88
Benign ovarian Tumors Dr. Fayez Khatib Department of Obstetric & Gynecology SZMC
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | clifford-nichols |
| View: | 225 times |
| Download: | 1 times |

Benign ovarian TumorsDr. Fayez Khatib
Department of Obstetric & Gynecology
SZMC

Normal adult ovary

Ovaries are normally not palpable in pre-menarche, and after the menopause
In the reproductive age group ovaries are palpable in the lean pts.
Ovarian size of different age groups
Premenopause - 3.5 x 2 x 1.5 cm
Early menopause 1 – 2 yrs- 2 x 1.5x0.5cm
Late menopause 2-5yrs- 1.5x0.75x0.5cm
Normal adult ovary
Variation in dimensions can result from
– Endogenous hormonal production(varies with age
and menstrual cycle)
– Exogenous substances, including OCs, GnRH
agonists or ovulation-inducing medication, may
affect size
Normal adult ovary

Lifetime Risk of ovarian neoplasm
A woman has 5–10% lifetime risk of undergoing surgery for a suspected ovarian neoplasm– 13–21% of these will be found to be have an ovarian malignancy
Differential diagnosis of the adnexal masses varies considerably with the age of the patients.
In pre-menarchal girls and post-menopausal women adnexal mass should be considered highly abnormal – requires immediate investigation.
In menstruating patients differential diagnosis is varied.

Normal adult ovary


Classification
• Neoplasms derived from the surface epithelium- 65-80% • Neoplasms derived from germ cells-10-15%
• Neoplasms derived from specialized gonadal stroma- 5-10%
• Neoplasms metastatic to the ovary-5%

Type
Epithelial
Germ cell
Specialized gonadal stromal
Metastatic
Ovarian Neoplasm By Age
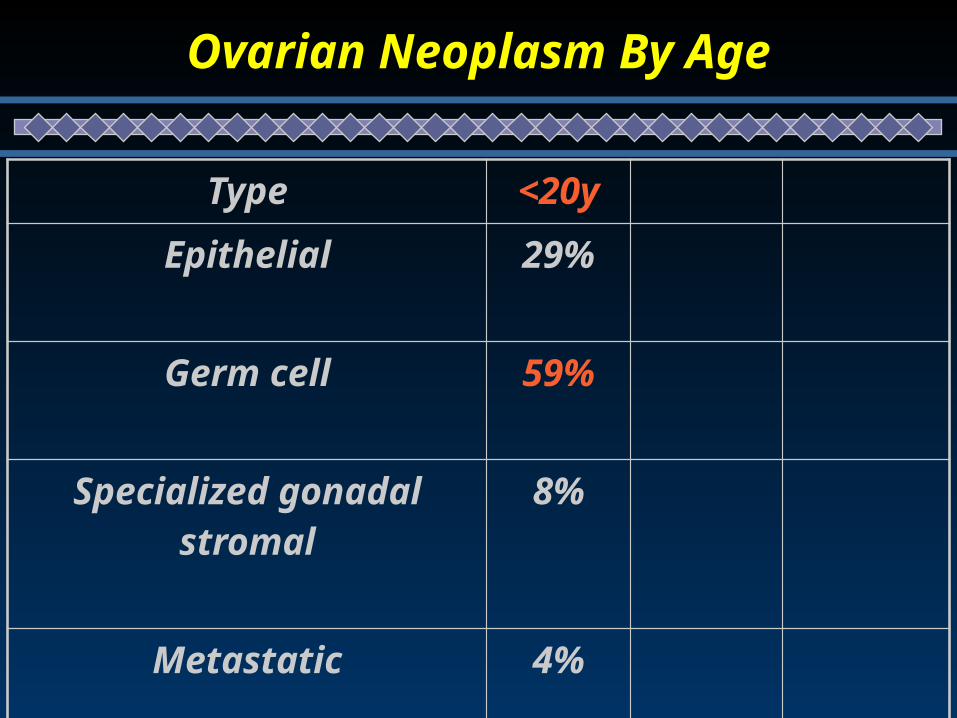
Type <20y
Epithelial 29%
Germ cell 59%
Specialized gonadal stromal 8%
Metastatic 4%
Ovarian Neoplasm By Age

Type 20-50y
Epithelial 71%
Germ cell 14%
Specialized gonadal stromal 5%
Metastatic 10%
Ovarian Neoplasm By Age

Type >50y
Epithelial 81%
Germ cell 6%
Specialized gonadal stromal 4%
Metastatic 9%
Ovarian Neoplasm By Age

