81
Avian Tumor viruses Dr./ Wafaa Abd El-ghany Assistant Professor of poultry dis., Fac. Vet. Med., Cairo Univ.

Avian Tumor
viruses
Dr./ Wafaa Abd El-ghany
Assistant Professor of poultry dis.,
Fac. Vet. Med., Cairo Univ.

(MD)Polyneuritis, Fowl
paralysis,
Neurolymphomatosis
Definition Marek’s disease is a contagious
lymphoproliferative disease of chickens which
is characterized by a mononuclear infiltration
of one or more of the following; peripheral
nerves, gonads, iris, various muscles and
skin.

Economic losses
MD constituted a serious economic threat to thepoultry industry because of the heavy losses sincevaccines are not 100% effective losses may occurbut they are no longer serious a problem.
1. Losses from mortality.
2. Decrease the production (meat and eggs).
3. High incidence of low graded carcasses.
4. Immunosuppression (vaccination failure and susceptibility to another infections).
5. High cost of vaccination.

Etiology Marek’s disease is caused by an alpha herpes virus
(double strand DNA virus).
it differs from the other oncogenic herpes viruseswhich are gamma herpes viruses.
Marek’s disease virus (MDV) is an ubiquitous virusin poultry populations of the world.
It is a highly cell associated herpes virus withlymphotropic properties and propagate in nucleuswith intra nuclear inclusion bodies.
Marek's disease is commonly associated withcoccidiosis in the field, this probably due to lack ofimmunity against coccidiosis in birds affected withMarek's disease.

Etiology MDV classification:
Pathogenic strains of MDV and their attenuatedvariants (serotype 1) (Rispen) virulent (oncogenic)for chickens.
Apathogenic strain (serotype 2) (SB1).
Turkey herpes virus HVT (serotype 3) isolatedfrom turkeys and non pathogenic for chickens.
Serotypes include [mild strain (MMDV), virulentstrain (VMDV), very virulent (VVMDV) and veryvirulent + (VVMD)+ strain].
Serotypes 2 and 3 are used in vaccination.
Very virulent stain is attenuated to make a vaccine(Rispen).
EtiologyPathotypes: Avirulent MDV (CVI 988) was isolated and was named
Rispens.
Virulence or oncogenicity is associated only with serotype I
MDVs, within this group a wide variation in pathogenic
potential is recognized.
The very virulent Marek’s disease virus (vvMDV) pathotype
virus strains were first noted in the lat 1970s mainly in HVT
vaccinated flocks with excessive MD losses and now appear
to be the dominant type.
MDV is normally propagated and assayed in newly hatched
chicks, tissue cultures and embryonated eggs.

Laboratory host system
Chicks: Virulent MDV inoculation in day old chicks induces histopathological lesions in nerves and visceral organs and immunological changes after 2-4 weeks.
Cell culture: in Duck EF or CKC, MDV induce plaques of rounded cells and giant cells with several hundreds of nuclei.
Chicken embryos: Via yolk sac induce pock lesions appear on CAM at the 18th day post inoculation.


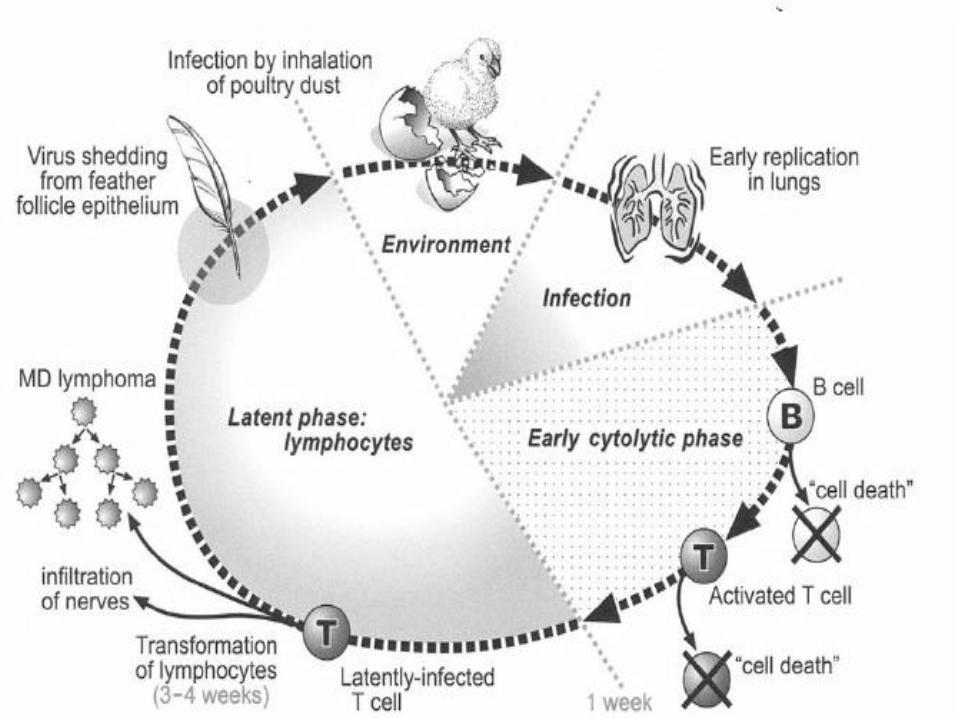
Pathogenesis The virus gains entrance via the respiratory
tract where it is picked up by phagocytic cells
(macrophages of the trachea).
shortly thereafter, cytolytic infection can be
detected in the spleen, bursa of fabricus and
thymus peaking at 3-6 days.
The primary target cells in all 3 organs are B
cells, although some activated T cells become
infected.
Resting T cells are refractory to infection.

Pathogenesis Four phases of infection can be delineated:
1. Cytolytic infection (Early productive-restrictive virus infection)causing primarily degenerative changes through 3-6 days. Itinclude serotypes I, II and III resulting in temporaryimmunosuppression.
2. Latent infection. It include serotypes I and II and it is non-pathogenic.
3. A second phase of cytolytic productive-restrictive infectioncoincident with permanent immunosuppression (destroy all Bcells). The virus metastasis in internal organs and skin invadethe epithelial cells causing focal cell death and necrosis withinflammatory changes then cause cutanous tumors in thefeather follicles.
4. A proliferative (lymphoid) phase involving non-productivelyinfected lymphoid cells that may progress to the point oflymphoma formation.

