. he Dr Anusha Vohra PH1.19-Antidepressants and Antimanic drugs Objectives Should be able to � Classify antidepressants and enumerate them. � Describe their mechanism of action, adverse effect and clinical uses. � Describe the advantages and disadvantages of SSRIs. � Explain what are SNRIs and atypical antidepressant and their important characteristics. DEPRESSION DEPRESSION � Reactive depression:- Psychotherapy alone or with antidepressants. � Endogenous depression:- Antidepressants alone or with electroconvulsive therapy (ECT). � MDP (bipolar depression):-Lithium, antidepressants and antipsychotics, with or without ECT. Limbic system Increased DA activity Depletion of NA &/ 5HT Increased NA activity Schizophrenia Behavioural Depression 1 Schizophrenia (Psychosis) (psychosis/neur osis) Mania
Transcript
.
he
Dr Anusha Vohra
PH1.19-Antidepressants and Antimanic drugs
ObjectivesShould be able to � Classify antidepressants and enumerate them.� Describe their mechanism of action, adverse
effect and clinical uses.� Describe the advantages and disadvantages of
SSRIs.� Explain what are SNRIs and atypical
antidepressant and their important characteristics.
DEPRESSION
DEPRESSION� Reactive depression:- Psychotherapy alone or
with antidepressants.� Endogenous depression:- Antidepressants
alone or with electroconvulsive therapy (ECT).� MDP (bipolar depression):-Lithium,
antidepressants and antipsychotics, with or without ECT.
Limbic system
Increased DA activity
Depletion of NA &/ 5HT
Increased NA activity
Schizophrenia
Behavioural Depression
(psychosis/neur Mania
1
Schizophrenia (Psychosis)
(psychosis/neurosis)
Mania
.
Pathophysiology of depressionMonoamine hypothesis
Mechanism Of Action� Monoamine hypothesis
� Neurotropic hypothesis
� Neuroendocrine hypothesis
Classification
1. Reversible inhibitors of MAO-A (RIMAs)� Moclobemide, Clorgyline
MONOAMINE OXIDASE (MAO) � MAO catalyze deamination of intracellular
monoamines� Two types Of MAO enzyme:-
� MAO-A� MAO-B
2
Vortioxetine, Vilazodone6.Selective NA reuptake inhibitor: Atomoxetine
.
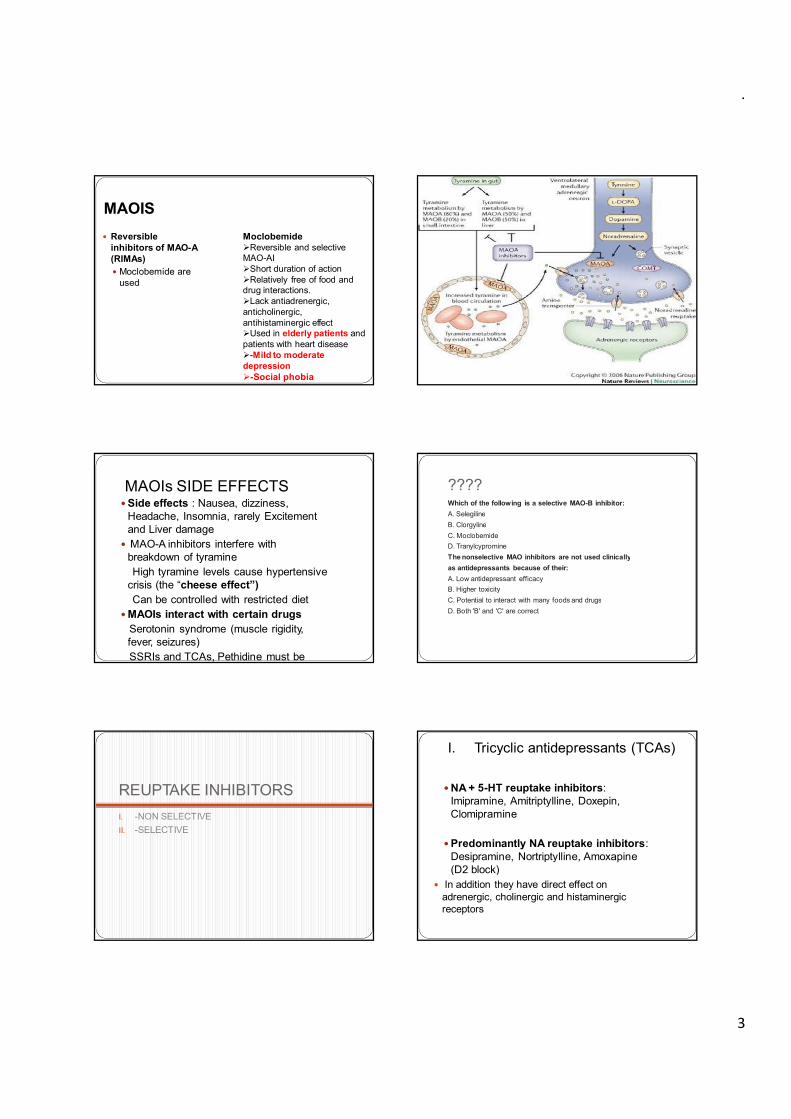
MAOIS� Reversible
inhibitors of MAO-A (RIMAs)� Moclobemide are
used
Moclobemide�Reversible and selective MAO-AI�Short duration of action�Relatively free of food and drug interactions. �Lack antiadrenergic, anticholinergic, antihistaminergic effect�Used in elderly patients and patients with heart disease�-Mild to moderate depression�-Social phobia
MAOIs SIDE EFFECTS�Side effects : Nausea, dizziness,
Headache, Insomnia, rarely Excitement and Liver damage