OVARIAN MASSES
FUNCTIONAL INFLAMMATORY NEOPLASTIC OTHERS
FOLLICULAR CYST
CORPUS LUTEUM CYST
THECA LUTEIN
TUBO OVARIAN ABSCESSBENIGN
BORDERLINE
MALIGNANT
ENDOMETRIOMAENLARGED PCOPAROVARIAN CYST
Types of Ovarian Tumors

FUNCTIONAL OVARIAN CYSTSa. Follicular cystsb. Corpus luteum cystsc. Theca luten cysts
BENIGN OVARIAN NEOPLASM1. Serous cystadenoma2. Mucinous cystadenoma3. Brener tumor4. Dermoid cysts 5. Fibroma
6. Endometrioma
Benign ovarian Tumors

These are cysts related to ovarian function i.e. the
process of ovulation
By far the most common clinically detectable
enlargements of the ovary in the reproductive years.
Can be reach up to 10 cm in diameter
All are benign and usually asymptomatic
Resolve spontaneously.
Functional cysts

• Follicular cysts
• Corpus luteum cysts
• Theca lutein cysts
Functional cysts

Follicular cysts
Cystic follicle is defined as Follicular cyst of diameter > 3cm
Most common functional cysts.
Rarely larger than 8cm.
Lined by granulosa cells
Found incidentally on pelvic examination
Usually resolve within 4 – 8 weeks with expectant management
May rupture or torse occasionally causing pain and peritoneal
symptoms.

Follicular cysts

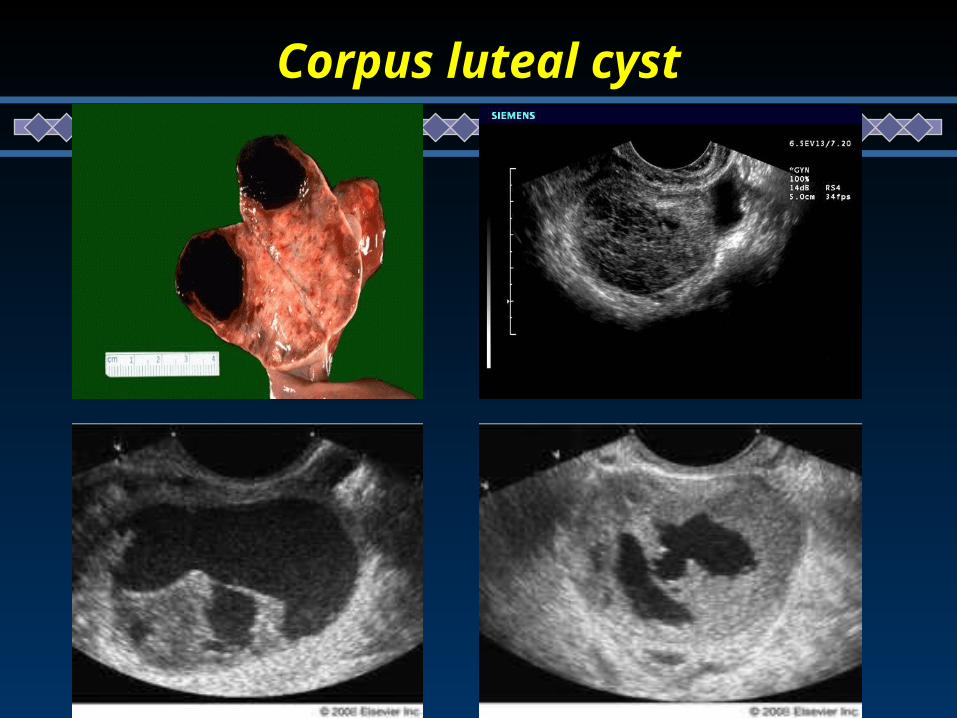
Corpus luteal cyst
Less common than follicular cyst.
May rupture leading to hemoperitoneum and requiring surgical
management( more in patients taking anti coagulants or with
bleeding diathesis)
Unruptured cysts may cause pain because of bleeding into
enclosed ovarian cyst cavity.
Corpus luteal cyst
Theca lutein cysts
Least common
Usually bilateral
Result from overstimulation of the ovary by β- hCG
Do not commonly occur in normal pregnancy
Often associated with hydatidiform moles, choriocarcinoma,
multiple gestations, use of clomiphene and GnRH analogues.
May be quite large (up to 30 cm) , multicystic, and regress
spontaneously.

