AUTHORIZATION AGREEMENT FOR DIRECT DEPOSITS (ACH CREDITS) Company Name: Toledo Mudlogging Services, Inc. I hereby authorize TOLEDO MUDLOGGING SERVICES. INC hereinafter called COMPANY, to initiate credit entries to my: (select one) Checking Account Indicated below at the depository financial institution named below, hereinafter called DEPOSITORY, and to credit the same to such account. I acknowledge that the origination of ACH transactions to my account must comply with the provisions of U.S. law. Depository Name: Zip: Routing Number: Account Number: This authorization is to remain in full force and effect until COMPANY has received written notification from me of its termination in such time and in such manner as to afford COMPANY and DEPOSITORY a reasonable opportunity to act on it. Savings Account Branch: City: State: Name: SS Number / Phone Number .( ). Email: Signature: Date: / /20. NOTE: ALL WRITTEN CREDIT AUTHORIZATIONS MUST PROVIDE THAT THE RECEIVER MAY REVOKE THE AUTHORIZATION ONLY BY NOTIFYING THE ORIGINATOR IN THE MANNER SPECIFIED IN THE AUTHORIZATION.
Transcript
AUTHORIZATION AGREEMENT FOR DIRECT DEPOSITS (ACH CREDITS)
Company Name: Toledo Mudlogging Services, Inc.
I hereby authorize TOLEDO MUDLOGGING SERVICES. INC hereinafter called COMPANY, to initiate credit entries to my: (select one)
Checking Account
Indicated below at the depository financial institution named below, hereinafter called DEPOSITORY, and to credit the same to such account. I acknowledge that the origination of ACH transactions to my account must comply with the provisions of U.S. law.
Depository Name:
Zip:
Routing Number:
Account Number:
This authorization is to remain in full force and effect until COMPANY has received written notification from me of its termination in such time and in such manner as to afford COMPANY and DEPOSITORY a reasonable opportunity to act on it.
Savings Account
Branch:
City:
State:
Name:
SS Number / Phone Number .( ).
Email:
Signature: Date: / /20.
NOTE: ALL WRITTEN CREDIT AUTHORIZATIONS MUST PROVIDE THAT THE RECEIVER MAY REVOKE THE AUTHORIZATION ONLY BY NOTIFYING THE ORIGINATOR IN THE MANNER SPECIFIED IN THE AUTHORIZATION.
M i l a m , T X
• Many, L A
do understand that if i do not complete fourteen (14) days
of training, or fail the urine analysis, the $200.00 expense of my pre-employment physical and drug
Position applied for (1) Days/hours available to work No Pref Thur
and salan/ desired (2) Mon Fri (Be specific) Tue Sat
Wed Sun
How many tiours can vou work weekly? Can you work niqhts?
Employment desired _ FULL-TIME ONLY _ PART-TIME ONLY _ FULL- OR PART-TIME
When available for work?
TYPE OF SCHOOL NAME OF SCHOOL LOCATION (Complete mailing
address)
NUMBER OF YEARS COMPLETED
MAJOR & DEGREE
High School
College
Bus. or Trade School
Professional School
HAVE YOU EVER BEEN CONVICTED OF A CRIME? _ No _ Yes
If yes, explain number of conviction(s), nature of offense(s) leading to conviction(s), how recently such offense(s) was/were committed, sentence(s) imposed, and type(s) of rehabilitation.
PLEASE PRINT ALL INFORMATION REQUESTED
EXCEPT SIGNATURE APPLICATION FOR EMPLOYMENT
DO YOU HAVE A DRIVER'S LICENSE? Yes
What is your means of transportation to work?
No
Driver's license number State of issue Expiration date
Have you had any accidents during the past three years? Have you had any moving violations dunng the past three years?
Operator Commercial (CDL) Chauffeur
How many? How Many?
OFFICE ONLY
Typing
Personal Computer
Yes No
Yes No
WPM
PC Mac
_ Y e s 10-key No
Other Skills
Word Processing
Yes No WPM
Please list two references other than relatives or previous employers.
