J. Clin. Endocrinol. Metab. 2008 93:363-371 originally published online Nov 20, 2007; , doi: 10.1210/jc.2007-2134
Christophe E. M. De Block, Ivo H. De Leeuw and Luc F. Van Gaal
Autoimmune Gastritis in Type 1 Diabetes: A Clinically Oriented Review
Society please go to: http://jcem.endojournals.org//subscriptions/ or any of the other journals published by The EndocrineJournal of Clinical Endocrinology & Metabolism To subscribe to
Autoimmune Gastritis in Type 1 Diabetes: A ClinicallyOriented Review
Christophe E. M. De Block, Ivo H. De Leeuw, and Luc F. Van Gaal
Department of Diabetology-Endocrinology, Antwerp University Hospital and University of Antwerp, B-2650 Edegem, Belgium
Context: Autoimmune gastritis and pernicious anemia are common autoimmune disorders, beingpresent in up to 2% of the general population. In patients with type 1 diabetes or autoimmunethyroid disease, the prevalence is 3- to 5-fold increased. This review addresses the epidemiology,pathogenesis, diagnosis, clinical consequences, and management of autoimmune gastritis in type1 diabetic patients.
Synthesis: Autoimmune gastritis is characterized by: 1) atrophy of the corpus and fundus; 2) autoan-tibodies to the parietal cell and to intrinsic factor; 3) achlorhydria; 4) iron deficiency anemia; 5) hyper-gastrinemia; 6) pernicious anemia may result from vitamin B12 deficiency; and 7) in up to 10% ofpatients, autoimmune gastritis may predispose to gastric carcinoid tumors or adenocarcinomas. Thisprovides a strong rationale for screening, early diagnosis, and treatment. The management of patientswith autoimmune gastritis implies yearly determination of gastrin, iron, vitamin B12 levels, and acomplete blood count. Iron or vitamin B12 should be supplemented in patients with iron deficiency orpernicious anemia. Whether regular gastroscopic surveillance, including biopsies, is needed in patientswith autoimmune gastritis/pernicious anemia is controversial. The gastric carcinoids that occur in thesepatients generally do not pose a great threat to life, whereas the danger of developing carcinoma iscontroversial. Nevertheless, awaiting a consensus statement, we suggest performing gastroscopy andbiopsy at least once in patients with autoantibodies to the parietal cell, iron-, or vitamin B12-deficiencyanemia, or high gastrin levels.
Conclusion: The high prevalence of autoimmune gastritis in type 1 diabetic patients and its possibleadverse impact on the health of the patient provide a strong rationale for screening, early diagnosis,periodic surveillance by gastroscopy, and treatment. (J Clin Endocrinol Metab 93: 363–371, 2008)
Autoimmune gastritis and pernicious anemia are commonautoimmune diseases with respective prevalences of 2 and
0.15–1% in the general population, increasing with age (1–3). Inpatients with type 1 diabetes (4, 5) or autoimmune thyroid dis-ease (6, 7), the prevalence is 3- to 5-fold increased.
Autoimmune gastritis is characterized by atrophy of the cor-pus and fundus, and the presence of circulating autoantibodies tothe parietal cell (PCA) and to their secretory product, intrinsicfactor (AIF) (8). Chronic autoaggression to the gastric protonpump, H�/K�ATPase, may result in decreased gastric acid se-cretion, hypergastrinemia, and iron deficiency anemia (9, 10). Ina later stage of the disease, pernicious anemia may result fromvitamin B12 deficiency, which is 10 times more common in type
1 diabetic than nondiabetic subjects (5). Finally, in up to 10% ofpatients, autoimmune gastritis may predispose to gastric carci-noid tumors or adenocarcinomas (11). Determining demo-graphic, immunological, and genetic risk factors, and early di-agnosis of autoimmune gastritis are important to prevent andtreat iron deficiency anemia, pernicious anemia, and (pre)ma-lignant gastric lesions [intestinal metaplasia and enterochromaf-fin-like (ECL) hyper/dysplasia].
History
Thomas Addison was the first to report a patient with autoim-mune atrophic gastritis in 1849 (12). He described a “very re-
doi: 10.1210/jc.2007-2134 Received September 21, 2007. Accepted November 13, 2007.First Published Online November 20, 2007
Abbreviations: AIF, Autoantibodies to the intrinsic factor; CgA, chromogranin A; ECL,enterochromaffin-like; HLA, human leukocyte antigen; PCA, autoantibodies to the parietalcell.
S P E C I A L F E A T U R E
C l i n i c a l R e v i e w
J Clin Endocrinol Metab, February 2008, 93(2):363–371 jcem.endojournals.org 363
markable form of anemia,” which was later called perniciousanemia that was linked to atrophy of the gastric mucosa by Flintin 1860 (13). Successful treatment with raw liver suggested thatthis megaloblastic anemia was caused by insufficiency of an ex-trinsic factor (vitamin B12) and an intrinsic factor in gastric juice(14). The discovery of AIF by Schwartz in 1960 (15) and PCA byIrvine et al. in 1962 (16) constituted the immunological expla-nation of the underlying atrophic gastritis that causes perniciousanemia (17).
Definition and Diagnosis of AutoimmuneGastritis(Table 1)
Autoimmune gastritis affects the parietal cell-containing gastriccorpus and fundus with sparing of the antrum (8, 18). PCA,targeted against gastric H�/K�ATPase, are detected in 60–85%and intrinsic factor antibodies in 30–50% of patients with au-toimmune gastritis (5, 19).
Besides pernicious anemia, iron deficiency anemia is fre-quently observed (9, 10). Furthermore, autoimmune gastritis ischaracterized by hypo- or achlorhydria, high serum gastrin, andlow pepsinogen I concentrations (20, 21). Chronic hypergas-trinemia causes the ECL cells in the oxyntic mucosa to undergohyperplasia (22), which may progress toward dysplasia and gas-tric carcinoid tumors (11, 21) (Fig. 1).
PCA are detected by immunofluorescence staining of the cy-toplasma of gastric parietal cells (23). However, Karlsson et al.(24) showed that the ELISA to detect gastric H�/K�ATPase an-tibodies is 10-fold more sensitive than the indirect immunoflu-orescence technique and has a high specificity. Current ELISAshave a sensitivity and specificity of respectively 85–93% and80–85%. PCA are detected 60–90% of patients with autoim-mune gastritis and/or pernicious anemia (1, 8, 23).
The recognition of antibodies to intrinsic factor derives fromthe work of Taylor et al. (25) and Schwartz (15). Two types ofautoantibodies bind to intrinsic factor (AIF). Type I AIF blockthe binding of vitamin B12 to intrinsic factor, thereby preventingthe transport of vitamin B12 from the stomach to its absorptionsite in the terminal ileum. Type I AIF are demonstrable in 70%of patients with pernicious anemia (24). Type II autoantibodies
do not interfere with vitamin B12 transport. They can be foundin 30–40% of patients with pernicious anemia.