Theca lutein cysts

Management of functional cysts
Expectant
Watchful waiting for two or three cycles is appropriate.
Combined oral contraceptives appear to be of no benefit.
Should cysts persist, surgical management is often indicated.
Oral contraceptives for functional ovarian cysts (Review)
Cochrane Database of Systematic Reviews 2011

Benign ovarian neoplasm

Classification
• Neoplasms derived from the surface epithelium• Neoplasms derived from germ cells
• Neoplasms derived from specialized gonadal stroma
• Neoplasms metaplastic to the ovary
• 30% of epithelial ovarian tumors in postmenopausal women are malignant
• 7% of epithelial ovarian tumors in premenopausal women are malignant
Serrous cystadenoma
Mucinous cystadenoma
Brenner tumor
Benign epithelial ovarian tumors
Borderline Epithelial Tumors
Atypical proliferating tumors
• Greater epithelial proliferation
• Noninvasive
• 15% of epithelial ovarian cancer
• Mean age at diagnosis: 40y
• Usually asymptomatic
• Can cause pain/pressure
• Diagnosed as ovarian mass/cyst
• CA-125 usually not elevated

Risk factors:
– Infertility
– Infertility drugs
– Hereditary?
• Protective:
– Multiple births
– Breast feeding
– Oral contraceptives
Borderline Epithelial Tumors

Treatment
– Surgery
• Cystectomy;USO – 12% recurrence (?)
• TAH + BSO – 2.5% recurrence (?)
• > 50% diagnosed at stage Ia
• Invasive / noninvasive implants:
Invasive implants are the most important predictor of recurrence
• Further therapy: not useful- Does not respond to chemotherapy
• 5 & 10-year survival > 90%, 20 year survival of 70%
Borderline Epithelial Tumors

Epithelial Ovarian Tumors - Serous Tumors
May occur on the ovarian surface, occasionally arises in extraovarian peritoneumUnilocular or multilocular containing clear serous fluid Endosalpingeal cell-type 60% BENIGN - bilaterality in 25%:Smooth glistening cyst
wall, no epithelial thickening or papillae, single layer of columnar cells line cyst
15% BORDERLINE - bilaterality in 34%:Epithelial atypia in cyst lining, with stratification and formation of papillae; No stromal invasion
25% MALIGNANT - bilaterality in 67%: Epithelial atypia often greater, complex architecture of papillae, multinodular. Stromal invasion present

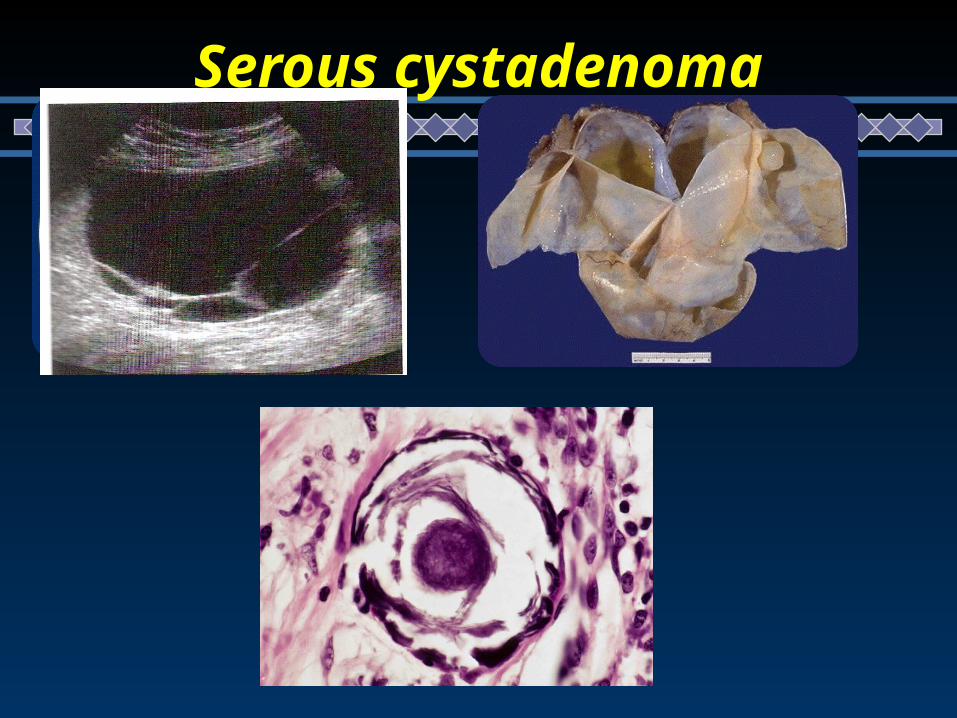
Serous cystadenoma
Generally benign
Bilateral – 10-25 %
Risk of malignancy : 5 – 15 % borderline malignant
20 -25% malignant
Size ranges from 5-40cm
GROSS : multilocular with papillary components.
MICRO : low columnar epithelium with cilia.
Characteristic psammoma bodies (end products of degeneration of
papillary implants)are found.
Associated fibrosis may lead to “cystadenofibroma”

