Rambam Health Care Campus and Technion, Haifa, Israel Rebecca Lopez-Alonso, Tania Mashiach, Elinor Barzilai, Michal Weiler-Sagie, Eldad J. Dann Should a bulky mediastinal mass measuring >7 cm be considered an adverse prognostic factor in patients with advanced Hodgkin lymphoma and a negative interim PET/CT ? “Humani nihil a se alienum putabat” “Nothing of humanity was foreign to him”
Transcript
Rambam Health Care Campus and Technion,
Haifa, Israel
Rebecca Lopez-Alonso, Tania Mashiach, Elinor Barzilai, Michal Weiler-Sagie, Eldad J. Dann
Should a bulky mediastinal mass measuring >7 cm be considered an adverse prognostic factor in
patients with advanced Hodgkin lymphoma and a negative interim PET/CT ?
“Humani nihil a se alienum putabat”
“Nothing of humanity was foreign to
him”
• The introduction of PET/CT in the staging and treatment evaluation algorithm changed the concept of therapy for many patients with advanced Hodgkin disease (HD).
• In the German HD9 study for advanced HD, 71% of patients (pts) were treated with radiation therapy (RT) for the initial mass measuring ≥5 cm.
• In the HD15 study, only 11% of pts underwent RT, i.e., those with a residual mass of ≥2.5 cm and a positive PET/CT at the end of therapy.
• This dramatic change in the strategy was demonstrated to be successful in terms of progression-free survival (PFS) in pts treated with 6 cycles of escalated BEACOPP (EB).
• However, the validity of this approach excluding RT from the management of pts receiving a less intensive regimen based on interim PET results is unclear. The GITIL study, the intergroup study and the H2 study omitted RT to a bulky mediastinal mass. But is there a cutoff that marks an increased risk for thoracic mediastinal mass?
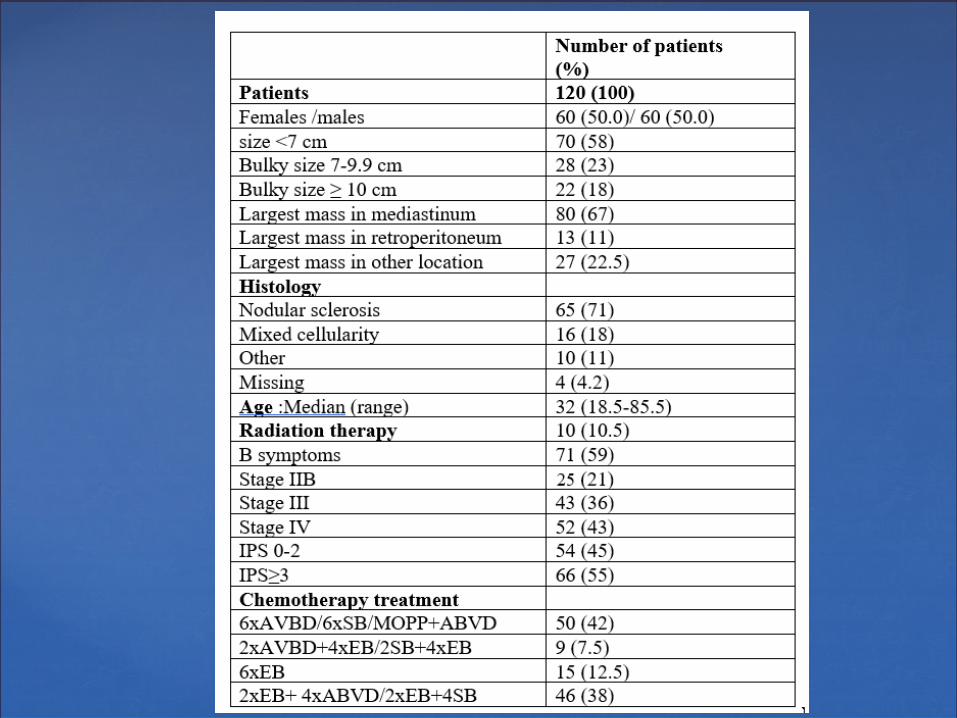
• The current analysis included patients with stage IIB III/IV HD treated between 2001-2010 who underwent baseline CT or PET/CT.
The current study has evaluated if a bulky disease is an adverse prognostic factor in patients receiving the
following treatment regimens:
•Initiation with escalated BEACOPP and its adjustment to ABVD or standard BEACOPP, based on negative interim PET/CT.
