MEASURING BILLING MEASURING BILLING ACCURACY THROUGH PROBE AUDITS ROY MASATANI, DIRECTOR, COMPLIANCE AUDIT, NATIONAL COMPLIANCE, ETHICS & INTEGRITY OFFICE (NCO), KAISER PERMANENTE MARTINA HEASLEY BA RHIT CPC MARTINA HEASLEY , BA, RHIT , CPC, CCS, AHIMA APPROVED ICD-10-CM/ PCS TRAINER, NCO AUDIT AHIA 31 st Annual Conference – August 26-29, 2012 – Philadelphia PA www.ahia.org
Transcript
MEASURING BILLING MEASURING BILLING ACCURACY THROUGH PROBE AUDITS
ROY MASATANI, DIRECTOR, COMPLIANCE AUDIT, NATIONAL COMPLIANCE, ETHICS & INTEGRITY OFFICE (NCO), N G O C (NCO), KAISER PERMANENTE
MARTINA HEASLEY BA RHIT CPC MARTINA HEASLEY, BA, RHIT, CPC, CCS, AHIMA APPROVED ICD-10-CM/PCS TRAINER, NCO AUDIT
AHIA 31st Annual Conference – August 26-29, 2012 – Philadelphia PAwww.ahia.org
Measuring Billing Accuracy Through Probe Audits
Discussion Topics
Probe Audits
About Kaiser Permanente
Discussion Topics
Target Risk Areas
Background & Purpose
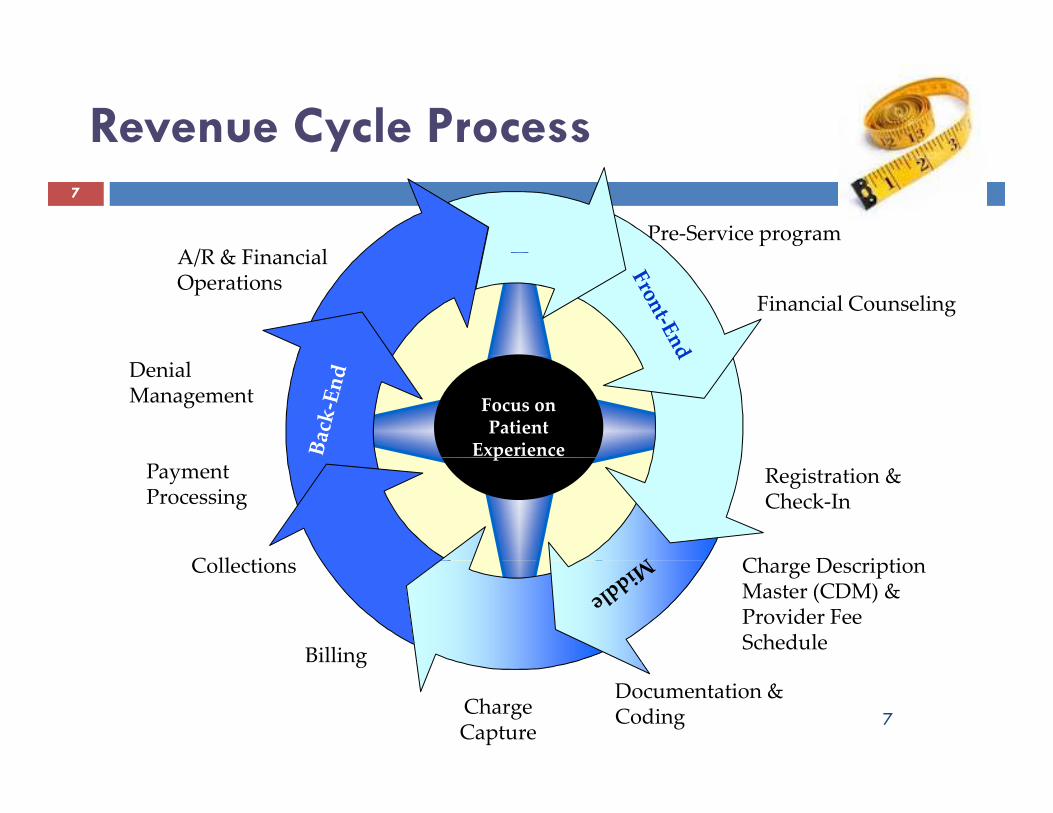
Revenue Cycle Process
Audit Objectives
Clinical Review
Sampling Methodology
Logistics, Timeline, & Schedule
Approach & Scope
Claims Audit
Scoring & Reporting
Comments & Questions
2
About Kaiser PermanenteAbout Kaiser Permanente
Kaiser Foundation Health Plans.Nonprofit, public benefit corporations that contract with individuals and groups for prepaid, comprehensive health care services. The Health Plans contract exclusively with the Permanente Medical Groups and Kaiser Foundation Hospitals for medical and hospital services for members and patients.