VIRUSRESPIRATORY TRACT PHAGOCYTIC
CELLSSPLEEN , BURSA AND THYMUS
3.Hyperplastic BURSAL AND THYMIC atrophy due to the suppressor
macrophage - TRANSANTIMMUNOSUPPRESION.
Both genetic susceptible and resistant birds are equally affected
4.LETANCY: started with the appearance of CMI as infection
become latent in T-CELLS
5. Second cytolysis effect: Genetic susceptible birds develop
TUMERES.2-3wpi.
6.Lymphoproliferative changes: the developed tumors either regressed or
developed continuously.

Susceptibility The natural host is chickens.
Pheasants and sparrows are experimental hosts and are refractory o infection.
Ducks become infected without disease after experimental MDV inoculation.
Turkeys show low rate of lymphoid tumors.
All ages are susceptible but 8 weeks old chickens are highly susceptible to MDV infection.
Infection and transmission Aapparently by the air borne route.
Direct or indirect contact.
Epithelial cells in the keratinizing layer (dander), of thefeather follicle replicate fully infectious virus, and these cellsserve as a source of contamination to the environment.
Many apparently normal birds are carriers and can transmitthe infection.
Continual shedding of the virus by infected birds after 2weeks from infection makes prevalence of infection, thevirus can live at 4C for 10 years inside the host.
Darkling beetles were shown to passively carry the virus.
MDV could be inactivated by variety of chemicaldisinfectants and the virus is affected by humidity.

Darkling beetles (Alphitobius diaperinus)
can be a carrier of MD

Incubation period Virus excrete beginning about 2 wk with maximal
shedding occurring between the 3rd and 5th wk.
Clinical sings and gross lesions, however, generallydo not appear until between the 3rd and 4th wk mostserious cases begin after the 8th or 9th wk and 16th
wk.
Incubation period of MDV is variable depends onmany factors; (either related to MDV or the host): virus strain (virulence),
dosage,
route of infection,
genetic resistance to the strain,
age,
sex of the host.
maternal antibody status,
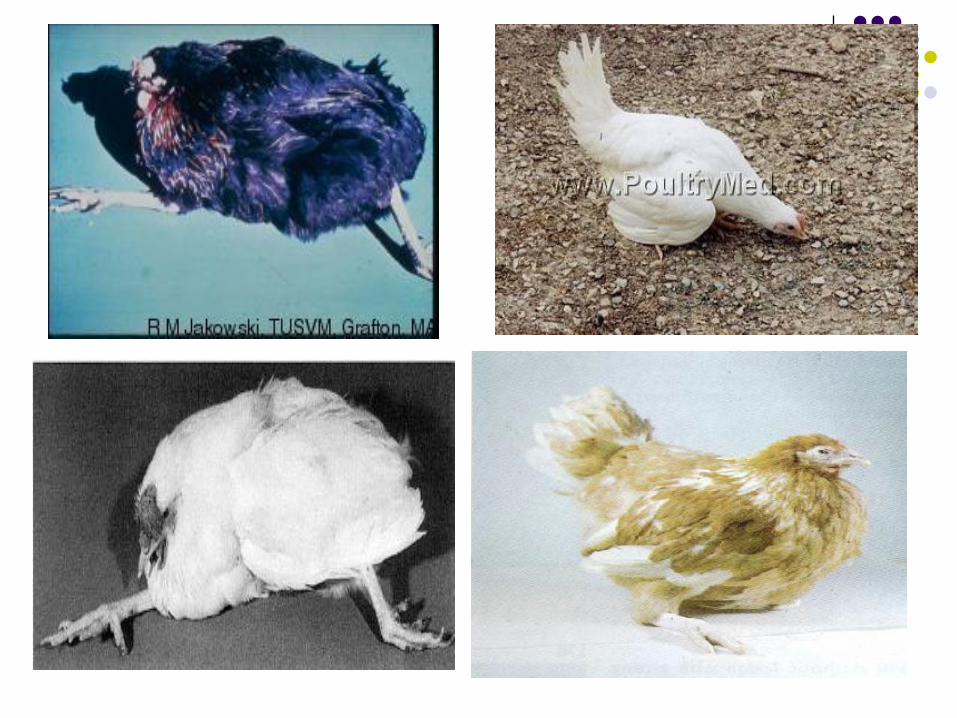
Clinical forms Classical (Neural) chronic from:- The virus affects primarily the peripheral nerves or
plexus (one or both or even part of the nerve) inducespraises and later complete paralysis of one or more ofextremities.
- Affection of the sciatic nerve resulting in progressivelameness of one or both legs, the bird lies on theground with a tendency to hold one leg forward orbackward (Ballerina position). The paralyzed bird isunable to reach food and water from starvation anddehydration.
- Affection of the brachial nerves can result indroopiness of the wings.

