21
Autism Spectrum Disorder and Epilepsy Gregory Neal Barnes MD/PhD Associate Director Pediatric Epilepsy Monitoring Unit Division of Pediatric Neurology
Autism Spectrum Disorder
and EpilepsyGregory Neal Barnes MD/PhD
Associate Director
Pediatric Epilepsy Monitoring Unit
Division of Pediatric Neurology
Overview
• Autism Spectrum Disorders (ASD)
• Epilepsy and ASD
• Treatment of Epilepsy in ASD
• Future Clinical Trials
Autism Spectrum Disorders
(ASD)
• Impaired social skills
• Impaired language skills
• Thought processing disorder

DSM IV Defined Diseases
• Autistic Disorder
• Pervasive Developmental Delay
• Asperger syndrome
• Childhood disintegrative disorder
• Rett syndrome

Causes of ASD

Increased Concentrations of Inhibitory Cells in ASD
Temporal Lobe

Increased Numbers of Inhibitory cells in a Mouse Model of
Autism and Epilepsy (PTEN Knockout Mouse)
Parv+ Cells
0
1000
2000
3000
Parv
+ N
eu
ron
s/m
m3
* *
CA1 CA3 DG SS PF BG
Neuropeptide Y+ Cells
0
500
1000
1500 *
CA1 CA3
NP
Y+
Neu
ron
s/m
m3
DG SS PF BG
DLX1-Cre PTEN Cell Counts
What Types of Epilepsy Occur in
ASD?
• Partial complex and generalized
epilepsies (all studies are
heterogeneous)
• In general most EEG studies suggest
epileptiform activity is prevalent in
children with ASD/epilepsy
compared to ASD alone
Risk of Epilepsy in ASD
Increases with:
• More cognitive challenges (such as
kids with mental retardation)
• Prenatal insults
• Fragile X syndrome
• Tuberous sclerosis syndrome
• Chromosomal syndromes
• Angelman’s syndrome
Risk of Epilepsy in ASD
Increases with:
• motor dysfunction (cerebral palsy)
• gender (more females, Rett
syndrome)
• Receptive language difficulties
(aphasia)

Risk of Epilepsy in ASD
Increases with:
• ? EEG findings
• Family history of epilepsy

Disorders More Common to
Occur in Kids with ASD and
Epilepsy
• Increased hyperactivity and
inattentiveness (ADHD)
• Communication disorders
• More impaired social interactions
• More impaired reciprocal
communications
Disorders More Common to
Occur in Kids with ASD and
Epilepsy
• More significant thought processing
disorder
• Obsessive Compulsive Disorder