The destruction of H�/K�ATPase-containing parietal cellsresults in hypo- or achlorhydria. This can be measured using24-h gastric pH-metry or after stimulation with pentagastrin.Hypochlorhydria is defined as a maximal acid output less than15 mmol H�/h after injection of pentagastrin. A progressivedecrease in acid secretion in the case of autoimmune gastritiswith a decreased parietal cell mass has been found (21, 26, 27).Total achlorhydria is diagnostic of pernicious anemia. Achlo-rhydria interrupts the negative feedback of somatostatin onantral gastrin-producing cells causing hypergastrinemia (28).Fasting serum gastrin levels correlate negatively with peakacid output, and positively with the degree of corpus atrophy(21, 29) and with PCA levels (21). Low serum pepsinogen Ilevels, resulting from destruction of chief cells or zymogeniccells, are also characteristic of autoimmune gastritis(20, 30, 31).
Endoscopy and Pathology
On endoscopy, the affected corpus and fundus mucosa appearsshiny and red because of the visibility of submucosal blood ves-sels. The stomach wall thins, and the rugal folds flatten or dis-appear. In biopsy specimens, lymphocytic infiltrates are presentin the submucosa and lamina propria (19, 21). In the next stage,there is a marked reduction in the number of oxyntic glands,parietal and zymogenic cells, followed by replacement of normalglands by glandular structures lined with mucus-containing cellsresembling those of the small bowel mucosa (intestinal metapla-sia) (Fig. 1). A proliferation of ECL cells in the oxyntic mucosa(22), due to sustained hypergastrinemia, can be seen, which mayprogress in a small proportion of patients toward gastric carci-noid tumors (11, 32–34).
Epidemiology
In the general population, there is an age-related increase in theprevalence of PCA, from 2.5% in the third decade to 12% in theeighth decade (1, 2). The prevalence is even higher in subjectsaffected by another autoimmune disorder. In type 1 diabetes,PCA are found in 10–15% of children and 15–25% of adults (4,5, 35–37) (Fig. 2). The respective prevalences of autoimmunegastritis and pernicious anemia in the general population are 2and 0.15–1% (2, 3, 38, 39), compared with respectively 5–10%and 2.6–4% in type 1 diabetes (5, 21, 38, 40, 41).
Iron deficiency anemia is present in 20–40% of patients withautoimmune gastritis (10, 42), whereas pernicious anemia can bediagnosed in up to 15–25% of patients (43). The progression ofautoimmune gastritis to pernicious anemia is likely to span20–30 yr (44).
Finally, gastric carcinoid tumors are observed in 4–9% ofpatients with autoimmune gastritis/pernicious anemia, which is13 times more frequent than in controls (11, 32–34, 45). Patientswith autoimmune gastritis/pernicious anemia also have a 3- to
TABLE 1. Characteristics of autoimmune gastritis
Atrophic fundus and corpus, antrum sparedPCA and AIFHypo/achlorhydriaHypergastrinemiaLow serum pepsinogen I concentrationsVitamin B12 deficient megaloblastic (pernicious) anemiaIron deficiency anemiaIncreased chromogranin A levels: ECL cell hyperplasia and gastric
carcinoidsAssociation with endocrine organ-specific autoimmune disease
Type 1 diabetes mellitusHashimoto’s thyroiditis, Graves’ diseaseAddison’s diseaseAutoimmune polyglandular syndrome types II and III
364 De Block et al. Autoimmune Gastritis in Type 1 Diabetes J Clin Endocrinol Metab, February 2008, 93(2):363–371
6-fold increased gastric cancer risk, ranging from 0.9–9% (11,32, 34, 46–48).
Pathogenesis
The target autoantigens in autoimmune gastritis are the 100-kdcatalytic �-subunit and the 60- to 90-kd glycoprotein �-subunitof the gastric H�/K�ATPase (49, 50). Autoantibodies to the PCAand to their secretory product, intrinsic factor, are present in theserum and in gastric juice. The titer of PCA correlates with theseverity of corpus atrophy and is inversely proportional to theconcentration of parietal cells (21, 29). CD4� T cells recognizingparietal cell H�/K�ATPase mediate autoimmune gastritis. Dur-ing normal cell turnover, parietal cells release H�/K�ATPase,which may result in its selective uptake and processing by anti-
gen-presenting cells (51). Alternatively, Helicobacter pylori in-fection may play an initiating role in the pathogenesis of auto-immune gastritis and pernicious anemia (52–55) by inducingautoreactive T cells through gastric H�/K�ATPase-H. pylorimolecular mimicry at the T-cell level (53, 54), epitope spreading,and bystander activation. B cells produce autoantibodies to gas-tric H�/K�ATPase and to their secretory product, intrinsic fac-tor with help from activated CD4� T cells (50). Finally, parietalcell loss from the gastric mucosa may result from CD4� T cellsinitiated perforin-mediated cytotoxicity or Fas-FasL apoptosis(55).
Regardless of whether PCA are pathogenic or not, their pres-ence provides a convenient diagnostic probe for autoimmuneatrophic gastritis. A precise understanding of the pathogenesis ofautoimmunity may lead to rational therapeutic strategies di-rected toward restoration of tolerance or impeding the progres-
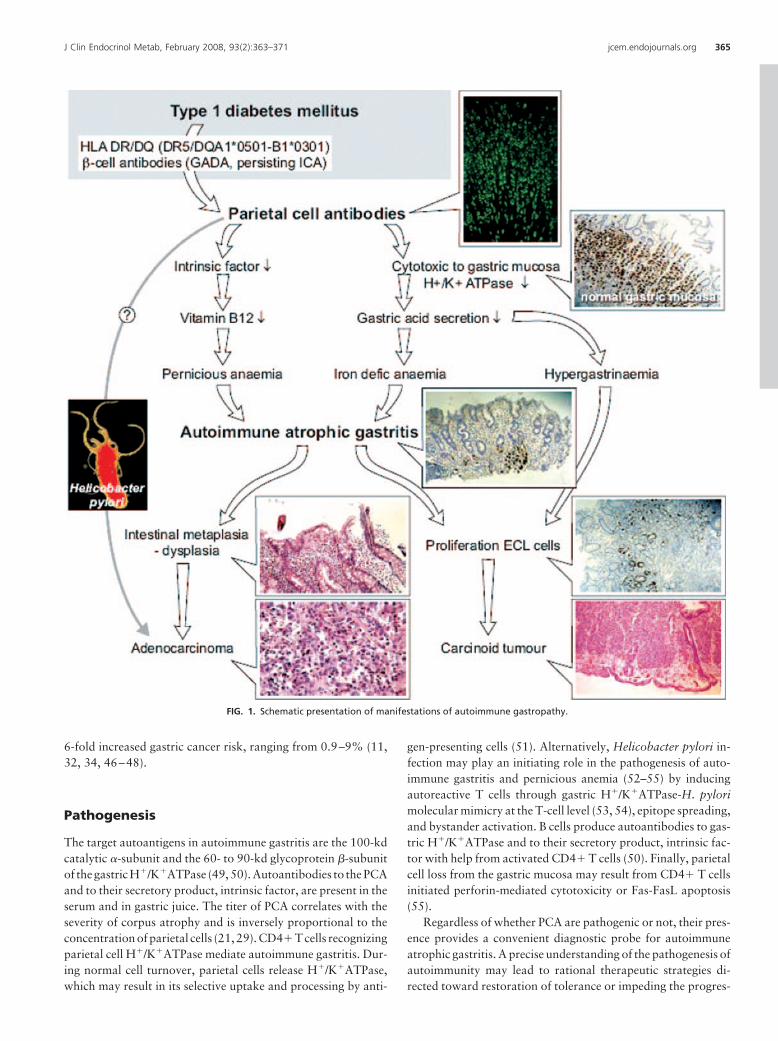
FIG. 1. Schematic presentation of manifestations of autoimmune gastropathy.