Clinical forms Classical (Neural) chronic from:- Affection of the intercostal and vagus nerves induces
false abdominal respiratory signs (difficult breathingand gasping).
- Occasionally, affection of cervical nerves mayresulting in torticollus.
- Affection of nerve supply the crop induces flaccidityof the crop (Pendulous crop).
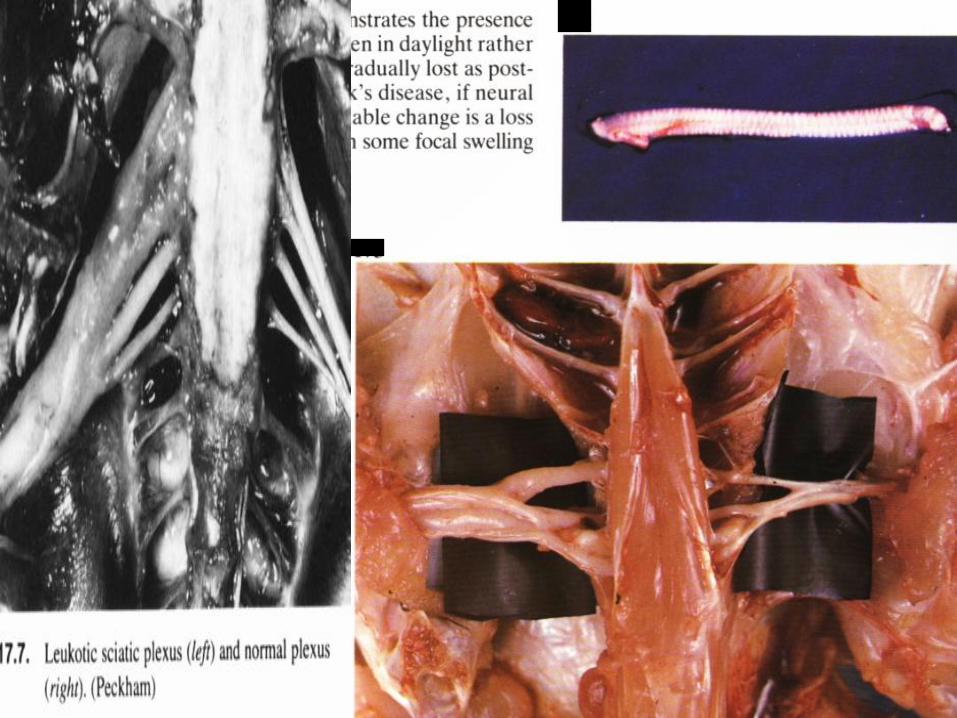
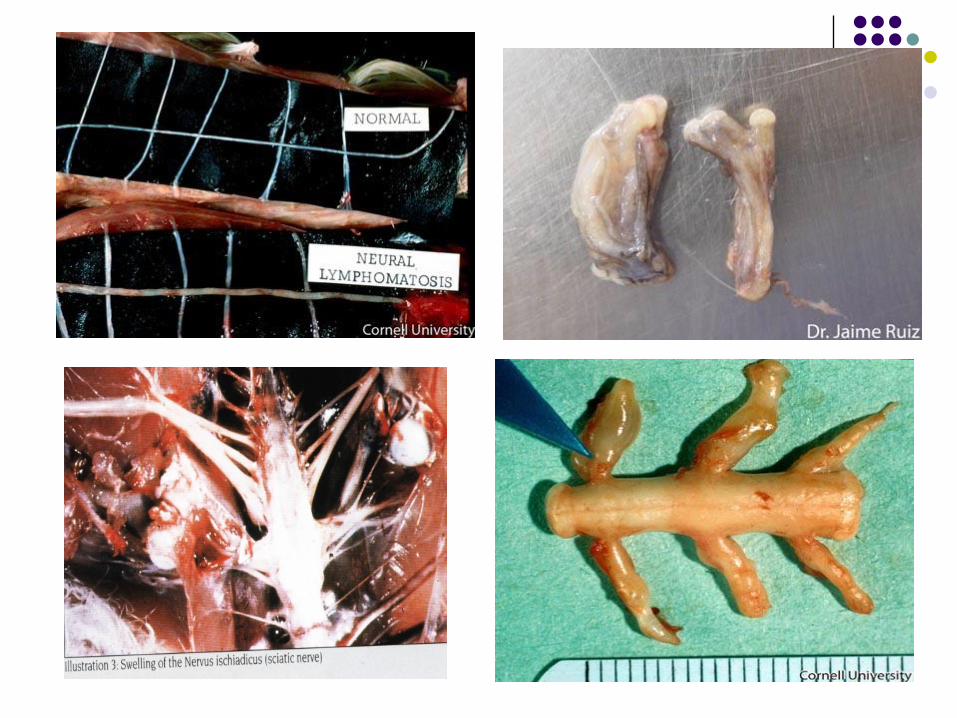
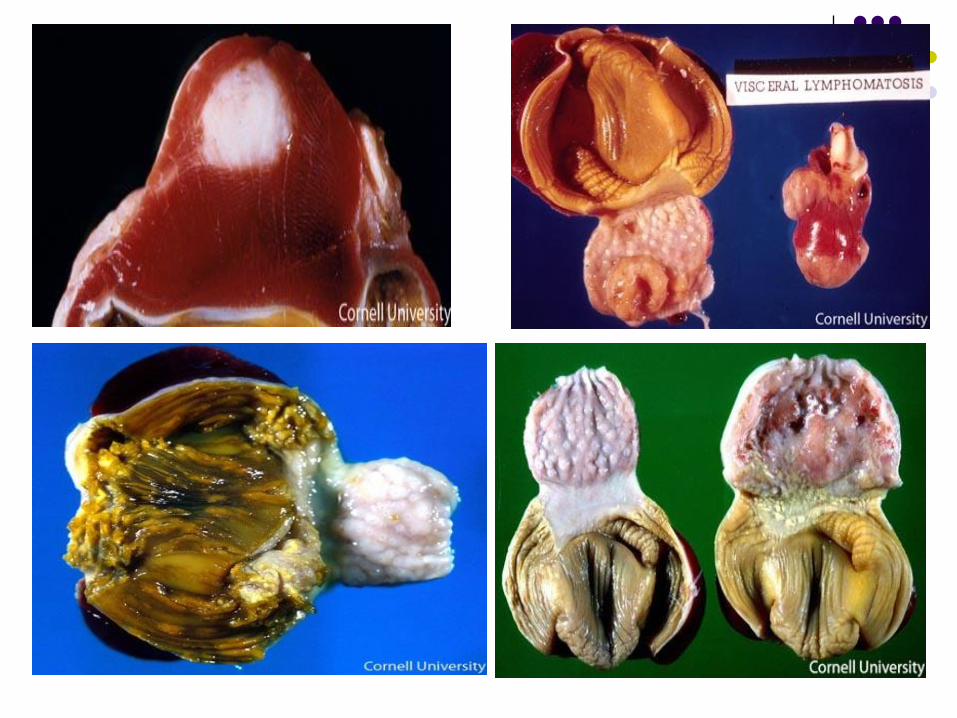
- The normal nerve is thin, glistening with crossstriation, while affected nerves show unilateral orbilateral diffuse thickening (oedematus or cord like)(2-3 times) with loss of cross station and glistening(dull appearance).

