50
Berrin Günaydın, MD, PhD Gazi University School of Medicine Department of Anesthesiology, Ankara, Turkey www.berringunaydin.com MANAGING A PATIENT WITH ABNORMAL PLACENTATION
| Date post: | 30-Dec-2015 |
| Category: |
Documents |
| Upload: | gary-williamson |
| View: | 230 times |
| Download: | 4 times |
Berrin Günaydın, MD, PhDGazi University School of Medicine
Department of Anesthesiology, Ankara, Turkey
www.berringunaydin.com
MANAGING A PATIENT WITH ABNORMAL PLACENTATION

Company NameHonoraria/Expenses
Consulting/ Advisory Board
Funded Research
Royalties/ Patent
Stock Options
Ownership/ Equity
PositionEmployee
Other (please specify)
Example: company XYZ
No, nothing to disclose
Yes, please specify: X
Faculty Disclosure
OUTLINE
Definition & Classification of Abnormal Placentation
Epidemiology & Incidence
Management
-Obstetric & Anesthetic
Definition and Classification
Placentation
Normal Abnormal
Adher
ence
of t
he B
LASTOCYST
to th
e de
sidua
lized
ENDOM
ETRIUM
ABNORMAL
adhe
renc
e of
the
place
nta
to M
YOMETRIU
M

1.Placenta Previa
2.Accreta Spectrum
3.Placental Abruption
4.Cesarean scar ectopic pregnancy & cervical pregnancy
ABNORMAL PLACENTATION
Silver & Barbour. Obstet Gynecol Clin N Am 2015

Types of Placenta Previa

-multiparity
-advanced maternal age
-previous cesarean delivery
-other uterine surgery
-previous placenta previa
-smoking
-no identifiable risk factors in 20% of all cases
Conditions Associated with Placenta Previa
Snegovskikh et al. Curr Opin Anesthesiol 2011

SPECTRUM
ACCRETA
INCRETA
PERCRETA
Silver & Barbour. Obstet Gynecol Clin N Am 2015

-1:2500 deliveries
(sole incidence)
-1:2065 (relative risk in the presence of placenta previa)
Epidemiology of Placenta AccretaO
ver
the
past
30
year
s it
incr
ease
d ne
arly
10
fold
Hull & Resnik.Clin Obstet Gynecol 2010

Pathophysiology
Possible mechanisms
1.Abnormal decidualization
Previous cesarean or other surgery scars, pelvic radiation,
placenta previa
2.Pathological over invasiveness of
trophoblast
Over expression of CD44 receptors, changes in growth-angiogenesis-invasion-related factors in trophoblast, alteration in adrenomedullin gene
expression, specific DNA mutations
SEVERE
Maternal & Fetal
Morbidity &
Mortality
Massive hemorrhage &
associated complications
DIC, MOD &/or failure
Clinical implications of abnormal placentation are important because…
WHY?