Name Name
Position
Company _
Address
Telephone
Position _
Company
Address _
Telephone
An application form sometimes makes it difficult for an individual to adequately summarize a complete background. Use the space below to summarize any additional information necessary to describe your full qualifications for the specific position for which you are applying.
PLEASE PRINT ALL INFORMATION REQUESTED
EXCEPT SIGNATURE
APPLICATION FOR EMPLOYMENT
MILITARY
HAVE YOU EVER BEEN IN THE ARMED FORCES? Yes
ARE YOU NOW A MEMBER OF THE NATIONAL GUARD? __Yes _ N o
Specialty Date Entered Disctiarge Date
Work Please list your work experience for the past five years beginning with your most recent job held. Experience If you were self-employed, give firm name. Attach additional sheets if necessary.
Name of employer Name of last Employment dates Pay or salary Address supervisor City, State, Zip Code From Start Phone number
From Start
To Final
Your last job title
Reason for leaving (be specific)
List the jobs you held, duties performed, skills used or learned, advancements or promotions while you worked at this company.
Name of employer Address City, State, Zip Code Phone number
Name of last supervisor
Employment dates Pay or salary
From
To
Start
Final
Your Last Job Title
Reason for leaving (be specific)
List the jobs you held, duties performed, skills used or learned, advancements or promotions while you worked at this company.
PLEASE PRINT ALL INFORMATION REQUESTED
EXCEPT SIGNATURE
APPLICATION FOR EMPLOYMENT
Work Please list your work experience for the past five years beginning with your most recent job held, experience If you were self-employed, give firm name. Attach additional sheets if necessary.
Name of employer Name of last Employment dates Pay or salary Address supervisor City, State, Zip Code From Start Phone number
From
To Final
Your last job title
Reason for leaving (be specific)
List the jobs you held, duties performed, skills used or learned, advancements or promotions while you worked at this company.
Name of employer Address City, State, Zip Code Phone number
Name of last supervisor
Employment dates Pay or salary Name of employer Address City, State, Zip Code Phone number From
To
Start
Final
Name of employer Address City, State, Zip Code Phone number
Your last job title
Reason for leaving (be specific)
List the jobs you held, duties performed, skills used or leamed, advancements or promotions while you worked at this company.
May we contact your present employer? Yes No
Did you complete this application yourself Yes No
If not, who did?
^ ^ L 0 U 1 S i A Ni A
0-.-. C O M M I S S I O N
1 0 0 1 N o r t h 23"^ S t ree t P o s t O f f i ce Box 4 4 1 8 7 B a t o n R o u g e , LA 7 0 8 0 4 - 4 1 8 7
B o b b y J i n d a l , G o v e r n o r C u r t E y s i n k . E x e c u t i v e D i rec to r
Office of Workers ' Compensat ion Admin is t ra t ion Second Injury Board
LA OWCA Second Injury Board Knowledge Questionnaire
The following questionnaire should only be comp le ted by indiv iduals that have been hired for employment. Your employer may ask t ha t y o u comp le te th is quest ionna i re fo l l ow ing you r in i t ia l h i re and per iodical ly thereaf ter .
The quest ionnai re may be used in the es tab l ishment of pr ior knowledge for the purpose of ob ta in ing Second Injury Fund rel ief f r o m the Second Injury Board. The Second Injury Board may re imburse your emp loyer for workers ' compensat ion c la ims tha t mee t cer ta in cr i ter ia should you become in jured on the job . This re imbursement in no way af fects the benef i ts o w e d to you by your emp loyer or the i r insurance company under the Louisiana Worke rs ' Compensat ion Act, La. R.S. 23 :1021-1361 .
WARNING
FAILURE TO ANSWER TRUTHFULLY AND/OR CORRECTLY TO ANY OF THE QUESTIONS ON THIS FORM MAY RESULT IN A FORFEITURE OF YOUR WORKERS COMPENSATION BENEFITS UNDER LA R.S. 23:1208.1.