Testing for Children with ASD
and Suspected Epilepsy?
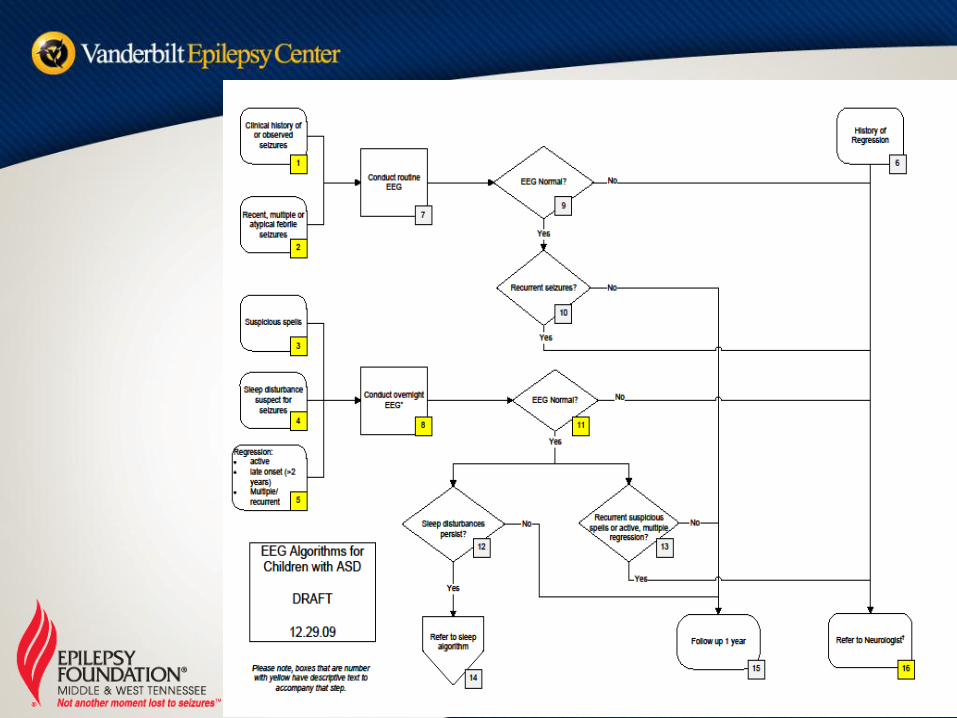
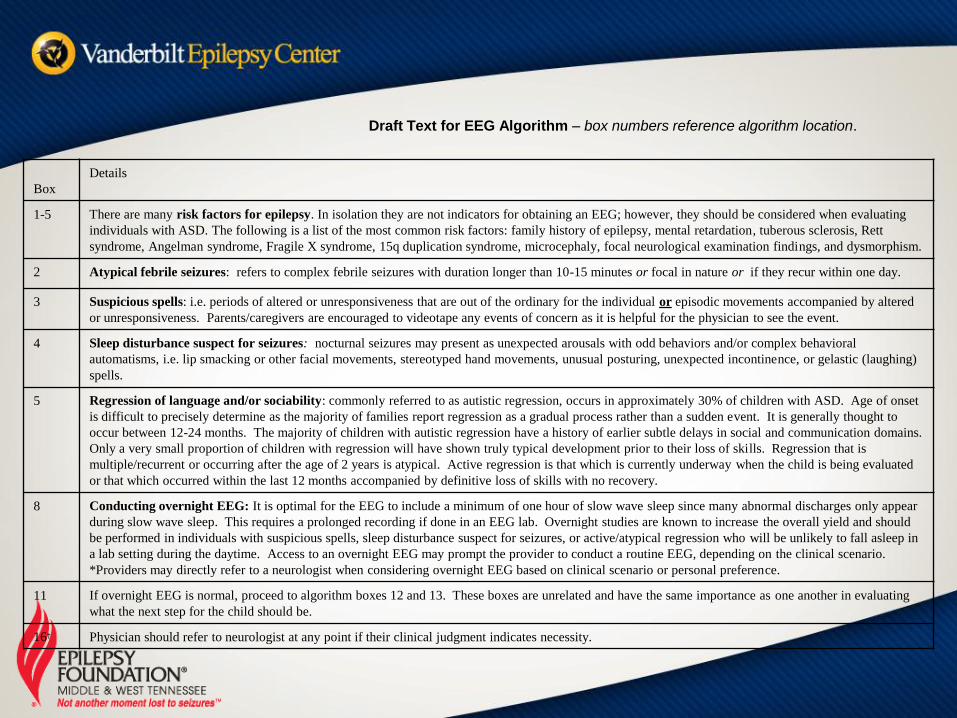
Draft Text for EEG Algorithm – box numbers reference algorithm location.
Box
Details
1-5 There are many risk factors for epilepsy. In isolation they are not indicators for obtaining an EEG; however, they should be considered when evaluating
individuals with ASD. The following is a list of the most common risk factors: family history of epilepsy, mental retardation, tuberous sclerosis, Rett
syndrome, Angelman syndrome, Fragile X syndrome, 15q duplication syndrome, microcephaly, focal neurological examination findings, and dysmorphism.
2 Atypical febrile seizures: refers to complex febrile seizures with duration longer than 10-15 minutes or focal in nature or if they recur within one day.
3 Suspicious spells: i.e. periods of altered or unresponsiveness that are out of the ordinary for the individual or episodic movements accompanied by altered
or unresponsiveness. Parents/caregivers are encouraged to videotape any events of concern as it is helpful for the physician to see the event.
4 Sleep disturbance suspect for seizures: nocturnal seizures may present as unexpected arousals with odd behaviors and/or complex behavioral
automatisms, i.e. lip smacking or other facial movements, stereotyped hand movements, unusual posturing, unexpected incontinence, or gelastic (laughing)
spells.
5 Regression of language and/or sociability: commonly referred to as autistic regression, occurs in approximately 30% of children with ASD. Age of onset
is difficult to precisely determine as the majority of families report regression as a gradual process rather than a sudden event. It is generally thought to
