42
BAD transmission & SAD distribution: who is today a no-option CLI patient? Vincenzo Foppa, 1462 “The miracle of the salvaged foot” Cappella Portinari, S. Eustorgio Church Milan, Italy

BAD transmission & SAD distribution: who is today a no-option CLI patient?
Vincenzo Foppa, 1462“The miracle of the salvaged foot” Cappella Portinari, S. Eustorgio Church Milan, Italy

Disclosure
In the last 2 years I have the following potential conflicts of interest to report:
Consultant: Medtronic, Abbott, Boston Scientific, Contract Medical International, Cook, Asahi, Ivascular, Biotronic, Limflow, Spectranetics, Shire, Kardia, Astra Zeneca, Orbus, Bard
Virtual shareholder: Limflow
Roberto Ferraresi, MD
In 2005, in an audit of the BASIL trial sites, approximately 50% of all SLI patients were still considered not revascularizable by either surgery or angioplasty, and were treated conservatively
The definition changes according to the available techniques in a certain era and place. We lack a consensus on the definition of no-option CLI patient!
Who is today a no-
option CLI patient?
In 1912 – no angio, no bypass, no angioplasty - every patient with supposed CLI was, by definition, a no-option one
1. PAD pattern: traditional background
2. What is the outflow foot vessels?
3. SAD & CLI: the true no-option pts

13,827 pts admitted to The
Methodist Hospital in Houston for
the treatment of arterial
atherosclerotic occlusive disease
from 1948 to 1983
1° key article 1985

“atherosclerotic lesions often tend
to be segmental and fairly well
localized, with relatively normal
proximal and distal arterial beds.
Such atheromas are usually
located in the proximal and/or
midproximal portions of the
arterial bed”
1° key article 1985

Less commonly, the
arteriosclerotic process occurs
predominantly in the distal
portion of the arterial bed…
1° key article 1985

We have identified a subset of individuals where
the tibial vessels were extensively diseased but
the dorsalis pedal artery was spared.
…. we will rely on intubation of the distal lumen
[of DPA] with a small 22-gauge angiocatheter and
gently inject heparinized balanced salt solution. If
flow is easy we will proceed. High resistance to
injection or inability to inject contraindicates
bypass placement.
High resistance to injection in DPA excluded
2° key article 1990
No-patent DPA pts excluded

Association of risk factors with the level of atherosclerotic target lesions. Red overlay on the
anatomic cartoon illustrates the association of risk factor with pattern of atherosclerotic lesions
3° key article 2006

4° key article 2007
Modified by Graziani L et Al.: Eur J Vasc Endovasc Surg 2007;33:453-60


Foot vessel disease was not considered: pts with foot vessel disease were excluded from proper diagnosis and often from active treatment options!




Vascular surgery & peripheral angioplasty were born to fight against large vessels disease in middle age pts, however today we must face an epidemic of old/diabetic/ESRD pts with a different pattern of PAD!
“The times they are a-changing’…”

1. PAD pattern: traditional background
2. What is the outflow foot vessels?
3. SAD & CLI: the true no-option pts

What is the outflow of foot arteries?
Foot arteries are the border between twodifferent diseases in terms of biology and clinical evolution: Big Artery Disease (BAD) & Small Artery Disease (SAD)

3 big foot arteries:• Dorsalis pedis• Lateral plantar• Medial plantar

Small arteries: all the branchesarising from the main arteries• Arch• Metatarsal• Calcanear• Digital
This is the final outflow of the inferior limb vascular tree!

Edmonds et al. raised the question if ischemic foot disease could
be explained by one disease (atherosclerosis), or by the
occurrence of 2 diseases (diabetic macroangiopathy [SAD] and
classical atherosclerosis [BAD]). They concluded that “the
detailed nature of PAD in diabetes has not been fully defined. Of
course, in a diabetic patient, particularly a patient who develops
arterial disease in later life, both diseases may co-exist”.
I am not the
only one!