Employer:
Employee Name:
Date of Birth ( m m / d d / y y y y ) : Ma le : • Female: •
Soc. Sec. # (last 4 digi ts on ly ) :
Home Address:
Telephone Number : ( )
Employee Signature:
Employer Witness:
Date:
Date;
PAGE OF
SIB FORM D 12/10 WWW. la works, net
[ Equal Opportunity Empioyer/Program \y aids and services are available upon tequesi to individuals wif i i disabil it ies • TDD# 600-259-5154
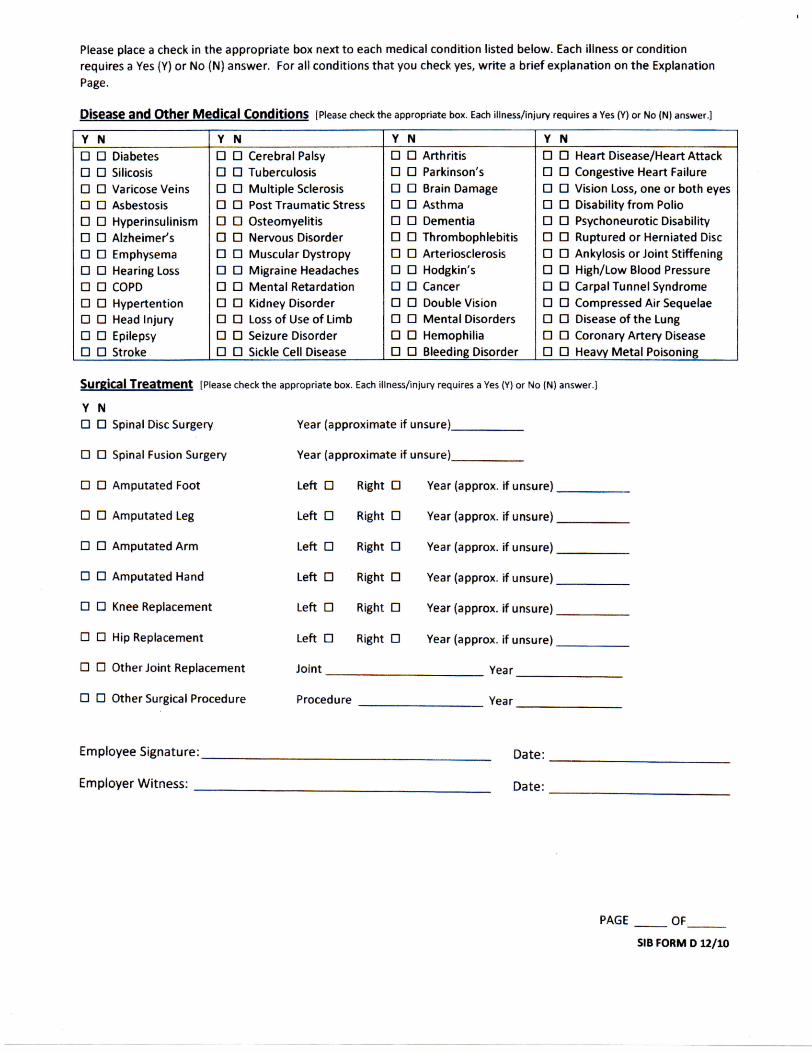
Please place a check in the appropriate box next to each medical condition listed below. Each illness or condition requires a Yes (Y) or No (N) answer. For ail conditions that you check yes, wri te a brief explanation on the Explanation Page.
Disease and Other Medical Conditions [Please check the appropriate box. Each illness/injury requires a Yes (Y) or No (N) answer.]
