to 7 on this scale. Most items on
this scale are generally regarded as undesirable in school age children in
western society if frequent and in combination and are seen as an indication
of some psycho-social difficulties. But ACER in the handbook for the
checklist points out that there can also be cultural variation in results
(Rowe 1979).
Analysis
This Social-Emotional Difficulty scale (derived from the ACER checklist) is
the primary focus in this assessment of the argument that long hours of non
maternal care in the. first twelve months of life is a risk factor in the
development of later problems of aggression, non-compliance, or
psychological problems. Although stage 1 of the study was not explicitly
designed to appraise Belsky's findings, the study's large sample base
Page 87
- 87 -
permits, at the very least, a preliminary examination of the longer term
effects of non-maternal care in the context of a broader non-'Strange
Situation' assessment.
The multivariate OLS approach undertaken here involved regressing the
Social-Emotional Difficulty scale on a variety of factors available in Stage
1 of the study and thought to be plausibly associated with the child's ~
socio-emotional and behavioural well-being, as indicated in the earlier
discussion.
These measures included indicators of:
- the child's child care arrangements at the early infancy stage (i.e.
whether the child had been placed in informal or formal care and the
average number of hours per week the child was cared for by a non-parent
in the first twelve months);
- the characteristics of the child (i.e. its gender, its sibling order and
whether it had a disability);
-the child's family situation (i.e. whether they have two parents, average
hours mother was in paid employment in the child's first year of life, and
how satisfied the child's mother was with life);
- three important measures of the social background of the child (i.e. the
degree of parental ~thnicity, parental education and fami~y income).
What is of interest in appraising the Belsky approach is the extent to
which the child care arrangements are seen to have a significant and
independent effect on the child's subsequent proneness to Social-Emotional
Difficulties - after controlling for the presumed influence (whether
realised directly or indirectly) of the various social background, family
situation and child characteristic factors. Our sample size and background
measures enable us to take a more 'ecological' approach than many other
studies have been able to attempt.
It should be noted that the initial correlations between the Social-
emotional Difficulty. scale and the three child care arrangement variables do
not provide bivariate support for the broad 'attachment' ·hypothesis. The
negligible relationships between informal (r= -.03) and formal (r= .02)
•
•
•
•
•
•
•
•
•
•
•
•
Page 88
•
•
•
•
•
•
•
•
•
- 88 -
child care and Social-Emotional Difficulty respectively, and that between
duration of non-maternal child-care and Social-Emotional Difficulty (r= .01)
are of such low magnitude, and/or in the opposite direction to Belsky's
hypothesis, that one might reasonably suppose further, more stringent,
multivariate analysis was unwarranted.
Nevertheles~, the possibility that the effect of child-care arrangement
on subsequent Social-Emotional Difficulty has been masked (or suppressed) by
the confounding influence of the social background, family situation and
child characteristic variables, some of which do exhibit non-negligible
zero-order relationships with the Soc~al-Emotronal Difficulty measure,
suggests that a further stage of multivariate assessment is required.
As Table 14 demons~rates, however, controlling for the various social
background, family situational and child-specific factors does not reveal
evidence of any suppressor effect(s) in action; rather, child care
arrangements are seen, again, to have no statistically significant influence
on level of Social-Emotional Difficulty - and given an N of over 8000, such
significance is not difficult to achieve.
INSERT TABLE 14 HERE
Instead, the most important, albeit weak, direct ('positive') influence
on the child's level.of Social-Emotional Difficulty is seen to be his/her
parents' degree of ethnicity; for example, net of other factors, children of
parents born in non-English speaking 'countries and speaking a language other
than English in the home are likely, on average, to score half a point
higher on the Social-Emotional Difficulty scale than children coming from
Australian born families and may be due to cultural differences or to the
difficulties of dealing with cultural differences. On the other hand,
social background factors such as family income and education exhibit
'negative' direct influences on the Social-Emotional Difficulty scale - that
is, children from the better educated and higher income families show lower
Social-Emotional Difficulty scores than do their less privileged peers.
Of the family situation factors, by far the most important (and in fact
the most important of the independent influences discussed here - importance
being gauged by the relative magnitudes of the unstandardised regression
coefficient x mean products) is the life satisfaction of the ~hild's mother.
Other things being equal, in families with 'satisfied' mothers, children are
Page 89
•
TABLE 14 • OLS REGRESSION OF SOCIAL-EMOTIONAL DIFFICULTY
ON FAMILY SOCIAL BACKGROUND AND SITUATION, CHILD CHARACTERISTIC AND CHILD CARE ARRANGEMENT VARIABLE •
",.
