PERCUTANEOUS RUPTURE OF LUMBAR SYNOVIAL CYSTS: WHEN WE DO IT, AND HOW WE DO IT ? AUTHORS: Y Kumar, K Hooda, D Hayashi, N Parikh, S Sharma, M Meszaros Yale New Haven Health System at Bridgeport Hospital Bridgeport, CT USA ASNR 2015 Abstract No: 1901
Transcript
PERCUTANEOUS RUPTURE OF LUMBAR SYNOVIAL CYSTS: WHEN WE DO IT, AND HOW WE DO IT ?
AUTHORS:Y Kumar, K Hooda, D Hayashi, N Parikh, S Sharma, M Meszaros
Yale New Haven Health System at Bridgeport HospitalBridgeport, CT USA
ASNR 2015 Abstract No: 1901
All authors have nothing to disclose.
PURPOSE
1. To review the indications of percutaneous rupture of lumbar synovial cysts.
2. To describe the techniques and limitations of percutaneous rupture of lumbar synovial cysts.
3. To discuss outcomes of percutaneous rupture of lumbar synovial cysts.
INTRODUCTION
Lumbar synovial cysts results from protrusions of synovial sheaths through a defect in the degenerated facet joints and extrude into the spinal canal.
These can cause radicular symptoms with mass effect on the nerve roots in the spinal canal.
As the cysts characteristically project anteromedially from the facet joint, the radiculopathy commonly involves the traversing nerve root.
Uncommonly, the cyst can extend anterolaterally relative to the facet causing compression of the exiting nerve within the neural foramen.
Alternatively, they can also lead to spinal canal stenosis due to large size.
Rarely, acute hemorrhage within a cyst may also result in a rapid exacerbation of symptoms, with severe cases resulting in cauda equina syndrome.
ROLE OF IMAGING
Although synovial cysts can be visualized with CT, MRI is better in further characterizing them.
Important characteristics to look for in MRI are: hypertrophic facet joint cyst location, whether epidural or
posterolateral T2 hypointense rim signal intensity of internal contents.
CT is valuable in detecting the wall calcifications which is very important in predicting the success of percutaneous rupture.
Characteristic MR appearance of Synovial Cyst in Lumbar Spine
DIFFENTIAL DIAGNOSIS
Usually diagnosis of synovial cyst is not a diagnostic dilemma due to its MRI characteristics and the neuroanatomic location. However, differential diagnosis includes: arachnoid cysts perineural (Tarlov) cysts Schwannomas migrated herniated disk fragments
Highly characteristic peripheral low signal intensity rim caused by the synovial lining of synovial cysts on T2-weighted is not an imaging feature of other intraspinal cysts such as arachnoid cysts, ganglia, or perineural cysts.
TREATMENT OPTIONS
Conservative Percutaneous aspiration Percutaneous steroid and local
anesthetic injections into the cysts Percutaneous rupture Surgical Resection
Percutaneous Rupture of Lumbar Synovial Cysts
Image guided synovial cyst rupture has been shown to be effective in pain relief and avoiding surgical treatment.
It relieves the mass effect over the nerve roots thus relieving the radicular pain.
PROCEDURE
Informed consent is obtained after explaining the risk and benefits of procedure.
Patient is places prone on the CT table and site is localized with limited CT.
The skin is prepped and draped in sterile fashion.
1% lidocaine is used for local anesthesia.
A 22-gauge needle is advanced to the facet joint near the synovial cyst.
Communication of the cyst with facet joint is verified with diluted contrast.
Subsequently, diluted contrast is pushed into the facet joint with 3 ml syringe with pressure until contrast is seen in the epidural space adjacent to synovial cyst suggesting rupture.
After cyst rupture, a mixture of steroid and local anesthetic is injected.