Y N Y N Y N Y N • • Diabetes • • Silicosis • • Varicose Veins • • Asbestosis • • Hyperinsulinism n n Alzheimer's • • Emphysema • • Hearing Loss • • COPD • • Hypertention • • Head Injury • • Epilepsy • • Stroke
• • Cerebral Palsy • • Tuberculosis • • Mult iple Sclerosis • • Post Traumatic Stress • • Osteomyelitis • • Nervous Disorder • • Muscular Dystropy • • Migraine Headaches • • Mental Retardation • • Kidney Disorder • • Loss of Use of Limb • • Seizure Disorder • • Sickle Cell Disease
• • Heart Disease/Heart Attack • • Congestive Heart Failure • • Vision Loss, one or both eyes • • Disability f rom Polio • • Psychoneurotic Disability • • Ruptured or Herniated Disc • • Ankylosis or Joint Stiffening • • High/Low Blood Pressure • • Carpal Tunnel Syndrome • • Compressed Air Sequelae • • Disease of the Lung • • Coronary Artery Disease • • Heavy Metal Poisoning
SurRJCal T r e a t m e n t [Please check the appropriate box. Each iiiness/injury requires a Yes (Y) or No (N) answer,]
Y N • • Spinal Disc Surgery Year {approximate if unsure)
• • Spinal Fusion Surgery Year (approximate if unsure)
• • Amputated Foot Left • Right • Year (approx. if unsure)
• • Amputated Leg Left • Right • Year (approx. if unsure)
• • Amputated Arm Left • Right • Year (approx. if unsure)
• • Amputated Hand Left • Right • Year (approx. if unsure)
• • Knee Replacement Left • Right • Year (approx, if unsure)
• • Hip Replacement Left • Right • Year (approx. if unsure)
• • Other Joint Replacement Joint Year
• • Other Surgical Procedure Procedure Year
Employee Signature: Date:
Employer Wi tness: ^ Date:
PAGE OF
SIB FORM D 12/10
EXPLANATION PAGE
Please use the space below to explain the illnesses and/or conditions that you checked a Yes (Y) or any other medical conditions that may not be listed on this form. Ask your employer for additional copies of this page if needed.
CONDITION; Year Diagnosed (approx):
Are you still treating for this condition? Yes • No •
Are you taking medication for this condition? Yes • No •
Do you have any permanent restrictions for this condition? Yes • No •
Brief Explanation:
CONDITION; Year Diagnosed (approx):.
Are you still treating for this condition? Yes • No •
Are you taking medication for this condition? Yes • No •
Do you have any permanent restrictions for this condition? Yes • No •
Brief Explanation;
CONDITION: Year Diagnosed (approx);
Are you still treating for this condition? Yes • No •
Are you taking medication for this condition? Yes • No •
Do you have any permanent restrictions for this condition? Yes • No •
Brief Explanation:
CONDITION: Year Diagnosed (approx):
Are you still treating for this condition? Yes • No •
Are you taking medication for this condition? Yes • No •
Do you have any permanent restrictions for this condition? Yes • No •
Brief Explanation:
Employee Signature: Date:
Employer Wi tness: Date;
PAGE OF
SIB FORM D 12/10
Please answer the fo l l ow ing quest ions .
1. Has any doctor ever res t r ic ted your act iv i t ies? Yes • No • If "Yes/ ' please list t he res t r ic t ions: Were the restr ic t ions: Pernnanent Tennporary Are you cur rent ly rest r ic ted? Yes • No • W h a t is the nnedical cond i t i on for wh i ch you are restr ic ted?
2. Are you present ly t rea t ing w i t h a doc tor , ch i roprac tor , psychiatr ist , psychologist or o the r heal th-care provider? Yes • No •
Please list the medical cond i t i on be ing t r e a t e d :
Doctor 's Name: _ S p e c i a l t y : .
Doctor 's Address:
3. If you are present ly tak ing prescr ip t ion med ica t ion o ther than those l isted on the Explanat ion Page, please comple te the requested i n fo rma t i on be low.
Med ica t ion : Prescribing Doctor :
Med ica t ion : Prescribing Doctor :
4. Have you ever had an on the job accident? Yes • No • if you answered "YES," please prov ide the da te for each in jury and the na ture of the in jury:
How long were you on compensa t ion?