� MAO-A inhibitors interfere with breakdown of tyramineHigh tyramine levels cause hypertensive
crisis (the “cheese effect”)Can be controlled with restricted diet
�MAOIs interact with certain drugsSerotonin syndrome (muscle rigidity, fever, seizures)SSRIs and TCAs, Pethidine must be avoided
????Which of the following is a selective MAO-B inhibitor:A. SelegilineB. ClorgylineC. MoclobemideD. TranylcypromineThe nonselective MAO inhibitors are not used clinicallyas antidepressants because of their:A. Low antidepressant efficacyB. Higher toxicityC. Potential to interact with many foods and drugsD. Both 'B' and 'C' are correct
� Direct membrane effects - reduced seizure threshold, arrhythmia
� Sexual distress: especially delay or interference with erection, ejaculation and occasionally orgasm
� Switch over� Sweating , fine tremors, insomnia� Acute poisoning
� ADs having CNS stimulant effect ?� Why therapeutic drug monitoring is needed??� Imipramine given to nondepressed individuals
produces:A. EuphoriaB. InsomniaC. Lethargy and light headednessD. Inappropriate behavior
????� Of the following, choose the antidepressant having
both high sedative and high anticholinergic activity:A. ImipramineB. AmitriptylineC. FluoxetineD. Trazodone� Imipramine produces the following actions except:A. EuphoriaB. Dryness of mouthC. Tachycardia
????� The mechanisms involved in the causation of dangerous cardiac
arrhythmias due to overdose of tricyclic antidepressants include the following except:
A. Intraventricular conduction blockB. Potentiation of noradrenalineC. Antagonism of acetylcholineD. Increased vagal tone� A 65-year-old man was brought to the hospital with complaints of
pain in lower abdomen and not having passed urine for 16 hours. The bladder was found to be full. His son informed that he was depressed for the last 2 years and only the day before a doctor had given him some medicine. Which of the following drugs is he most likely to have received?
� Tricyclic antidepressants abolish the antihypertensive action of the
4
C. TachycardiaD. Lowering of seizure threshold
Tricyclic antidepressants abolish the antihypertensive action of the following drug ? A. Enalapril, B. Clonidine, C. Atenolol, D. Diltiazem
.
SELECTIVE SEROTONIN REUPTAKE INHIBITORS Advantages over TCAs
No anticholinergic effectsMost commonly prescribed class. why ???� Major limitations of TCAs1. Frequent anticholinergic, cardiovascular and
neurological side effects.2. Relatively low safety margin..3. Lag time of 2–4 weeks before antidepressant
action manifests.4. Significant number of patients respond
incompletely and some do not respond.