occur between 12-24 months. The majority of children with autistic regression have a history of earlier subtle delays in social and communication domains.
Only a very small proportion of children with regression will have shown truly typical development prior to their loss of skills. Regression that is
multiple/recurrent or occurring after the age of 2 years is atypical. Active regression is that which is currently underway when the child is being evaluated
or that which occurred within the last 12 months accompanied by definitive loss of skills with no recovery.
8 Conducting overnight EEG: It is optimal for the EEG to include a minimum of one hour of slow wave sleep since many abnormal discharges only appear
during slow wave sleep. This requires a prolonged recording if done in an EEG lab. Overnight studies are known to increase the overall yield and should
be performed in individuals with suspicious spells, sleep disturbance suspect for seizures, or active/atypical regression who will be unlikely to fall asleep in
a lab setting during the daytime. Access to an overnight EEG may prompt the provider to conduct a routine EEG, depending on the clinical scenario.
*Providers may directly refer to a neurologist when considering overnight EEG based on clinical scenario or personal preference.
11 If overnight EEG is normal, proceed to algorithm boxes 12 and 13. These boxes are unrelated and have the same importance as one another in evaluating
what the next step for the child should be.
16† Physician should refer to neurologist at any point if their clinical judgment indicates necessity.
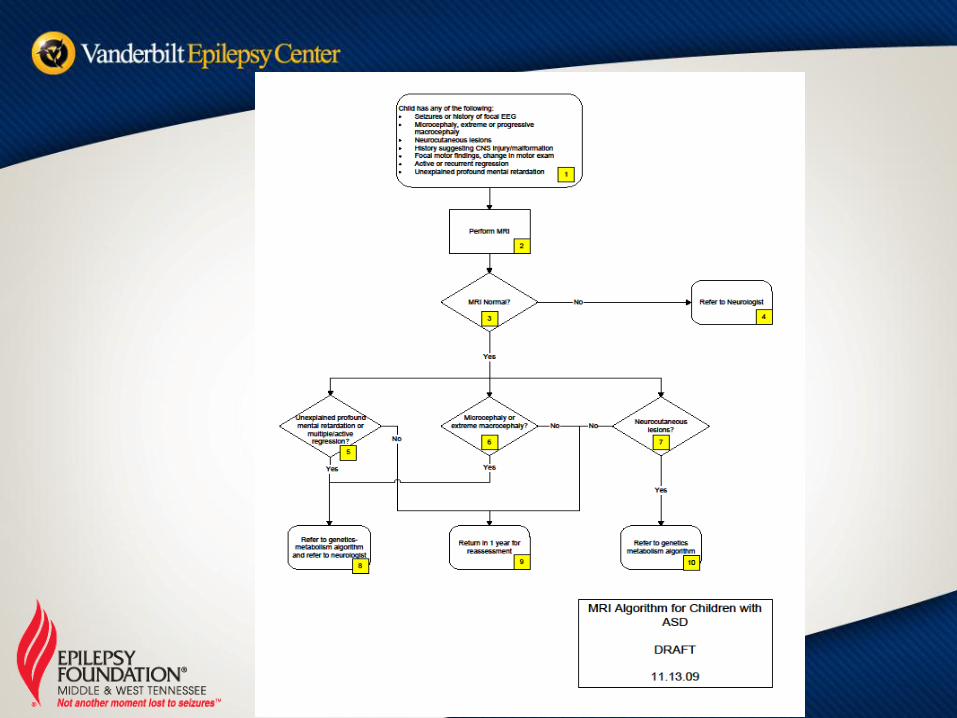