Name of Employer :
5. Has a doctor r e c o m m e n d e d a surgical p rocedure , wh ich has not been c o m p l e t e d pr ior t o th is date, including but not l im i ted t o knee, hip or shou lder rep lacement? Yes • No • If you answered YES, please prov ide :
Recommended surgery:
Approx imate date of r e c o m m e n d a t i o n :
Doctor 's Name: Specialty:
Doctor 's Address:
Employee Signature: Date:
Employer Wi tness: Date:
PAGE OF
SIB FORM D 12/10
WARNING
FAILURE TO ANSWER TRUTHFULLY AND/OR CORRECTLY TO ANY OF THE QUESTIONS ON THIS FORM MAY RESULT IN A FORFEITURE OF YOUR WORKERS COMPENSATION BENEFITS UNDER LA R.S. 23:1208.1.
I have c o m p l e t e d th is f o r m hones t l y and t o t h e best o f m y k n o w l e d g e . I u n d e r s t a n d t h a t p rov i d i ng false I n f o r m a t i o n o r o m i t t i n g p e r t i n e n t i n f o r m a t i o n cou ld resu l t i n loss o f m y w o r k e r s c o m p e n s a t i o n benef i t s shou ld I become i n j u red o n t h e j o b .
Employee Signature: . Date:
Employee Pr in ted:
I a m an au tho r i zed rep resen ta t i ve o f t he e m p l o y e r des igna ted t o o b t a i n and r e v i e w t h e i n f o r m a t i o n p rov ided by t he e m p l o y e e o n th is ques t i onna i r e , i have c o n f i r m e d t h a t t h e e m p l o y e e unders tands t he consequences associated w i t h p r o v i d i n g false i n f o r m a t i o n o r o m i t t i n g p e r t i n e n t I n f o r m a t i o n . I have c o n f i r m e d t h a t t h e e m p l o y e e is ab le t o read and unde rs tand t h e i n f o r m a t i o n p r o v i d e d on th is ques t i onna i re or I have persona l ly read t h e q u e s t i o n n a i r e t o t h e e m p l o y e e . I have p r o v i d e d t h e e m p l o y e e w i t h as m a n y copies o f t h e Exp lana t ion Page as n e e d e d . I have c o n f i r m e d t h e n u m b e r o f and labe led t h e pages o f th is ques t ionna i re .
Employer Wi tness: Date:
Employer Wi tness Pr in ted :
Ti t le:
PAGE OF
SIB FORM D 12/10
Form W-4 (2015) P u r p o s e . C o m p l e t e F o r m W - 4 so that you r e m p l o y e r c a n w i t h h o l d the co r rec t federa l i n c o m e tax f r o m you r pay . Cons ide r c o m p l e t i n g a n e w F o r m W - 4 e a c h year a n d w h e n you r pe rsona l or f inanc ia l s i tua t ion c h a n g e s .
E x e m p t i o n f r o m w i t h h o l d i n g . If y o u are e x e m p t , c o m p l e t e o n l y l ines 1 , 2 , 3 , 4, a n d 7 a n d s ign t he f o r m t o va l i da te it. Your e x e m p t i o n for 2 0 1 5 exp i res February 16, 2 0 1 6 , See Pub . 505 , Tax W i t h h o l d i n g a n d E s t i m a t e d Tax,
N o t e . If ano the r pe rson can c l a im y o u as a d e p e n d e n t o n h is or her tax re turn , y o u c a n n o t c la im e x e m p t i o n f r o m w i t h h o l d i n g if your i n c o m e e x c e e d s $ 1 , 0 5 0 a n d inc ludes m o r e t han $ 3 5 0 of u n e a r n e d i n c o m e (for e x a m p l e , interest a n d d i v idends ) .
Exceptions. A n e m p l o y e e m a y be ab le to c l a im e x e m p t i o n f r o m w i t h h o l d i n g e v e n if t he e m p l o y e e is a d e p e n d e n t , if the e m p l o y e e :
• Is a g e 65 or o lder ,
• Is b l i nd , or
• Wil l c l a im a d j u s t m e n t s to i n c o m e ; tax c red i t s ; or i t em ized d e d u c t i o n s , o n his o r her tax re tu rn .