Abnormal Placentation
Correction & Treatment
Fetal Outcome
• MASSIVE TRANSFUSION• ICU Admission• Interventional Radiologıc Procedures
Fetal morbidity & mortality is related to complications of premature birth
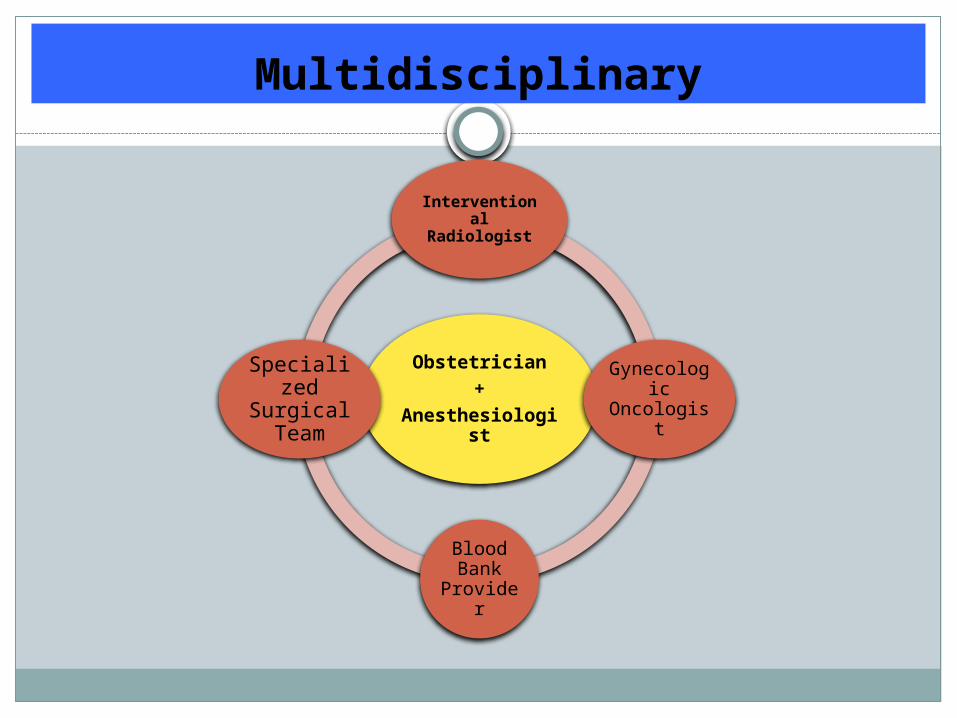
Multidisciplinary
Obstetrician+
Anesthesiologist
Interventional
Radiologist
Gynecologic
Oncologist
Blood Bank
Provider
Specialized
Surgical Team
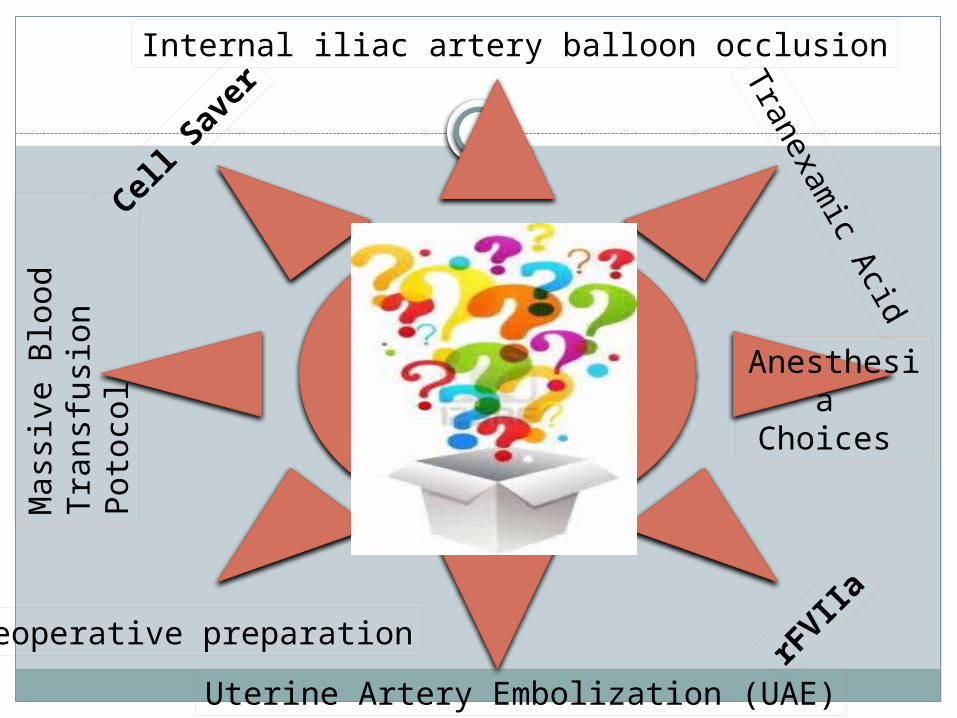
OBSTETRIC & ANESTHETIC MANAGEMEN
T
Cell S
aver
Mas
sive
Blo
od
Tra
nsfu
sion
Pot
ocol
Internal iliac artery balloon occlusion
Tranexamic A
cid
Preoperative preparation
Uterine Artery Embolization (UAE)
rFVIIa
Anesthesia Choices
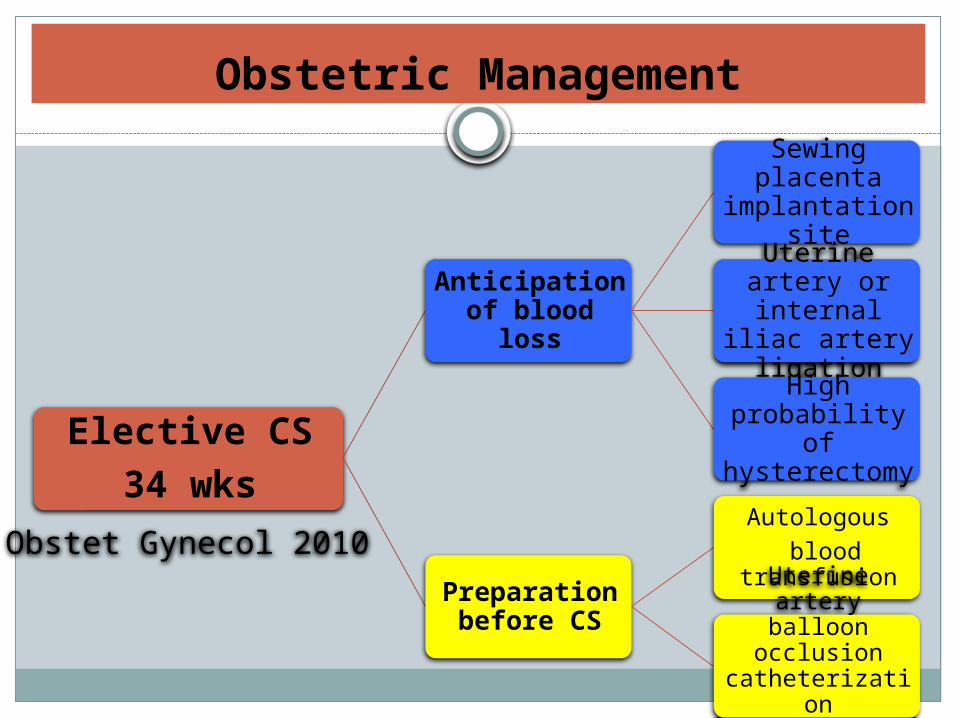
Obstetric Management
Elective CS
34 wks
Anticipation of blood loss
Sewing placenta implantation site
Uterine artery or internal iliac
artery ligation
High probability of hysterectomy
Preparation before CS
Autologous
blood transfusion
Uterine artery balloon occlusion
catheterization preoperatively
Obstet Gynecol 2010