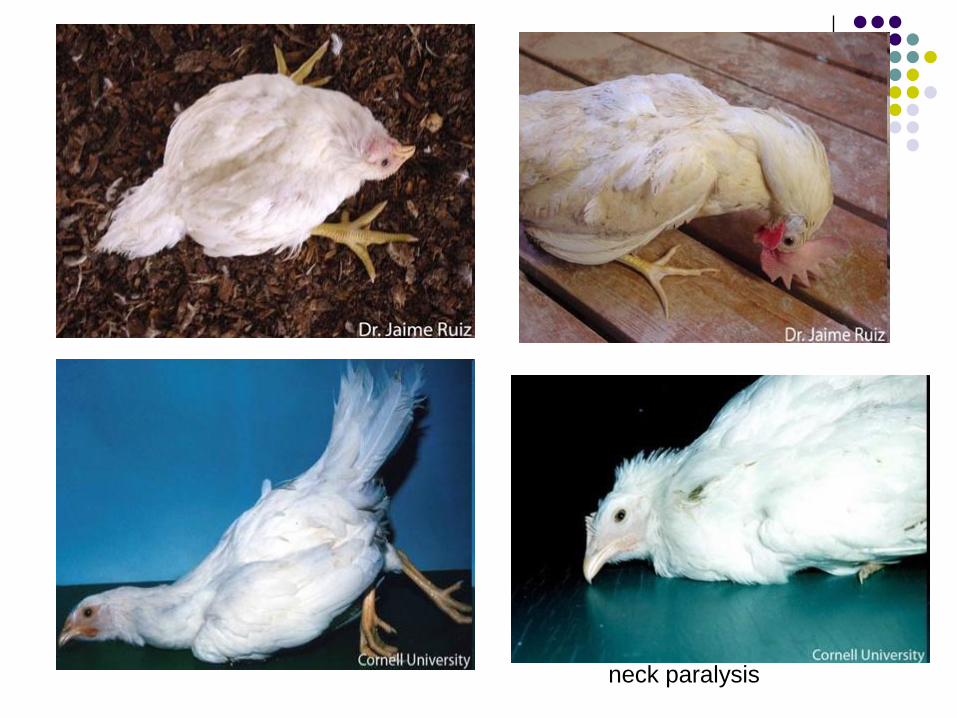
neck paralysis




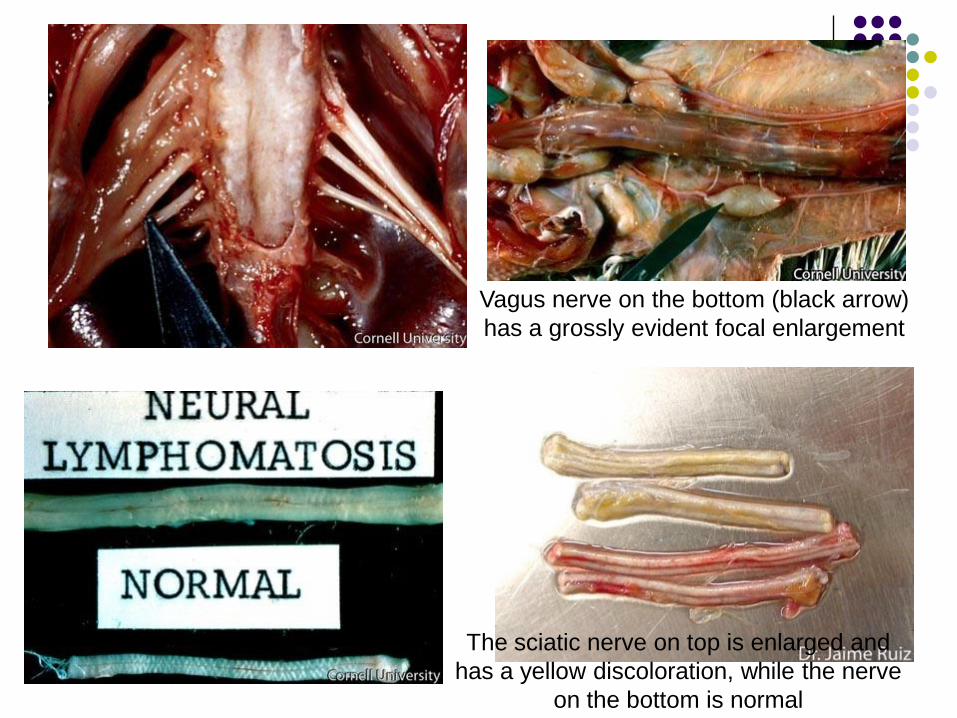
Vagus nerve on the bottom (black arrow)
has a grossly evident focal enlargement
The sciatic nerve on top is enlarged and
has a yellow discoloration, while the nerve
on the bottom is normal


Clinical formsOcular form: Concentric annular or spotty de-pigmentation or
diffuse bluish fading to diffuse grayish spots(opacity) (lymphocytic infiltration) of the goldenyellow iris.
The circular pupil at first becomes irregular(Serrated) and at advanced stages is only a smallpinpoint (slit like) opening.
Blindness may result from involvement of iris (Lossof light accommodation).
The eyes take the shape of (Fish eyeappearance).
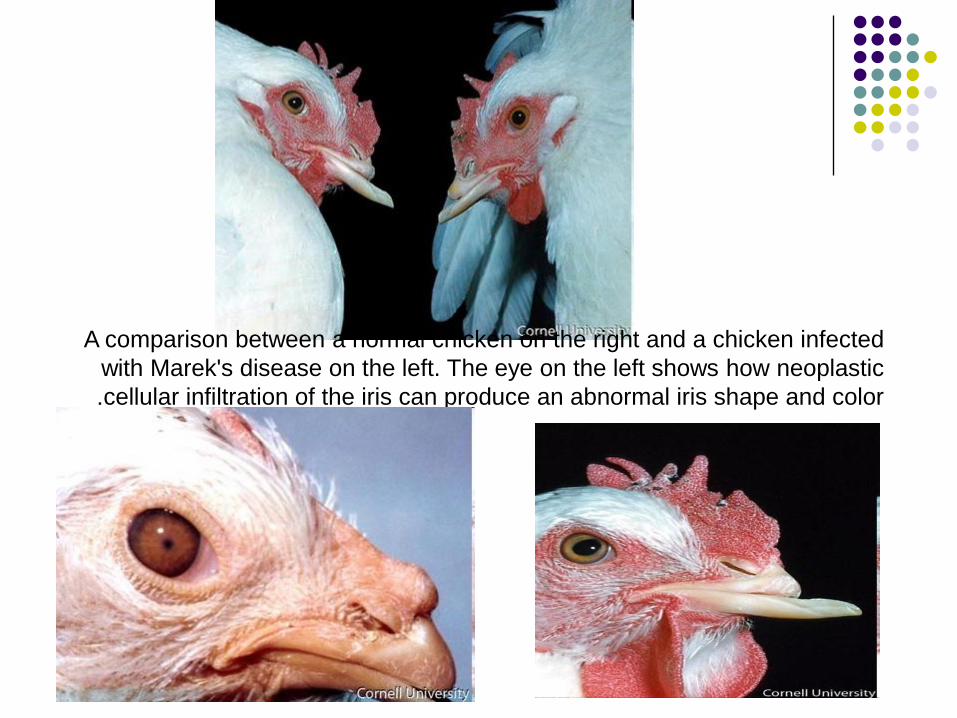
A comparison between a normal chicken on the right and a chicken infected
with Marek's disease on the left. The eye on the left shows how neoplastic
cellular infiltration of the iris can produce an abnormal iris shape and color .