J Clin Endocrinol Metab, February 2008, 93(2):363–371 jcem.endojournals.org 365
sion of autoimmunity. Whether H. pylori could trigger autoim-mune gastritis or not remains controversial. However, shouldthis be the case, H. pylori eradication could prevent autoimmunegastric disease. Currently, it is recommended that H. pylori in-fection should be tested and treated in patients with gastric at-rophy, intestinal metaplasia/dysplasia, and hypo- orachlorhydria.
Predisposing Factors
Accurate prediction of autoimmune diseases (autoimmune gas-tritis) using antibodies (PCA and AIF), and demographic (age,gender) and genetic [human leukocyte antigen (HLA) class II,cytotoxic T lymphocyte-associated protein 4, others] risk factorsmight help to prevent these diseases. Primary prevention includesavoiding those environmental factors (H. pylori) that might trig-ger the disease. Secondary prevention consists of modulating thedestructive process (CD4� T cells mediating oxyntic gland at-rophy) before the onset of clinical symptoms [iron deficiency,pernicious anemia, and (pre)malignant gastric lesions]. How-ever, at present, there is no consensus on whom to screen or atwhat frequency.
Demographic factorsAdvancing age is a risk factor that has been associated with
PCA positivity. In the general population, PCA positivity in-creases from 2.5% in the third decade to 12% in the eighthdecade (1, 2). In type 1 diabetic patients, PCA are present in10–15% of children and 15–25% of adults (41). Some authors(4, 35) report a female preponderance for PCA positivity, al-though this has not been consistently observed (37, 41).
Endocrine and immunological factorsAutoimmune gastritis is frequently accompanied by other au-
toimmune diseases, including type 1 diabetes (5) and autoim-mune thyroid disease (Hashimoto’s thyroiditis and Graves’ dis-ease) (6, 38, 56). Autoimmune gastritis is also part of theautoimmune polyglandular syndrome type 3 (57). Perniciousanemia occurs in up to 4% of type 1 diabetic patients (5, 40),
2–12% of patients with autoimmune thyroid disease (6, 58), 6%of those with Addison’s disease, 9% of those with primary hy-poparathyroidism, and 3–8% of those with vitiligo (1) (Fig. 3).
In patients with type 1 diabetes, immunological risk factorsthat have been associated with PCA positivity include persistentislet cell antibody positivity (35, 36), glutamic acid decarboxyl-ase-65 antibody positivity (41, 59), and thyroid peroxidase au-toantibody positivity (41, 59). The association with glutamicacid decarboxylase-65 antibodies might be explained by the factthat glutamate decarboxylase-65 is not only present in the pan-creas and brain but can also be found in the thyroid gland andstomach. PCA are more frequent in type 1 diabetic patients thanin their first-degree relatives, even after HLA matching, suggest-ing that the diabetic condition itself plays an important role (60).
PCA can be found in 22% of patients with Graves’ disease and32–40% of those with autoimmune hypothyroidism (61–64).Pernicious anemia is present in 2% of patients with Graves’ dis-ease and 4–12% of those with Hashimoto’s thyroiditis (6, 61,62). Moreover, up to 50% of patients with autoimmune gastritis/pernicious anemia show thyroid peroxidase autoantibodies (21,62). These results support the recommendation of screening pa-tients with autoimmune thyroid disease for autoimmune gastri-tis. The close association between autoimmune thyroid diseaseand autoimmune gastritis suggests an immunological cross-re-action. In this respect, one group found a homologous 11-residuepeptide in thyroid peroxidase and the gastric parietal cell anti-gen, the H�/K�ATPase (65).
Immunogenetic factorsA genetic predisposition to autoimmune gastritis/pernicious
anemia has been suggested by its familial occurrence, and thepresence of PCA and autoimmune gastritis in 20–30% of rela-tives of patients with pernicious anemia (1, 5, 58).
HLA haplotypes can partly determine the tissue to which anautoimmune process develops. However, the evidence of a linkbetween pernicious anemia and particular HLA haplo/genotypesis weak. Associations of pernicious anemia with HLA DR4, withDR2 (66, 67) and DR5 haplotypes (5), have been reported. Intype 1 diabetic patients, a weak association between PCA pos-
FIG. 2. Prevalence of PCA in type 1 diabetes. �, Positive; f, female; m,male.
Fig. 3. Prevalence of PCA, AIF, autoimmune gastritis, and perniciousanemia in the general population and endocrine diseases. �, Positive; Ab,; t1DM, type 1 diabetes mellitus.
366 De Block et al. Autoimmune Gastritis in Type 1 Diabetes J Clin Endocrinol Metab, February 2008, 93(2):363–371
itivity and the HLA-DQA1*0501-B1*0301 haplotype, linked toHLA-DR5, has been observed (59). Patients who manifest bothpernicious anemia and endocrine disease often have a DR3/DR4genotype (66). These data suggest genetic heterogeneity.
In mouse models of autoimmune gastritis, four distinct ge-netic regions that confer susceptibility to autoimmune gastritishave been identified (68): two loci on distal chromosome 4,called Gasa1 and Gasa2; and two on chromosome 6, calledGasa3 and Gasa4 (51). Importantly, three of these four suscep-tibility loci are nonmajor histocompatibility complex genes thatcolocalize with those of type 1 diabetes (51, 54). This is thestrongest concordance identified between any two autoimmunediseases so far.
No association of autoimmune gastritis/pernicious anemiawith another two autoimmune disease candidate genes (theAIRE gene and cytotoxic T lymphocyte-associated protein 4) hasbeen reported.
Environmental factorsH. pylori might be implicated in the induction of autoimmune
gastritis (52, 53, 55). This hypothesis is supported by studiesreporting a high prevalence of H. pylori seropositivity and a lowprevalence of positive H. pylori staining in subjects with atrophiccorpus gastritis (69–72). Furthermore, the finding of gastric au-toantibodies in 20–50% of H. pylori-infected patients and re-ports of a positive correlation between gastric autoantibodiesand antibodies to H. pylori in patients with autoimmune gastri-tis/pernicious anemia (71, 73–76) suggest that chronic H. pyloriinfection is linked with gastric autoimmunity. However, a cor-relation between H. pylori and PCA has not been reported in allstudies (39, 77, 78). Moreover, others found no or a negative linkbetween H. pylori and atrophic corpus gastritis (79). On theother hand, H. pylori eradication in patients who have antigas-tric antibodies leads to the loss of those antibodies in some sub-jects (80). These data add new information to the possible re-versibility of gastric mucosa atrophy.