Complications
Maternal Hemorrhag
e
Peripartum Hysterecto
my
Goals
Massive Blood
Transfusion
Save uterus
General Management

Prophylactic Internal Iliac Artery Balloon Occlusion
It does reduce pulse pressure
distal to the occlusion site,
thus minimizes blood loss
during hysterectomy
1.To stop hemorrhage for avoiding hysterectomy and saving fertility
2.To decrease obstetric hemorrhage prior to hysterectomy (bleeding vessels are better identified)

Neonatal Outcome after internal iliac artery balloon occlusion for placenta accreta
n=19 parturients with accreta/percreta5-F balloon catheter was inserted in bilateral
common iliac arteries at the department of Interventional Radiology 1 h before CS
Taiwanese J Obstet Gynecol 2011
Apgar 1 min<7 Apgar 5 min<7
Spinal Anesthesia (n=7)0.5% hyperbaric bupivacaine 10-11 mg
1/7 0/7
General Anesthesia (n=12)
-IVGA -ketamine+propofol (n=5)-ETGA-Thiopental+sch+sevoflurane (n=7)
4/12
1/53/7
(p=0.393)
0/12
0/50/7
(p=0.879)

Surgical Management of Accreta Spectrum
Criteria for accreta referral
centerMultidiscipilinary
teamICU & facilitiesBlood services
Antepartum management of SUSPECTED accreta
Surgical management of SUSPECTED accreta
Surgical management of previously UNSUSPECTED accreta
Placenta Accreta Spectrum: Accreta, Increta & Percrata. Obstet Gynecol Clin North Am 2015

Preoperative Blood Bank Communication
In case of SUSPECTED placenta accreta, blood bank is called to request blood products & to inform about the possibility of massive transfusion
In routine accreta cases, 4 units of matched RBCs + 4 units of FFP are readily available in the OR beforehand
In emergency cases, when placenta accreta is diagnosed intraoperatively, anesthesiologist calls blood bank for massive transfusion protocol 6 units of O negative RBCs + 4 units of AB FFP
20 min later additional 10 units AB FFP+ 10 units of platelets+ 10 units of
cryoprecipitate (having an option of rFVIIa )

