39
Authentic Biology Human Genetics Debbie A Lawlor ([email protected]) Nic J Timpson ([email protected])

Authentic Biology Human Genetics
Debbie A Lawlor ([email protected])
Nic J Timpson ([email protected])

• What is a genome-wide association study?
• Why are we interested in gene-disease association?

2000 2007

DNA tests to revolutionise fight against
cancer and help 100,000 NHS patients Monday 10 December 2012
Prime Minister David Cameron ...to transform cancer
treatment in England with new proposals to introduce
high-tech DNA mapping for cancer patients and those
with rare diseases, within the NHS. The UK will be the
first country in the world to introduce the technology
within a mainstream health system.... The genome
profile will give doctors a new, advanced
understanding ... ensuring they have access to the
right drugs and personalised care far quicker than
ever before.
Plans for NHS database of patients' DNA angers privacy campaigners Critics of initiative to be unveiled by David Cameron talk of 'Big Brother' system that could identify individuals The Guardian | TheObserver
NHS faces privacy storm over
plan to store thousands of
patients' DNA to help develop
life-saving treatments.
Daily Mail




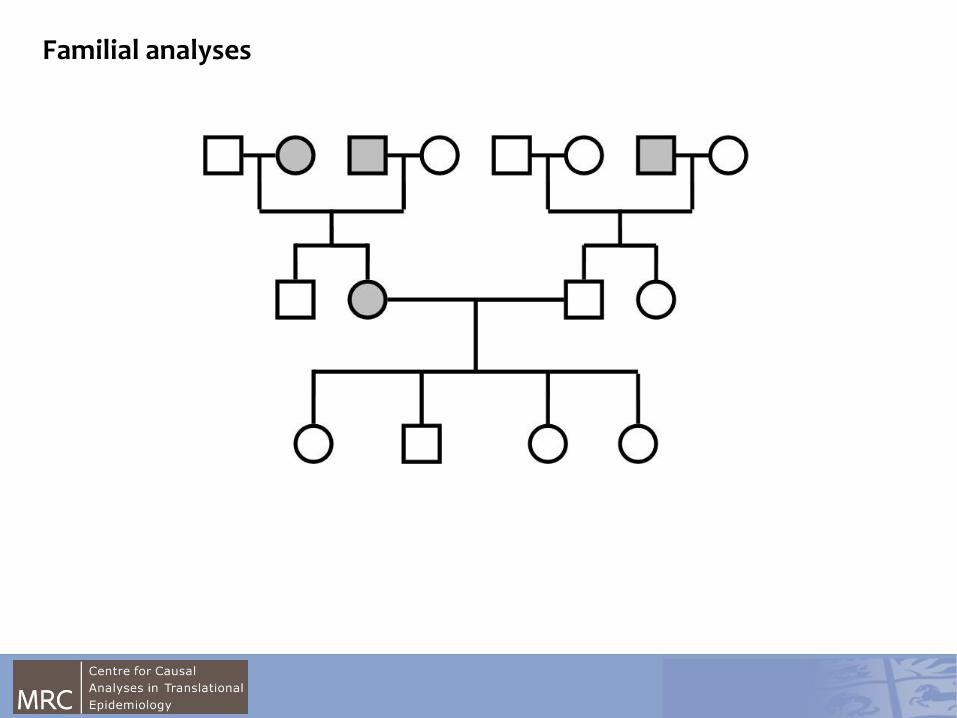
Familial analyses

Montague et al, Nature 387:903–908
Monogenic Obesity
Michael et al Nature (2000) 404, 661-671
0500
1000
1500
Frequency
20 40 60
BMI
- Severely obese cousins from a highly consanguineous family. - Both children had undetectable levels of serum leptin.
- Individuals were found to be homozygous for a frameshift mutation in the “ob” gene, which resulted in a truncated protein that was not secreted.
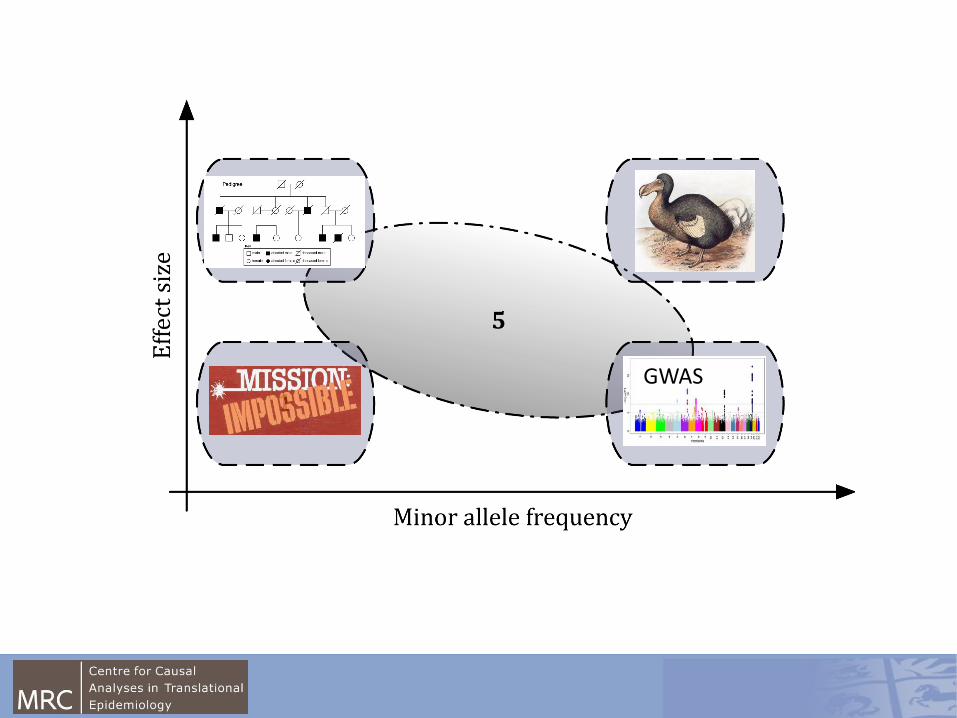
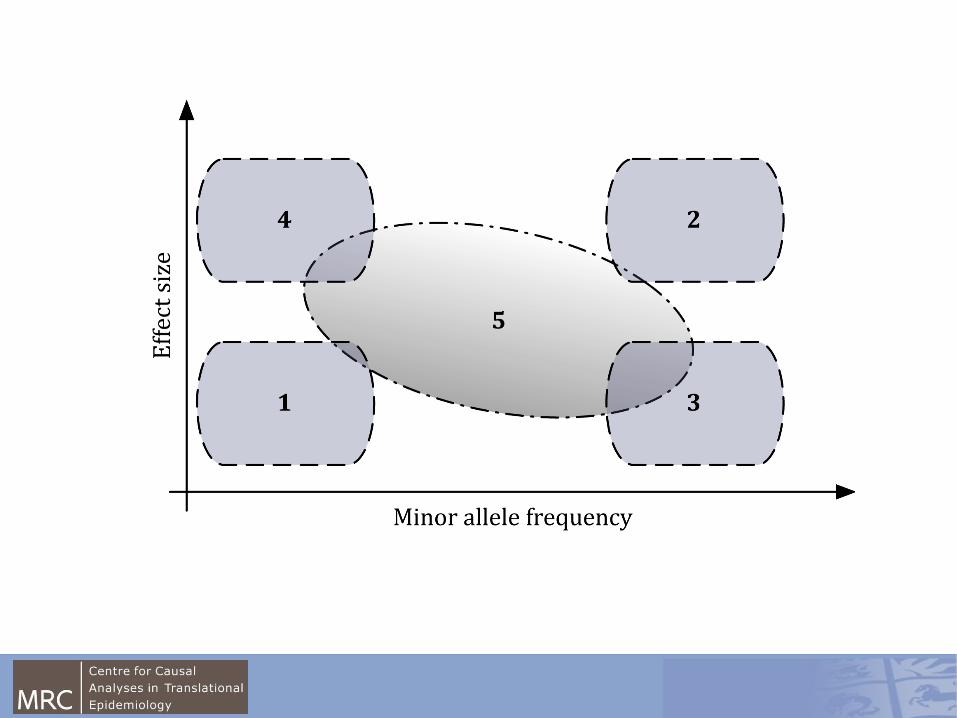
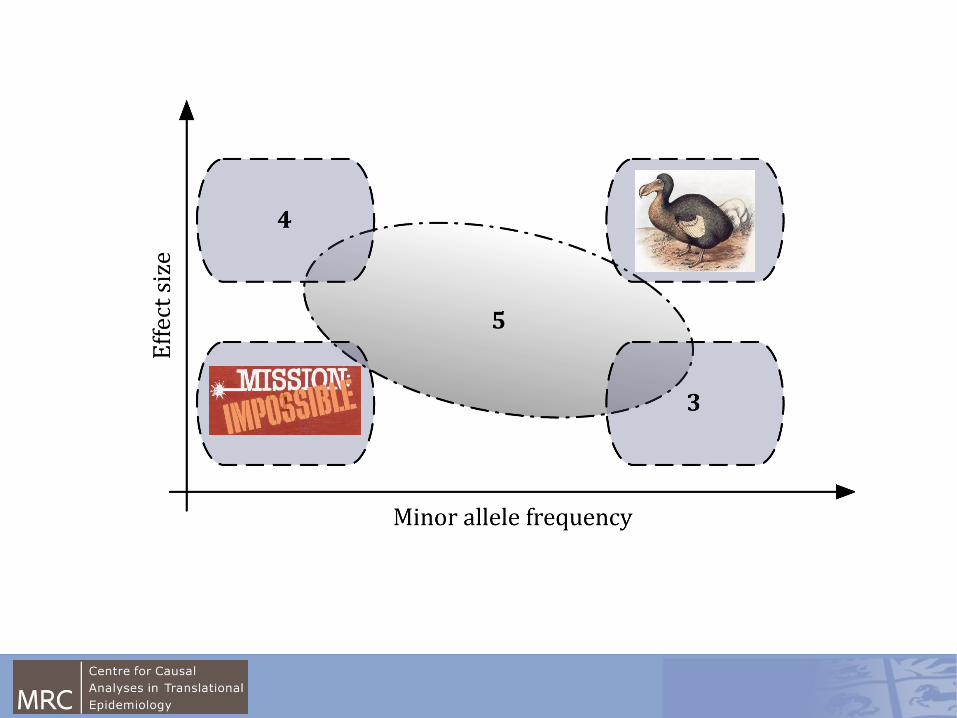
GWAS

