60
Back to Basics, 2015 POPULATION HEALTH: Infectious Diseases and Outbreak Investigation Dr. Nicholas Birkett School of Epidemiology, Public Health and Preventive Medicine 03/2015 1
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | byron-melvyn-barton |
| View: | 215 times |
| Download: | 1 times |
1
Back to Basics, 2015POPULATION HEALTH:
Infectious Diseases and Outbreak Investigation
Dr. Nicholas BirkettSchool of Epidemiology, Public Health and
Preventive Medicine
03/2015

2
78-5 Outbreak Management (1)
Key Objectives• Know the defining characteristics of an
outbreak and how to recognize one when it occurs.
• Demonstrate essential skills involved in controlling an outbreak and its impact on the public, in collaboration with public health authorities as appropriate.
03/2015
3
78-5 Outbreak Management (2)
Enabling Objectives• Define an outbreak
– An excessive number of cases beyond that usually expected.
• Describe and understand the main steps in outbreak management and prevention.
• Demonstrate skills in effective outbreak management including infection control when the outbreak is due to an infectious agent.
03/2015

4
78-5 Outbreak Management (3)
Enabling Objectives (cont)
• Describe the different types of infection control
practices and justify which type is most appropriately
implemented for different outbreak conditions.
• Demonstrate effective communication skills with
patients and the community as a whole.
• Describe appropriate approaches to prevent or reduce
the risk of the outbreak recurring.
03/2015

5
78-5 Outbreak Management (4)
Enabling Objectives (cont)• Understand key features of communicable
diseases• Understand communicable disease
epidemiology
03/2015

6
78-5 Outbreak Management (5)
• Physicians are crucial participants in the control of outbreaks of disease.
• Must be able to • Diagnose cases
• Recognize outbreaks
• Report these to public health authorities
• Work with authorities to limit the spread of the outbreak.
• Common example• Assist in the control of an outbreak of influenza or
diarrhoea in a nursing home03/2015

7
Infectious Disease Summary
• Terminology• Nature of diseases• Outbreaks/epidemics
– Identification– Methods of control
03/2015

803/2015
903/2015
Foodborne• Botulism• Clostridium perfringens• Hepatitis A• Norovirus• Salmonellosis• Shigellosis• Staphylococcal disease• Trichinosis
Water & Foodborne• Amebiasis• Cholera• Giardiasis• Legionellosis• E coli
Person-to-person spread• Aseptic meningitis• Hepatitis B and C• Respiratory Infections
(e.g., influenza)• Herpes simplex• Streptococcal disease• Tuberculosis• Leprosy
Infections: Sources and agents (1)

1003/2015
Arthropod Borne• Encephalitis (West Nile)• Lyme Disease• Malaria• Plague• Rocky Mountain Spotted
Fever
Sexually Transmitted• HIV/AIDS• Gonorrhea• Syphilis• Chlamydia trachomatis
Vaccine preventable• Chickenpox• Diphtheria, pertussis,
tetanus• Hepatitis A and B• HPV• Influenza• Measles, mumps, rubella• Meningococcal• Pneumococcal• Poliomyelitis
Infections: Sources and agents (2)
Zoonotic• Psittacosis• Q fever• Rabies• Hantavirus• West Nile
Fungal• Candidiasis• Coccidioidomycosis• Histoplasmosis
Prions• Kuru• vCJD

11
Terminology (1)• Infectivity
– The ability of an agent to invade and multiply in a host (an infection).
– Dose of organism required to establish infection in 50% of animals.
• Pathogenicity– The ability of an agent to produce clinically apparent illness.
• Pathogen– Infectious and non-infectious substances capable of producing
tissue damage or initiating a process which can lead to a disease.
03/2015

12
Terminology (2)• Virulence
– The proportion of clinical cases which produce severe disease and/or permanent sequelae.
• Immunogenicity– The ability of an agent to produce specific immunity against the
agent– Can be produced in general body or within specific sites such as
the GI tract.– Determines the ability of an agent to re-infect the same host
• e.g. measles vs. gonorrhea
03/2015

13
Terminology (3)• Reservoir
– Living organisms or inanimate matter in which infectious agent normally lives and multiplies
• Fomites (Vehicle)– Inanimate objects contaminated with infectious agent (not
the reservoir).• E.g. toys in a daycare center.
03/2015