MonitoringAfter massive transfusion, check every hour
PTT
PT*Fibrinogen
levels
Cl
K
Mg
Ca
None of these tests adequately assess platelet function, FXIII, clot stability or fibrinolytic
activity
Iatrogenic;masssive
transfusion of salin
Dilutional or citrate binding
Overload due high K in stored
RBC
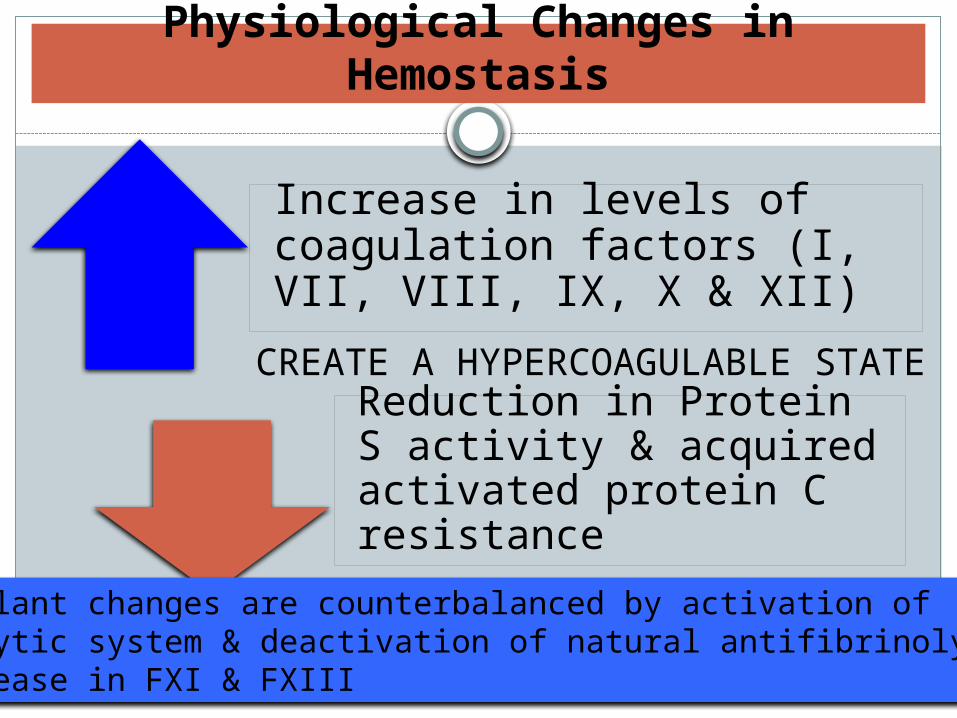
Increase in levels of coagulation factors (I, VII, VIII, IX, X & XII)
Reduction in Protein S activity & acquired activated protein C resistance
Physiological Changes in Hemostasis
Procoagulant changes are counterbalanced by activation offibrinolytic system & deactivation of natural antifibrinolytics via decrease in FXI & FXIII
CREATE A HYPERCOAGULABLE STATE
Physiological changes in FXI & FXIII during pregnancy
Lab
ora
tory
in
vest
igat
ion
Relative deficiency of FXI & FXIII cause decreased polymerization of fibrin monomers into fibrin & diminishes the crosslinks of α2-antiplasmin to fibrin (which makes fibrin much less resistant to degradation)
Relatively low levels of FXI & FXIII decrease activation of thrombin activatable fibrinolysis inhibitor resulting in decreased antifibrinolytic potential
Levels of D-dimers & FDP increase with rapid depletion of fibrinogen & FXIII
GOALS CONCERNS
ANESTHESIA TECHNIQUE

