23
Benign Paroxysmal Positional Vertigo (BPPV)
| Date post: | 16-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | everydayhearingcom |
| View: | 143 times |
| Download: | 7 times |

Benign Paroxysmal Positional Vertigo (BPPV)

What is BPPV?
BPPV stands for benign paroxysmal positional vertigo. It is a disorder of the vestibular system
of the inner ear.
It is the most common vestibular disorder.
The vestibular system in the inner ear is responsible for maintaining balance.

Benign
Benign means that it is not life-threatening and will generally not progress.

Paroxysmal
Paroxysmal describes how the symptoms occur suddenly, in brief episodes of mild to intense
vertigo.
Positional
Positional describes how changes in head position cause symptoms. These positional
changes may be looking up and down, laying down or rolling over in bed, or sitting up quickly.
Vertigo
Vertigo is used to describe the sensation of movement or spinning that occurs following a
position change.

Anatomy of BPPV
• The vestibular system of the inner ear is made up of:– 2 organs called the utricle and saccule– 3 semicircular canals: posterior, anterior, and
horizontal
• Attached to a membrane within the utricle and saccule are microscopic calcium carbonate crystals called “otoconia” that help sense movement.
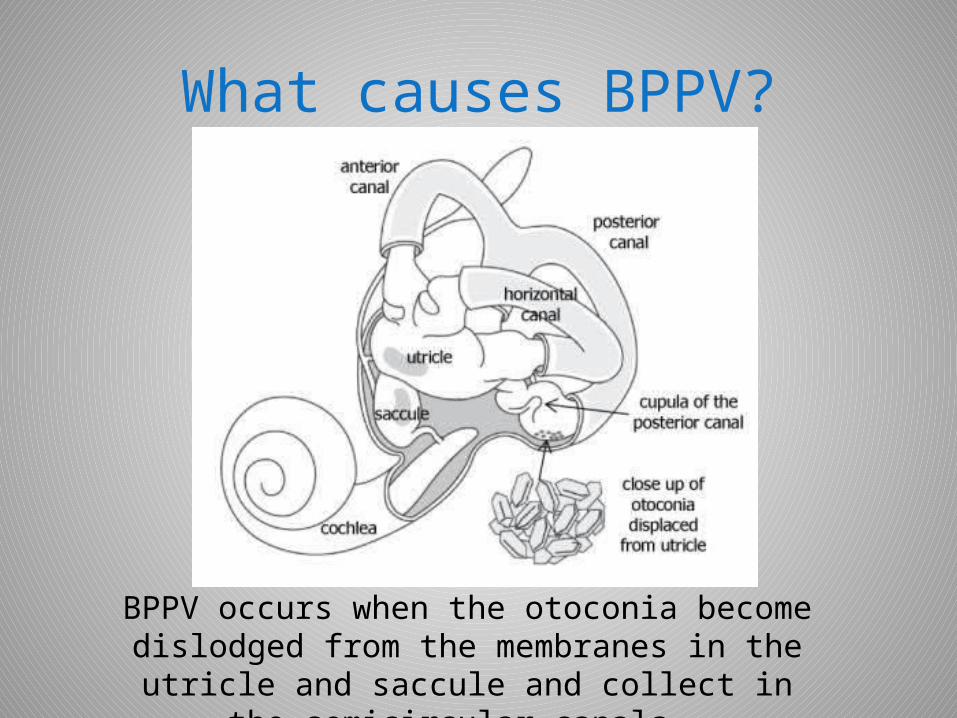
What causes BPPV?
BPPV occurs when the otoconia become dislodged from the membranes in the utricle and saccule and
collect in the semicircular canals.

What causes BPPV?
When the head moves, this causes the displaced otoconia in the semicircular canals to move. This
movement of otoconia sends a false signal to the brain, causing vertigo.
What causes BPPV?
• BPPV is more likely to occur over the age of 50 and is, in most cases, a result of an age-related degeneration of the vestibular system.
• Other causes may include:– Mild to severe head injury – Whiplash– Surgery causing trauma to the ear– Extensive dental work– Prolonged inactivity– Migraine– Other vestibular abnormalities

Types of BPPV
• Classified by which semicircular canal the otoconia have migrated to: anterior, posterior, or horizontal.
• Classified by whether the otoconia are free-floating in the semicircular canal (called canalithiasis) or have become attached to the membrane within the semicircular canal (called cupulothiasis).
• Classified as unilateral or bilateral.

The most common type of BPPV is unilateral posterior canal canalithiasis.
Types of BPPV

What are the symptoms of BPPV?
• Brief episodes of vertigo (spinning sensation) triggered by head or body movements.
• Episodes of vertigo typically last less than 1 minute.
• In cupulothiasis type BPPV, episodes can last several minutes.
• Symptoms range from mild to severe. In severe cases of vertigo, nausea and vomiting can occur.

What is nystagmus?
Nystagmus describes the involuntary eye movements that occur during episodes of BPPV. It is a quick back and forth “beating” movement
of the eyes.

Diagnosis of BPPV
• Medical and case history
• Auditory evaluation
• Vestibulonystagmography Test (VNG)
• Positioning testing to include the Dix-Hallpike maneuver.
Dix-Hallpike Maneuver
The Dix-Hallpike maneuver is performed by moving the patient’s head and body into
different positions and observing the nystagmus. The characteristics of the nystagmus will
determine which semicircular canal is being affected. Vertigo will likely occur during the Dix-
Hallpike if you have BPPV.
How is BPPV treated?
• Canalith Repositioning Procedure (CRP)– A specific series of head and body movements. – Used to relocate the otoconia from the semicircular canal
back into the utricle or saccule. – Performed by a trained technician or Doctor.
• Brandt-Daroff exercises– Home-based exercises involving repeating a series of head
movements 2-3 times for 3 weeks. – Can be performed by the patient themselves without
assistance.
Types of Canalith Repositioning
• The type of canalith respositioning procedure performed to treat BPPV will depend on which type of BPPV has been diagnosed.
• The two most common canalith repositioning procedures used to treat posterior canal BPPV are:– The Epley Maneuver– The Semont Maneuver

The Epley Maneuver
Involves 4 sequential movements of the head and body with a 30 second or more rest at
each position.

The Semont Maneuver
Involves quickly moving the patient from laying on one side to the other. The head is held in a specific
position during movements.
Canalith Repositioning Procedure
Following a CRP, the patient should restrict head and body movements for a period of 24-72
hours. Sleeping position may also be restricted during this time as well. This gives the otoconia sufficient time to “settle” back into the utricle
and saccule following treatment.
Can BPPV cause lasting problems?
• Most cases of BPPV can be successfully treated after one or two canalith repositioning procedures.
• BPPV is likely to re-occur several times within a person’s lifetime.
• Although BPPV is not life-threatening, the symptoms can be very debilitating before treatment occurs.

Resources:
http://www.mayoclinic.org/diseases-conditions/vertigo/basics/definition/con-20028216
http://vestibular.org/understanding-vestibular-disorders/types-vestibular-disorders/benign-paroxysmal-positional-vertigo

















![Benign Paroxysmal Positional Vertigo: An Overview€¦ · BPPV, most commonly including canal paresis of the in-volved side. In 2003, Vibert [28] found a correlation be-tween BPPV](https://static.documents.pub/doc/80x56/605bebb8e76d74078e269a34/benign-paroxysmal-positional-vertigo-an-overview-bppv-most-commonly-including.jpg)