Preliminary results of RCHOP in the treatment of DLBCL R. Tissir A.Quessar, M.Rachid, S. Benchekroun hematology and oncology department in 20 Août 1953 Hospital, university center IBN Rochd Casablanca Morocco
Transcript
Preliminary results of RCHOP in the treatment of DLBCL R. Tissir A.Quessar, M.Rachid, S. Benchekroun hematology and oncology department in 20 Août 1953 Hospital, university center IBN Rochd Casablanca Morocco
Background Diffuse large B-cell lymphoma (DLBCL) is the most commonly
occurring lymphoma in the Western world. It’s account for about one-third of all lymphomas in adults
DLBCLs are clinically, biologically, and pathologically heterogeneous with biologically distinct subtypes that have different expected treatment outcomes.
The rituximab has been registered in Europe since 1998. since the introduction of rituximab (RCHOP) in TTT of DLBCL a revolutionary improvement in treatment outcome was achieved, especially in the low risk group according to IPI.
In our unit the RCHOP become the standard of TTT since 2009
Treatment strategies for patients with diffuse large B-cell lymphoma: Blood and Lymphatic Cancer: Targets and Therapy 2012:2 87–98
Purpose
To analyze the outcome of patients with DLBCL treated
by RCHOP regimen in our unit
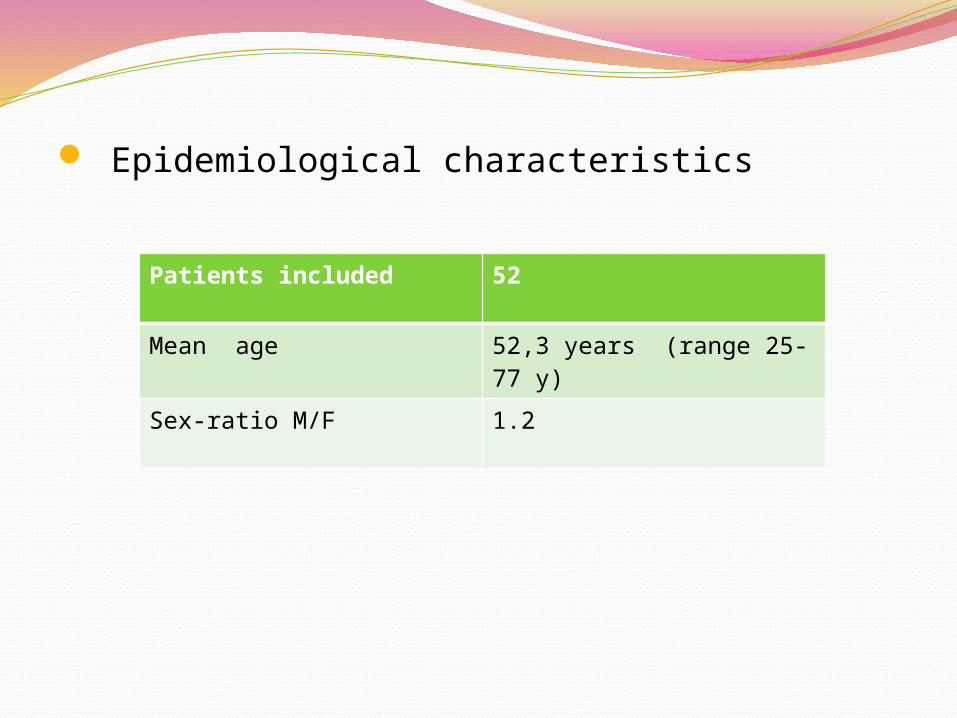
Patients and Methods Population:
- Newly diagnosed untreated patients with nodal DLBCL aged ≥18y, who received a minimal of 3 RCHOP21. during the period from Novembre 2009 until June 2011 (20months)
The diagnosis :