GENERALANESTHESIA
REGIONALANESTHESIA
INTRAOPERATIVE RECALL
ASPIRATION
FAILED INTUBATION
DECREASED RISK OF MATERNAL DEATH
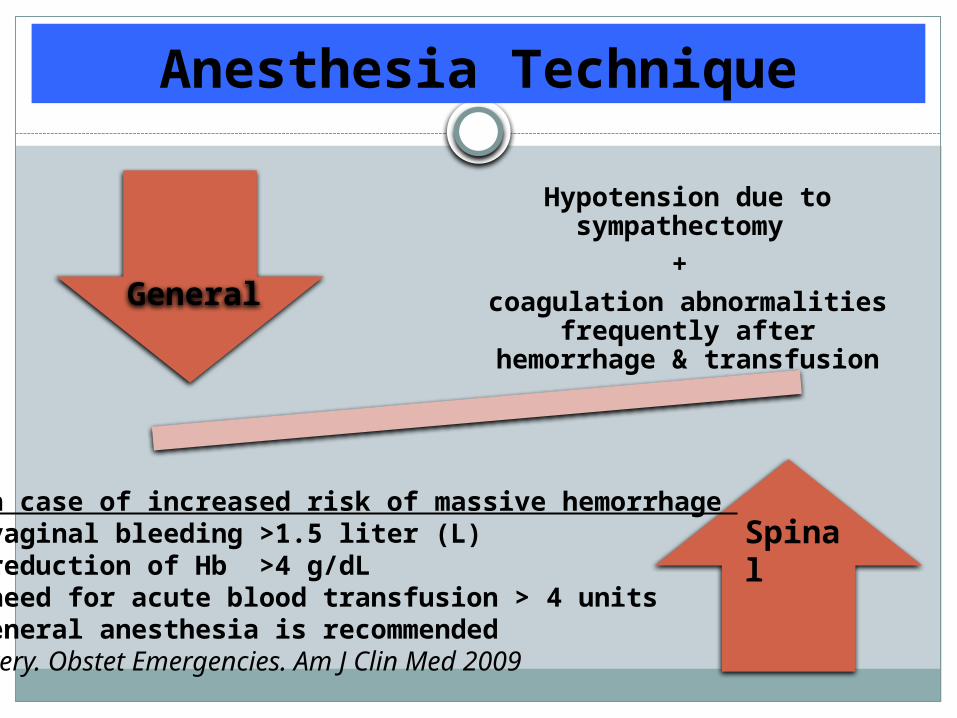
Hypotension due to sympathectomy
+
coagulation abnormalities frequently after hemorrhage &
transfusion
Anesthesia Technique
General
Spinal In case of increased risk of massive hemorrhage +vaginal bleeding >1.5 liter (L)+reduction of Hb >4 g/dL +need for acute blood transfusion > 4 unitsgeneral anesthesia is recommendedAvery. Obstet Emergencies. Am J Clin Med 2009
Spinal
Epidural
Neuraxial Anesthesia
or
For PERIPARTUM INTERVENTION it is considered to be a standard practice in many developed countries. Curr Opin Anesth 2011
In patients requiring general anesthesia for emergency deliveries, risk can be reduced by use of regional anesthesia after careful antenatal assessment with no medical contraindication for regional anesthesia. ACOG Anesthesia for emergency deliveries. Number 104. March 1992
Cell saver
Damage Control
Resuscitation
(DCR)
Blood loss
Blood loss management
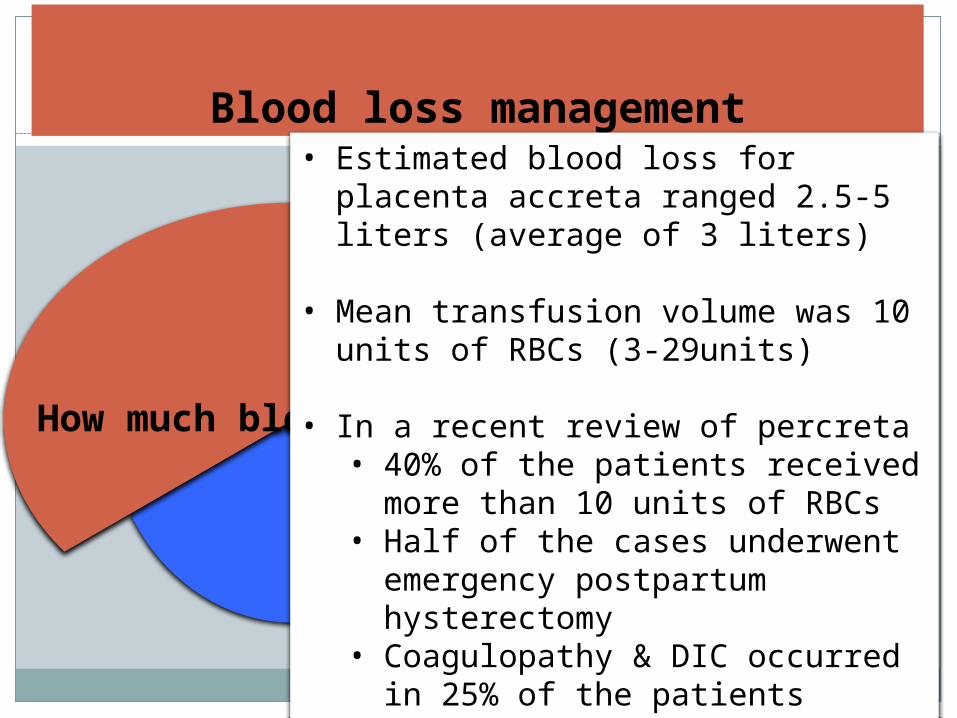
How much blood is
lost?
Blood loss management• Estimated blood loss for placenta accreta
ranged 2.5-5 liters (average of 3 liters) • Mean transfusion volume was 10 units of
RBCs (3-29units)
• In a recent review of percreta• 40% of the patients received more
than 10 units of RBCs • Half of the cases underwent
emergency postpartum hysterectomy• Coagulopathy & DIC occurred in 25%
of the patients
Clin Obstet Gynecol 2010

Cell saver
in 1970s
Blood loss management
• Use of autologous RBC salvage can decrease transfusion requirements of allogenic blood products
• Concerns about risk of amniotic fluid embolism (AFE) & maternal alloimmunization
• Theoretically, washing process and leukocyte-reducing filter should eliminate the risk of AFE
• Contamination of maternal circulatory system with amniotic fluid during CS with or without cell saver is similar
• However, caution for risk of severe hypotension if cell salvage is used for CS
Anesthesiology 2000, J Crit Care 2001
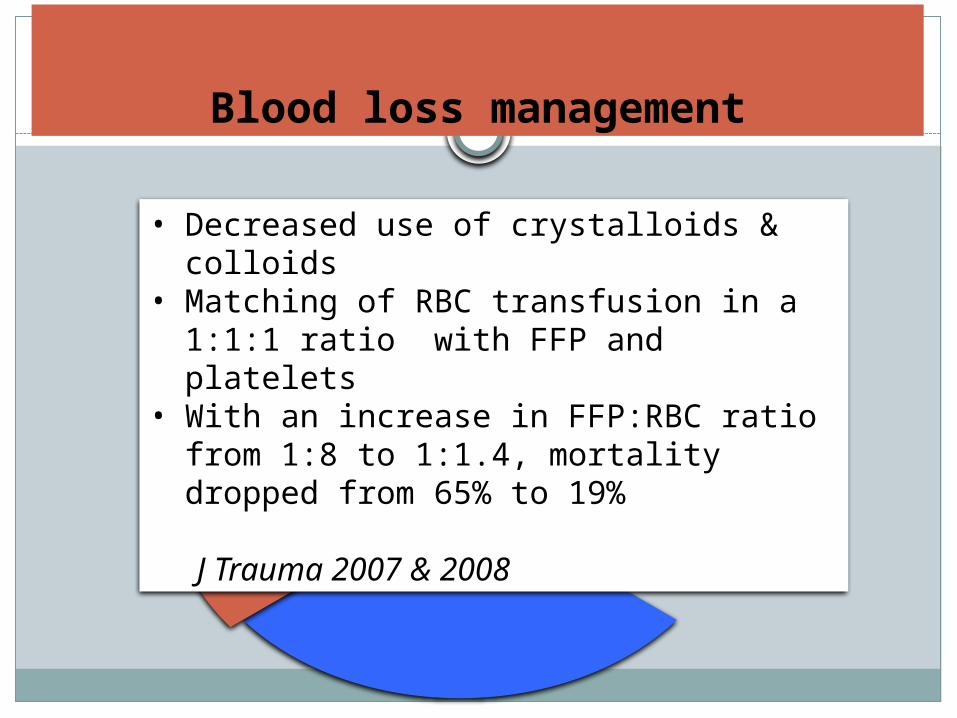
Damage Control
resuscitation in 2005
Blood loss management
• Decreased use of crystalloids & colloids • Matching of RBC transfusion in a 1:1:1 ratio
with FFP and platelets• With an increase in FFP:RBC ratio from 1:8 to
1:1.4, mortality dropped from 65% to 19%
J Trauma 2007 & 2008

