Aviation Ophthalmology. Wg Cdr Malcolm Woodcock RAF Ophthalmology Royal Centre for Defence Medicine. Should we correct the vision of military aircrew surgically?. Wg Cdr Malcolm Woodcock RAF Ophthalmology Royal Centre for Defence Medicine. OR. What about laser eye surgery Doc?. - PowerPoint PPT Presentation
Aviation Ophthalmology Aviation Ophthalmology Wg Cdr Malcolm Woodcock Wg Cdr Malcolm Woodcock RAF Ophthalmology RAF Ophthalmology Royal Centre for Defence Royal Centre for Defence Medicine Medicine
Transcript
Aviation OphthalmologyAviation Ophthalmology
Wg Cdr Malcolm Woodcock Wg Cdr Malcolm Woodcock
RAF OphthalmologyRAF Ophthalmology
Royal Centre for Defence Royal Centre for Defence MedicineMedicine
Should we correct the vision of Should we correct the vision of military aircrew surgically?military aircrew surgically?
Wg Cdr Malcolm Woodcock Wg Cdr Malcolm Woodcock
RAF OphthalmologyRAF Ophthalmology
Royal Centre for Defence MedicineRoyal Centre for Defence Medicine
OROR
What about laser eye What about laser eye surgery Doc?surgery Doc?
IntroductionIntroduction
Vision is the most important sense needed Vision is the most important sense needed for flying for flying
Vision is the only sensory means for Vision is the only sensory means for orientation in spaceorientation in space
Two steps in visionTwo steps in vision– At the eyeAt the eye– In the brainIn the brain
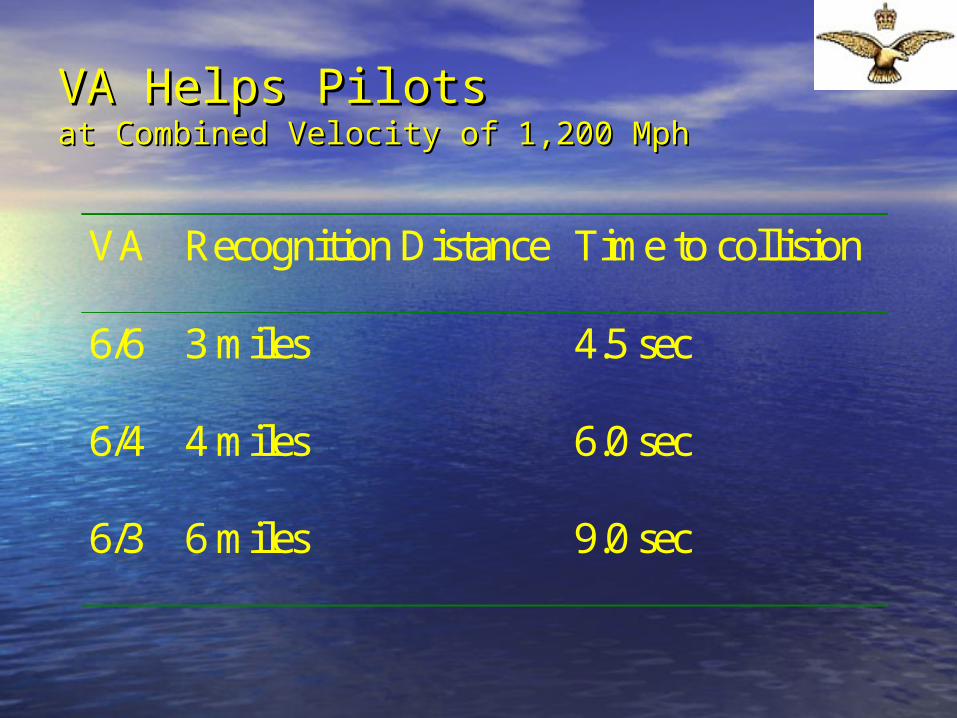
VA Helps PilotsVA Helps Pilotsat Combined Velocity of 1,200 Mphat Combined Velocity of 1,200 Mph
VA Recognition Distance Time to collision
6/6 3 miles 4.5 sec
6/4 4 miles 6.0 sec
6/3 6 miles 9.0 sec
90% thickness90% thicknesskeratotomykeratotomy
Radial keratotomy (RK)Radial keratotomy (RK)
Diurnal variationDiurnal variation Variation with altitudeVariation with altitude RegressionRegression Weakened corneaWeakened cornea Unsuitable for aircrewUnsuitable for aircrew
PainlessPainless– No de-epithelialisationNo de-epithelialisation
Flap loss / damageFlap loss / damage– Ejection riskEjection risk– Trauma riskTrauma risk
Unknown time to flap Unknown time to flap stabilitystability
Retinal detachmentRetinal detachment– Suction ringSuction ring
Sands of SaharaSands of Sahara
LASIK LASIK vs.vs. PRK PRK
Flap decentration of lasikFlap decentration of lasik Raised IOP of lasikRaised IOP of lasik Pain of PRKPain of PRK Equal correction of myopia 1-3 dioptresEqual correction of myopia 1-3 dioptres Lasik more accurate 3-6 dioptresLasik more accurate 3-6 dioptres SE of glare, halos, reduced night visionSE of glare, halos, reduced night vision
– Different proportions but equal effectsDifferent proportions but equal effects
US Navy ExperienceUS Navy Experience
30/30 naval aviators av –3.25d30/30 naval aviators av –3.25d– All achieved 20/20 unaidedAll achieved 20/20 unaided– Glare / halo transient Glare / halo transient – Night vision worse (1 declined other eye)Night vision worse (1 declined other eye)
No effects on NFL of PRKNo effects on NFL of PRK African Americans have excellent outcomesAfrican Americans have excellent outcomes No effect on PRK from ejectionNo effect on PRK from ejection
– NFO S-3B VikingNFO S-3B Viking
Schallhorn SC et al. Preliminary results of PRK in active duty United States Navy personnel. Ophthalmology 1996 Jan;103(1):5-27.