14
Terminology (4)• Vector
– An animate source of an infectious agent. • The vector may be infected with the organism (e.g. mosquitoes and
malaria) or just be a mechanical carrier (e.g. flies). • Usually insects or small mammals such as rodents.
• Zoonoses– Diseases transmitted to humans from animals (e.g. anthrax)– Do they develop human-to-human spread
• Bird flu
03/2015

15
Terminology (5)• Emerging Infectious Disease
– An infectious disease where the incidence in humans has increased in the past 2 decades or threatens to increase in the near future (CDC)
– Complex set of diseases and contributing conditions• Habitat destruction• War • Famine • Poverty • Climate change• Genetic Drift
03/2015

16
Terminology (6)• Carrier
– An infected person without apparent clinical disease who remains infectious (e.g. Typhoid Mary)
• Index Case– The first case to be diagnosed in an outbreak– Sometimes defined as the first case noticed in the outbreak
• Contacts– People who have possibly been infected due to relevant
contact with an infectious case
03/2015

17
Terminology (7)
• Attack Rate– The probability that people will get ill from the disease.
Usually applied in an outbreak situation.
03/2015
18
Terminology (8)
• Secondary Attack Rate– Similar to ‘attack rate’ but excludes the index case(s).
Formula is:
03/2015

19
Terminology (9)
• Case Fatality Rate (CFR)– The probability of death in people with an
infection.
03/2015

2003/2015

2103/2015

2203/2015

23
Pathogenic Mechanisms (1)
• Direct Tissue Invasion (Group A Strep)• Production of Toxins (Diphtheria)• Allergic Host Reaction • Resistant/latent infection (carriers)• Enhancement of host susceptibility to drugs
(e.g. Reye’s syndrome and ASA).• Immune Suppression
03/2015

24
Reservoirs (examples of transmission patterns)
• Human Human Human
• Animal Animal Animal
Human
03/2015
Vector
Animal
Vector
Human
2503/2015

26
Virulence
• Parasite borne diseases are usually more virulent
• Spread by direct contact requires an alive and active host
• Agents often lose virulence as an epidemic passes– Ebola (previous epidemics)– Virulent strains kill host and don’t spread
03/2015

27
Epidemics (1)• Epidemic
– Now often called an ‘outbreak’, especially if localized– The occurrence (in a community or region) of a
disease/condition/behaviour clearly in excess of normal expectancy
– Public’s reaction/view differs from technical definition
• Pandemic– An epidemic covering a very wide area and affecting a
large proportion of the population– Controversial definition
• Consider H1N1 outbreak
03/2015
28
Epidemics (2)• Endemic
– the occurrence of a disease/condition at a relatively constant level in a given setting, usually with on-going transmission
03/2015

29
Epidemics (3)
• Conditions increasing likelihood of an epidemic– Agent conditions
• Introduction of a new pathogen
• Increased amount of a pathogen
• Change in the virulence of a pathogen.
– Population conditions• An adequate number of exposed and susceptible persons.
– An effective means of transmission between the source
of the pathogen and the susceptible person.
03/2015

30
Epidemics (4)
• Types of epidemics– Common source
• Point source• Ongoing exposure• Need not be geographically localized
– Propagated/progressive– Mixed
• Epidemic curve• Spot maps• Note that epidemics can arise from behaviour as well as from
traditional infectious sources.
03/2015