•Initiation with ABVD therapy and its up-grading to escalated BEACOPP based on positive interim PET/CT.
•Omitting radiation therapy based on the end-of-therapy negative PET/CT.•We assessed the relapse rate of patients with mass 0-7 , 7-9.9,≥ 10 cm
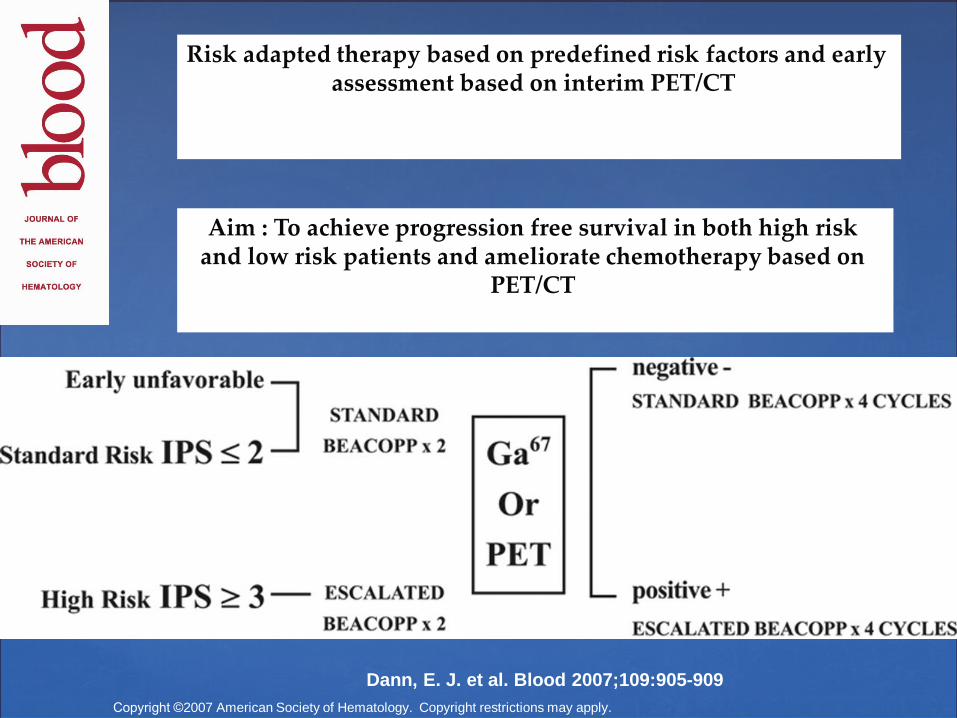
Risk adapted therapy based on predefined risk factors and early assessment based on interim PET/CT
Aim : To achieve progression free survival in both high risk and low risk patients and ameliorate chemotherapy based on
PET/CT
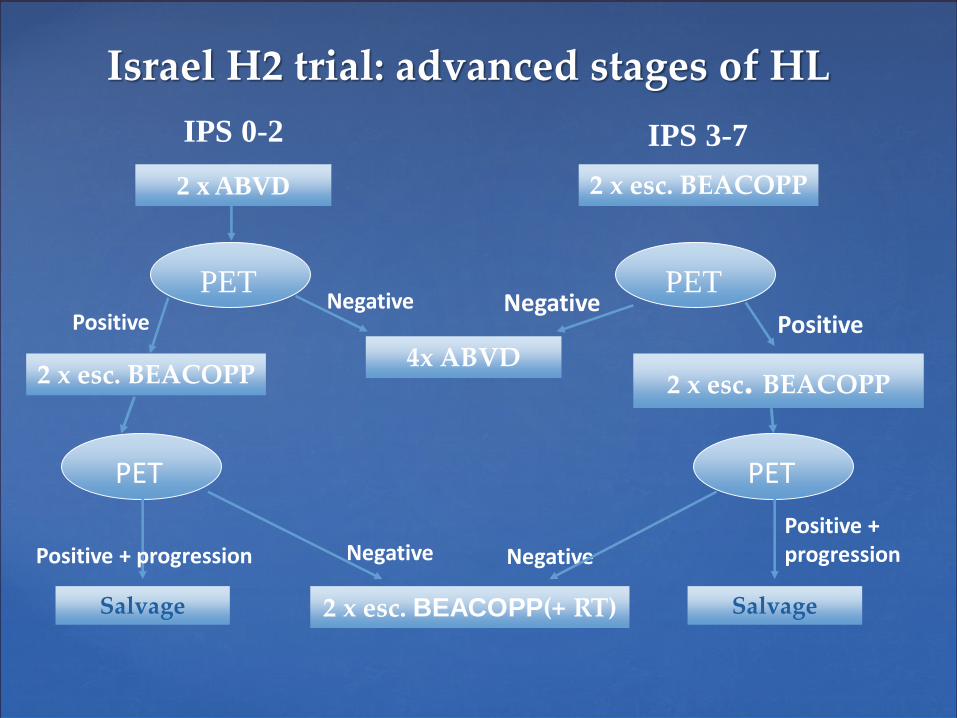
Israel H2 trial: advanced stages of HL
2 x ABVD
IPS 0-2
PETNegative
Positive
2 x esc. BEACOPP
PETNegative
Positive
2 x esc. BEACOPP