Clinical Presentation
Iron deficiency anemiaApproximately 20–30% of patients with iron deficiency ane-
mia with no evidence of gastrointestinal blood loss may haveautoimmune gastritis (9, 42, 81). Iron deficiency anemia maydevelop in advance of pernicious anemia, or both conditions maycoexist (82, 83).
Examination of the peripheral blood shows a hypochromic,microcytic anemia, decreased serum iron levels (male � 50 �g/dland female � 40 �g/dl), a transferrin saturation less than or equalto 20%, and a decreased ferritin concentration (male � 20 �g/liter and female � 12 �g/liter). However, these parameters areinfluenced by gender, acute phase responses, acute liver injury, ormalnutrition (84). A Perls staining of a bone marrow smearshowing absence of iron that is stored as hemosiderin in thereticuloendothelial cells of the bone marrow is definitive proof ofiron deficiency, but invasive. The soluble transferrin receptor hasbeen proposed as the best noninvasive and sensitive marker of
functional iron status because of its small day-to-day variation,and independence of inflammation, liver parenchymal, and hor-monal status (10, 85).
Symptoms and signs of iron deficiency include pallor, fatigue,reduced exercise or work performance, and palpitations, re-duced learning ability, defects in immunity, and even an in-creased frequency of premature births (84). Early detection andtreatment of iron deficiency and the conditions that are at itsorigin could significantly reduce morbidity. Treatment consistsof oral supplementation of 600 mg FeSO4. Alternatively, ironcan be infused iv (84).
The iron status of an individual depends on the amount ofdietary iron, its bioavailability, and the extent of iron losses (84).Although no absorption of iron occurs in the stomach, the gastrichydrochloric acid plays a significant role. Hydrochloric acid notonlyhelps to removeprotein-bound ironbyproteindenaturationbut also helps in the reduction of ferric iron (Fe2�) to the ferrousstate (Fe3�), necessary to improve absorption (86). Decreasedgastric acidity, due to chronic autoaggression to parietal H�/K�ATPase in autoimmune gastritis (27), may reduce the avail-ability of iron for absorption and lead to iron deficiency anemia(9, 10).
Pernicious anemiaPernicious anemia can be considered an end stage of auto-
immune gastritis (44). Approximately 10–15% of PCA-positivepatients and up to 25% of those with autoimmune gastritispresent with pernicious anemia (1, 5).
Two mechanisms are responsible for vitamin B12 malabsorp-tion in patients with pernicious anemia. First, the progressive lossof parietal cells leads to failure of intrinsic factor production anda reduction in vitamin B12 absorption. Second, intrinsic factorautoantibodies prevent the formation of the vitamin B12-intrin-sic factor complex (19).
Examination of the peripheral blood reveals macrocytosisand anemia, a low serum vitamin B12 concentration, and normalfolate concentration. A Schilling test, which measures vitaminB12 absorption in the presence and absence of intrinsic factor, isused to establish pernicious anemia as the cause of vitamin B12deficiency (19).
The usual presentation of vitamin B12 deficiency is withsymptoms of anemia. Gastrointestinal manifestations include asmooth and beefy red tongue (atrophic glossitis), and a predis-position to gastric tumors (see Gastric carcinoid tumors andGastric cancer). Neurological complications include peripheralneuropathy manifested by paraesthesia and numbness usually ofthe legs, and cerebral manifestations such as confusion, impairedmemory, and even frank psychosis (megaloblastic madness)(19, 87).
Early detection and treatment of vitamin B12 deficiency andthe underlying conditions could significantly reduce morbidity.The classical treatment is by daily im injections with 100 �gvitamin B12 for 1 wk, followed by monthly injections of 100 �gvitamin B12. In severe cases, parenteral administration of 1000�g/d for 1 wk, followed by 1000 �g/wk for 1 month, and thenby monthly im injection of 1000 �g is proposed (19, 88).
J Clin Endocrinol Metab, February 2008, 93(2):363–371 jcem.endojournals.org 367
Gastric carcinoid tumorsGastric carcinoid tumors, evolving from ECL cell hyper/dys-
plasia induced by hypergastrinemia, may develop in 4–9% ofpatients with autoimmune gastritis/pernicious anemia (11, 32–34, 89). Up to 85% of gastric carcinoid tumors are associatedwith autoimmune gastritis/pernicious anemia (90–92). In type 1diabetes, ECL cell proliferative changes occur in approximately9% of PCA-positive patients and in up to 30% of those withautoimmune gastritis (93). This provides a strong rationale forscreening, early diagnosis, and treatment.
The tumors are usually incidentally identified during diag-nostic endoscopic evaluation for anemia. The most frequentlyreported symptoms include abdominal pain, flushing and diar-rhea, anemia-related symptoms, and extremely rarely a carci-noid syndrome (92). Gastroscopy with histological examination[immunostaining for chromogranin A (CgA) and/or neuron-spe-cific enolase] is the most powerful diagnostic tool. However, agastroscopy can be considered unpleasant, and is hampered bythe fact that such lesions are usually not endoscopically detect-able, or unevenly distributed, and may be overlooked (91, 94).Moreover, part of an increased ECL cell density in atrophic mu-cosa may not be true hyperplasia but rather an expression of aselective glandular atrophy sparing the ECL cells. Thus, mor-phology is subject to sampling error and may over- or underes-timate ECL cell mass. Serum CgA measurements may indicatethe presence of an increased ECL cell mass more accurately thanmorphological methods (95). CgA can be released into the cir-culation from ECL cells of the stomach (65). Its levels correlatestrongly with ECL cell density in the corpus and fundus mucosaand with gastrin levels (33, 93, 95, 96). CgA has a specificity of85–90% and a sensitivity of 70–80% in diagnosing neuroen-docrine tumors. A recent study showed a sensitivity of 100% andspecificity of 59% for CgA to detect ECL cell hyper/dysplasia(93). Therefore, we recommend, besides performing a gastros-copy with biopsy, measuring CgA in PCA-positive patients, par-ticularly those with hypergastrinemia, who are at risk for devel-oping autoimmune gastritis and, possibly, carcinoid tumors.
Gastric carcinoid tumors are relatively benign lesions, metas-tasizing in less than 10% of cases, and death rarely results fromthese tumors (92).
An algorithm for the appropriate management of patientswith gastric carcinoid tumors has been proposed by Gilligan etal. (97). For autoimmune gastritis-associated carcinoid tumorsless than 1 cm and/or fewer than three to five in number, ex-pectant therapy or endoscopic removal of accessible tumors, fol-lowed by endoscopic surveillance are appropriate (11, 34, 91,94, 97). For lesions more than 1 cm in size and/or more than fivein number, antrectomy has been proposed (91, 98). Eitherantrectomy or endoscopic polypectomy should be followed byendoscopic surveillance at 6-month intervals, and any recurrenceshould be treated with surgical excision. Ferraro et al. (99)showed in a limited group of eight patients with hypergastrine-mic atrophic gastritis that once a day administration of oct-reotide is safe and effective in reducing hypergastrinemia andassociated ECL changes. In a small number of patients, a spon-taneous regression has been reported (100).