T h e e x c e p t i o n s d o not a p p l y t o s u p p l e m e n t a l w a g e s g r e a t e r t h a n $ 1 , 0 0 0 , 0 0 0 ,
B a s i c i n s t r u c t i o n s . If y o u a re no t e x e m p t , c o m p l e t e t he P e r s o n a l A l l o w a n c e s W o r k s h e e t b e l o w . T h e w o r k s h e e t s o n p a g e 2 fu r t he r a d j u s t y o u r w i t h h o l d i n g a l l o w a n c e s b a s e d o n i t e m i z e d d e d u c t i o n s , c e r t a i n c r e d i t s , a d j u s t m e n t s t o i n c o m e , o r t w o - e a r n e r s / m u l t i p l e j o b s s i t u a t i o n s .
C o m p l e t e all w o r k s h e e t s t ha t a p p l y . H o w e v e r , y o u m a y c l a i m f e w e r (or zero) a l l o w a n c e s . Fo r regu la r w a g e s , w i t h h o l d i n g m u s t b e b a s e d o n a l l o w a n c e s y o u c l a i m e d a n d m a y no t b e a f lat a m o u n t o r p e r c e n t a g e of w a g e s .
H e a d o f h o u s e h o l d . Gene ra l l y , y o u c a n c l a i m h e a d of h o u s e h o l d f i l ing s t a tus o n y o u r t ax re tu rn on l y if y o u a re u n m a r r i e d a n d pay m o r e t h a n 5 0 % of t h e c o s t s of k e e p i n g u p a h o m e fo r you rse l f a n d y o u r d e p e n d e n t ( s ) o r o t h e r q u a l i f y i n g i nd i v i dua l s . S e e P u b , 5 0 1 , E x e m p t i o n s , S t a n d a r d D e d u c t i o n , a n d Fi l ing I n f o r m a t i o n , for i n f o r m a t i o n .
Tax credi ts . You can take projected tax credits into account in figuring your allowable number of withholding allowances. Credits tor child or dependent care expenses and the child tax credit may be claimed using the Personal A l lowances Workshee t below. See Pub, 505 lor information on converting your other credits into withholding allowances.
N o n w a g e i n c o m e . If y o u have a large a m o u n t of n o n w a g e i n c o m e , s u c h as interest or d i v i dends , cons ide r m a k i n g es t ima ted tax p a y m e n t s us ing F o r m 1040 -ES , E s t i m a t e d Tax for Ind iv idua ls , O the rw ise , y o u m a y o w e add i t i ona l tax. If y o u have pens ion or annu i t y i n c o m e , see P u b , 5 0 5 t o f ind ou t if y o u shou ld ad jus t you r w i t h h o l d i n g o n F o r m W - 4 or W - 4 P ,
T w o e a r n e r s o r m u l t i p l e j o b s . If y o u h a v e a w o r k i n g s p o u s e o r m o r e t h a n o n e j o b , f i gu re t h e t o t a l n u m b e r of a l l o w a n c e s y o u are e n t i t l e d t o c l a i m o n al l j o b s u s i n g w o r k s h e e t s f r o m on l y o n e F o r m W - 4 , Y o u r w i t h h o l d i n g usua l l y wi l l be m o s t a c c u r a t e w h e n all a l l o w a n c e s a re c l a i m e d o n t h e F o r m W - 4 for t h e h i g h e s t p a y i n g j o b a n d zero a l l o w a n c e s a re c l a i m e d o n t h e o t h e r s . S e e P u b , 5 0 5 fo r de ta i l s .
N o n r e s i d e n t a l i e n . If y o u a re a n o n r e s i d e n t a l i en , see N o t i c e 1 3 9 2 , S u p p l e m e n t a l F o r m W - 4 I n s t r u c t i o n s fo r N o n r e s i d e n t A l i ens , b e f o r e c o m p l e t i n g th is f o r m .
C h e c k y o u r w i t h h o l d i n g . A f t e r y o u r F o r m W - 4 t a k e s e f fec t , u s e P u b , 5 0 5 t o see h o w t h e a m o u n t y o u a re h a v i n g w i t h h e l d c o m p a r e s t o y o u r p r o j e c t e d to ta l t ax fo r 2 0 1 5 , S e e P u b , 5 0 5 , e s p e c i a l l y if y o u r e a r n i n g s e x c e e d $ 1 3 0 , 0 0 0 (Single) o r $ 1 8 0 , 0 0 0 (Mar r ied ) ,
Future deve lopments . Information about any future developments affecting Form W-4 (such as legislation enacted after we release it) will be posted at www.irs.govM.