1915 pts with symptomatic PAD
183 claudicants 1732 CLI pts
9.8
45.5
46.3
Prox
BTK
Dist
BTK
BTA
vessels
Arch 25,1
Prevalence of disease (%)
P-TPT
SFA
ATG
Aggregated segments
0 artery 14.31 artery 24.32 arteries 37.73 arteries 23.7
0 artery 13.21 artery 25.52 arteries 44.93 arteries 16.4
0 artery 27.91 artery 20.22 arteries 31.53 arteries 20.4
> 50% 2-3 foot BAD
25% arch disease = SAD

ATG
BTK
BTA
vessels
Arch
Aggregated segments
ATK
Female Sex Hypertension Tobacco smoke
Patients’ Age Underweight subjects Diabetes Dialysis Status

BAD-Patient 1
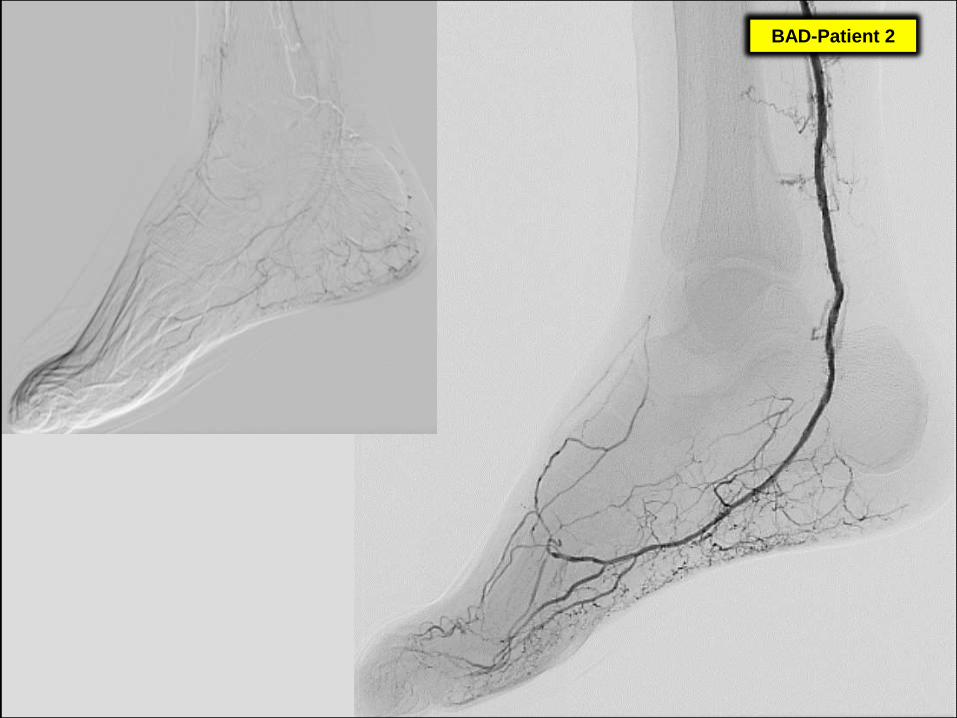
BAD-Patient 2

BAD-Patient 3

BAD-Patient 4

In BAD-patients outflow is good!
Revascularization can arrive at a
healthy foot distribution system Patient 4 BAD
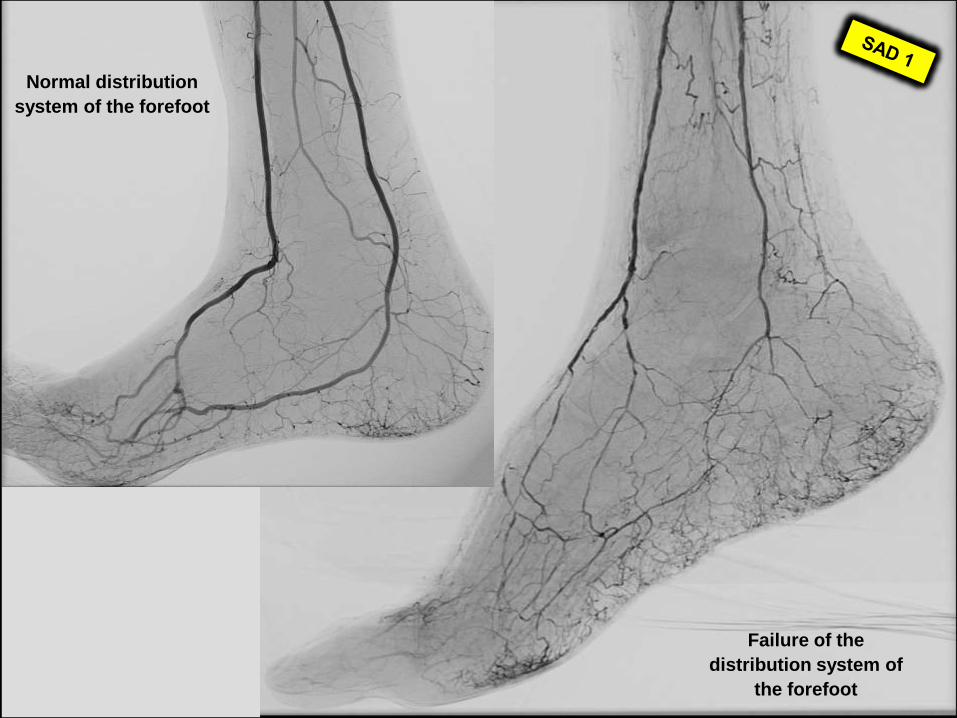
Normal distribution
system of the forefoot
Failure of the
distribution system of
the forefoot


Normal distribution
system of the forefoot
Failure of the
distribution system of
the forefoot


In the majority of the cases
SAD is an expression of
MAC (medial artery
calcification)

In the vast majority of the
cases SAD is an untreatable
disease, either surgically or
percutaneously, and is able
to jeopardize the fate of the
leg (and of the patient!)

1. PAD pattern: traditional background
2. What is the outflow foot vessels?