Epithelial Ovarian Tumors - Serous Tumors
Serous Cystadenoma
Serous cystadenoma

Epithelial Ovarian Tumors - Serous Tumors
Bilateral cystadenoma

Epithelial Ovarian Tumors - Mucinous Tumors
Mucinous tumors are much less likely to be bilateral and to be malignant than Serous tumors! 80% BENIGN - only 5% bilateral 10% BORDERLINE 10% MALIGNANT - only 20% bilateral
• Cystic, mucin producing , usually multilocular• Mostly intestinal-type cell, can also resemble endocervical cells• May reach enormous size•• 5% Pseudomyxoma peritonei: peritoneal cavity becomes filled with gelatinous mucinous fluid (similar to cyst contents), which mats together the abdominal viscera; Rx is surgical, and repeated operations are required.

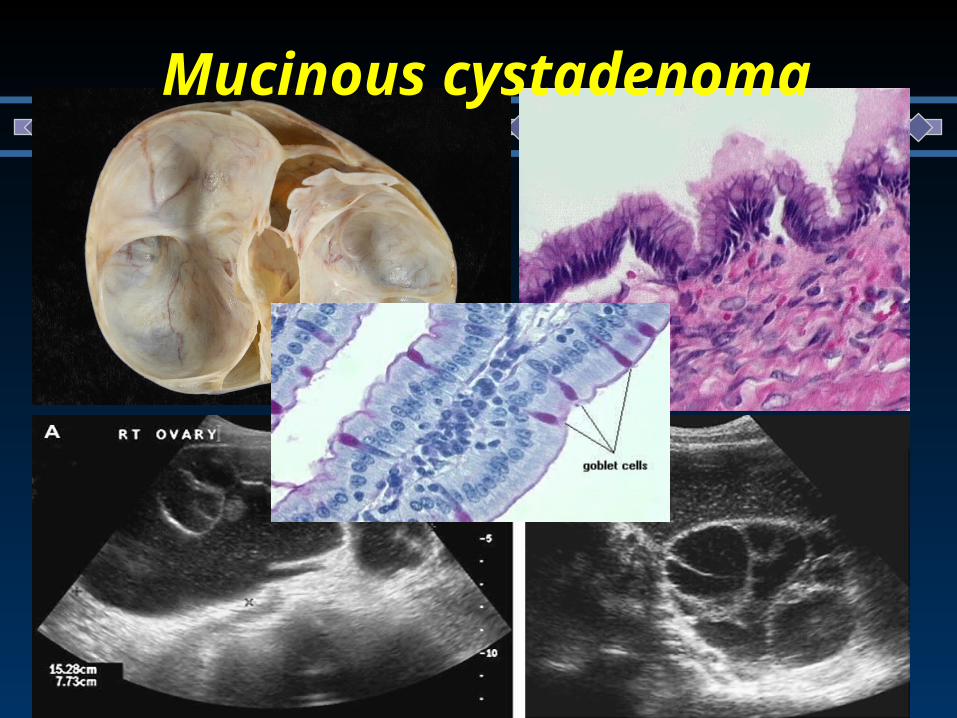
Mucinous cystadenoma
Have tendency to become huge masses
Round to ovoid masses with smooth capsules that are usually
translucent or bluish to whitish gray.
Interior divided by discrete septa into loculi containing clear ,
viscid fluid.
Epithelium – tall, pale staining, secretary with basal nuclei and
goblet cells
5 – 10% are malignant

Epithelial Ovarian Tumors - Mucinous Tumors
Benign Mucinous Tumor of Ovary

Epithelial Ovarian Tumors - Mucinous Tumors
Benign Mucinous Tumor of Ovary
Mucinous cystadenoma