Strategies for massively bleeding parturients
EARLY administration of criyoprecipitate & tranexamic acid are currently considered
for bleeding obstetric patients
Curr Opin Anesthesiol 2011 J Anesth 2007
Optimize FFP to RBC ratioAccording to DCR mixture of 1 U RBC+1 U FFP + 1 U platelet has a hematocrit of 29%, platelet of 85 000/mm3 & coagulation factor activity of 62%
Use of cryoprecipitate & antifibrinolytic agents-Fibrinogen 2-3 g/L recommended for adequate hemostasis-FXIII level should be kept >50-60%-30 mL/kg of FFP or 3 mL/kg of criyoprecipitate is required to increase fibrinogen level by 1 g/L
Consider FVII rFVIIa of 81.5-92 μg/kg reduced hemorrhage in 76-85% of patients without thromboembolic events(hypothermia, acidosis or low fibrinogen may cause failure to respond to rFVIIa)
Minimize use of crystalloids & colloids to avoid dilutional coagulopathy
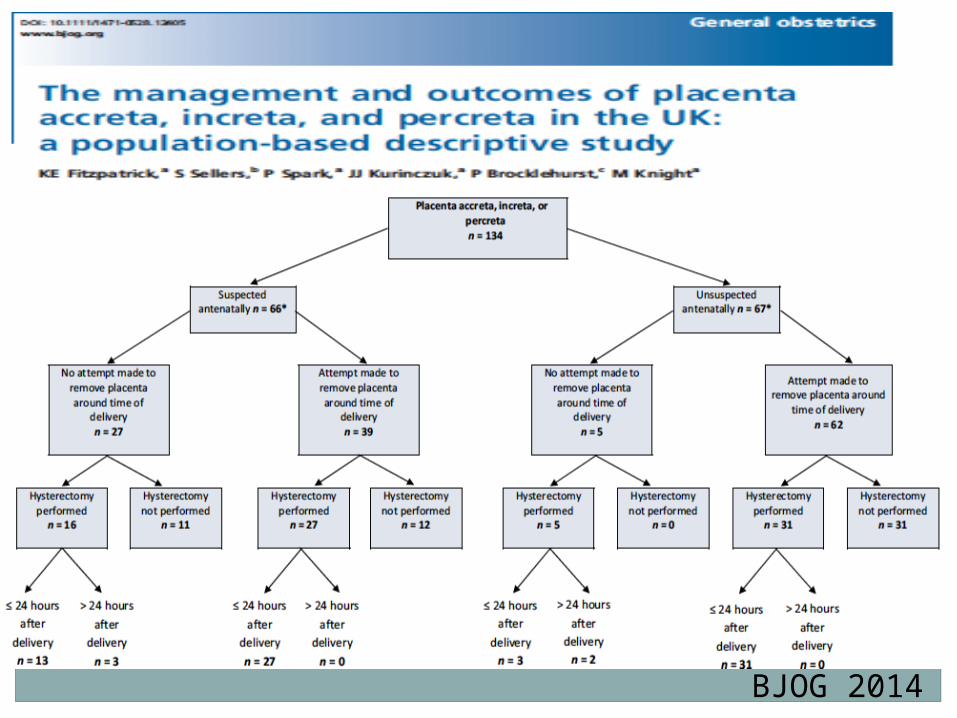
BJOG 2014