Lymphoid infiltration of iris that
causes white discoloration. The
A normal eye is on the left. pupil
is often irregular


Clinical forms
Acute form: Non specific sings.
This form occurs in young birds raised intensively
at the age of 3-8 weeks up to 12 wk, with rapid
course and high morbidity and mortality up to 50%.
Some birds show depression, ataxia, unilateral or
bilateral paralysis, diarrhea, dehydration,
emaciation and coma.
Many birds die suddenly without showing signs.

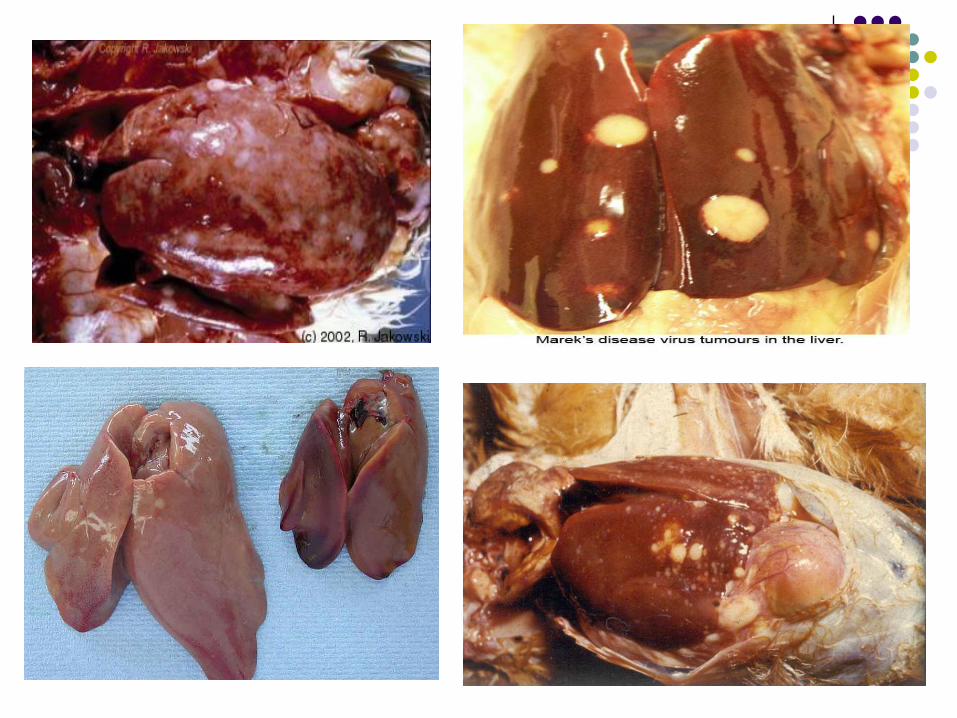