31
Epidemic Curves: point source (1)
03/2015

32
Epidemic Curves: propagated (2)
03/2015
10 days
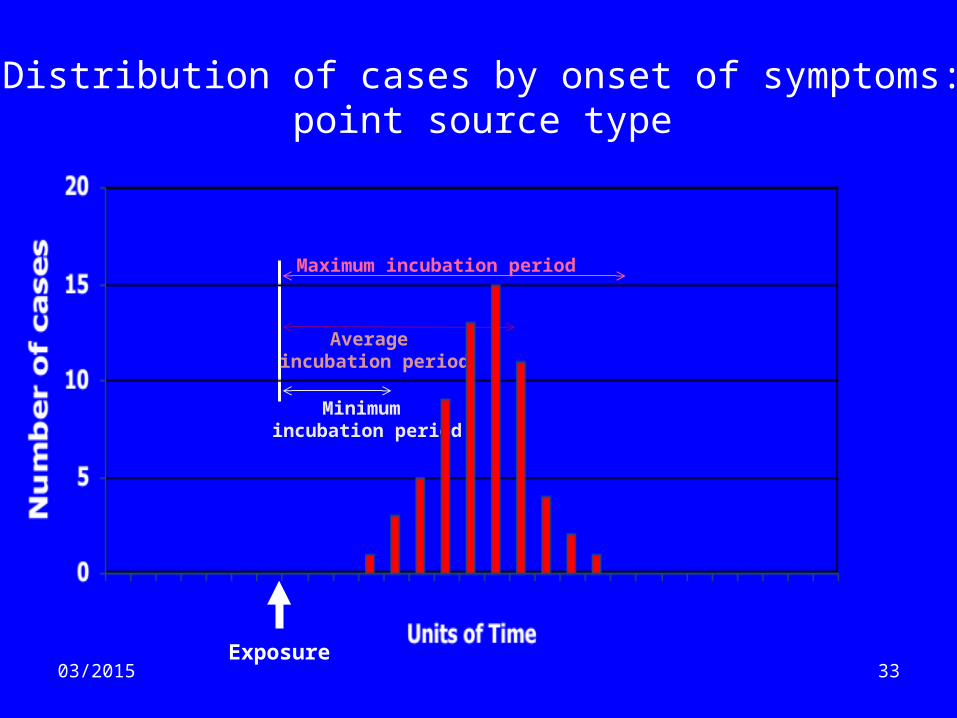
3303/2015Exposure
Maximum incubation period
Average incubation period
Minimum incubation period
Distribution of cases by onset of symptoms:point source type

3403/2015
Exposurebegins & continues
Distribution of cases by onset of symptomsPoint source, Continuous exposure type

3503/2015

3603/2015

37
Factors Influencing Spread of Disease in a Population (1)
• Period of infectivity in relationship to symptoms– Includes consideration of carrier states
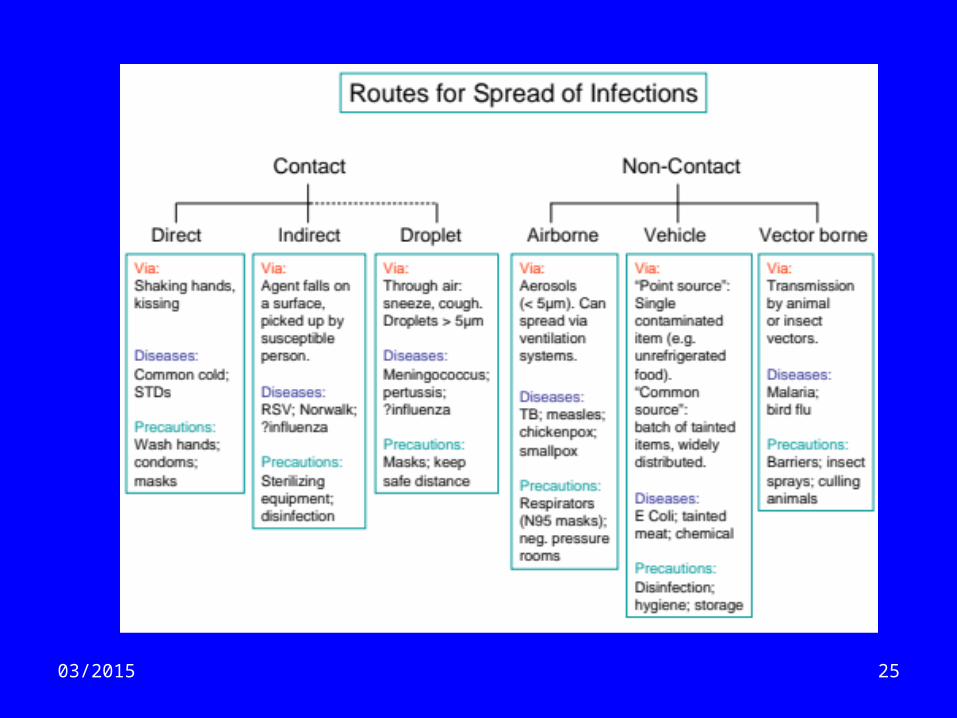
• Herd immunity• Type of spread
– Direct– Indirect– Airborne
• Transmission mechanics– Consider sexual vs. droplet spread
03/2015

3803/2015
Develop disease
Immune
Herd Immunity

39
Outbreak Control (1)
• Twin goals:– Minimize the impact to the affected community– Understand the cause and mode of transmission
• Goals can conflict:– Need to take action in absence of full information– Need to collect full information base
03/2015

