16
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | noreen-peters |
| View: | 217 times |
| Download: | 0 times |

Behavioral Health: Challenges and Opportunities in Indian Country
Pamela S. Hyde, J.D.SAMHSA Administrator
National Indian Health Board (NIHB)Board Meeting
Washington, DC • January 24, 2012

FOCUS AREAS FOR TODAY’S DISCUSSION
BUDGET UPDATE & REVISED APPROACH GRANT-MAKING
PREVENTION CHALLENGES: SUICIDE & HEART DISEASE
PREVENTION: SUICIDE & HEART DISEASE
TLOA UPDATE & INAGUARAL NEWSLETTER
SAMHSA REGIONAL ADMINISRATORS
3

BUDGET UPDATE
Promising news: SAMHSA ↓ ~1% while others saw sharp cuts
• The 1% reduction = strategic and creative decisions to sustain
Disappointing news: proposed new BH-TPG not funded
• A multi-year non-competitive award in the amount of $50K to prevent substance abuse and suicide
SAMHSA still fielding inquiries from tribal communities asking when the RFA will be out this year – w/o appropriation from the ACA Prevention Fund, SAMHSA isn’t able to support the program
4
REVISED APPROACH TO GRANT-MAKING
Braided funding within SAMHSA & with partnersEngaging with States, Territories & Tribes
• Funding for States to plan or sustain proven efforts• Requiring/encouraging work with communities
Revised BG application • Tribal impact:
• In Section G: Tribal Consultation - States must show evidence tribal consultation was part of planning process
• Tribes will not have to waive sovereignty in order to receive BG funds/services
• Must include a copy of suicide prevention plan - if no plan then must demonstrate how one will be developed
5

SAMHSA’S STRATEGIC INITIATIVES
AIM: Improving the Nation’s Behavioral Health (1-4)AIM: Transforming Health Care in America (5-6)AIM: Achieving Excellence in Operations (7-8)
1. Prevention
2. Trauma and Justice
3. Military Families
4. Recovery Support
5. Health Reform
6. Health Information Technology
7. Data, Outcomes &
Quality
8. Public Awareness &
Support
6

PREVENTION CHALLENGES AI/AN COMMUNITIES
Higher adolescent death ratesHigher past month binge alcohol useHigher past month illicit drug useHigher sexual assault rates against femalesHigher homicide rates against women Higher rates of intimate partner violence against womenHigher rates of incarceration and arrestHigher rates of historical traumaHigher youth suicide ratesHigher rates of heart disease
7
1.Prevention
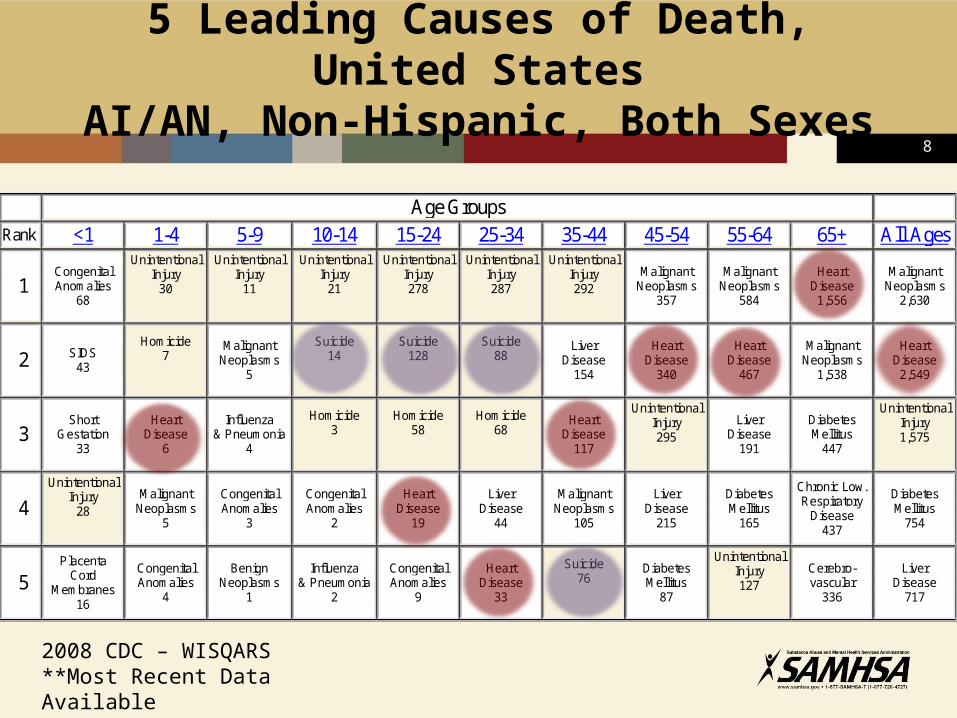
5 Leading Causes of Death, United StatesAI/AN, Non-Hispanic, Both Sexes
Age Groups
Rank <1 1-4 5-9 10-14 15-24 25-34 35-44 45-54 55-64 65+ All Ages
1
Congenital Anomalies
68
Unintentional Injury
30
Unintentional Injury
11
Unintentional Injury
21
Unintentional Injury 278
Unintentional Injury 287
Unintentional Injury 292
Malignant Neoplasms
357
Malignant Neoplasms
584
Heart Disease 1,556
Malignant Neoplasms
2,630
2
SIDS 43
Homicide 7
Malignant Neoplasms
5
Suicide 14
Suicide 128
Suicide 88
Liver Disease
154
Heart Disease
340
Heart Disease
467
Malignant Neoplasms
1,538
Heart Disease
2,549
3
Short Gestation
33
Heart Disease
6
Influenza & Pneumonia
4
Homicide 3
Homicide 58
Homicide 68
Heart Disease
117
Unintentional Injury 295
Liver Disease
191
Diabetes Mellitus
447
Unintentional Injury 1,575
4
Unintentional Injury
28
Malignant Neoplasms
5
Congenital Anomalies
3
Congenital Anomalies
2
Heart Disease
19
Liver Disease
44
Malignant Neoplasms
105
Liver Disease
215
Diabetes Mellitus
165
Chronic Low. Respiratory
Disease 437
Diabetes Mellitus
754
5
Placenta Cord
Membranes 16
Congenital Anomalies
4
Benign Neoplasms
1
Influenza & Pneumonia
2
Congenital Anomalies
9
Heart Disease
33
Suicide 76
Diabetes Mellitus
87
Unintentional Injury 127
Cerebro- vascular
336
Liver Disease
717
2008 CDC – WISQARS**Most Recent Data Available
8