Gastric cancerA three to six times higher gastric cancer risk in patients with
autoimmune gastritis/pernicious anemia has been observed insome (11, 32, 34, 46–48) but not all (101, 102) studies. Theprevalence of gastric carcinoma in patients with pernicious ane-mia is 1–3%, and 2% of patients with gastric carcinoma havepernicious anemia (103).
Achlorhydria, overgrowth of bacteria promoting the forma-tion of N-nitroso compounds, and a high dietary salt consump-tion might promote the formation of a gastric carcinoma (104,105).
Regular endoscopic surveillance is warranted in patients withpernicious anemia (32–34). Patients with mild/moderate muco-sal dysplasia should be followed endoscopically every 5 yr (32).Polyps should be removed, and adenocarcinoma should be ex-cised. Complete surgical eradication of a gastric tumor, withresection of adjacent lymph nodes, is the only chance for a cure(106).
Management Proposal
Early detection of PCA, autoimmune gastritis, and associatedpathology (Fig. 1) is important in preventing iron deficiency ane-mia, which may influence work capacity and cardiopulmonarystatus, and pernicious anemia, which can cause neurologicalcomplications and (pre)malignant gastric lesions. For type 1 di-abetic patients, it seems prudent to test PCA status at the onsetof diabetes and then yearly for 3 yr, then five yearly thereafter,or at any other time if there are clinical indications because thetest may later become positive. Particularly those patients withpositive glutamate decarboxylase-65 antibodies and thyroid per-oxidase antibodies should be screened.
Treating patients with PCA and/or autoimmune gastritis im-plies a proper follow-up. At yearly intervals, gastrin, iron, vita-min B12 levels, and a complete blood count should be performed.Iron or vitamin B12 supplements should be given to patients withiron deficiency or pernicious anemia. It is controversial whetherpatients with autoimmune gastritis/pernicious anemia should beplaced under a surveillance program with regular gastroscopies,including multiple gastric biopsies. The gastric carcinoids thatoccur in these patients generally do not pose a great threat to life,whereas the danger of developing carcinoma is controversial.Nevertheless, awaiting a consensus statement, we suggest per-forming gastroscopy and biopsy at least once in patients withPCA positivity, anemia, or high gastrin levels. Patients with mildto moderate mucosal dysplasia should be followed endoscopi-cally every 5 yr (32). Polyps should be removed, and adenocar-cinoma should be excised. Gastric carcinoid tumors are rare andhave a far better outcome than carcinoma (92). Endoscopic sur-veillance at 5-yr intervals has been proposed for ECL cell hyper-plasia (11), especially for those patients with high gastrin (�300ng/liter) and CgA (�120 ng/ml) levels (93). For gastric carcinoidtumors associated with autoimmune gastritis, smaller than 1 cmand/or fewer than three, expectant therapy or endoscopic re-moval of accessible tumors is proposed (97).
368 De Block et al. Autoimmune Gastritis in Type 1 Diabetes J Clin Endocrinol Metab, February 2008, 93(2):363–371
ConclusionsAutoimmune gastritis and pernicious anemia are among themost common autoimmune diseases with respective prevalencesof 2 and 0.15–1% in the general population, increasing with age.Moreover, in patients with autoimmune thyroid disease or type1 diabetes, the prevalence is 3- to 5-fold increased.
In the clinical setting, PCA are a good marker of autoimmunegastropathy, such as iron deficiency anemia, pernicious anemia,and autoimmune gastritis. The well-known complications ofthese three disorders can influence the prognosis of the patient.Treating patients with PCA and/or autoimmune gastritis impliesa proper follow-up. At yearly intervals, gastrin, iron, vitaminB12 levels, and a complete blood count should be performed.Moreover, both autoimmune gastritis and pernicious anemiapredispose to gastric carcinoid tumors, which manifest them-selves only late in the disease process. The possible adverse im-pact on the health of the patient provides a strong rationale forscreening, periodic surveillance by gastroscopy with biopsy,early diagnosis, prevention, and/or treatment.
Understanding the current advances in autoimmune gastritisis key to the development of novel therapeutic strategies directedtoward restoration of tolerance or toward impeding the progres-sion of autoimmunity, and for making rational choices in themanagement of autoimmune gastropathy.
Acknowledgments
We thank Professor doctor Paul Pelckmans of the Department of Gas-troenterology and Hepatology, and Professor doctor E. Van Marck ofthe Department of Pathology for their collaboration throughout thisproject.
Address all correspondence and requests for reprints to: ChristopheDe Block, M.D., Ph.D., Department of Diabetology-Endocrinology,Antwerp University Hospital and University of Antwerp, Wilrijkstraat10, B-2650 Edegem, Belgium. E-mail: [email protected];[email protected].
Part of the studies mentioned and performed by the authors has beensupported by a grant from the European Foundation for the Study ofDiabetes.
Disclosure Statement: The authors have nothing to disclose.
References
1. Whittingham S, Mackay IR 1985 Pernicious anemia and gastric atrophy. In:Rose NR, Mackay IR, eds. The autoimmune diseases. New York: AcademicPress; 243–266
2. Jacobson DL, Gange SJ, Rose NR, Graham NM 1997 Epidemiology andestimated population burden of selected autoimmune diseases in the UnitedStates. Clin Immunol Immunopathol 84:223–243
3. Carmel R 1996 Prevalence of undiagnosed pernicious anemia in the elderly.Arch Intern Med 156:1097–1100
4. Riley WJ, Toskes PP, Maclaren NK, Silverstein J 1982 Predictive value ofgastric parietal cell autoantibodies as a marker for gastric and hematologicabnormalities associated with insulin dependent diabetes. Diabetes 31:1051–1055
5. De Block CE, De Leeuw IH, Van Gaal LF 1999 High prevalence of manifes-tations of gastric autoimmunity in parietal cell antibody-positive type 1 (in-sulin-dependent) diabetic patients. The Belgian Diabetes Registry. J Clin En-docrinol Metab 84:4062–4067.