40
Outbreak Control (2)
• Establish the diagnosis– Clinical examination– History, especially of exposure to:
• other sick people• travel• agents
– Laboratory testing• Rapid response vs. definitive tests
• Determine pattern of spread– Type of outbreak– Epidemiological study of exposures ‘in common’, etc.
03/2015
41
Outbreak Control (3)
• Effective and clear communication with general public is essential– Designate one spokesperson– Regular press briefings– Lessons from the SARS outbreak
03/2015

42
Outbreak Control (4)
• General strategies for addressing outbreaks– Reduce host susceptibility– Interrupt Transmission of the Agent
• Strategies can be useful for– Controlling an active outbreak– Preventing the onset of an outbreak
03/2015

43
Outbreak Control (5)
• Reduce host susceptibility– During an outbreak
• Immunization (active and passive)
– Before an outbreak, or during a long outbreak• Nutrition• Improve living conditions• Improve other social determinants of health
– A large part of the reason that infectious outbreaks are now so uncommon
03/2015

44
Outbreak Control (6)• Interrupt Transmission of the Agent
– Identify source of outbreak and remove it– Quarantine/isolation– Case treatment– Contract tracing
03/2015

45
Outbreak Control (7)• Interrupt Transmission of the Agent (cont)
– Food inspections– Environmental clean-up– Animal population control
• Rabies vaccination of wild animals
– Insect spraying• Monitor for animal infections
03/2015

46
Outbreak Control (8)• Isolation
– Applies to propagated epidemics– Deals with people who are already ill– Separate the infectious persons or animals from
others during the period of communicability– Usually isolate for at least two incubation periods– If incubation period is unknown
• Try and estimate it based on transmission patterns• Be conservative
03/2015

47
Outbreak Control (9)• Quarantine
– Applies to propagated epidemics– Places restrictions on the activities of well people
who (may) have been exposed to a communicable disease during its period of communicability.
– Quarantine for the longest usual incubation period– Often at least two incubation periods.– ‘active surveillance’ is an alternative
03/2015

48
Outbreak Control (10)• Quarantine (cont)
– More controversial than isolation since it affects people who are not currently ill (and may never get ill).
– We expect some people who are quarantined to get sick
03/2015

49
Outbreak Control (11)
Immunization• Passive or active• Passive can be more useful for acute outbreak control
Chemoprophylaxis• Treat people with disease• Preventive use of antibiotics for people exposed
– tuberculosis– meningococcal infection
03/2015

50
Outbreak Control (12)
Harm Reduction (for long term outbreaks)• Focus on prevent adverse effects from harmful
exposures– Needle exchange– Safe Injection sites
Inactivate agent• water purification; chlorination
03/2015

51
Outbreak Control (13)
Contact tracing• Done by the Public Health Department• Applies to diseases with person-to-person spread
– Especially STIs
• A ‘contact’– Someone who interacted with the index case in
such a way that they may have become infected
• Need to treat every ‘contact’
03/2015

52
Outbreak Control (14)
Contact tracing (cont)• Index case is given chance to contact his/her
‘contacts’• If that doesn’t happen, PHU can take proactive action
and contact cases• For TB, PHU takes the lead in
– contact tracing– Ensuring preventive treatment using Directly
Observed Treatment methods.
03/2015
53
Outbreak Control (15)
Personal hygiene measures• hand hygiene (#1 strategy)• cough etiquette• protective clothing (masks, gowns)• avoid at risk situations
Family/community measures• preventing sexual abuse of children leads to reduction in STIs• Needle exchange and related programmes.
03/2015