- on the basis of excisional lymph node or tissue biopsy according to WHO criteria 2008
Staging comprised clinical examination, thoracic and abdominal computed tomography scans
Bone marrow biopsy
Patients and methods CBC,routine blood chemistry LDH, protein electrophoresis , renal and
liver function
Echocardiography in patient with a history of cardiac disease or older
Viral screening test : HVC,HVB,HIV
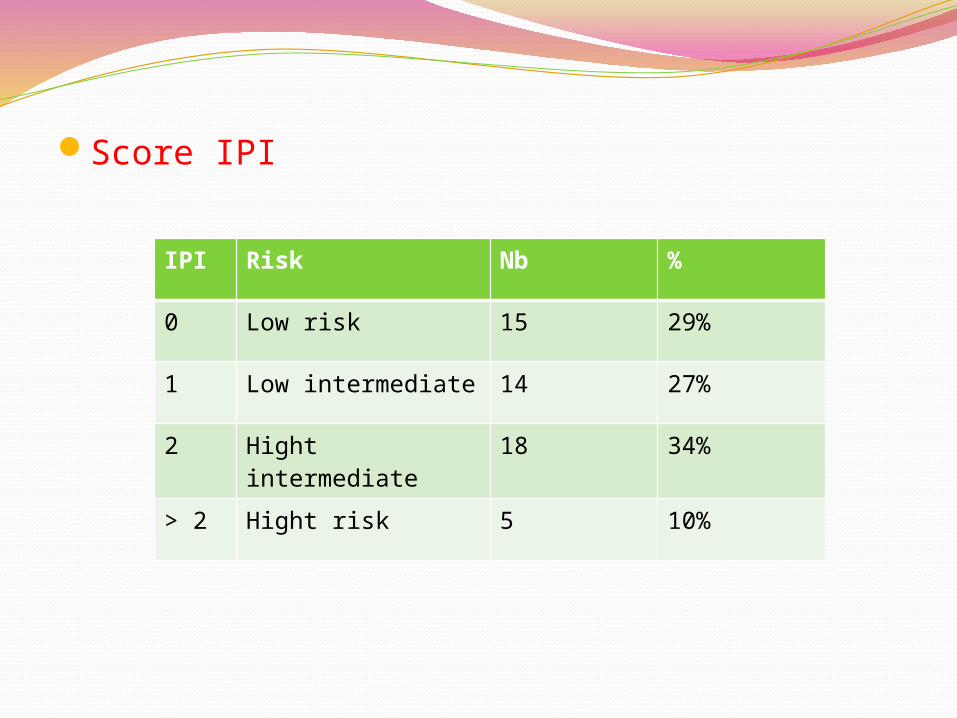
Prognostic factor according IPI , aaIPI
The response evaluation :abnormal radiological tests at baseline were repeated after 3to 4 cycles and after the last cycle of treatment, the bone marrow biopsy was repeated in the end of TTT if initially involved
The OS and EFS were performed by Kaplein Meyer method
Data were analyzed using Epi info system.
Patients and methods patients were excluded : - extranodal localisation, - less than 3 RCHOP - TTT CHOP
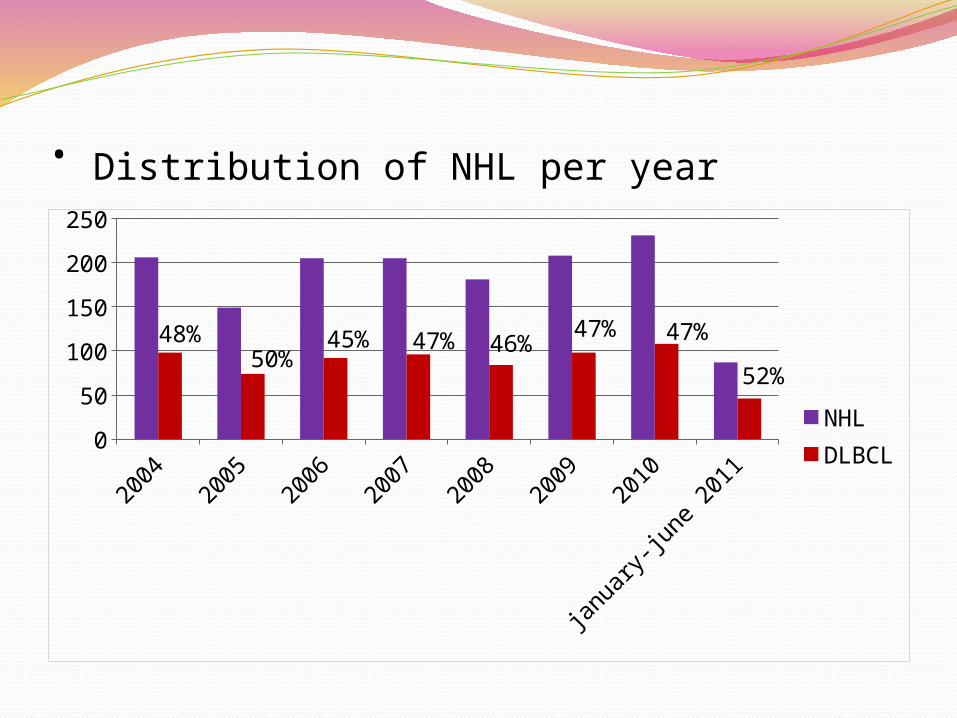
• Distribution of NHL per year
2004
2005
2006
2007
2008
2009
2010
janu
ary-
june
201
10
50
100
150
200
250
48%50%
45% 47% 46%47% 47%
52% NHLDLBCL
169 patients were assigned from Nov 2009 until june2011
- 83 nodal 49% : 12 CHOP 19 lost befor TTT 52 RCHOP - 86 extranodal




















![Lymphoma - ISD Scotland · [DLBCL/Burkitts Lymphoma] MYCDATE Date (DD/MM/CCYY) 10 15 MYC Testing Result [DLBCL/Burkitts Lymphoma] MYCRESULT Integer 2 16 Location of Diagnosis {Cancer}](https://static.documents.pub/doc/80x56/5fe202d4c67e945f1a036fa7/lymphoma-isd-scotland-dlbclburkitts-lymphoma-mycdate-date-ddmmccyy-10-15.jpg)