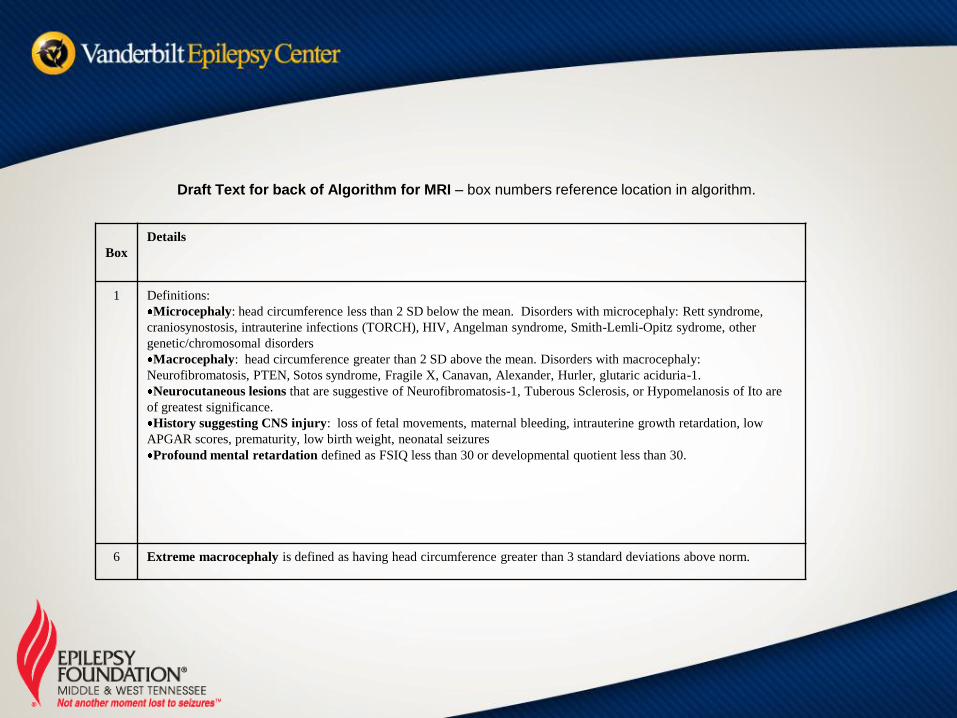
Draft Text for back of Algorithm for MRI – box numbers reference location in algorithm.
Box
Details
1 Definitions:
Microcephaly: head circumference less than 2 SD below the mean. Disorders with microcephaly: Rett syndrome,
craniosynostosis, intrauterine infections (TORCH), HIV, Angelman syndrome, Smith-Lemli-Opitz sydrome, other
genetic/chromosomal disorders
Macrocephaly: head circumference greater than 2 SD above the mean. Disorders with macrocephaly:
Neurofibromatosis, PTEN, Sotos syndrome, Fragile X, Canavan, Alexander, Hurler, glutaric aciduria-1.
Neurocutaneous lesions that are suggestive of Neurofibromatosis-1, Tuberous Sclerosis, or Hypomelanosis of Ito are
of greatest significance.
History suggesting CNS injury: loss of fetal movements, maternal bleeding, intrauterine growth retardation, low
APGAR scores, prematurity, low birth weight, neonatal seizures
Profound mental retardation defined as FSIQ less than 30 or developmental quotient less than 30.
6 Extreme macrocephaly is defined as having head circumference greater than 3 standard deviations above norm.
Treatment of Children with ASD
and Epilepsy
• No data in the literature
• Partial Epilepsies- Trileptal,
Depakote, Lamictal, Zonegran
• Generalized Epilepsies- Depakote,
Lamictal, Zonegran
Treatment of Children with ASD
and Epilepsy
• ADHD
• Strattera, Stimulant medications
(Ritalin, Adderal, etc)
• OCD
• Risperadal, Abilify
• Aggression
• Neuroleptics, Depakote, Lamictal
Treatment of Children with ASD
and Epilepsy
• Neuropsychological testing where
appropriate
• Identified specific learning
disabilities
• Classroom modifications
• Special Education Services

