Now we have the ability to ask all available hypotheses at the genetic level simultaneously and to avoid the biases of candidacy.
Technological advance

0.05
.1.15
Density
20 30 40 50 60
BMI
BUT, are these “genes for obesity”?
FTO effect ~0.1SD
across the distribution
Equivalent to <1kg per
change at this gene
0100
200
300
400
500
Frequency
20 30 40 50 60
BMI
0500
1000
1500
Frequency
20 40 60
BMI

Uses of GWAS
• Better understanding of disease
• New drug treatments
• Whether none genetic modifiable risk factors cause disease
Uses of GWAS
• Better understanding of disease
• New targets/mechanisms
• Whether none genetic modifiable risk factors cause disease
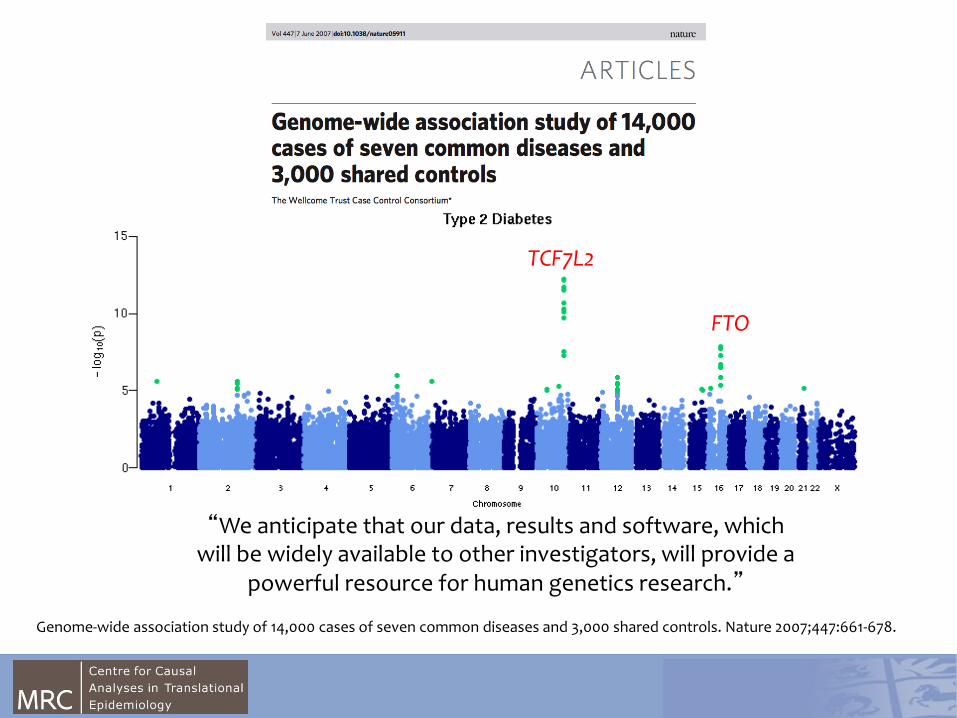
“We anticipate that our data, results and software, which will be widely available to other investigators, will provide a
powerful resource for human genetics research.”
TCF7L2
FTO
Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature 2007;447:661-678.