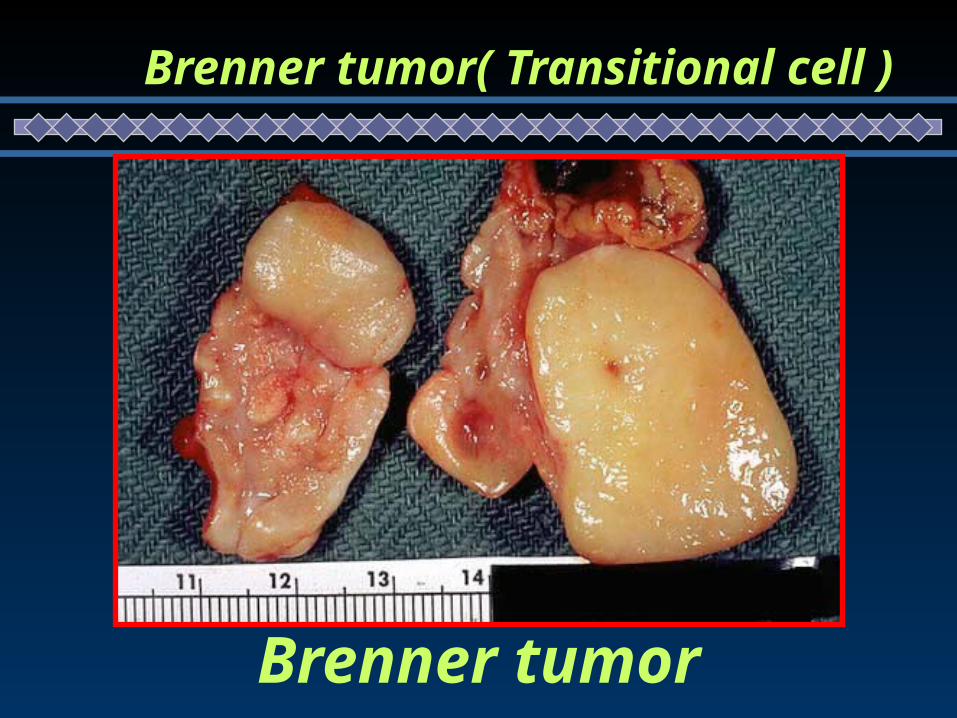
Brenner tumor( Transitional cell ):Fibroepithelial tumors derived from the surface epithelium of the ovary
which undergoes metaplasia to form urothelial-like components.
Mean age at presentation: 50 years
Rare- Constitute 1 - 2 % of all ovarian neoplasms
Usually benign ; But scattered reports of malignant Brenner’s available
Solid , grossly identical to fibroma,
Unilateral- 7 % are bilateral, left side predominance
Endocrinologically inert, but could be ass. with virilization and
endometrial hyperplasia - PMB- In postmenopausal women
On microscopy – markedly hyperplastic fibromatous matrix interspersed with nests of epitheloid cells showing “coffee beans” pattern
Brenner tumor( Transitional cell )
Brenner tumor
Brenner tumor( Transitional cell )

Brenner tumor( Transitional cell )

Brenner tumor: “coffee beans”
Brenner tumor( Transitional cell )

Classification
• Neoplasms derived from the surface epithelium
• Neoplasms derived from germ cells• Neoplasms derived from specialized gonadal stroma
• Neoplasms metaplastic to the ovary

Germ Cell Tumors
10-15 % of ovarian tumors are germ cells, 3% of them are malignant Rapidly growing Produce symptoms:
Abdominal pain Distension Torsion Rupture
Pelvic pressure Menstrual disorders Virilism

Germ Cell Tumors
Classification of germ cell neoplasms • Teratoma
• Mature cystic teratoma • Monodermal teratoma (e.g. struma ovarii)• Immature teratoma
• Dysgerminoma• Yolk sac tumor (endodermal sinus tumor) • Embryonal carcinoma• Choriocarcinoma

Germ Cell Tumors- Teratoma
Mature cystic teratoma(Dermoid): - Benign neoplasm Most common ovarian teratoma and most common ovarian germ
cell tumor Typically occurs during reproductive years Cystic tumor with firm capsule, filled with sebaceous material and
hair (occasionally teeth can be found) Thickened area from which hair and teeth arise is called
"Rokitansky's protuberance" Composed of mature elements derived from all three germ layers
(ectodermal elements such as skin, hair, sebaceous glands, and mature neural tissue predominate; cartilage, bone, respiratory and intestinal epithelium are common)