� No anticholinergic effects� No postural hypotension-suitable in elderly� No sedation� Do not precipitate convulsions� Do not cause cardiac arrhythmias� No effect on cognitive or psychomotor function�Relative safety and better acceptability�Longer t1/2 due to its active metabolites
SSRIs� Citalopram safe with warfarin� Dapoxetine used to treat PME� Escitalopram most specific SSRI� Fluoxetine (prototype)longest acting� Fluvoxamine (shortest)� Paroxetine (most teratogenic)� Sertraline safe with warfarin
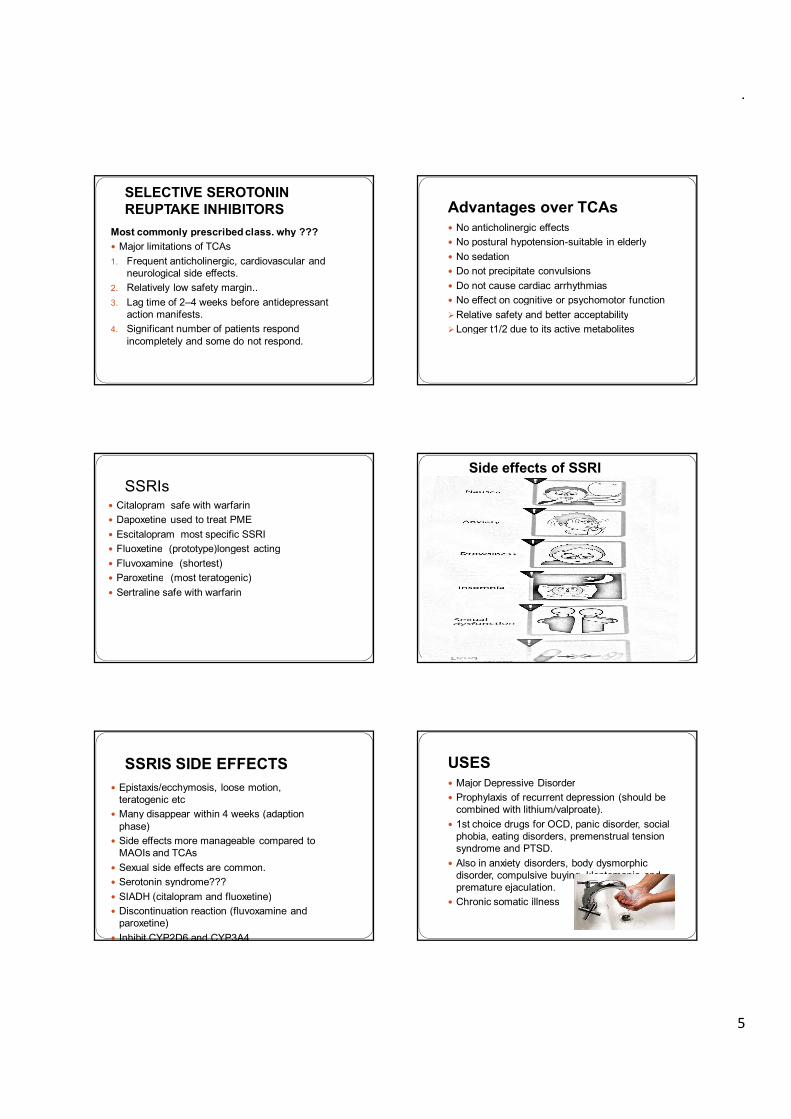
Side effects of SSRI
SSRIS SIDE EFFECTS� Epistaxis/ecchymosis, loose motion,
teratogenic etc� Many disappear within 4 weeks (adaption
phase)� Side effects more manageable compared to
MAOIs and TCAs� Sexual side effects are common.� Serotonin syndrome???� SIADH (citalopram and fluoxetine)
USES� Major Depressive Disorder� Prophylaxis of recurrent depression (should be
combined with lithium/valproate).� 1st choice drugs for OCD, panic disorder, social
phobia, eating disorders, premenstrual tension syndrome and PTSD.
� Also in anxiety disorders, body dysmorphicdisorder, compulsive buying, kleptomania and premature ejaculation.Chronic somatic illness
5
� SIADH (citalopram and fluoxetine)� Discontinuation reaction (fluvoxamine and
paroxetine)� Inhibit CYP2D6 and CYP3A4
� Chronic somatic illness
.