TCF7L2

Uses of GWAS
• Better understanding of disease
• New targets/mechanisms
• Whether none genetic modifiable risk factors cause disease

Example: Definition of FTO effect
Science 2007;316:889-894.
Pauling Centre for Human Sciences – Feb 2012

FTO
TMEM18
MC4R
GNPDA2 BDNF
NEGR1
SH2B1
ETV5
MTCH2
KCTD15
SEC16B
TFAP2B FAIM2
NRXN3
GPRC5B RBJ
MAP2K5
QPCTL
FANCL
TNNI3K
LRRN6C
FLJ35779
SLC39A8
TMEM160
CADM2
LRP1B
PRKD1
MTIF3
ZNF608
PTBP2
RPL27A
NUDT3
ORIGINAL FINDINGS Frayling et al Loos et al Willer et al 2007/9
WEIGHT & WAIST Lindgren et al 2009
NOVEL BMI Speliotes et al 2010
Pauling Centre for Human Sciences – Feb 2012

FTO – An effect through appetite?
American Journal of Clinical Nutrition 2008;88:971-978.
N Engl J Med 2008; 359:2558-2566
Science 2007;318:1469-1472
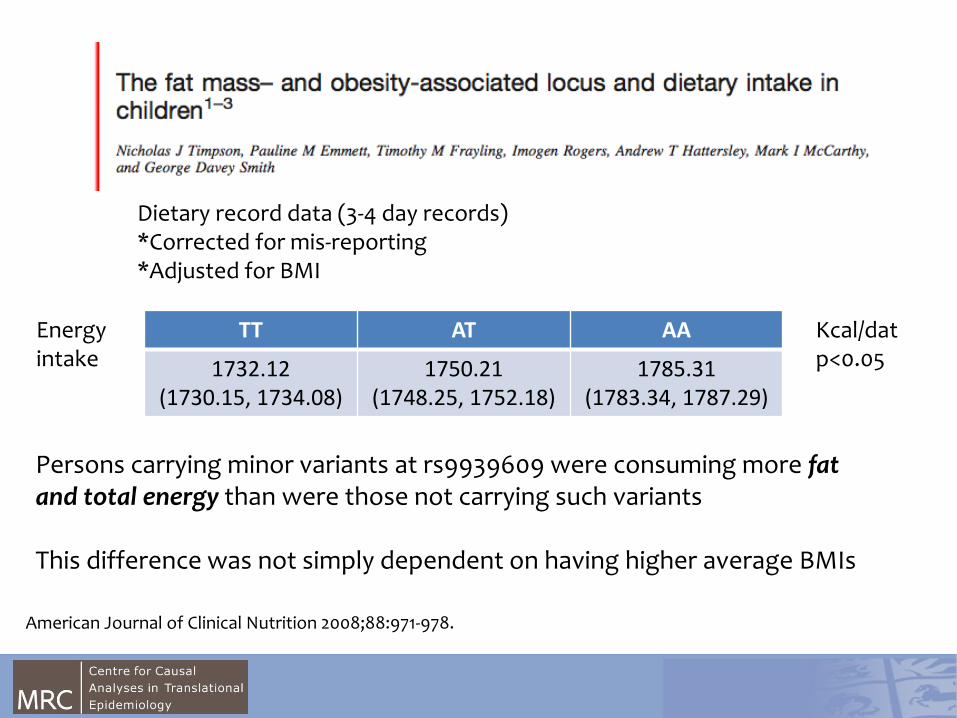
TT AT AA
1732.12 (1730.15, 1734.08)
1750.21 (1748.25, 1752.18)
1785.31 (1783.34, 1787.29)
Kcal/dat p<0.05
Persons carrying minor variants at rs9939609 were consuming more fat and total energy than were those not carrying such variants This difference was not simply dependent on having higher average BMIs
Dietary record data (3-4 day records) *Corrected for mis-reporting *Adjusted for BMI
Energy intake
American Journal of Clinical Nutrition 2008;88:971-978.