Therapies for prevention & treatment
Fitzpatrcik et al. BJOG 2014
Matsuoka et al. Anesthetic management of patients with placenta previa accreta for CS: a 7-year single-center experience. Masui 2015
Weiniger et al. Outcomes of prospectively-collected consecutive cases of antenatal-suspected placenta accreta. IJOA 2013
Placenta Accreta
Lilker et al. Anesthetic considerations for placenta accreta. IJOA 2011
n=56892 deliveries including n=23 placenta accreta underwent UAE under epidural &/or general anesthesia
Bayram, Ilgıt, Altan Gunaydin et al. Evaluation UAE on size and
symptomatology of Leiomyoma under PCA with meperidine
Placenta Increta(Sultan et al. CSA for cesarean hsyterectomy and massive hemorrhage
in a parturient with placenta increta. Can J Anesth 2012)A multiparous parturient with complete
placenta previa scheduled for CS under CSE anesthesia
However, continuous spinal anesthesia (CSA) was employed because of the inadvertent dural puncture occurred during epidural insertion
After delivery, surgical team confirmed placenta previa with increta followed by hysterectomy with adherent placenta in situ
Because of the extensive bleeding, 3.8 L RL + 1.5 L hespan + 16 units of RBC & FFP + 4 units apheresis platelets + 1 unit cryoprecipitate were given and CSA was converted to general anesthesia