3. SAD & CLI: the true no-option pts

0.51 (0.29 - 0.89)
0 artery ref.1 artery 1.7 (0.76 - 3.83)2 arteries 1.86 (0.72 - 4.83)3 arteries 4.84 (1.12 - 20.88)
0 artery ref.1 artery 1.69 (0.74 - 3.87)2 arteries 5.81 (1.91 - 17.62)3 arteries 5.71 (1.03 - 31.78)
Any of BTA and Arch
13.25 (1.69 - 104.16)
0.53 (0.26 - 1.1)
1.17 (0.68 – 2.01)
Prox
BTK
Dist
BTK
BTA
vessels
Arch
P-TPT
SFA
ATG
Aggregated segments
Risk factors for CLIOdds Ratio (95% CI)

CLI

CLI

1. Our data suggest that FAD, and particularly SAD, could play a
crucial role in CLI and should be considered as a crucial target (or
limit) for revascularization strategy.
2. It is remarkable to note that the most common test worldwide
applied in detection of PAD, the ABI, is unable to reveal FAD, and
that CT & MR-angiography are rarely extended and reliable in
detecting FAD.
3. Based on this study, we should consider inappropriate to perform a
proper clinical assessment and revascularization strategy in CLI
patients without a complete angiographic evaluation of FAD &
particularly SAD.

A no-option CLI pt is a pt with advanced SAD!
Who is today a no-
option CLI patient?
BAD transmission & SAD distribution: who is today a no-option CLI patient?
Vincenzo Foppa, 1462“The miracle of the salvaged foot” Cappella Portinari, S. Eustorgio Church Milan, Italy

