Often bilateral (15 -25%)
Malignant change occurs in 1-3%. Usually of a squamous type.
Complications include torsion-(Risk of torsion is 15%), rupture,
infection, hemolytic anemia
An ovarian cystectomy is almost always possible, even if it appears
that only a small amount of ovarian tissue remains
Mature cystic teratoma(Dermoid):
Germ Cell Tumors- Teratoma

Germ Cell Tumors- Teratoma
Dermoid Cyst
mamillae or Rokitansky's protuberances

Germ Cell Tumors- Teratoma
Dermoid Cyst

Germ Cell Tumors- Teratoma
Dermoid Cyst

Germ Cell Tumors- Teratoma
Dermoid Cyst

Germ Cell Tumors- Teratoma
Monodermal teratoma A teratoma composed predominantly of one tissue element Most common type is "struma ovarii", which is mature
thyroid tissue

Classification
• Neoplasms derived from the surface epithelium
• Neoplasms derived from germ cells
• Neoplasms derived from specialized gonadal stroma
• Neoplasms metaplastic to the ovary

Fibroma
Most common benign, solid neoplasms of the ovary.
Compose approx 5% of benign ovarian neoplasms and 20% of all solid
tumors of the ovary.
Frequently seen in middle-aged women.
Characterized by their firmness and resemblance to myomas
Misdiagnosed as exophytic fibroids or primary ovarian malignancy
Not hormonally active
Fibromas may be associated with ascites or hydrothorax as a result of
increased capillary permeability thought to be a result of VEGF
Mieg’s syndrome (ovarian fibromas, ascites and hydrothorax) is uncommon
and usually resolves after surgical excision.

Fibroma

Thecoma
Solid fibromatous lesions that show varying degrees
of yellow or orange discoloration
Almost always confined to one ovary
Usually >40 years, 65% after menopause
May be hormonally active and hence associated
with estrogenic or occasionally androgenic effects.
Rarely malignant
Gonadoblastomas
Gonadoblastoma is a rare benign tumor that has the potential for
malignant transformation and affects a subset of patients with an
intersex disorder or disorder of sex development (DSD).
Arise in patients with dysgenetic gonads - 46 XY f/b 45XO/ 46 XY mosaic.
Contain both germ cells and sex cord stromal cells.
Presents usually as phenotypic female <30 years with primary amenorrhea
and virilization.
Treatment – laparoscopy or laparotomy with removal of b/l dysgenetic
gonads.
Further treatment depends on malignant germ cell component
Classification
• Neoplasms derived from the surface epithelium
• Neoplasms derived from germ cells
• Neoplasms derived from specialized gonadal stroma
• Neoplasms metaplastic to the ovary

Endometriomas
Most common site of involvement is the ovary. Large hemorrhagic cyst (chocolate cyst), Cyst walls are
usually thick and fibrotic. They may completely replace normal ovarian tissue. USG: anechoic cysts to cysts with diffuse low-level echoes
to solid-appearing masses. They may be unilocular or multilocular with thin or thick
septations Malignant transformation: 0.3% to 0.8% Management: medical and/ or surgical


Clinical presentation
Asymptomatic – accidentally discovered on USG Chronic pattern of pain, increasing abdominal girth over months
or weeks. Associated with secondary symptoms of anorexia, nausea,
vomiting, urinary frequency. Could be associated with primary or secondary amenorrhea,
menstrual irregularities, virilization, precocious puberty Become acutely symptomatic if undergoes torsion, rupture or
hemorrhage. Benign ovarian neoplasms are indistinguishable clinically from
malignant counterparts

Complications
Torsion
Intracystic hemorrhage
Infection
Rupture
Pseudomyxoma peritonei
Malignancy

Diagnostic evaluation of the patient with an adnexal mass
Complete physical examination
Pelvic ultrasound examination, Doppler?
Computed tomography scan with contrast enhancement
Tumor markers-( ca-125)
Laparoscopy, laparotomy

Evaluation
Abdominal and vaginal examinationAssess
– Laterality – Cystic Vs solid– Mobile Vs fixed– Smooth Vs irregular– Ascites– Cul-de-sac nodules

Unilateral
Cystic
Mobile
No ascites
No cul de-sac nodules
Slow or no growth
Clinical features of benign ovarian masses