Schallhorn S, Tanzer D, Fulton D. Update on refractive surgery in Naval aviation. Presented at the Aerospace Medical Association 73rd annual meeting, Montreal, Canada, May 2002.
USAF PRK studyUSAF PRK study
80 subjects 20 80 subjects 20 controlscontrols
20% required 20% required correction postopcorrection postop– Aimed for –0.5d Aimed for –0.5d
postop refractionpostop refraction
No effect from altitudeNo effect from altitude No effect from G No effect from G
loadingloading No decrease in HUD No decrease in HUD
readabilityreadability
Tredici T, Ivan D Results and conclusions of the USAF Photorefractive Keratectomy (PRK) study. Presented at the Aerospace Medical Association 73rd annual meeting, Montreal, Canada, May 2002.
Other TechniquesOther Techniques
Clear lens extractionClear lens extraction– For high myopesFor high myopes– Danger of RDDanger of RD
Phakic intraocular lensesPhakic intraocular lenses– May cause lens opacitiesMay cause lens opacities
LASLASEEKK– PRK without the painPRK without the pain
Current State of Play for Civilian Current State of Play for Civilian ApplicantsApplicants JAR class 1 certificationJAR class 1 certification
– Preoperative refraction + 5.00 to -6.00 dioptresPreoperative refraction + 5.00 to -6.00 dioptres– Must be examined by eye specialist at CAA medical Must be examined by eye specialist at CAA medical
div Gatwickdiv Gatwick– 1 year before certification 1 year before certification
JAR class 2 certificationJAR class 2 certification– Preoperative refraction +5.00 to -8.00 dioptresPreoperative refraction +5.00 to -8.00 dioptres– Ophthalmic report about surgery and its results to Ophthalmic report about surgery and its results to
AMEAME– 1 year before certification1 year before certification
Current Pilots – When Can They Fly?Current Pilots – When Can They Fly?
JAR class 1 recertificationJAR class 1 recertification– Must be examined by eye specialist at CAA Must be examined by eye specialist at CAA
medical div Gatwickmedical div Gatwick• Stable refractionStable refraction
– 6/12 to 1 year before certification 6/12 to 1 year before certification
Class 2 recertificationClass 2 recertification– Ophthalmic report about surgery and its Ophthalmic report about surgery and its
results to AMEresults to AME
RAF Refractive Surgery (Currently!)RAF Refractive Surgery (Currently!)
Cost to be borne by the Cost to be borne by the individualindividual
To be performed under To be performed under conditions of strict audit by conditions of strict audit by DMS consultantsDMS consultants
To incorporate latest wavefront To incorporate latest wavefront technologytechnology
Grounded for 6/12-1 year until Grounded for 6/12-1 year until refraction stablerefraction stable
Predominantly affects blue / green discriminationPredominantly affects blue / green discrimination DiseaseDisease
– Macular blue / yellowMacular blue / yellow– Optic nerve red / greenOptic nerve red / green
Drugs Drugs – Inc alcohol, tobacco and OCPInc alcohol, tobacco and OCP– ‘‘Viagra blue’Viagra blue’
Old ageOld age
Electronic Flight Electronic Flight Instrumentation Systems (EFIS)Instrumentation Systems (EFIS)
Increase information Increase information to aircrew through to aircrew through use of coloured use of coloured screensscreens
Use blues and Use blues and yellows as best yellows as best contrasting colours for contrasting colours for normal visionnormal vision
EFIS IssuesEFIS Issues
Effect of colour vision Effect of colour vision defects uncertaindefects uncertain– Colour anomalousColour anomalous– Acquired defects Acquired defects – No research No research
Blue / yellow testing?Blue / yellow testing?– Periodic for acquired Periodic for acquired
defects?defects?
Holmes Wright LanternHolmes Wright Lantern
No longer madeNo longer made Long term replacement neededLong term replacement needed Fletcher CAM test a possibility but not Fletcher CAM test a possibility but not
fully tested or validatedfully tested or validated
ConclusionsConclusions
Medical standards Medical standards required to maintain required to maintain air safety in the face air safety in the face ofof– Changing technologyChanging technology– Changing experienceChanging experience
Wg Cdr Malcolm WoodcockWg Cdr Malcolm Woodcock
Department of OphthalmologyDepartment of Ophthalmology
Worcestershire Royal HospitalWorcestershire Royal Hospital
Defence Consultant Adviser in Ophthalmology Defence Consultant Adviser in Ophthalmology Royal Centre for Defence Medicine Royal Centre for Defence Medicine Selly Oak Hospital Selly Oak Hospital