http://millionhearts.hhs.gov9
NATIONAL ACTION ALLIANCE FOR SUICIDE
PREVENTION A public-private partnership established in 2010 to revise and
advance the National Strategy for Suicide Prevention (NSSP)
Leadership: • John McHugh, Secretary of the Army• Former Senator Gordon H. Smith, Pres/CEO, Nat’l Assoc of Broadcasters
Vision: The National Action Alliance for Suicide Prevention envisions a nation free from the tragic experience of suicide
Priorities: • 1: Update/implement the Surgeon General’s NSSP by 2012• 2: Public awareness and education• 3: Focus on suicide prevention among high-risk populations
10
10

NATIONAL ACTION ALLIANCE FOR SUICIDE
PREVENTION 11

AI/AN SUICIDE PREVENTION ACTIVITIES
Next steps being considered by BIA, BIE, IHS and SAMHSA re: suicide prevention and lessons learned from last year’s regional listening sessions and the two Action Summits for suicide prevention (Phoenix & Anchorage) – report coming soon
One of the Action Summit workshops on the use epidemiological data to prevent suicide grew out of a workgroup consisting of Tribal and State representatives that was facilitated by SAMHSA’s CAPT
SAMHSA’s Office of Behavioral Health Equity is planning a 2-day BH institute in conjunction with the American Indian Higher Education Consortium Student Conference (Rapid City) - March
• Focus: National dialogue on BH in tribal college setting
• Focus: How students and faculty can promote BH in their communities
12
UPDATES - TLOA SECTION 241SAMHSA HAS LEAD TO:
Create and staff a SAMHSA Office of Indian Alcohol and Substance Abuse (OIASA)
• Director’s position: Interviews held, decision soon Develop a MOA with Justice, Interior and HHS
Secure operating framework for a Tribal Action Plan (TAP)
• SAMHSA’s Collaborative for the Application of Prevention Technologies (CAPT)
• Native American Center for Excellence (NACE) Support for Tribes Pursuing Tribal Action Plans under the Tribal Law and Order Act
• Tribal Action Plan Guidelines 2011
Establish Inventory/Resource Workgroup
Establish an Education Services Workgroup
Seek Tribal Leader input (consultation)
Establish Newsletter Workgroup
13
NEWSLETTER WORKGROUP LAUNCHES FIRST ISSUE
Published quarterly
Includes reviews of exemplary alcohol/SA programs
Provides valuable information and circulated w/o charge
Interagency Council will work together to disseminate the newsletter electronically in order to reach schools, tribal offices, BIA regional offices and agencies, IHS area and service unit offices, IHS alcohol programs, and other entities serving AI/AN
Available on the new SAMHSA IASA website, www.samhsa.gov/tloa
14

REGIONAL ADMINISTRATORS
• Region I: BostonA Kathryn Power M. Ed.
• Region II: New YorkDennis O. Romero
• Region III: PhiladelphiaJean Bennett
• Region IV: AtlantaStephanie McCladdie
• Region V: ChicagoJeffrey A. Coady, Psy.D
• Region VI: DallasMichael Duffy RN, BSN
• Region VII: Kansas CityLaura Howard, JD
• Region VIII: DenverCharles Smith, Ph.D.
• Region IX: San FranciscoJon Perez, PhD.
• Region X: SeattleDavid Dickinson
Among first activities for RAs - HHS Regional Consultation Sessions
RAs to communicate SAMHSA’s message and to convey BH challenges and successes from the field to headquarters
15

SAMHSA’S CONTINUED FOCUS
People - NOT moneyPeople’s lives - NOT diseasesSometimes focus so much on a
disease/condition we forget people come to us with multiple diseases/conditions, multiple social determinants, multiple cultural attitudes
It’s a public health issue!Behavioral health is essential to
health!
16

