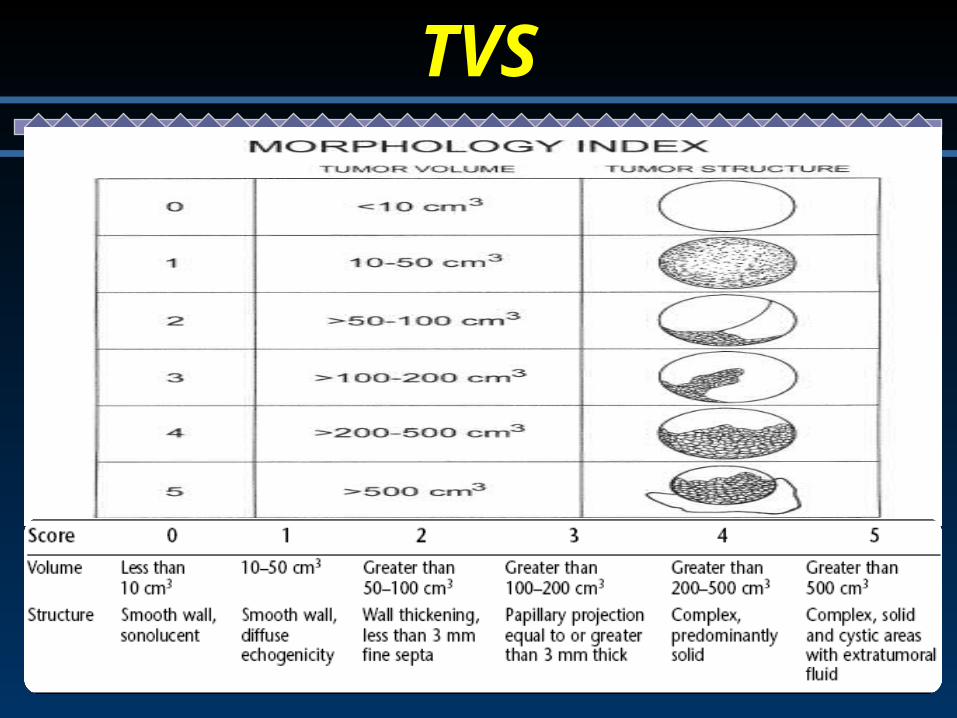
TVS
Pattern recognition is superior to all other scores.
Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet Gynecol2008, RCOG 2011
TVS
Doppler Evaluation
Hypoxic tissue in tumors recruit low-resistance, high-flow blood
vessels
Role in evaluating ovarian mass is controversial – as the ranges
of values of RI,PI between benign and malignant masses overlap.
PI<1, RI<0.4
Adding Doppler does not seem to yield much improvement in the
diagnostic precision, but increases the confidence with which a
correct diagnosis of benignity or malignancy is made..

Other imaging modalities
CT, MRI, PET not recommended in the initial evaluation
CT scan: evaluating
– LN involvement,
– Omental mets, peritoneal deposits, hepatic mets,
– Obstructive uropathy
– Probable alternate primary site when cancer is suspected based upon TVS
MRI : differentiating non adnexal pelvic masses (like leiomyomata),
expensive and inconvenient.
ACOG GUIDELINES 2007

1. Unilocular
2. Smooth surface
3. No solid elements
4. No external or internal outgrowth
5. No ascites
6. Unilateral
7. Normal Doppler flow
Radiological features of benign ovarian masses

Tumor markers
CA-125HE4BHCGLDHAFP

Calculation of RMI (Risk malignancy index):
RMI=MxUxCA-125

Calculation of RMI (Risk malignancy index):
It is an effective way of triaging patients into low , moderate, high risk for malignancy, according to which the referral to a higher centre and management protocol will differ.
It is recommended that a ‘risk of malignancy index’ should be used to select those women who require primary surgery in a cancer centre by a gynecological oncologist.
RCOG Guideline No. 34 October 2003


Operative intervention

Indications for surgery
Any solid ovarian lesion
Any ovarian lesion with papillary vegetation on the
cyst wall
Any adnexal mass >10cm in diameter
Palpable adnexal mass in a premenarchal or
postmenopausal women
Torsion or rupture suspected

Ovarian mass in childhood:History and physical examination
Appr. Imaging studies
Simple cyst- Observe and reassess
Solid or solid cystic
MRI and tumor markers
High suspicion of malignancy
Low suspicion of malignancy
Laparotomy laparoscopy
Frozen section Malignant – oophorectomy and staging
Benign - cystectomy