Case No. 1
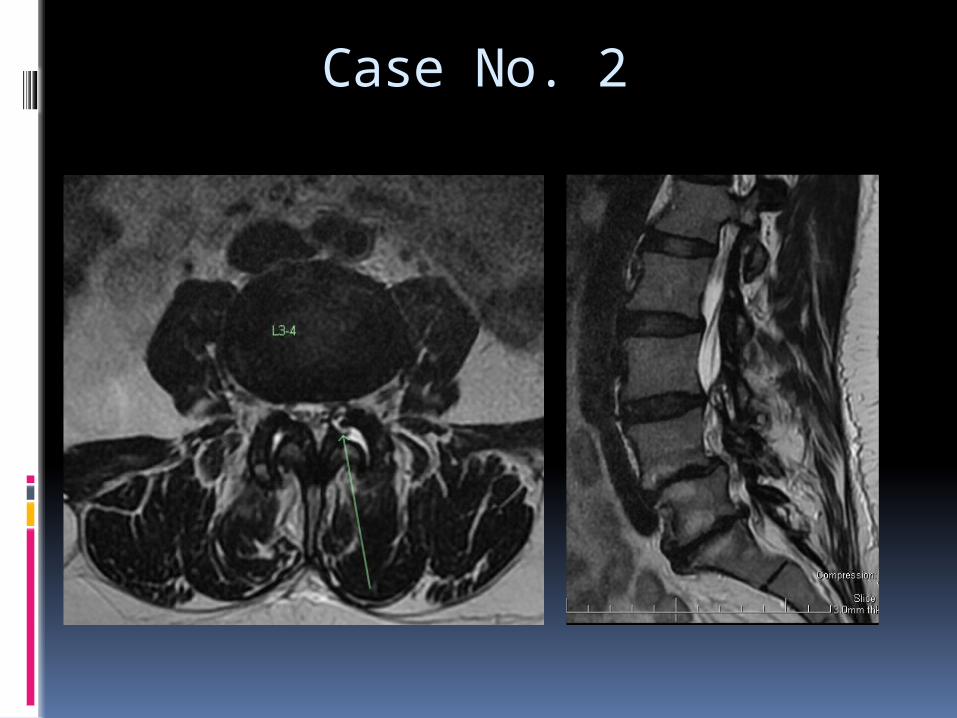
Case No. 2
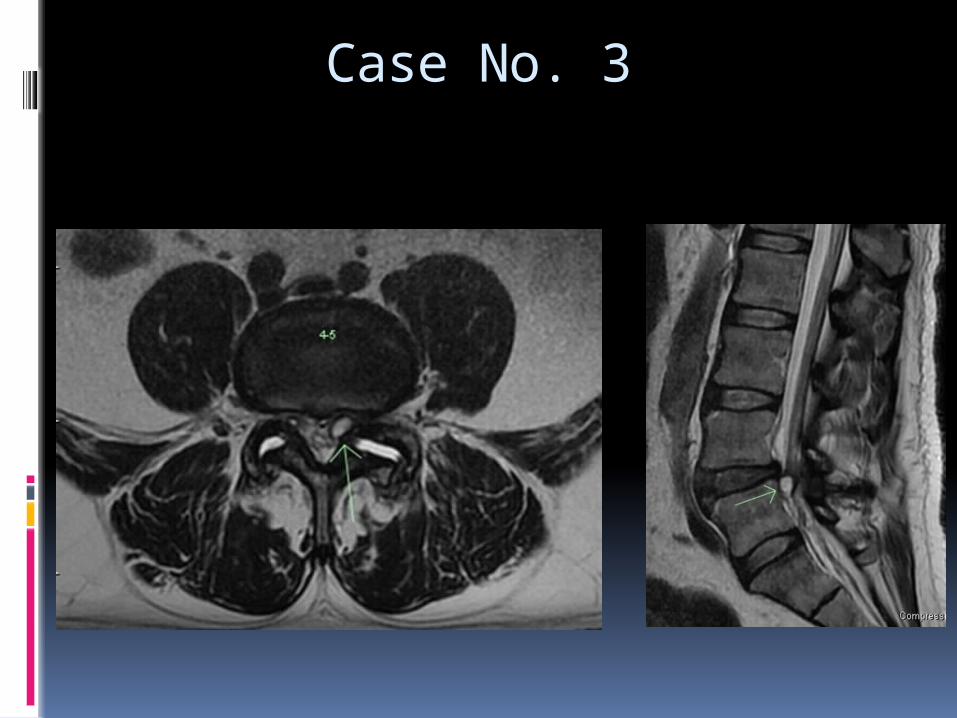
Case No. 3
Factors Predicting Success of Percutaneous rupture of Synovial Cyst
Synovial cyst wall calcification decreases the success rate of percutaneous rupture of the lumbar synovial cyst.
Presence of T2 hyper intense signal in the cyst is a favorable MR finding.
SUMMARY
Lumbar facet joint cysts are increasingly recognized as a cause of low back pain.
Therapeutic interventions range from epidural steroid injections, facet joint injections to surgical resection.
CT guided lumbar facet joint cyst rupture/decompression appears to be a viable treatment option.
REFERENCES Foley BS. Percutaneous Rupture of a Lumbar Synovial Facet
Cyst. Am J Phys Med Rehab. 2009;88(12): 1046
Yim D, Piduru SM, et al. Lumbar facet joint cyst intervention: A minimally invasive treatment option we can offer our spine patients for a common cause of radiculopathy. J Vasc Interv Radiol. 2013;24(4) Suppl:S177
Julia F. Martha, BS et al. Outcome of percutaneous rupture of lumbar synovial cysts: a case series of 101 patients. Spine J 2009;9(11):899-904.
Lumbar facet joint synovial cysts: does T2 signal intensity predict outcomes after percutaneous rupture? AJNR 2013 Aug;34(8):1661-4