6. Centanni M, Marignani M, Gargano L, Corleto VD, Casini A, Delle Fave G,
Andreoli M, Annibale B 1999 Atrophic body gastritis in patients with auto-immune thyroid disease. An underdiagnosed association. Arch Intern Med159:1726–1730
8. Strickland RG, Mackay I 1973 A reappraisal of the nature and significanceof chronic atrophic gastritis. Am J Dig Dis 18:426–440
9. Marignani M, Delle Fave G, Mecarocci S, Bordi C, Angeletti S, D’Ambra G,Aprile MMR, Corleto VD, Monarca B, Annibale B 1999 High prevalence ofatrophic body gastritis in patients with unexplained microcytic and macro-cytic anemia. Am J Gastroenterol 94:766–772
10. De Block CE, Van Campenhout CM, De Leeuw IH, Keenoy BM, Martin M,Van Hoof V, Van Gaal LF 2000 Soluble transferrin receptor level: a newmarker of iron deficiency anemia, a common manifestation of gastric auto-immunity in type 1 diabetes. Diabetes Care 23:1384–1388
11. Kokkola A, Sjoblom SM, Haapiainen R, Sipponen P, Puolakkainen P, Jarvi-nen H 1998 The risk of gastric carcinoma and carcinoid tumours in patientswith pernicious anaemia: a prospective follow-up study. Scand J Gastroen-terol 33:88–92
12. Addison T 1849 Anaemia: disease of the suprarenal capsules. London MedGaz 8:517–518
13. Flint A 1860 A clinical lecture on anaemia, delivered at the Long IslandCollege Hospital. American Medical Times 1:181–186
14. Castle WB 1953 Development of knowledge concerning the gastric intrinsicfactor and its relation to pernicious anemia. N Engl J Med 249:603–614
15. Schwartz M 1960 Intrinsic factor antibody in serum from patients with per-nicious anaemia. Lancet 2:1263–1267
16. Irvine WJ, Davies SH, Delamore IW, Williams AW 1962 Immunologicalrelationship between pernicious anemia and thyroid disease. Br J Med 2:454–456
17. Irvine W 1965 Immunologic aspects of pernicious anemia. N Engl J Med273:432–438
18. Kaye MD 1987 Immunological aspects of gastritis and pernicious anaemia.Baillieres Clin Gastroenterol 1:487–506
19. Toh BH, Van Driel IR, Gleeson PA 1997 Mechanisms of disease: perniciousanemia. N Engl J Med 337:1441–1448
20. Varis K, Kekki M, Harkonen M, Sipponen P, Samloff IM 1991 Serum pep-sinogen I and serum gastrin in the screening of atrophic pangastritis with highrisk of gastric cancer. Scand J Gastroenterol Suppl 186:117–123
21. De Block C, De Leeuw I, Bogers J, Pelckmans P, Ieven M, Van Marck E, VanAcker K, Van Gaal L 2003 Autoimmune gastropathy in type 1 diabetic pa-tients with parietal cell antibodies: histological and clinical findings. DiabetesCare 26:82–88
22. Solcia E, Fiocca T, Villani L, Gianatti A, Cornaggia M, Chiaravalli A, CurzioM, Capella C 1991 Morphology and pathogenesis of endocrine hyperplasias,precarcinoid lesions, and carcinoids arising in chronic atrophic gastritis.Scand J Gastroenterol Suppl 180:146–159
23. Fisher JM, Taylor KB 1965 A comparison of autoimmune phenomena inpernicious anemia and chronic atrophic gastritis. N Engl J Med 272:499–503
24. Karlsson FA, Burman P, Loof L, Olsson M, Scheynius A, Mardh S 1987Enzyme linked immunosorbent assay of H�/K�ATPase, the parietal cell an-tigen. Clin Exp Immunol 70:604–610
25. Taylor KB, Roitt IM, Doniach D, Couchman KG, Shapland C 1962 Auto-immune phenomena in pernicious anemia: gastric antibodies. Br Med J2:1347–1352
26. Perasso A, Testino G, de’Angelis P, Augeri C, de Grandi R 1990 Gastric chiefcell mass in chronic gastritis. Count and relationships to parietal cell mass andfunctional indices. Hepatogastroenterology 38(Suppl 1):63–66
27. Burman P, Mardh S, Norberg L, Karlsson FA 1989 Parietal cell antibodies inpernicious anemia inhibit H�, K�-adenosine triphosphatase, the protonpump of the stomach. Gastroenterology 96:1434–1438
28. Trudeau WL, McGuigan JE 1971 Relations between serum gastrin levels andrates of gastric hydrochloric acid secretion. N Engl J Med 284:408–412
29. Sipponen P, Valle J, Varis K, Kekki M, Ihamaki T, Siurala M 1990 Fastinglevels of serum gastrin in different functional and morphologic states of theantrofundal mucosa. An analysis of 860 subjects. Scand J Gastroenterol 25:513–519
30. Samloff IM, Varis K, Ihamaki T, Siurala M, Rotter JI 1982 Relationshipsamong serum pepsinogen I, serum pepsinogen II, and gastric mucosal histol-ogy. A study in relatives of patients with pernicious anemia. Gastroenterology83:204–209
31. Alonso N, Granada ML, Salinas I, Lucas AM, Reverter JL, Junca J, Oriol A,Sanmarti A 2005 Serum pepsinogen I an early marker of pernicious anemiain patients with type 1 diabetes. J Clin Endocrinol Metab 90:5254–5258
J Clin Endocrinol Metab, February 2008, 93(2):363–371 jcem.endojournals.org 369
velopment of gastric dysplasia in pernicious anaemia: a clinical and endo-scopic follow-up study of 80 patients. Gut 31:1105–1109
33. Borch K, Renvall H, Liedberg G 1985 Gastric endocrine cell hyperplasia andcarcinoid tumors in pernicious anemia. Gastroenterology 88:638–648
34. Sjoblom SM, Sipponen P, Jarvinen H 1993 Gastroscopic follow-up of per-nicious anaemia patients. Gut 34:28–32
35. Maclaren NK, Riley WJ 1985 Thyroid, gastric, and adrenal autoimmunitiesassociated with insulin-dependent diabetes mellitus. Diabetes Care 8(Suppl1):34–38
36. Betterle C, Zanette F, Pedini B, Presoto F, Rapp LB, Monciotto CM, RigonF 1984 Clinical and subclinical organ-specific autoimmune manifestations intype 1 (insulin-dependent) diabetic patients and their first-degree relatives.Diabetologia 26:431–436
37. Landin-Olsson M, Karlsson FA, Lernmark A, Sundkvist G 1992 Islet cell andthyrogastric antibodies in 633 consecutive 15- to 34-yr-old patients in thediabetes incidence study in Sweden. Diabetes 41:1022–1027
38. Betterle C, Mazzi PA, Pedini B, Accordi F, Cecchetto A, Presotto F 1988Complement-fixing gastric parietal cell autoantibodies. A good marker forthe identification of type A chronic atrophic gastritis. Autoimmunity 1:267–274
39. Oksanen A, Sipponen P, Karttunen R, Miettinen A, Veijola L, Sarna S, Raute-lin H 2000 Atrophic gastritis and Helicobacter pylori infection in outpatientsreferred for gastroscopy. Gut 46:460–463