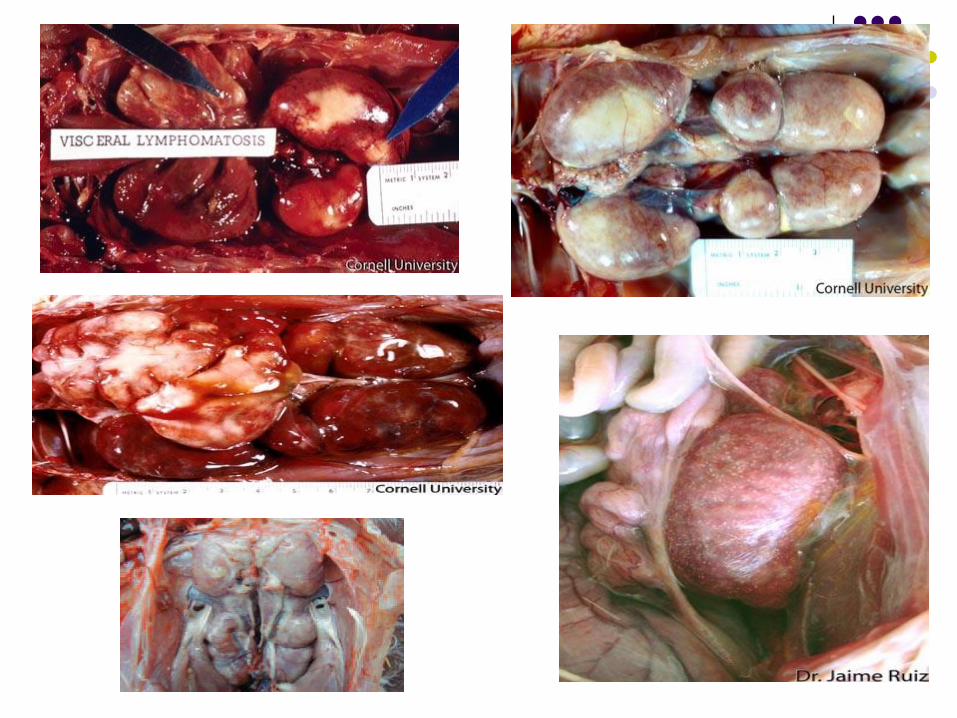
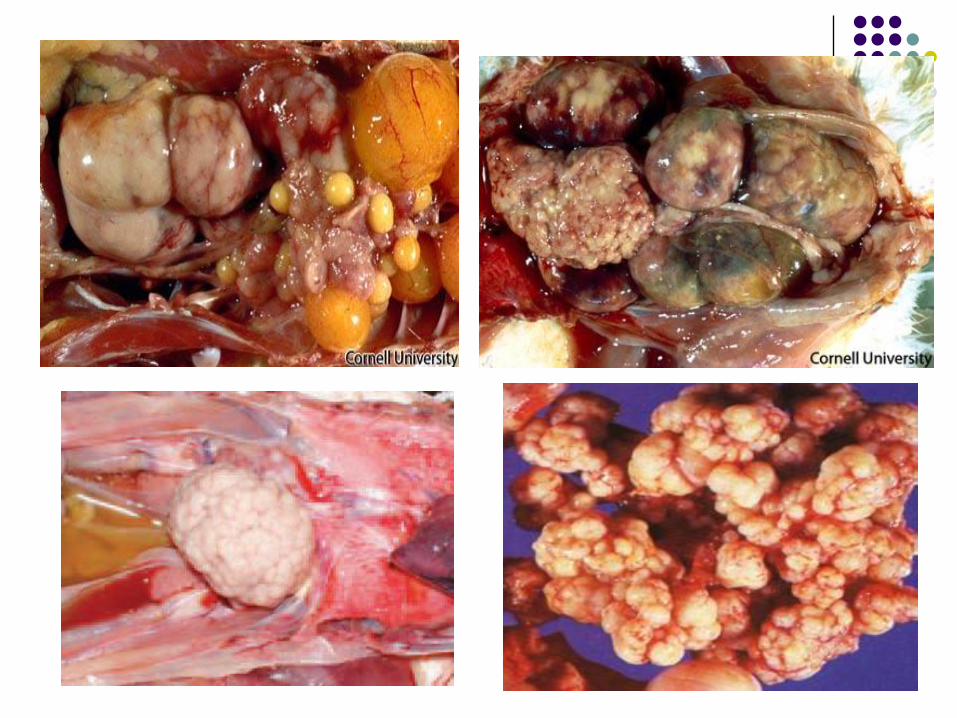
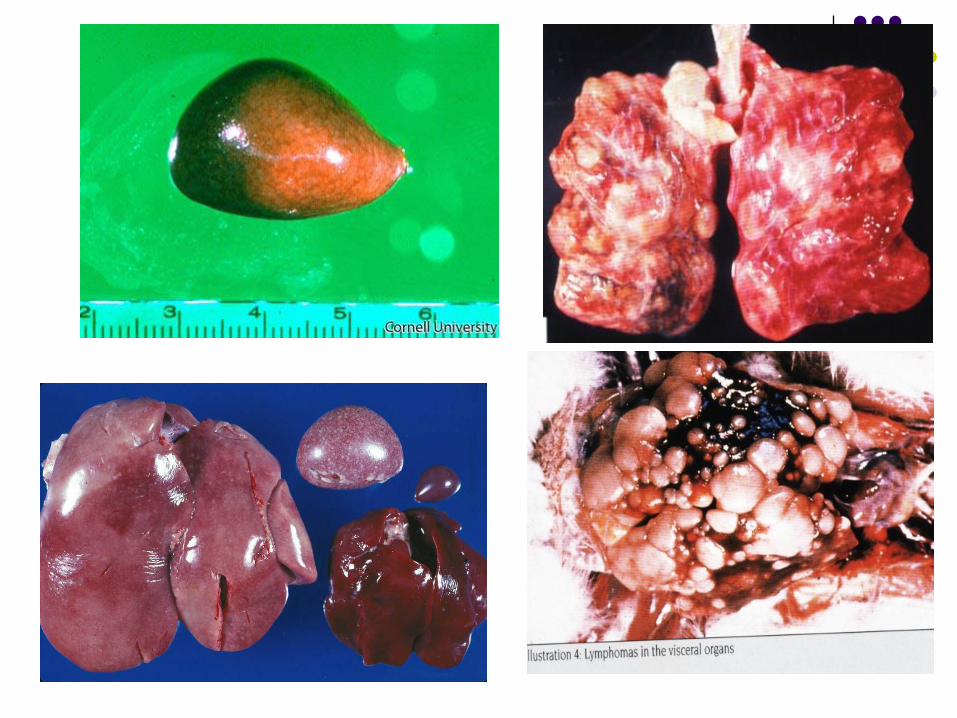
Clinical forms
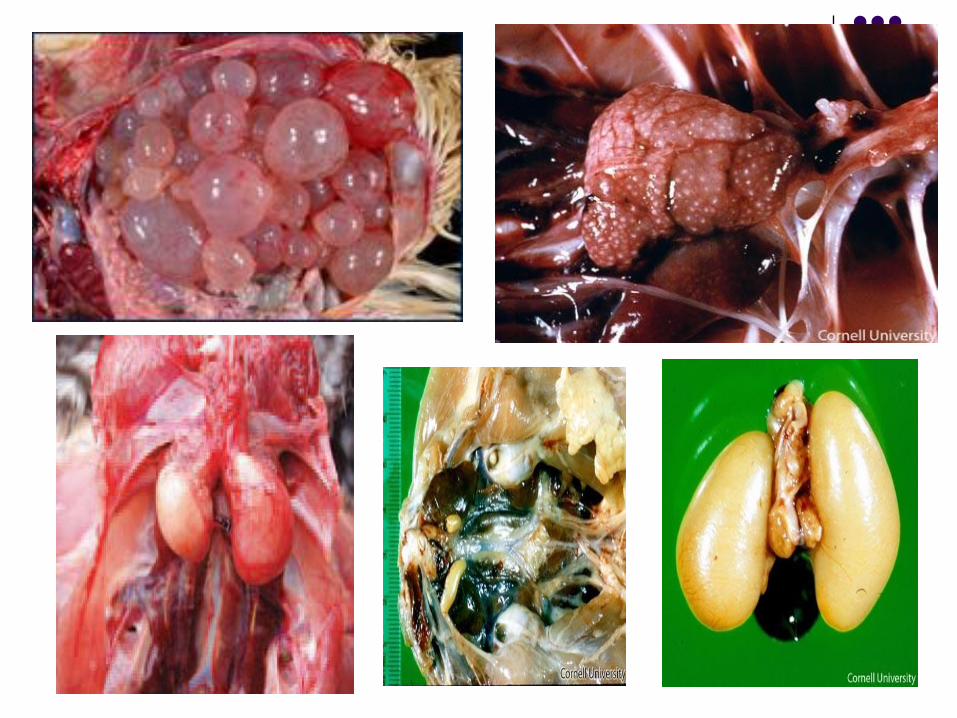
Acute form: Tumors with variable sizes in the liver, spleen,
kidneys, brain, proventriculus, digestive tract,
heart, lungs, gonads, muscles, spinal cord and
dorsal root ganglia.
The ovary showed cauliflower appearance.
Affected organs may show diffuse
enlargement only (5-7 times than normal)
without tumors formation.