VARIABLE b B
• SOCIAL BACKGROUND
ETHNICITY .47 .20 EDUCATION
DEGREE -.21 -.05 • < 11 YEARS .27 .08 FAMILY INCOME
($100) -.04 -.09
FAMILY SITUATION • TWO PARENTS NS NS NO. HOURS WORKED NS NS SATISFACTION WITH LIFE -.71 -.13
CHILD'S CHARACTERISTICS • MALE .13 ·.04 ELDEST .23 .07 DISABILITY .32 .05
CHILD CARE ARRANGEMENTS • INFORMAL NS NS FORMAL NS -NS HOURS CARED FOR BY OTHERS NS NS
INTERCEPT 2.14
ADJR .10 P<.OOOO •
EXCEPT WHERE NOTED, ALL VARIABLES SIGNIFICANT AT P<.OOO •
•
•
Page 90
•
•
•
•
..
•
•
• "
- 90 -
seen to have almost one (out of seven) fewer symptoms of Social-Emotional
Difficulty than the children of mothers who are 'not satisfied' with their
life. However, this relationship is probably because mother's reports of
child behaviour tend to reflect some aspects of the mother as well as the
child, although they are the most viable method of obtaining information
about children, as discussed earlier (Lancaster 1986).
In addition, being a boy, an eldest sibling and/or a disabled child are
attributes of children exhibiting very slightly, but significantly, greater
levels of Social-Emotional Difficulty, once other factors have been taken
into account.
It should be emphasised, however, that none of the above factors
constitutes, on the basis of the data examined here, a mono-causal
explanation of childhood social-emotional problems; nor together do they
'explain' a compelling proportion of the variation in levels of Social
Emotional Difficulty. What these data and their measures do provide even in
the preliminary manner presented here, are reasons to suspect that
attachment theory may well be downplaying the role social background, family
situational and child-specific factors play in the child's socio-emotional
and-behavioural development, especially when assessed in the wider, more
realistic context of the survey setting.
Discussion
The analysis reported here is not conclusive. However, it does suggest that
long hours of non-maternal care in the first years of life and mothers
working are not the primary cause of socio-emotional difficulties on school
entry. Rather, this analysis suggests that socio-emotional difficulties as
measured by the Social-Emotional Difficulty scale, are related to broader
family background factors and characteristics of mother and child. However,
it is important to note that this preliminary ~inding is not entirely at
odds with those reported by 8elsky when he asserts:'Nor has it been my
goal to argue that nonmaternal care per se poses risks to the child. It is
clear that many factors and processes are confounded, that not all children
realize the risks, and that some account of variation in development of
infants with extensive nonmaternal care is called for. All too often,
however, those accounts that have been offered fall short from an empirical
standpoint' (Belsky; 1988, 265).
Page 91
- 91 -
As pOinted out in the introduction, there are many changes in Australian
society which are affecting the way in which children are reared in early
childhood. The increasing number of mothers returning to the labour force
is only one of these changes; however, it is the one which is the focus of
much concern and controversy. More young children would suffer the effects
of poverty if their mothers did not work, and there is much research to
demonstrate tha~ poverty has a negative and limiting effect on child
development.
The Stage 2 data from interviews of 728 mothers (selected from Stage 1
on the basis of the differing forms of caring for children) will provide the
opportunity to include more sensitive measures of family functioning, as
well as maternal and child characteristics, and to examine child outcomes
for both direct and indirect effects. There is also a more comprehensive
range of measures of child outcomes included in Stage 2: Clay's concepts of
print (reading), Larson's copying test (a Piagetian non-language based
test), the ACER Teacher Checklist (which includes teacher's perceptions of
the child's memory and attention, language skills, and most importantly for
purposes of continuing an examination of the issues presented in this
chapter, social development and emotional development), in addition to the
ACER Parent checklist filled· in by mothers at Stage 1. Information on the
child's personality as an infant and at the present time is also available
as well as mother's perception of how the child is adjusting to the school
situation. stage 2 also includes open ended material which is available in
both coded form or as quotes. This open ended material provides the
opportunity for case studies to both illustrate and explore the interaction
of the various factors which may affect child development in greater depth.