Energy intake Kcal/day/BW
Church et al. Nature Genetics 2010;42:1086–1092

Uses of GWAS
• Better understanding of disease
• New targets/mechanisms
• Whether none genetic modifiable risk factors cause disease

• BMI is associated with a wide range of health outcomes, including associations with greater glucose, insulin and adverse lipid profile
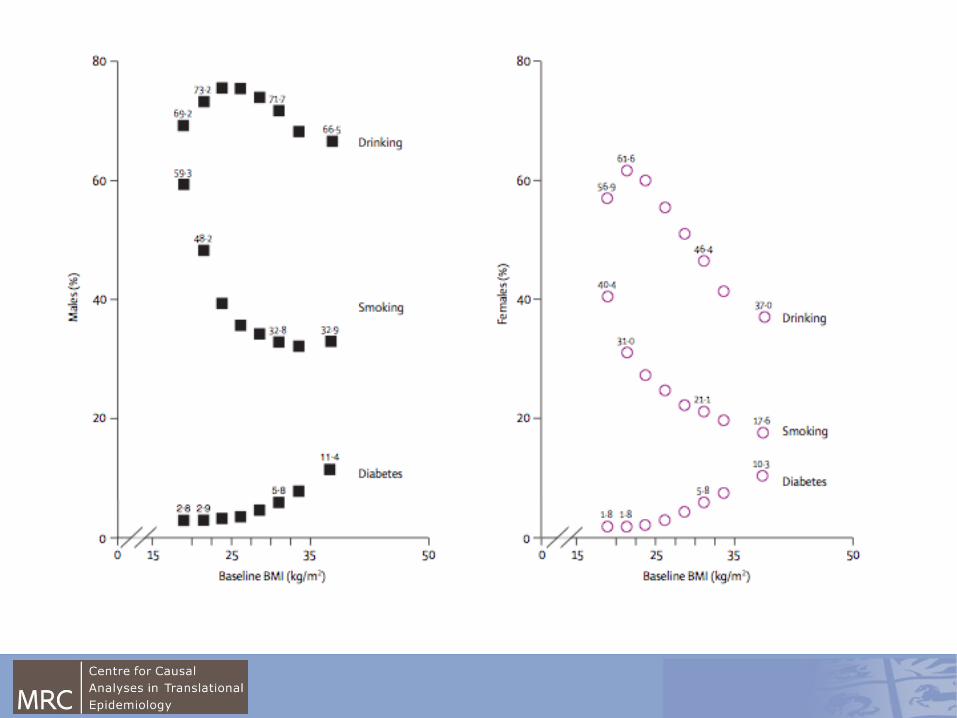
• Is the association exaggerated due to confounding by e.g. SEP, physical activity?
• Is the association an underestimate because of masking (confounding) by smoking and reverse causality?
Example: Is greater BMI causally associated with adverse metabolic & vascular traits?

Body mass Heart Disease
Diabetes
CONFOUNDED
Confound it! The batteries are dead
Body mass genes

0.05
.1.15
Density
20 30 40 50 60
BMI
Nature’s randomised controlled trials Random allocation of alleles e.g. coding for BMI
TT
Higher BMI
AT or AA
Lower BMI
TT AT/AA p
Manual Social Class 56% 57% 0.8
Smoking 44% 44% 0.9
Sedentary 65% 64% 0.3
CHD Outcomes CHD Outcomes

Triangulation of associations
BMI
FTO genotype
Metabolic traits
a c
b

Triangulation: Insulin
FTO genotype
BMI Fasting Insulin
a = 0.088SD greater BMI per A allele FTO
b = 0.038SD greater insulin per 0.088 SD BMI
c = ??

Triangulation: Insulin
FTO genotype
BMI Fasting Insulin
a = 0.088SD greater BMI per A allele FTO
b = 0.038SD greater insulin per 0.088 SD BMI
c = 0.039SD per A allele FTO

-0.06
-0.04
-0.02
0
0.02
0.04
0.06
0.08
-0.04 -0.02 0 0.02 0.04 0.06 0.08
Insulin
Glucose
HDL
LDL
Triglycerides
SBP
DBP
ALT
GGT
HbA1c
Expected SD change in trait per 0.1 SD BMI
Observed SD change in trait per FTO A allele
Observed effect sizes were exactly as expected for all traits
Error bars show 95% CIs

Points to take away from this introduction:
**What is known about the genetics of complex traits like adiposity? **How did we make those discoveries and how has technology drive change? **How should we interpret genetic associations with complex traits? **What can be done with associations of common genetic variation with obesity/BMI – function/phenotype definition/causality/?

Then we figure out the function of genes with cell biology studies in zebrafish

Date What Who
12th
Dec.
Introduction to human genetics/
GWAS
Debbie Lawlor, Nic Timpson,
Rebecca Richmond, Kaitlin
Ward ....
17th
Dec.
Authentic biology symposium Queen
Mary’s London
9th Jan. Human GWAS practical Nic Timpson, Rebecca
Richmond, Kaitlin Ward,
Debbie Lawlor ....
Xth Jan. Zebra Fish husbandary and genetic
tools
Chrissy Hammond
Yth Jan. ZFIN identification of disease gene
orthologues
Going forward – time-table

