Marek's disease tumors in the oropharynx.





Artherosclerosis (fatty proliferation on
vessels of blood vessels on the surface of
the gizzard.
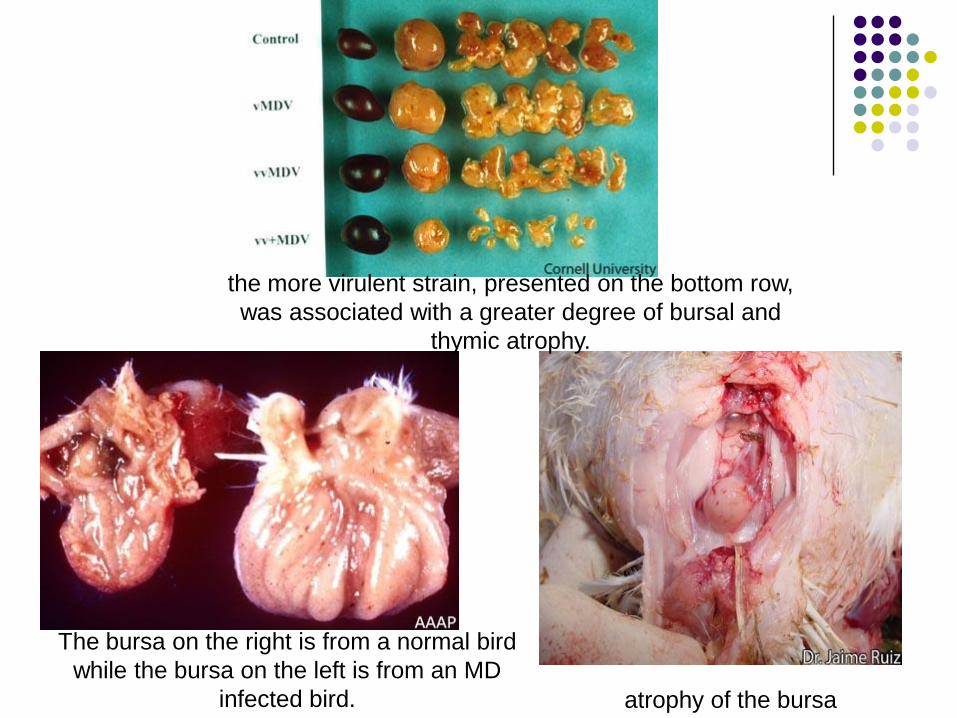
atrophy of the bursa
The bursa on the right is from a normal bird
while the bursa on the left is from an MD
infected bird.
the more virulent strain, presented on the bottom row,
was associated with a greater degree of bursal and
thymic atrophy.

The Bursa on the left has a diffuse tumor
involving several plicae, with focal areas of
necrosis
Tumor in the deep pectoral muscle
Clinical forms
Skin form: Noticed in broiler chickens on postmortem
examination in abattoirs as enlargement of
feather follicles and associated lymphoid
infiltrations.






Clinical forms Transient paralytic form: Occurs in 12–18 weeks old pullets become
paralyzed and may recover with 24 hours if movedto a quiet place.
Peracute form: Occur in 3–5 weeks old chicks; manifested
with sudden death.
Anaemia:• in 3–6 weeks old chicken.

Diagnosis Virus isolation Samples for MD diagnosis:
MDV is highly cell associated therefore, it is important thatthe sample for virus isolation are blood (buffy coat) in acutephase, feather follicles in chronic phase and cellularsuspension of tumor tissues or spleen.
Inoculation of embryonating eggs.
Isolation in cell cultures.
Chicken inoculation.
Isolate identification Immunofluorescent staining with serotype-specific
monoclonal antibodies.
Antigen detection FA test, IP test, AGP test, ELSA, PCR and DNA probes.
Antibody demonstration AGP, FA, ELISA, and VN.
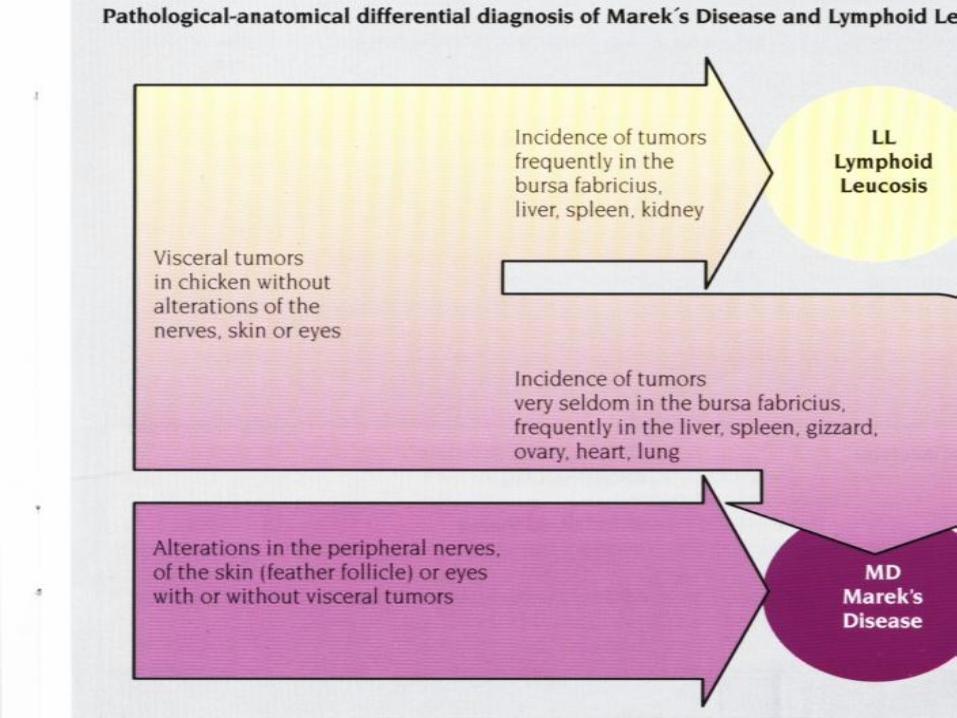
Differential diagnosis
Acute form: Lymphoid leucosis (LL),
Reticuloendotheliosis (REV), avian tuberculosis (ATB),
coligranuoloma and long cystodes infestation.
Neural form: Vit. B2 deficiency (histopathology and
therapeutic treatment) and Neurotoxins.
Eye lesion: Physiological condition.
ND (P/M exam, and virus isolation and identification).
Respiratory diseases (ND, IB and ILT ect..): (P/M
exam, and virus isolation and identification), also no
P/M lesions of MD in respiratory tact (pseudo
respiratory disease).