Ovarian mass in reproductive age group
<5 cms. >/= 5 cms
USG USG
cystic
observationComplex,
solid, suspicious
Persistence or progression
surgery
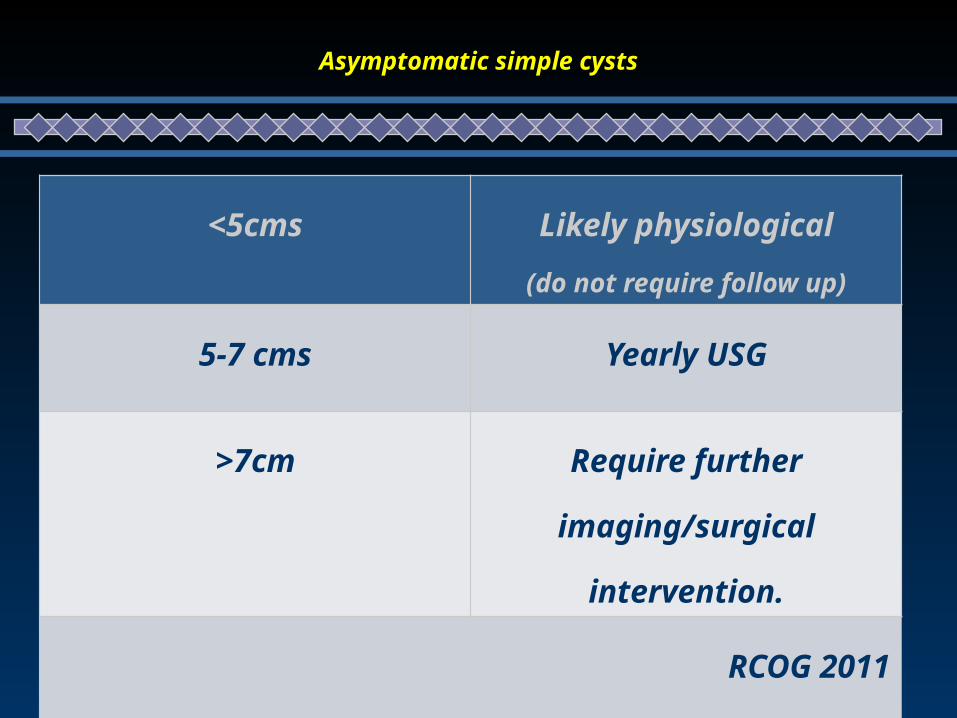
Asymptomatic simple cysts
<5cms Likely physiological
(do not require follow up)
5-7 cms Yearly USG
>7cm Require further
imaging/surgical intervention.
RCOG 2011

Cyst Aspiration
Diagnostic cytology has poor sensitivity to detect
malignancy, ranging from 25% to 82%
Not therapeutic, even when a benign mass is
aspirated
Approx. 25% of cysts will recur within 1 year
Aspiration of a malignant mass may induce spillage
and seeding of cancer cells into the peritoneal cavity

Ovarian mass In Postmenopausal women

Ovaries atrophic and shouldn’t be palpable on pelvic
examination.
Presence of palpable ovary must alert the physician to the possibility
of an underlying malignancy.
Incidence in asymptomatic post menopausal women –
1.5% by pelvic examination
3.3% to 14.5% by USG
Causes -10% functional
90% neoplastic (either benign or malignant). Obstet gynecol survey, 2002
Ovarian mass In Postmenopausal women

Simple, unilateral, unilocular ovarian cysts, less than 5 cm in diameter, have a low
risk of malignancy. It is recommended that, in the presence of a normal serum
CA125 levels, they be managed conservatively.
Aspiration is not recommended for the management of ovarian cysts in
postmenopausal women.
It is recommended that a ‘risk of malignancy index’ should be used to select
women for laparoscopic surgery, to be undertaken by a suitably qualified surgeon.
It is recommended that laparoscopic management of ovarian cysts in
postmenopausal women should involve oophorectomy (usually bilateral) rather
than cystectomy.
Ovarian mass In Postmenopausal women

Operative intervention

Operative Modalities
Laparoscopy vs laparotomy – decision based on suspicion of malignancy and
technical expertise
No RCTs comparing recurrence rates following laparoscopy or laparotomy.
The objective is to try cystectomy if possible.
Laparoscopic surgery for benign ovarian tumours is associated with less pain,
shorter hospital stay, and fewer adverse events than with laparotomy.
Cochrane Database of Systematic Reviews 2009

The standards for laparoscopy in benign tumours
1. Careful examination of the external surface of the tumour
and sampling of the peritoneal cavity
2. Avoidance of any tumoral rupture
3. Protection of the ovarian tumour with an endoscopic bag
before removal
Operative Modalities


