Persona l A l l o w a n c e s W o r k s h e e t (Keep for your records.)
Enter " 1 " if:
Enter " 1 " for yourself if no one else can claim you as a dependent A • You are single and have only one job; or • You are married, have only one job, and your spouse does not work; or . . . B
^ • Your wages from a second job or your spouse's wages (or the total of both) are $1,500 or less. Enter " 1 " for your spouse. But, you may choose to enter "-0-" if you are married and have either a working spouse or more than one job. (Entering "-0-" may help you avoid having too little tax withheld.) C Enter number of dependents (other than your spouse or yourself) you will claim on your tax return D Enter " 1 " if you will file as head of household on your tax return (see conditions under Head of household above) . . Enter " 1 " if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit . . (Note. Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.) Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information. • If your total income will be less than $65,000 ($100,000 if married), enter "2" for each eligible child; then less " 1 " if you have two to four eligible children or less "2" if you have five or more eligible children. • If your total income will be between $65,000 and $84,000 ($100,000 and $119,000 if married), enter " 1 " for each eligible child . . . Add lines A through G and enter total here. (Note. This may be different from the number of exemptions you claim on your tax return.) •
/ " I f you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions For accuracy, and Adjustments Worksheet on page 2 . complete all • if you are single and have more than one job or are married and you and your spouse both work and the combined worksheets earnings from all jobs exceed $50,000 ($20,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 to that apply. avoid having too little tax withheld.
• If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below.
Separate here and give Form W-4 to your employer. Keep the top part for your records. -
Employee's Withholding Allowance Certificate W-4 F o r m
Department of the Treasury Internal Revenue Service
O M B N o . 1 5 4 5 - 0 0 7 4
• W h e t h e r y o u a r e e n t i t l e d t o c l a i m a c e r t a i n n u m b e r o f a l l o w a n c e s o r e x e m p t i o n f r o m w i t h h o l d i n g i s s u b j e c t t o r e v i e w b y t h e I R S . Y o u r e m p l o y e r m a y b e r e q u i r e d t o s e n d a c o p y o f t h i s f o r m t o t h e I R S . :@15
Y o u r f i rs t n a m e a n d m i d d l e in i t ia l Las t n a m e 2 Y o u r s o c i a l s e c u r i t y n u m b e r
H o m e a d d r e s s ( n u m b e r a n d s t ree t o r ru ra l r ou te ) 3 • S i n g l e M a r r i e d M a r r i e d , b u t w i t h h o l d at h ighe r S i n g l e ra te .
Note. If married, but legally separated, or spouse is a nonresident alien, check the "Single" box.
C i ty or t o w n , s t a te , a n d Z I P c o d e 4 If y o u r l a s t n a m e d i f f e r s f r o m t h a t s h o w n o n y o u r s o c i a l s e c u r i t y c a r d ,
c h e c k h e r e . Y o u m u s t c a l l 1 - 8 0 0 - 7 7 2 - 1 2 1 3 f o r a r e p l a c e m e n t c a r d . • Q
5 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2) 6 Additional amount, if any, you want withheld from each paycheck 7 I claim exemption from withholding for 2015, and I certify that I meet both of the following conditions for exemption.
• Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and • This year I expect a refund of all federal income tax withheld because I expect to have no tax liability. If you meet both conditions, write "Exempt" here • 7
Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete. Employee's signature (This form is not valid unless you sign it.) • Date^
8 E m p l o y e r ' s n a m e a n d a d d r e s s ( E m p l o y e r : C o m p l e t e l ines 8 a n d 10 on l y if s e n d i n g t o t h e IRS.) 9 Office code (optional) 10 Emp loye r ident i f i ca t ion n u m b e r (EIN)
For Privacy Act and Paperwork Reduction Act Notice, see page 2. Gat , N o , 1 0 2 2 0 Q F o r m W-4 (2015)