????� The antidepressant which selectively blocks 5-
� The antidepressant which selectively blocks 5-hydroxytryptamine uptake is:
A. FluoxetineB. AmoxapineC. DesipramineD. Dothiepin� Advantages of selective serotonin reuptake inhibitors
(SSRIs) include the following except:A. No interference with ejaculation and orgasmB. Minimal sedative actionC. Unlikely to cause fall in BPD. Lack of seizure precipitating potential
� Current drug of choice for severe depression� Venlafaxine (fastest) and minimum drug interaction� Duloxetine (longest)� Milnacipran
� Mechanism of Action� Very similar to SSRIs� Works on both neurotransmitters
� Side effects� Similar to SSRIs � HypertensionUSESSimilar to SSRIsDuloxetine & Milnacipran: fibromyalgia Duloxetine: diabetic neuropathic pain & stress urinary
incontinence
????� Classify antidepressants� Describe the advantages and disadvantages of
SSRIs.
Atypical antidepressants � Trazodone : Blocks 5-HT reuptake and 5-HT2-
antagonist; blocks α1 -adrenergic receptors� Mianserin :Increases NA releases by blocking
Clomipramine-slow effect7. Enuresis- Imipramine 25 mg at bed time 8. Neuropathic pain- Amytryptaline, Duloxetine /±
Pregabalin/gabapentin9. Migraine-Amytryptaline- prop. Esp. in mixed headache
6
� They are combined with Lithium/Valproate/lamotrigine/atypical antipsychotics-to prevent switch over in bipolar depression
� ECT can be used initially in severe cases
9. Migraine-Amytryptaline- prop. Esp. in mixed headache10. Smoking cessation: Bupropion
.
???Mechanism of antidepressant action?
?????Safest SSRI to be used with warfarin� Mechanism of antidepressant action?
� Uses of antidepressants ??� Safest SSRI to be used with warfarin� Longest and shortest acting SSRI � Most specific SSRI� Most teratogenic SSRI� Faster acting antidepressants� Therapeutic window phenomenon
Should be able to-� Classify antimanic drugs� Describe Lithium mechanism of action, important
uses, adverse effects and drug interactions.� Describe use of other drugs in Mania
Anti-manic Mood Stabilizers� Anti-manic: � Means these drugs control mania symptoms
� Mood Stabilizer:� Means they make the mood stable and prevent mood
swings in Bipolar disorder
7
.
Antimanic- Mood Stabilizers
Main Agent
Lithium Carbonate
OlanzapineRisperidoneQuetiapineAripiprazole
Anticonvulsants
Sodium Valproate
CarbamazepineLamotrigine
•Atypical Antipsychotics
� Other mechanisms:� Since Li+ is closely related to Na+, it may substitute for Na+ in
generating action potentials & Na+ exchange� Inhibit noradrenaline and dopamine turnover� Inhibition of noradrenaline sensitive adenyl cyclase enzyme� Uncoupling of receptors from their G-proteins� Effects on specific protein kinase C affecting the production of proteins
and causing long term mood stabilization� Action:
� Selective inhibition of overactive neurons� Antimanic effect in Mania� Mood stabilization in the bipolar disorder
� No noticeable effect on normal individuals � Not a sedative or antidepressant� Other actions ??
Lithium: Pharmacodynamics Lithium: Pharmacokinetics� Absorption:� Virtually complete within 6-8 hours� Peak plasma levels in 30 min. to 2 hours
� Distribution:� In total body water� Slow entry into intracellular compartment� No protein binding� Freely crosses placenta and secreted in milk: Absolutely
contra-indicated in pregnancy and lactation)
� Metabolism:� None (Also liver is not affected by Lithium)
� Excretion:� In urine with a half-life of about 20 hours� Lithium clearance is about 20% of creatinine clearance
(Serum creatinine levels must be done before starting the treatment besides, blood counts, electrolytes, pregnancy test and thyroid function test not liver function test)
� Excretion ↑ by: ↑ salt intake*, mannitol and alkalization of urine
� Excretion ↓ by: ↓ salt intake, diuretics and newer NSAIDs
Lithium: Clinical Use�Acute Mania Valproate/Atypical antipsychotics± BZDsAfter episode is under control- Lithium for 6-12m�Prophylaxis in bipolar disorder0.5–0.8 mEq/L –lithium plasma level is maintained Therapy is given based on type, cycle length, comorbid
condition and concurrent medication.Gradually introduced and gradually withdrawn
Lithium: Dosage� Dose:� Start with 300 mg bid or tid → then increased gradually� Usual dose range is 600 to 1200 mg/ day� Plasma Lithium concentration should be approximately 1