PET
Negative
2 x esc. BEACOPP
PET
Negative
2 x esc. BEACOPP(+ RT)
Positive + progression
Salvage
Positive + progression
Salvage
4x ABVD
IPS 3-7
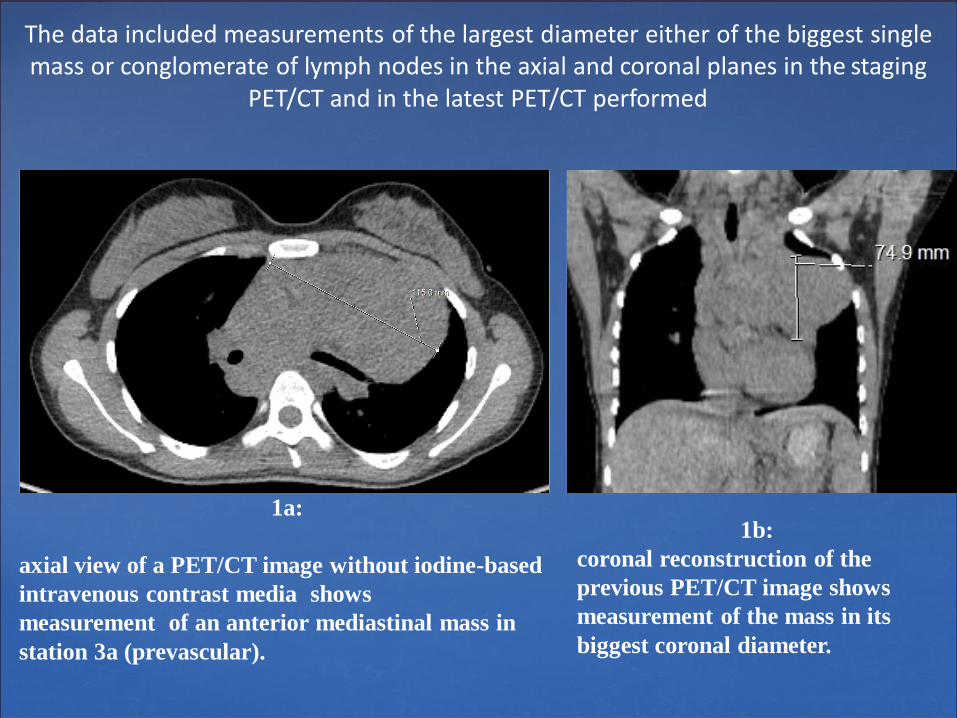
The data included measurements of the largest diameter either of the biggest single mass or conglomerate of lymph nodes in the axial and coronal planes in the staging
PET/CT and in the latest PET/CT performed
1a:
axial view of a PET/CT image without iodine-based
intravenous contrast media shows
measurement of an anterior mediastinal mass in
station 3a (prevascular).
1b:
coronal reconstruction of the
previous PET/CT image shows
measurement of the mass in its
biggest coronal diameter.