Immunity1- Immunologic response is probably the basis to
resistance in MD.
2- Vaccinal immunity is the prime means of control.
3- Immunolgic response may contribute to the
cellular mass of lymphoma.
4- MD can be immunosuppressive.
Immunity1- Immune Response of MD: Both humoral and cell
mediated.
In Humoral Immunity; Precipitating and virusneutralizing VN antibodies can be detected within 1-2wks. These antibodies generally persist throughout thelife of the bird.
A humoral antibody response is not required forresistance to MD.
Cell Mediated immunity (CMI); is important. Thepossibility that a surface antigen found on MDVtransformed cells could be involved in immunity(MATSA).
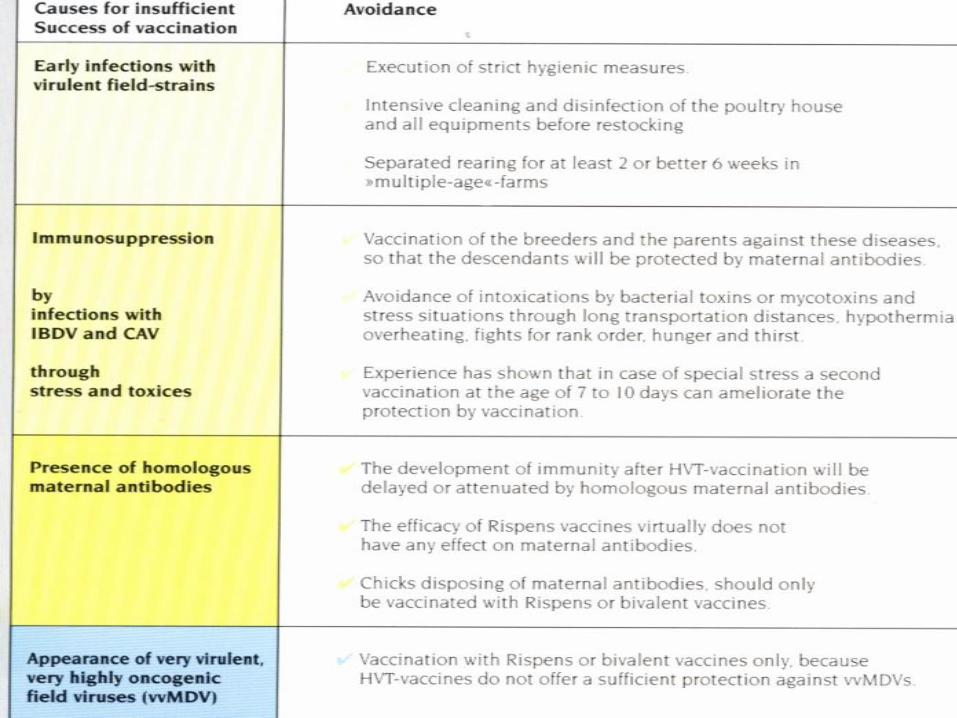
ImmunityVaccinal immunity: Immunity from live vaccine including HVT, attenuated MDV and
serotypes 2 MDV appears.
All protect against early replication of virulent viruses in thelymphoid organs.
TO OVERCOME MATERNAL IMMUNITY:
1. Use of cell-associated vaccine.
2. Increase dose through double vaccination.
3. Increase dose to 10,000 pfu / bird.
4. In-ovo vaccination at 18 days of embryonic life.
5. Vaccination ob breeder with serotype 1 or 2 or1+2 and use serotype 3 for young to avoid HOMOLOGUS antibodies.
Immunity
Immunosuppression: Directly for MDV infection through lytic infection of
lymphocytes.
Indirectly from activity of suppressor cell populations.
The MD tumor cells themselves might have suppressoractivity.
Permanent immunosuppression tends to correlate witheventual tumor development.
Both humoral immunity and cell mediated immunity canbe depressed by MDV infection, So, MDV infection canincrease susceptibility to primary and secondaryinfections.
Prevention & control I- Biosecurity:
Because embryo transmission is unimportant in MD, isolation
rearing and environmental sanitation constitute a primary control
method. Strict biosecurity practices to limit the extent of early MDV
exposure. All-in-All out, avoid multi-age system. Good ventilation.
Avoid Immunosuppressant agents and stress factors.
II-Genetic selection:
Selection programs for resistance have historically been based on
progeny testing or reproduction from survivors of exposed breeding
flocks.
III- Vaccination:
Vaccines based on all three serotypes, mixtures of serotypes and
recombinant DNA vaccine are all capable of protecting chickens
against MD.

Types of MD vaccines
Non pathogenic serotype (2 or 3) [cell free
turkey haemorrhagic virus (THV)].
Attenuated seroyype (1) (cell free).
Cell associated.
Recombinant.
One day old chicks must be vaccinated
against MD by S/C injection or in ovo with
either monovelant or bivelant live vaccine in
dose of 1000 pfu /bird.

Prevention & control Factors affecting efficacy of vaccines:
Age at vaccination:
- At 1 day old and Ovo vaccination.
- Embryo vaccination was advantageous even in the presence
of maternal antibodies.
- The shorter the interval between vaccination and exposure to
the virulent filed virus, the poor the level of protection.
Dose:
- Both cell-associated and cell-free vaccines are given at dose
usually in excess of 1000 plaque forming units (PFU)/chick.
Route of administration:
- The intramuscular route may be slightly more effective than
the subcutaneous route.
Prevention & control Factors affecting efficacy of vaccines:
Genetic resistance:HVT vaccine (in a genetically resistant chicken) providedbetter immunity than did the bivalent HVT + SB-1 vaccine ina susceptible chicken.
Other infections:IBD, RE virus, reovirus and chicken anemia agent or otherimmunosuppressives.
Proper handling of vaccine during thawing andreconstitution.It should be realized that vaccination does not prevent
infection with vvMD virus, but it does protect the birds fromdeveloping the clinical disease if they become exposed.
Vaccinated birds harbor and shed the filed virus if theybecome exposed and thus remain potent source of infectionfor non-vaccinated susceptible birds.