mEq/ L (range 0.6 to 1.4 mEq/ L)� Plasma Lithium concentration monitoring is necessary
because of � its very low therapeutic index (Low safety margin Toxicity > 1.5 mEq/L)� Considerable individual variation in the rate of Li excretion
8
� Recurrent neuropsychiatric illness, cluster headache and as adjuvant to antidepressants in resistant nonbipolarmajor depression
otorotor disorders e.g. disorders e.g. incoordinationincoordination of movements, of movements, ataxia, ataxia, choreoathetosischoreoathetosis, dysphasia and , dysphasia and hyperactivity** hyperactivity**
ncrease in weight & oedemancrease in weight & oedema
There is no antidote of Lithium
� Lithium levels are dangerously increased by:� Diuretics� Newer NSAIDs(So Lithium’s dose should be reduced with them)
ALTERNATIVES TO LITHIUM -Valproate� Widely used now as an antimanic drug� First line drug in acute mania� Effective even in patients not responding to
Lithium� Also being evaluated as a prophylactic� Dose: Start with 750 mg/day and then increased
rapidly up to 1500-2000 mg/day� Advantage here is that the dose can be increased
rapidly without much side effects� Devalproax
Carbamazepine� Used as an alternative to Lithium� In patients not responding to Lithium� Used to treat acute mania and also for prophylaxis� Used alone or in combination with Lithium� Less effective
� Lamotrigine: maintenance therapy of type II bipolar disorder
�Atypical antipsychotics
Summarise � Classification of antidepressants � MAOIs and their role in depression� TCAs, their mechanism of action, adverse effect
and limitations� SSRIs and SNRIs advantages and disadvantages� Atypical antidepressants� Antimanic drugs classification� Lithum mechanism of action, phamacokinetics,
adverse effect and uses � Other agents used in mania
?????� Choose the correct statement about
moclobemide: A. It is a reversible inhibitor of MAO-A with short
duration of action B. Patients taking it need to be cautioned not to
consume tyramine rich food C. It is contraindicated in elderly patientsD. It produces anticholinergic side effects
9
� Other agents used in mania
.
?????Imipramine produces the following actions
?????The mechanisms involved in the causation of � Imipramine produces the following actions
except: A. Euphoria B. Dryness of mouth C. Tachycardia D. Lowering of seizure threshold
The mechanisms involved in the causation of dangerous cardiac arrhythmias due to overdose of tricyclic antidepressants include the following except:
A. Intraventricular conduction block B. Potentiation of noradrenalineC. Antagonism of acetylcholine D. Increased vagal tone
????A 65-year-old man was brought to the hospital with
complaints of pain in lower abdomen and not having passed urine for 16 hours. The bladder was found to be full. His son informed that he was depressed for the last 2 years and only the day before a doctor had given him some medicine. Which of the following drugs is he most likely to have received:
A. AlprazolamB. SertralineC. AmitryptylineD. Trazodone
???� Tricyclic antidepressants abolish the
antihypertensive action of the following drug: � A. Enalapril� B. Clonidine� C. Atenolol� D. Diltiazem
????� The following is a tetracyclic antidepressant that
has additional dopamine blocking and neurolepticproperties, as well as greater propensity to cause seizures in overdose:
� A. Amoxapine� B. Doxepin� C. Dothiepin� D. Trazodone
?????� Choose the selective serotonin reuptake inhibitor
that is less likely to inhibit CYP2D6 and CYP3A4 resulting in fewer drug interactions:
� A. Sertraline� B. Paroxetine� C. Fluoxetine� D. Fluvoxamine
10
.
Dental implications1. Dry mouth with TCAs1. Dry mouth with TCAs2. Sympathomimetics with TCAs/MAOIs3. Serotonin syndrome with tramadol4. NSAIDs with SSRIs5. TCAs,SSRIs-macrolides antibiotics6. Bupropion: dry mouth 7. SSRI with BZD8. Amitryptyline and Dothiepin: atypical facial pain9. Tramadol/Pethidine with MAOIs–hypertensive episodes10. Untreated depression: poor oral hygiene11. Postural hypotension with TCAs12. Dry mouth/dental caries:lithium13. NSAIDs/ Metronidazole- increased lithium toxicity
� Are you able to :-� Classify antidepressants and enumerate them.� Describe their mechanism of action, adverse
effect and clinical uses.� Describe the advantages and disadvantages of
SSRIs.� Explain what are SNRIs and atypical
antidepressant and their important characteristics.