Kaiser Foundation Hospitals.Nonprofit, public benefit corporation that owns and operates community hospitals in California, Oregon, and Hawaii; owns outpatient facilities in several states; provides or arranges hospital services; and sponsors charitable, educational, and research activities.
P t M di l GPermanente Medical Groups.Partnerships or professional corporations of physicians, represented nationally by The Permanente Federation, which contract exclusively with the Kaiser Foundation Health Plans to provide or arrange medical services for members and patients to provide or arrange medical services for members and patients.
3
About Kaiser PermanenteAbout Kaiser Permanente
Integrated health care delivery systemIntegrated health care delivery system
Serving 9 states and the District of Columbia
More than 9 million members
533 medical offices
Over 15,800 physicians
36 hospitals and medical centers
Approximately 167,000 employees
44.2 billion annual revenues
4
as of December 31, 2010
Background
With increased federal a diting occ rring thro gh
g
With increased federal auditing occurring through recovery audit contractors (RAC) and others, it is important to be proactive in identifying, correcting, or important to be proactive in identifying, correcting, or preventing documentation, coding, and billing errors.
N l C l h & Off (NCO)National Compliance Ethics & Integrity Office (NCO) was requested by leadership to conduct billing compliance probe audits for professional and hospital compliance probe audits for professional and hospital services to validate billing and reporting accuracy.
5
Purpose p
To establish annual Programwide review in response to To establish annual Programwide review in response to government concerns and market pressures.
To provide base-line assessment of revenue cycle p ycompliance performance across business units.
To present a standardized set of compliance metrics across business units.
To evaluate potential high risk areas identified during l i k t annual risk assessment processes.
Report revenue cycle accuracy that is consistent and Report revenue cycle accuracy that is consistent and comparable across applicable locations/settings.
Provide actionable information for proactive Provide actionable information for proactive operational improvement (i.e. identification of missed opportunities for revenue due to incomplete or pp pinaccurate charge capture, inaccurate paper or electronic claims, etc).
Support Sarbanes-Oxley (SOX) control requirements and reinforce revenue cycle compliance requirements.
8
Approach & Scope
Target and random claims audits will cover, at
Approach & Scope
Target and random claims audits will cover, at minimum, the most recent four months and additional months where available and as necessary.
Claims will be reviewed offsite (remotely) utilizing the standards for 837P electronic forms for professional billing and 837I for hospital billing, where available.
9
Approach & Scope (cont.)
Electronic claims will be obtained and utilized when
Approach & Scope (cont.)
Electronic claims will be obtained and utilized, when available.
Patient statements and related billing information will Patient statements and related billing information will be made available or viewed electronically as needed.
If claims and/or patient statements are not available If claims and/or patient statements are not available in electronic formats, they will be audited utilizing hard copy, paper-based information.py, p p
Observe PHI precautions.
10
Claims AuditsClaims Audits
Two TypesypAUDIT TYPE
DESCRIPTION
TARGETRISKS
Focused audit included review of selected key claims field l t d li i l l t f ifi t t i kRISKS locators and clinical elements for specific target risk areas. Medicare FFS claim selections were based on target risks per OIG, RAC, and other sources. Audit included both professional and hospital services (inpatient and outpatient).
Random audit included review of all high risk (as determined by Revenue Cycle) coding and clinical elements to support SOX requirement.
RANDOMSAMPLES
Claims were selected from all lines of business for professional and hospital services (inpatient and outpatient).
l i d f l d li f
11
Guarantor statements were also reviewed for selected lines of business (financial classes).