40. Ungar B, Stocks AE, Whittingham S, Martin FIR, Mackay IR 1968 Intrinsic-factor antibody, parietal-cell antibody, and latent pernicious anaemia in di-abetes mellitus. Lancet 2:415–417
41. De Block CE, De Leeuw IH, Vertommen JJ, Rooman RP, Du Caju MV, VanCampenhout CM, Weyler JJ, Winnock F, Van Autreve J, Gorus FK, BelgianDiabetes Registry 2001 �-cell, thyroid, gastric, adrenal and coeliac autoim-munity and HLA-DQ types in type 1 diabetes. Clin Exp Immunol 126:236–241
42. Annibale B, Capurso G, Delle Fave G 2003 The stomach and iron deficiencyanaemia: a forgotten link. Dig Liver Dis 35:288–295
43. Toh BH, Alderuccio F 2004 Pernicious anaemia. Autoimmunity 37:357–36144. Irvine WJ, Cullen DR, Mawhinney H 1974 Natural history of autoimmune
achlorhydric atrophic gastritis. Lancet 2:482–48545. Kaplan LM, Graeme-Cook FM 1997 Case records of the Massachusetts Gen-
eral Hospital (Case 9–1997). A 39 year-old woman with pernicious anemiaand a gastric mass. N Engl J Med 336:861–867
46. Hsing A, Hansson L, McLaughlin J, Nyren O, Blot W, Ekbom A, FraumeniJr JF 1993 Pernicious anemia and subsequent cancer: a population-basedcohort study. Cancer 71:745–750
47. Brinton L, Gridley G, Hrubec Z, Hoover R, Fraumeni Jr JF 1989 Cancer riskfollowing pernicious anaemia. Br J Cancer 59:810–813
48. Carpenter C, Patalas E 2000 Case records of the Massachusetts GeneralHospital (Case 40–2000): a 38-year-old woman with gastric adenocarci-noma. N Engl J Med 343:1951–1958
49. Karlsson FA, Burman P, Loof L, Mardh S 1988 Major parietal cell antigen inautoimmune gastritis with pernicious anemia is the acid-producing H�, K�-adenosine triphosphatase of the stomach. J Clin Invest 81:475–479
50. Toh BH, Sentry JW, Alderuccio F 2000 The causative H�/K�ATPase antigenin the pathogenesis of autoimmune gastritis. Immunol Today 21:348–354
51. van Driel IR, Baxter AG, Laurie KL, Zwar TD, La Gruta NL, Judd LM, ScarffKL, Silveira PA, Gleeson PA 2002 Immunopathogenesis, loss of T cell toler-ance and genetics of autoimmune gastritis. Autoimmun Rev 1:290–297
52. Appelmelk B, Faller G, Claeys D, Kirchner T, Vandenbroucke-Grauls C 1998Bugs on trial: the case of Helicobacter pylori and autoimmunity. ImmunolToday 19:296–299
53. Amedei A, Bergman MP, Appelmelk BJ, Azzurri A, Benagiano M, TamburiniC, van der Zee R, Telford JL, Vandenbroucke-Grauls CM, D’Elios MM, DelPrete G 2003 Molecular mimicry between Helicobacter pylori antigens andH�, K�-adenosine triphosphatase in human gastric autoimmunity. J ExpMed 198:1147–1156
54. van Driel IR, Read S, Zwar T, Gleeson PA 2005 Shaping the T cell repertoireto a bona fide autoantigen: lessons from autoimmune gastritis. Curr OpinImmunol 17:570–576
55. D’Elios MM, Appelmelk BJ, Amedei A, Bergman MP, Del Prete GF 2004Gastric autoimmunity: the role of Helicobacter pylori and molecular mim-icry. Trends Mol Med 10:316–323
56. Lam-Tse WK, Batstra MR, Koeleman BP, Roep BO, Bruining MG, AanstootHJ, Drexhage HA 2003 The association between autoimmune thyroiditis,autoimmune gastritis and type 1 diabetes. Pediatr Endocrinol Rev 1:22–37
57. Betterle C, Dal Pra C, Mantero F, Zanchetta R 2002 Autoimmune adrenalinsufficiencyandautoimmunepolyendocrine syndromes: autoantibodies, au-
toantigens, and their applicability in diagnosis and disease prediction. EndocrRev 23:327–364
58. Doniach D, Roitt IM, Taylor KB 1963 Autoimmune phenomena in perni-cious anaemia: serological overlap with thyroiditis, thyrotoxicosis and sys-temic lupus erythematosus. Br Med J 1:1374–1379
59. De Block CE, De Leeuw IH, Rooman RP, Winnock F, Du Caju MV, Van GaalLF 2000 Gastric parietal cell antibodies are associated with glutamic aciddecarboxylase-65 antibodies and the HLA DQA1*0501-DQB1*0301 hap-lotype in Type 1 diabetes mellitus. Belgian Diabetes Registry. Diabet Med17:618–622
60. De Block CE, De Leeuw IH, Decochez K, Winnock F, Van Autreve J, VanCampenhout CM, Martin M, Gorus FK, Belgian Diabetes Registry 2001 Thepresence of thyrogastric antibodies in first-degree relatives of type 1 diabeticpatients is associated with age and proband antibody status. J Clin EndocrinolMetab 86:4358–4363
61. Burman P, Ma JY, Karlsson FA 1998 Autoimmune gastritis and perniciousanaemia. In: Weetman AP, ed. Endocrine autoimmunity and associated con-ditions. Dordrecht, The Netherlands: Kluwer Academic Publishers; 243–267
62. Weetman AP 2005 Non-thyroid autoantibodies in autoimmune thyroid dis-ease. Best Pract Res Clin Endocrinol Metab 19:17–32
63. Carmel R, Spencer CA 1982 Clinical and subclinical thyroid disorders asso-ciated with pernicious anemia. Arch Intern Med 142:1465–1469
64. Segni M, Borrelli O, Pucarelli I, Delle Fave GF, Pasquino AM, Annibale B2004 Early manifestations of gastric autoimmunity in patients with juvenileautoimmune thyroid disease. J Clin Endocrinol Metab 89:4944–4948
65. Elisei R, Mariotti S, Swillens S, Vassart G, Ludgate M 1990 Studies withrecombinant autoepitopes of thyroid peroxidase: evidence suggesting anepitope shared between the thyroid and the gastric parietal cell. Autoimmu-nity 8:65–70
66. Ungar B, Mathews J, Tait BD, Cowling DC 1981 HLA-DR patterns in per-nicious anaemia. Br Med J (Clin Res Ed) 282:768–770
67. Van den Berg-Loonen EM, Hilterman TL, Bins M, Engelfriet CP 1982 In-creased incidence of HLA-DR2 in patients with pernicious anemia. TissueAntigens 19:158–160
68. Baxter AG, Jordan MA, Silveira PA, Wilson WE, van Driel IR 2005 Geneticcontrol of susceptibility to autoimmune gastritis. Int Rev Immunol 24:55–62
69. Karnes Jr WE, Samloff IM, Siurala M, Kekki M, Sipponen P, Kim SW, WalshJH1991Positive serumantibodyandnegative tissue staining for Helicobacterpylori in subject with atrophic body gastritis. Gastroenterology 101:167–174
71. Ma JY, Borch K, Sjostrand SE, Janzon L, Mardh S 1994 Positive correlationbetween H,K-adenosine triphosphatase autoantibodies and Helicobacter py-lori antibodies in patients with pernicious anemia. Scand J Gastroenterol29:961–965
72. Annibale B, Aprile MR, D’ambra G, Caruana P, Bordi C, Delle Fave G 2000Cure of Helicobacter pylori infection in atrophic body gastritis patients doesnot improve mucosal atrophy but reduces hypergastrinemia and its relatedeffects on body ECL-cell hyperplasia. Aliment Pharmacol Ther 14:625–634