The analysis presented here provides no support for the theory that long
hours in non-maternal care in the first year of life is a risk factor which
is associated with later psychological problems. While the arguments about
the effects of non-maternal care continue, mothers who have no choice but to
work continue to have difficulty in finding child care places for their
children; the majority, whether through choice or not, must rely on informal
care, particularly for infants. Information from Stage 2 of this study will
provide further detailed analysis of the effects of different contexts of
care using a range of outcome measures and, much needed information for
informed policy and decision making in Australia.
•
•
•
•
•
•
•
•
•
•
•
•
Page 92
•
•
•
•
•
•
•
•
• ;
REFERENCES
ABS (1986), Australia in brief: Census 1986, Cat. No. 2501.0.
ABS (1988), Births Australia, Catalogue No.3301.0.
ABS (1988), Deaths Australia, Catalogue No.3302.0.
ABS (1990) Labour force status and other-characteristics of families,
Australia, Catalogue No. 6224.0.
Amato, P. R., (1987), Children in Australian families, Prentice Hall,
Sydney.
Belsky, J. (1987), 'Science, social policy and day care: a personal
odyssey', paper presented at the biennial meeting of the Society for
Research in Child Development.
Be1sky, J. (1988), 'The "effects" of infant day care reconsidered' Early
childhood research quarterly, Vol.3, No.3, pp.235-272.
Belsky, J. and Rovine, M.J. (1988), 'Nonmaternal care in the first year of
life and the security of infant-parent attachment', Child development,
NO.59, pp.157-167.
Belsky, J. and Steinberg, L. (1978), 'The effects of day care: a critical
review', Child development, Vol.49, No.4, pp.929-949.
'Bowlby, J. (1973), separation: anxiety and anger, Penguin, Harmondsworth.
Bronfenbrenner, U. (1986), 'Ecology of family as a context for human
development: research perspectives' Developmental psychology, Vol.22, No.6,
pp.723-742.
Brownlee, H. and King, A. (1989), 'The estimated impact of the family
package on child poverty', in Edgar, D., Keane, D. and McDonald, P~ (eds),
Child poverty, AlIen and Unwin, Melbourne.
Page 93
- 93 -
Campbell, Dame Kate (1976), 'The Progress of Infant Welfare Services in
victoria Over the Past Fifty Years', paper presented at the Jubilee
Conference on Maternal and Child Health, Melbourne.
Carey, W.B. (1982), 'Validity of parental assessments of development and
behavior' American journal of diseases of children, Vol.136, pp.97-99.
carmichael, G. and McDonald, P. (1987), 'The rise and fall of divorce in
Australia 1968-1985', Paper presented at the Population Association of
America meeting, San Francisco.
Chibucos, T.R. and Kail, P.R. (1981), 'Longitudinal examination of father
infant interaction and infant-father attachment', Merrill-Palmer quarterly,
Vol.27, No.2, pp.81-96.
Child, Adolescent and Family Health Service (1989), Celebratinq Eiqhty Years
of Community Child Health Care, Adelaide.
Child, Adolescent and Family Health Service, (no date), Child Welfare
History - the qrowth of Mothers and Babies Health Association.
Child Health Services in Western Australia, (c 1972).
Clarke, A. and Clarke, A.D.B. (1976), Early experience: myth and evidence,
Open Books, Somerset.
Clarke-Stewart, A. (1980), 'The father's contribution to children's
cognitive and social development in early childhood', in PEDERSON, F.R. ed.,
The father-infant relationship: observational studies in the family setting;
Praeger, New York.
Clarke-Stewart, A. (1988), 'The "effects" of infant day care reconsidered',
Early childhood research quarterly, Vol.3, No.3, pp~293-318.
Clausen, J.H. (1966), 'Family structure, socialization, and personality',
Lois Hoffman (ed), Review of Child Development Research, Sage, New York.
Dally, A. (1982), Inventing motherhood: the consequences of an ideal,
Burnett Books, London.
in
•
•
•
•
•
•
•
•
•
•
•
•
Page 94
•
•
•
•
•
•
•
•
•
•
• J
• i
- 94 -
Department of Immigration, Local Government anD Ethnic Affairs, Australia's
population trends and prospects 1988, AGPS, Canberra.
Department of Public Health Infant Health Service, (1964), The Infant Health
Service of Western Australia.
Donaldson, M. (1978), Children's minds, Fontana, Glasgow. ,.
Edgar, D. (1971),'Competence, autonomy and conformity in adolescent
socialisation', in Conference Papers, Vol.l, unpublished.
Edgar, D. (1974), The competent teacher, Angus and Robertson, Sydney.
Edgar, D. (1975) ,Sociology of Education: a book of readings, Mcgraw-Hill,
Sydney.