Target Risk Areas – Professional Billing (PB) ExamplesBilling (PB) - Examples
New vs. Established Patient Visits.V lid t th t ti t i it d t i d t ti t h h l d • Validate that new patient visit codes were not assigned to patients who have already
had a new patient visit with specialty within previous 3 years.Modifier 25.• Validate accuracy of application of modifier 25 and ensure proper documentation. Validate accuracy of application of modifier 25 and ensure proper documentation. Improper use of modifier creates concern for claims which include E/M codes for services that were not ordinarily identified as significant, separately identifiable, and above and beyond usual care associated with the procedure.
M difi 59Modifier 59.• Validate accuracy of application of modifier 59 (distinct procedural services was performed).
Anesthesia BillingAnesthesia Billing.• Validate that anesthesia services rendered were adequately documented, units correctly reported, and required modifiers accurately applied.
Infusion Administration Codes.
12
• Validate that infusion administration codes (96300-96425) were properly coded and documented including related medications.
12
Target Risk Areas – Hospital Billing (HB) Examples(HB) - Examples
Short Stay.V lid h d i i f 1 d 2 d d b di l d • Validate that admission for 1 and 2 day stays were supported by medical record
documentation.3 Day Rule.• Validate that outpatient hospital diagnostic and non-diagnostic services provided Validate that outpatient hospital diagnostic and non diagnostic services provided within 3 days of an inpatient admission which are related to the admission were appropriately bundled and billed as part of the inpatient admission.
High Risk DRGs (870-872)• Validate that the reported medical severity diagnosis-related group was documented and supported for accurate billing.
Infusion Administration Codes.• Validate that facility related infusion administration codes (related to physician • Validate that facility-related infusion administration codes (related to physician 96300-96425) codes are properly coded and documented including related medications.
1313
Clinical Review for Random or Target AuditsAudits
Clinical staff (i.e. RNs) review claims to evaluate
Scored elements on selected PB samples.Pl f C
( )medical record completeness.
• Plan of Care.• Authentication.• Supervision Requirements.• Orders• Orders.
Scored elements on all HB samples.• Orders for admission, discharge, treatment & medication.
Di h i hi 30 d f di h• Discharge summary within 30 days of discharge.• Authenticated entries with date, time, and signature, written
initials or unique computer logon.• H&P within 30 days prior to or 24 hours after admission.H&P within 30 days prior to or 24 hours after admission.
14
Sampling Methodology
Sample Universe and Claims
Sampling Methodology
pFor TARGET - initial samples of ten claims for each selected inherently high risk area to be expanded to 25 if errors are found HB and PB risks were identified throughfound. HB and PB risks were identified through:• Annual Joint Revenue Cycle, SOX & NCO risk assessment process.
• Clinical Care Delivery toolkit assessments, prior internal and external audit findings and CAPs, and analysis of denial rates for preventable and targeted denials.
For RANDOM - sample of 60 PB claims across all applicable p pplocations, 30 HB inpatient and outpatient claims across all locations, most service types, plus guarantor statements.
Obtain electronic access to patient statements, medical records, and other billing information via partnership with
Resources, Schedules
, g p plocation business units.
Observe PHI precautionsSchedule overlapping location audits based on availability of Schedule overlapping location audits based on availability of coding auditors.Coding auditors perform as both auditors and quality assurance for different location business units.Utilize clinical reviewers judiciously.Non-coding auditors act as coordinators to keep team(s) on g p ( )track.
18
Timeline - SAMPLE
Planning - research location-specific process flow,
Timeline SAMPLE
Planning research location specific process flow, etc. – Week 1 through 8.
Kick off meeting with client partners – Week 2.Entrance conference with client leadership – Week 9.
Plan
Conduct audit and QC results – Week 9 through 12.Vet preliminary observations with client; share
preliminary scores – Week 13 through 16.D t
Review, Evaluate, Test Controls
Exit conference and draft report to – Week 17 through 19.
Comments back from client – Week 22.Fi l t ith CAP t l t W k 24Communicate and
Document Exceptions
Final report with CAP template – Week 24.Completed CAP returned – Week 28.