73. Uibo R, Vorobjova T, Metskula K, Kisand K, Wadstrom T, Kivik T 1995Association of Helicobacter pylori and gastric autoimmunity: a population-based study. FEMS Immunol Med Microbiol 11:65–68
74. Negrini R, Savio A, Poiesi C, Appelmelk B, Buffoli F, Paterlini A, Cesari P,Graffeo M, Vaira D, Franzin G 1996 Antigenic mimicry between Helicobac-ter pylori and gastric mucosa in the pathogenesis of body atrophic gastritis.Gastroenterology 111:655–665
75. Faller G, Steiniger H, Kranzlein J, Maul H, Kerkau T, Hensen J, Hahn EG,Kirchner T 1997 Antigastric autoantibodies in Helicobacter pylori infection:implications of histological and clinical parameters of gastritis. Gut 41:619–623
76. Claeys D, Faller G, Appelmelk BJ, Negrini R, Kirchner T 1998 The gastricH�/K� ATPase is a major autoantigen in chronic Helicobacter pylori gas-tritis with body mucosa atrophy. Gastroenterology 115:340–347
77. Kohlstadt IC, Antunez De Mayolo EA 1993 Parietal cell antibodies amongPeruvians with gastric pathology changes. Scand J Gastroenterol 28:973–977
78. De Block CEM, De Leeuw IH, Bogers JJPM, Pelckmans PA, Ieven M, VanMarck EAE, Van Hoof V, Maday E, Van Acker KL, Van Gaal LF 2002Helicobacter pylori, parietal cell antibodies and autoimmune gastropathy intype 1 diabetes mellitus. Aliment Pharmacol Ther 16:281–289
79. Villako K, Kekki M, Maaroos HI, Sipponen P, Tammur R, Tamm A, Ke-evallik R 1995 A 12-year follow-up study of chronic gastritis and Helico-bacter pylori in a population-based random sample. Scand J Gastroenterol30:964–967
80. Faller G, Winter M, Steininger H, Lehn N, Meining A, Bayerdorffer E, Kirch-
370 De Block et al. Autoimmune Gastritis in Type 1 Diabetes J Clin Endocrinol Metab, February 2008, 93(2):363–371
ner T 1999 Decrease of antigastric autoantibodies in Helicobacter pylorigastritis after cure of infection. Pathol Res Pract 195:243–246
81. Rockey DC, Cello JP 1993 Evaluation of the gastrointestinal tract in patientswith iron-deficiency anemia. N Engl J Med 329:1691–1695
82. McIntyre AS, Long RG 1993 Prospective survey of investigations in outpa-tients referred with iron deficiency anaemia. Gut 34:1102–1107
83. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J 2006 Vari-able hematologic presentation of autoimmune gastritis: age-related progres-sion from iron deficiency to cobalamin depletion. Blood 107:1673–1679
84. Andrews NC 1999 Disorders of iron metabolism. N Engl J Med 341:1986–1995
85. Skikne BS, Flowers CH, Cook JD 1990 Serum transferrin receptor: a quan-titative measure of tissue iron deficiency. Blood 75:1870–1876
86. Schade SS, Cohen RJ, Conrad ME 1968 The effect of hydrochloric acid oniron absorption. N Engl J Med 279:672–674
87. Lindenbaum J, Healton EB, Savage DG, Brust JCM, Garrett TJ, Podell ER,Marcell PD, Stabler SP, Allen RH 1988 Neuropsychiatric disorders caused bycobalamin deficiency in the absence of anemia or macrocytosis. N Engl J Med318:1720–1728
88. Lane LA, Rojas-Fernandez C 2002 Treatment of vitamin B12-deficiency ane-mia: oral versus parenteral therapy. Ann Pharmacother 36:1268–1272
89. De Block CE, De Leeuw IH, Pelckmans PA, Michielsen PP, Bogers JJ, VanMarck EA, Van Gaal LF 2000 Autoimmune hepatitis, autoimmune gastritis,and gastric carcinoid in a type 1 diabetic patient: a case report. J DiabetesComplications 14:116–120
90. Harvey RF, Bradshaw MJ, Davidson CM, Wilkinson SP, Davies PS 1985Multifocal gastric carcinoid tumours, achlorhydria, and hypergastrinaemia.Lancet 1:951–954
91. Rindi G, Luinetti O, Cornaggia M, Capella C, Solcia E 1993 Three subtypesof gastric argyrophil carcinoid and the gastric neuroendocrine carcinoma: aclinicopathologic study. Gastroenterology 104:994–1006
92. Modlin IM, Kidd M, Latich I, Zikusoka MN, Shapiro MD 2005 Currentstatus of gastrointestinal carcinoids. Gastroenterology 128:1717–1751
93. De Block CE, Colpin G, Thielemans K, Coopmans W, Bogers JJ, PelckmansPA, Van Marck EA, Van Hoof V, Martin M, De Leeuw IH, Bouillon R, VanGaal LF 2004 Neuroendocrine tumor markers and enterochromaffin-like cellhyper/dysplasia in type 1 diabetes. Diabetes Care 27:1387–1393
94. Gough DB, Thompson GB, Crotty TB, Donohue JH, Kvols LK, Carney A,Grant CS, Nagorney DM 1994 Diverse clinical and pathologic features ofgastric carcinoid and the relevance of hypergastrinemia. World J Surg 18:473–479
95. Borch K, Stridsberg M, Burman P, Rehfeld JF 1997 Basal chromogranin Aand gastrin concentrations in circulation correlate to endocrine cell prolifer-ation in type A gastritis. Scand J Gastroenterol 32:198–202
96. Peracchi M, Gebbia C, Basilisco G, Quatrini M, Tarantino C, Vescarelli S,Massironi S, Conte D 2005 Plasma chromogranin A in patients with auto-immune chronic atrophic gastritis, enterochromaffin-like cell lesions and gas-tric carcinoids. Eur J Endocrinol 152:443–448
97. Gilligan CJ, Lawton G, Tang L, West A, Modlin I 1995 Gastric carcinoidtumors: the biology and therapy of an enigmatic and controversial lesion.Am J Gastroenterol 3:338–352
99. Ferraro G, Annibale B, Marignani M, Azzoni C, D’Adda T, D’Ambra G,Bordi C, Delle Fave G 1996 Effectiveness of octreotide in controlling fastinghypergastrinemia and related enterochromaffin-like cell growth. J Clin En-docrinol Metab 81:677–683
101. Eriksson S, Clase L, Moquist-Olsson I 1981 Pernicious anemia as a risk factorin gastric cancer: the extent of the problem. Acta Med Scand 210:481–484
102. Schafer LW, Larson DE, Melton III LJ, Higgins JA, Zinsmeister AR 1985 Riskof development of gastric carcinoma in patients with pernicious anemia: apopulation-based study in Rochester, Minnesota. Mayo Clin Proc 60:444–448
103. Kuipers EJ 1998 Review article: relationship between Helicobacter pylori,atrophic gastritis and gastric cancer. Aliment Pharmacol Ther 12(Suppl 1):25–36
104. Ruddell WS, Bone ES, Hill MJ, Walters CL 1978 Pathogenesis of gastriccancer in pernicious anaemia. Lancet 1:521–523
105. Correa P 2004 Is gastric cancer preventable? Gut 53:1217–1219106. Fuchs CS, Mayer RJ 1995 Gastric carcinoma. N Engl J Med 333:32–41
J Clin Endocrinol Metab, February 2008, 93(2):363–371 jcem.endojournals.org 371