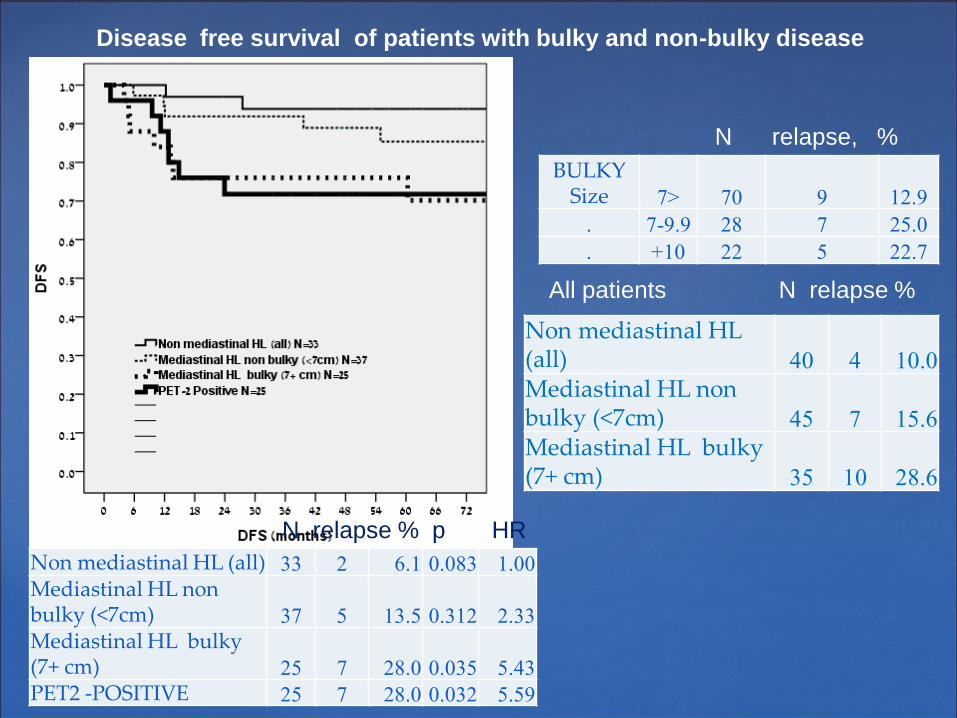
Disease free survival of patients with bulky and non-bulky disease
BULKY Size <7 70 9 12.9
. 7-9.9 28 7 25.0
. 10+ 22 5 22.7
Non mediastinal HL (all) 40 4 10.0
Mediastinal HL non bulky (<7cm) 45 7 15.6
Mediastinal HL bulky (7+ cm) 35 10 28.6
All patients N relapse %
Non mediastinal HL (all) 33 2 6.1 0.083 1.00
Mediastinal HL non bulky (<7cm) 37 5 13.5 0.312 2.33
Mediastinal HL bulky (7+ cm) 25 7 28.0 0.035 5.43
PET2 -POSITIVE 25 7 28.0 0.032 5.59
N relapse % p HR
N relapse, %
Multivariate Cox regression analysis and 5-y DFS±SE
P value Adjusted 95.0% CI for HR 5-y DFS±SE
HR Lower Upper
3 factors
Non-mediastinal HL
(all)
0.083 1 0.938±0.04
Mediastinal HL,
non-bulky (<7cm)
0.312 2.33 0.45 12.01 0.85±0.06
Mediastinal HL,
bulky (7+ cm)
0.035 5.43 1.13 26.14 0.69±0.1
PET2 -POSITIVE 0.032 5.59 1.16 26.96 0.71±0.09
For patients with IPS ≥ 3, treatment
was initiated with escalated BEACOPP
IPS ≥ 3
For patients with IPS 0-2 treatment
was initiated with ABVD
IPS 0-2
Pts Events %
IPS 0-2.
.
.
Non-mediastinal HL (all) 14 2 14.3
Mediastinal HL, non-bulky (<7cm) 17 2 11.8
Mediastinal HL bulky (7+ cm) 15 6 40.0
PET2 -POSITIVE 8 1 12.5
. Other 66 10 15.2
IPS 3+.
.
.
Non-mediastinal HL (all) 19 0 0.0
Mediastinal HL, non-bulky (<7cm) 20 3 15.0
Mediastinal HL, bulky (7+ cm)
10 1 10.0
PET2 -POSITIVE 17 6 35.3
Conclusions
Masses located in the mediastinum, measuring more than 7 cm in any of the planes, have a negative prognostic effect; thus, the cutoff of 7 cm can be used to describe bulky disease in the mediastinum.
The location of the mass has shown to be a prognostic factor: bulky masses (>7 cm) located in the mediastinum are associated with a 5-time increase in the risk of progressive disease (HR 5.4, p=0.03).
Positive interim PET has an HR for progression of 5.59, p=0.03
The relapse rate in patients with thoracic bulky disease >7 cm is substantially reduced if therapy is initiated with EB.
These findings are awaiting more extensive evaluation in a much larger cohort of patients.