Report
Resolve
Report
19
Workforce Schedule - SAMPLEPhase I ‐ PLAN & PREPARE: (1) Verify data received, prep tool, codify criteria, train staff, perform walk through or interview regional staff/populate prep questionairre, hold ePhase II ‐ EXECUTE: (2) Conduct audit, clinical review, and QA (for data accuracy and for individuals)Phase III CONCLUDE: (3) Vet results with client update DB draft report and CAP prepare exit slides hold exit conference finalize report and CAP report to leadershipPhase III ‐ CONCLUDE: (3) Vet results with client, update DB, draft report and CAP, prepare exit slides, hold exit conference, finalize report and CAP, report to leadership
Q1 Q2 Q3 Q4FEB
REG AUD QA REG AUD QA B l f A di (3)B l f A di (3)
SEP
PB TARGET AUDIT PB RANDOM AUDITOCTJUL AUG
VVVVVVVVVV
JAN JUNMAR APR
VVVVVVVVVV
MAY2 Auditors & 2 QA
REG AUD QA 60 REG AUD QA 60
REG AUD QA REG AUD QA 120
REG 120 REG AUD QA 120
Bal of Audit (3)
Bal of Audit (3)
HB TARGET AUDIT
Bal of Audit (3)
Bal of Audit (3)
Balance of Audit (3)
AUD QA
VVVVVVVVVVVV2 Auditors &
VVVVVVVVVVVV
HB RANDOM AUDIT
Balance of Audit (3)
REG AUD QA 120
REG AUD QA 120
REG AUD QA 120
REG AUD QA 120
Balance of Audit (3)
HB TARGET AUDIT
Bal of Audit (3)
VVVVVVVVVVVV
2 QA
VVVVVVVVVVVV
HB RANDOM AUDIT
Balance of Audit (3)
Balance of Audit (3)REG AUD QA 120
MA (1)
AUD QA 60
NCL AUD QA 60
Bal of Audit (3)
Bal of Audit (3)
VVVVVVVVVVVV
GS & RA for PB & HB2 Auditors & 2 QA
VVVVVVVVVVVV
Balance of Audit (3)
(1)NCL (1)
AUD QA 60
NW (1)
AUD QA 60
NW (1)
AUD QA 60
Bal of Audit (3)
Bal of Audit (3)
Bal of Audit (3)
VVVVVVVVVV
VVVVVVVVVV
20
Scoring
Random
Scoring
Overall location-specific score and results by category: • Coding information.• Service elements (for example, demographics).• Financial elements.• Medical record completeness . Heat Map
ColorDescription
Green - Meets 95% or above accuracyResults by payor type, place of Green Meets Expectations
95% or above accuracy
Yellow – Needs Attention
80% to 94% accuracy
service, and type of service.Guarantor Statement scoring by
element.Attention
Red –Does not Meet
E t ti
79% or below accuracy
TargetOverall location-specific score and lt b h i k Expectationsresults by each risk.
21
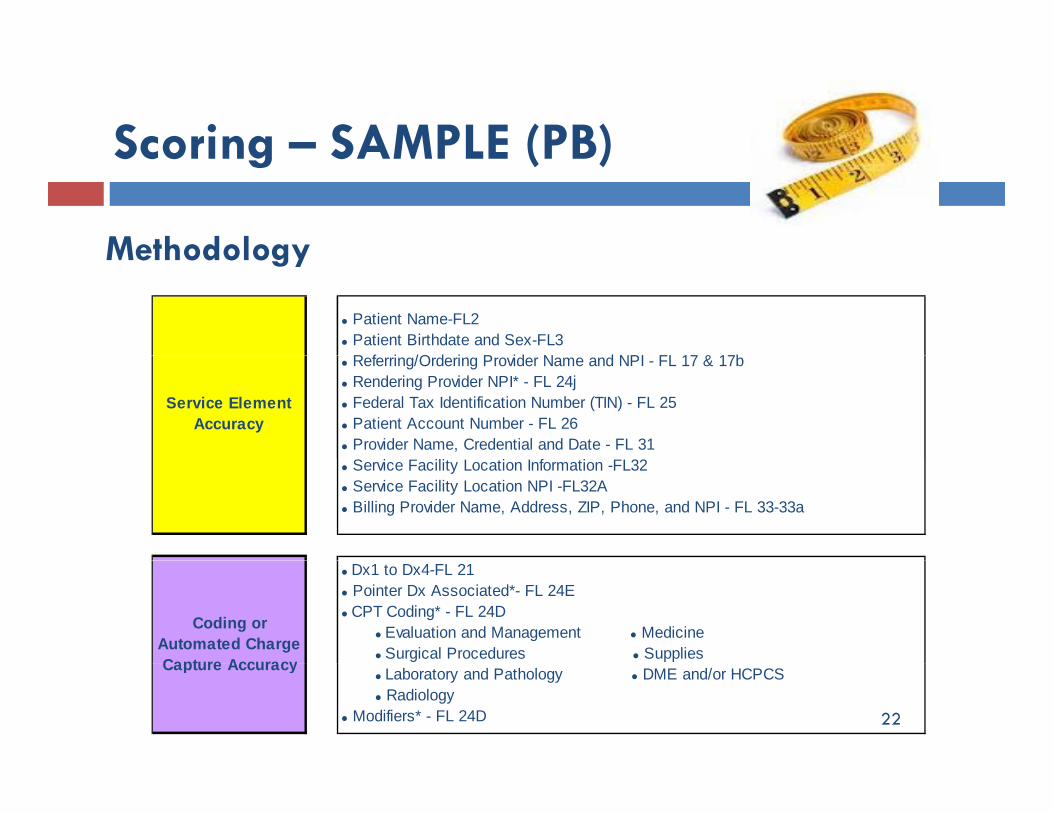
Scoring – SAMPLE (PB)
Methodology
Scoring SAMPLE (PB)
Methodology