Edgar, D. (1980), Introduction to Australian society, Prentice Hall, Sydney.
Edgar, D., Keane,D., and McDonald P. (eds.) (1989), Child Poverty, AlIen and
Unwin, Sydney and .AIFS, Melbourne.
Ellison, E.S. (1983), 'Issues concerning parental harmony and children's
psychosocial adjustment', American journal of orthopsychiatry, Vol.53, No.l,
pp.73-80.
Fein, G.G. and FOx, N. (1988), 'Infant day care: a special issue', Early
childhood research guarterly, Vol.3, No.3, pp. 227-234.
Foster, M. (1988-8.9), 'The French puericultrice', in Children and Society,
No.4, pp. 319-334.
Gandevia, Bryan (1978), Tears often shed: child health and welfare from
1788, Permagon Press, Sydney.
Ginsberg, H. and Opper, S. (1979), Piaget's theory of intellectual
development, Prentice Hall, Englewood Cliffs.
Harrison, J.F.C. (1973), The Early victorians 1823-1851, St Albans, Panther.
Page 95
- 95 -
Henderson, R.W. (1981), 'Home environment and intellectual performance', in
R.W.Henderson (ed), Parent-child Interaction, Academic Press, New York.
Hoffman, L.W. (1983), 'Maternal employment and the young child' in
Perlmutter, M. (ed) Minnesotta symposium on child psychiatry, pp.l01-127.
Inkeles, A. (19~5), 'Social structure and the socialization of competence',
Harvard Educational Review, Vol.36, pp.265-283.
Kagan, J. (1984), 'continuity and change in the opening years of life', in
Emde, R.N. and Harmon, R.J., Continuities and aiscontinuities in
development, 'Plenum, New York.
Karen, R. (1990), 'Becoming attached', in The Atlantic monthly, February,
pp.35 - 70.
King, D. and Mackinnon, C. E. (1988·), 'Making difficult choices easier: a
review of research on day care and children's development' Family relations,
Vol.137, pp.392-398.
Lamb, M. (1976), The role of the father in child development, Wiley, London.
Lamb, M. (1977), 'Father-infant and mother-infant interaction in the first
year of life', Child development, Vol.48, pp.167-181.
Lancaster, S., Prior, M. and Adler, R. (1986), 'Child behavior ratings: the
influence of maternal characteristics', Psychology Department, La Trobe
University, Melbourne.
MacDonald, Prof. W.B. (1975), 'Why mothers do not bring their children to
child health centres', paper presented at Liberal Party of Australia (West
Australia Division), State Women's Council Current affairs Convention, 26th
and 27th May.
McDonald, Peter (1990), 'The 1990s: Social and economic change affecting
families', Family Matters, No. 26, April, Australian Institute of Family
Matters.
Maas, F. (1987), 'Families in poverty in the 19805', Newsletter, No.10, May,
Australian Institute of Family Studies.
•
•
•
•
•
•
•
•
•
•
•
•
Page 96
•
•
•
•
•
•
•
•
•
• !
• )
- 96 -
Maas, F. (1989), 'Demographic trends affecting the workforce', Paper
presented at Corporate Childcare: the Boottom Line, a conference organised
by Childcare at Work Ltd., Sydney.
Mayall, B. and Foster, M. (1989), Child health care: living with children,
working for children, Heinemann, Oxford.
Mccartney, K. and Galanopoulos, A. (1988), 'Childcare and attachment: a new
frontier the second time around', American journal of orthopsychiatry, Vol.
58, NO. 1, pp.16-24.
Meade, A. (Convenor) (1988), Education to be more: report of the early
childhood care and education working group, Wellington.
Minuchin, S. (1978), Families and family therapists, Tavistock, London.
Nye, F.I. (1957), 'child adjustmen~ in broken and unhappy unbroken homes'
Marriage and family living, vol.19, pp.356-361
Oakley, A. (1981), Subject women, Martin Robertson, Oxford.
Ochiltree, G. (1990), Children in stepfamilies, Prentice Hall, Sydney.
Ochiltree, G. and Amato, P. (1984), 'Family conflict and child competence',
Australian family research conference Nov. 1983, Proceedings Vol VI, AIFS,
Melbourne.
Parke, R. D. (1981), Fathering, Fontana, Glasgow.
Pederson, F. A. (i980), The father-infant relationship: observational
studies in the family setting, Praeger, New York.
Porter, B, and O'Leary, K.D. (1980), 'Marital discord and childhood behavior
problems' Journal of abnormal child psychology, Vol.8, No.3, pp.287-295.