54
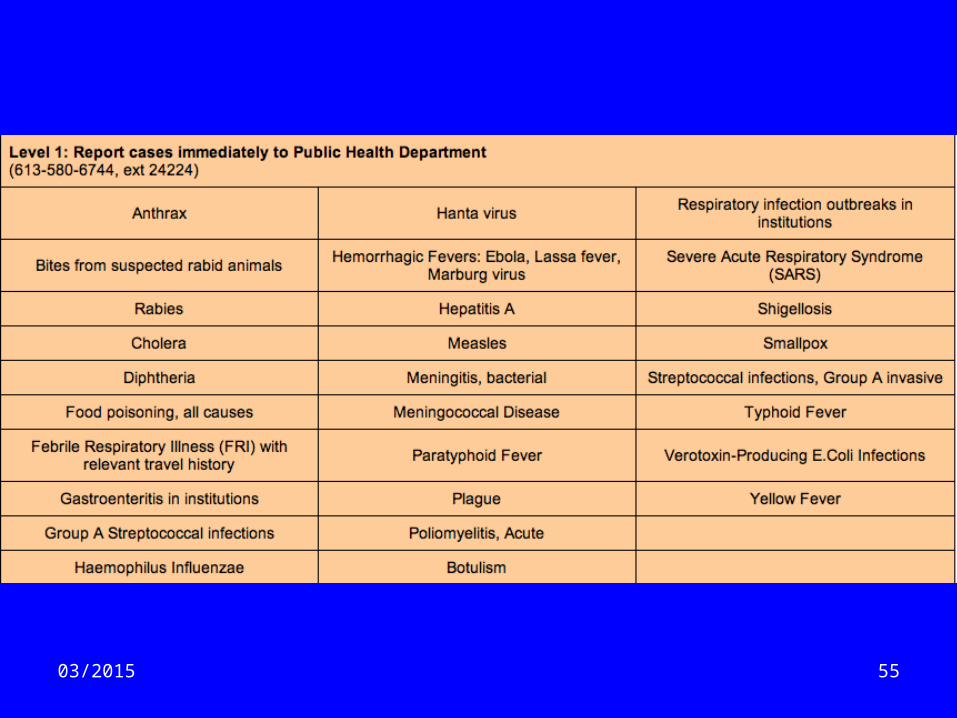
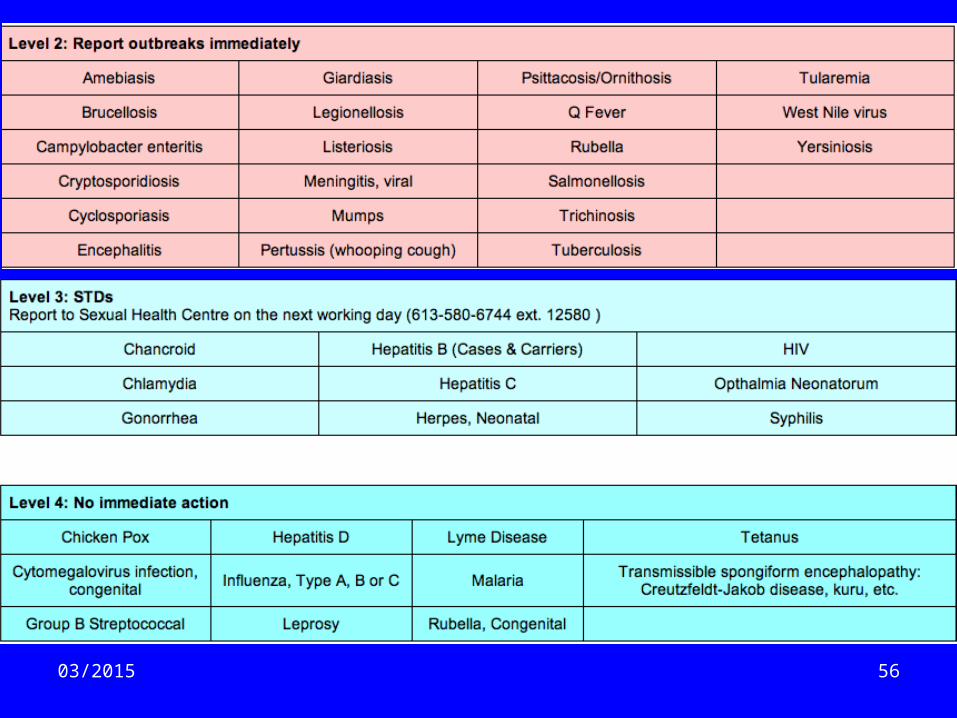
Surveillance (1)The continuing scrutiny of all aspects of occurrence and spread of disease that are pertinent to effective control• Reportable diseases.
– legal obligation to report designated diseases to local public health department
– list includes (among many others)• AIDS• food poisoning• encephalitis• STIs• influenza• Lassa fever• SARS• plus many more
03/2015
5503/2015
5603/2015

#1


59
Surveillance (2)The continuing scrutiny of all aspects of occurrence and spread of disease that are pertinent to effective control
• Reportable diseases.• Sentinel practices• Animal/water surveys• Environmental monitoring• Mortality (vital statistics)• Provincial laboratory tests• Epidemic investigations• Disease registries• CIHI and related data.03/2015

6003/2015

