• Patient Name-FL2 • Patient Birthdate and Sex-FL3
R f i /O d i P id N d NPI FL 17 & 17b
Service Element Accuracy
• Referring/Ordering Provider Name and NPI - FL 17 & 17b• Rendering Provider NPI* - FL 24j• Federal Tax Identification Number (TIN) - FL 25• Patient Account Number - FL 26• Provider Name, Credential and Date - FL 31• Service Facility Location Information -FL32• Service Facility Location NPI -FL32A• Billing Provider Name, Address, ZIP, Phone, and NPI - FL 33-33a
Coding or Automated Charge Capture Accuracy
• Dx1 to Dx4-FL 21• Pointer Dx Associated*- FL 24E• CPT Coding* - FL 24D • Evaluation and Management • Medicine • Surgical Procedures • Supplies
• Financial Class - FL 1• Patient Medicare Health Insurance Claim (HIC) Number - FL 1a
Financial Accuracy
• Insured Policy Group or FECA Number - FL11 • Date of Illness, Injury or Pregnancy (LMP) - FL 14;• Hospitalization Dates Related to Current Services (from/through) - FL18• Anesthesia Time - FL19• Date(s) of Service* - FL 24A• Place of Service* - FL 24B• Charge for Service* - FL 24F• Days/Units of Service* - FL 24G
Amount Collected from Patient FL 29
Medical Record
• Amount Collected from Patient - FL 29
• Plan of Care• Authentication
23
Medical Record Completeness
• Authentication• Supervision Requirements• Orders with Appropriate Signature
Scoring (cont )Scoring (cont.)
Methodology (cont )
Accuracy Rate per Attribute
Number of Accurate Lines/Claims
Total Number of Applicable Lines/Claims
Methodology (cont.)
Attribute Total Number of Applicable Lines/Claims
Error Rate per Attribute
Number of Incorrect Lines/ClaimsTotal Number of Applicable Lines/Claims
* attribute counted both on the line and claim level.
per Attribute Total Number of Applicable Lines/Claims
Some Field Locators (FL) exist at claim and line item level (e.g. rendering provider NPI), others at claim level only (e.g. patient
24
g p ) y ( g pname) and others at line item level only (e.g. CPT)
RESULTS Target Claims Overall results demonstrated an accuracy rating greater than 95%. Based on the results of the location review, it is our opinion that the billing
compliance controls for target Medicare FFS professional service claims tested Met Expectations. The table below considers all errors. The overall accuracy rate was greater than 95% at both the line and claim levels.