Prosser, B. (1981), Families and work, Family Information Bulletin No.l,
Institute of Family Studies, Melbourne.
Poulter, Jean (1976), 'The Part Played by Nurses', paper presented at the
Jubilee Conference on Maternal and Child Health, Melbourne.
Page 97
- 97 -
Raschke, H.J·. and Raschke, V.J. (1979), 'Family conflict and children's self
concepts: a com~arison of intact and single-parent families' Journal of
marriage and the family, Vol.4, No.2, pp.367-374.
Rheingold, H. (1971), 'The social and socializing infant' in D.A. GOSLIN
(ed), Handbook of socialization theory and research, Rand McNally, Chicago.
Richters, J.E. and Zahn-Waxler, C. (1988), 'The infant day care controversy:
current status and future directions', Early childhood research guarterly,
Vol.3, No.3, pp.319-336.
Rutter, M. (1976), 'Parent-child separation: psychological effects on the
children' in Clarke A. M. and Clarke, A.D.B. (eds), Early experience: myth
and evidence, Open Books, Somerset.
Rutter, M. (1981a), 'The city and the child' American journal of
orthopsychiatry, Vol.5, No.4, pp.610-625~
Rutter, M. (1981b), Maternal deprivation reassessed, Penguin, Harmondsworth.
Rutter, M. (1984), 'Continuities and discontinuities in socioemotional
development: empirical and conceptual perspectives', in Erode, R.N. and
Harmon, R.J. (eds), Continuities and discontinuities in development, Plenum,
New York.
Rutter, M. (1989), 'Pathways from childhood to adult life', Journal of child
psychology and psychiatry, Vol.30, NO.1, pp.23-51.
Scarr, S. and Dunn, J. (1987), Mother care/other care, Penguin,
Harmondsworth.
Schachere, K. (1990), 'Attachment between working mothers and their infants:
the influence of family processes', American Journal of orthopsychiatry,
Vol.60, No.1, pp.19-33.
Schaffer, H.R. and Crook, C.C. (1978), 'The role of the mother in early
social development', in H. McGurk (ed), Issues in childhood social
development, Methuen, London.
•
•
•
•
•
•
•
•
•
•
••
•
Page 98
•
•
•
•
•
•
•
•
•
- '::it! -
Skolnick, A. (1981), 'The family and its discontents', Society, Jan-Feb,
pp.42-47.
Smith, M. Brewster (19690, Social psychology and Human Values, Aldine,
Chicago.
Southern Community Health Services Research Unit, (1990), Nothing or no-one
could have told me what it was going to be like, South Australian Health
Commission, Adelaide.
Teale, W.H. (1982), 'Pre-schoolers and literacy: some insights from
research', Australian Journal of Reading, Vol.5, NO.3, pp.153-162.
Tizard, B. (1986), The care of young children: implications of recent
research, Thomas Coram Institute, Working and occasional papers 1, London.
Weston,R. (1985), 'Marriage and the, nature of family poverty', Paper
presented at the National Conference of the United Nations Association of
Australia: National status of Women Committee.
White, Burton L. (1979a), 'The family: the major influence on the
development of competence', in N. Stinnet, B. Chesser and J. De Frair,
Building Family Strengths: Blueprints for action, University of Nebraska,
Lincoln.
White, Burton L. (1979b), The Origins of Human Competence: the final report
of the Harvard Pre-school Project, Lexington Books, Lexington.
Wine, J.D. (1981), 'From defect to competence', Social competence, Guilford,
New York.
Zelizer, V. (1985), Pricing the priceless child, Basic Books, New York.
Zinsser, C. (1989), Born and raised in East Urban, a report to the Ford
Foundation on a community study of informal and unregulated child care,
Center for Public Advocacy Research, New York.
Page 99
•
•
•
• --'
•
. -
Ref:;"··::;.r--t on Stage C'ne of.
the Ear-! ."" Chi lc:lhc .. :::; .. j
C:ontexts Study:
• \. ---- - I
• FAMILY
• INFORMATIO!~ CENTRE
A',· 1 :., r>.'-U" , ,,,. . p. ,', j;<j ~ , , I U I E
01" L ... 'L. { ~ I IJ iJ I L 8 .
•
••
•
Page 100
a!!r-ft Australian Institute of Family Studies 766 Elizabeth Street Melbourne Victoria 3000 Telephone (03t34£9160;:f~~,i
. ""-. ~ :"
•
•
•
•
~.
•
•
•
•