% Line Item
%Claim % Line Item
%Claim % Line Item
%Claim % Line Item
%Claim % Line Item
%Claim
(88 li
Location
Overall
Accuracy RateService Element
AccuracyCoding
AccuracyMedical Record Completeness
Total Lines and Claims
Financial Accuracy
Overall(88 lines,
53 claims) XX% XX% XX% XX% XX% XX% XX% XX% XX%NA
Overall Results, Figure 1
26
Overall Results, Figure 1
Conclude AuditConclude Audit
Discuss Results with ClientsDraft and Final Reports.• Executive Summary.• B k d• Background.• Scope & Objectives.• Opinion.• Summary of Results• Summary of Results.Corrective Action Plan.• Control Objective.
C i i• Criteria.• Deficiencies.• Potential Risks.• R t C• Root Cause.• Recommendation.
27
28
APPENDICES
Claim – Field Locations (PB)
Claim – Field Locators (HB)Claim Field Locators (HB)
Audit Definitions
R f & T lReferences & Tools
Claim Type Field Locators (FL)
CMS 1500
yp ( )30
Demographic
33 fields on CMS 1500.Some fields report
Billi
pdemographics, others are specific to coding & billing.
Required or conditional Billing
Billing Coding
Required or conditional.Some pertain to the whole
claim.
Coding Some pertain to a specific
line item.
30
UB-04 FL
Inpatient - 81 fields on the UB-04; some are the same as CMS 1500 fields and some have no equivalence:
Type of Bill.Type of Admission/Visit. Patient Status. Condition Codes.Occurrence Occurrence Codes/Spans/Dates.Value Codes/Amounts.Revenue Codes.
31
UB-04 FL (cont.)( )
Outpatient: Some fields on the same form are used differently from Inpatient to Outpatient :
Inpatient claims show revenue codes and accommodation rates accommodation rates. Outpatient claims list line items, e.g., ER, Lab, Radiology services, each of which may require HCPCS codes.
Meets Expectations–when taken 4 — Critical Risk Related business or D — Challenging Resolution of exception may be complexMeets Expectations –when taken as awhole, business objective willlikely beachieved, or one or more moderate/modest issues were identified.
4 — Critical Risk –Related business or control objective cannot be achievedwithout resolution of issue;
D — Challenging –Resolution of exception may be complex due to historical culture, significant changes to systems, and/or requires significant redesign of process, which willlikely need a high degree of management attention orsubstantial commitment of resources;
Needs Attention -when taken as a whole,business objective will likely not beachieved or one or more significant /modest issues were identified.
3 — Significant Risk – Remediation of issue would strongly support businessor control objective;
C — Difficult - Resolution of exception may involve culture or structural changes, buy-in from other functional areas and may impact on other processes;
Does not Meet Expectations -when takenas a whole, business objective will notbe achieved, or one or more critical /significant issues
2 — ModerateRisk – Issue presents moderate risk such that related business objective may not be achieved;
B — Medium - Resolution of exception may require business process changes or implementation of control activities andmay require incremental resources;
gwere identified.
1 — Modest Risk – Issue is considered a process deficiency or opportunity, not akey control, but if operating wouldreinforce or supplement other controls.
A — Fair – Resolution of exception is correctable in the normal course of business.
The type of eachfinding is defined as follows:
33
reinforce or supplement other controls. The type of each finding is defined as follows:Design – controls are not designed properly to meet business objectives.Execution – properly designed controls are not operating as intended to meet business objectives.
References & Tools
CMS Claims Processing Manual.
References & Tools
gUB-04 and CMS 1500 data.ED – facility based services apply medical center-specific level setting tool. Audit Database.Eli ibilit V ifi ti S tEligibility Verification Systems.E/M Guidelines (1995 or 1997). National Standards e g ICD-9-CM Official Guidelines for National Standards, e.g. ICD-9-CM Official Guidelines for Coding & Reporting ICD-9-CM Codebook, AHA Coding Clinic, CPT Codebook, CPT Assistant, HCPCS Level II, HCPCS A i Assistant. Claims Editing Software. 34
Save the Date: August 25-28 2013August 25-28, 2013