Case 1. Placenta Previa
ES 34 yr old medical doctor36 weeks gestation84 kg, 161 cm Repeat CSPelvic USG & MRI revealed placenta previa totalis (+)Potantial placenta accreta??increta??percreta??
Gunaydin et al. The Management of Neuraxial Anesthesia of Emergent CS for Placenta Previa. TurkJ Anesthesiol Reanim 2015
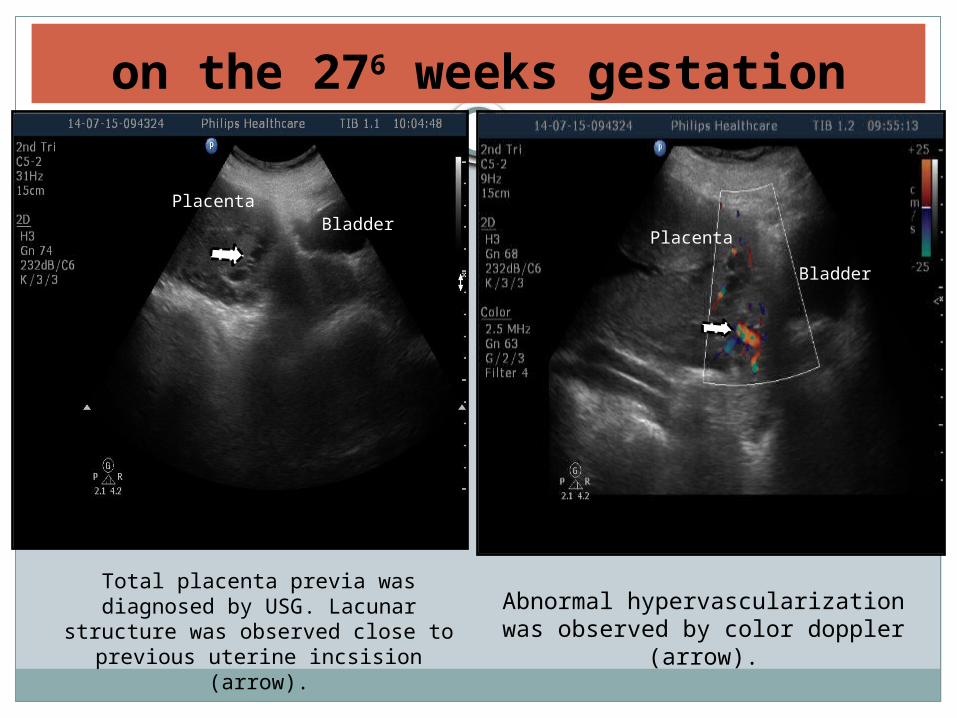
on the 276 weeks gestation
Total placenta previa was diagnosed by USG. Lacunar structure was
observed close to previous uterine incsision (arrow).
Placenta
Bladder
Abnormal hypervascularization was observed by color doppler (arrow).
PlacentaBladder
Maternal History
2006 Missed abortion (8 weeks)
2007 CS was performed due to fetal distress CS at the 383weeks,
3150 g newborn was born2009
Biochemical pregnancy 2012
CS was performed due to oligohydramniosis, 2650 g newborn was born 2014
MTHFR mutation (heterozygot), Clexan 0.4 IU
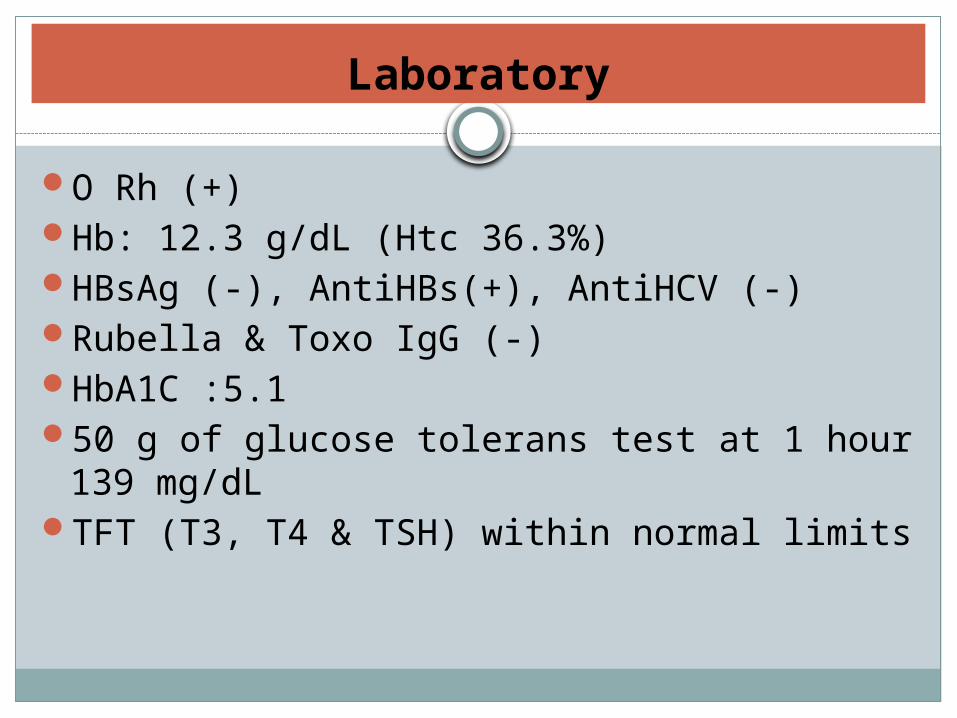
Laboratory
O Rh (+)Hb: 12.3 g/dL (Htc 36.3%)HBsAg (-), AntiHBs(+), AntiHCV (-)Rubella & Toxo IgG (-)HbA1C :5.150 g of glucose tolerans test at 1 hour 139 mg/dLTFT (T3, T4 & TSH) within normal limits
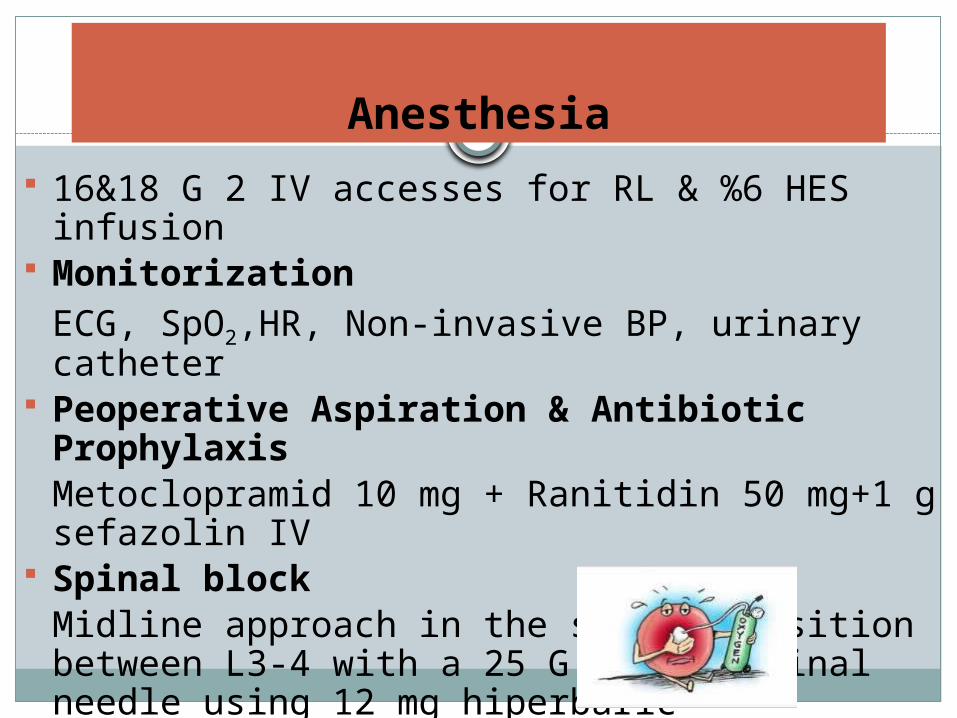
Anesthesia
16&18 G 2 IV accesses for RL & %6 HES infusion Monitorization
ECG, SpO2,HR, Non-invasive BP, urinary catheter Peoperative Aspiration & Antibiotic Prophylaxis
Metoclopramid 10 mg + Ranitidin 50 mg+1 g sefazolin IV Spinal block
Midline approach in the sitting position between L3-4 with a 25 G Pencan spinal needle using 12 mg hiperbaric bupivacaine+10 µg fentanyl+ 150 µg morphine
Operation table tilted to left 15
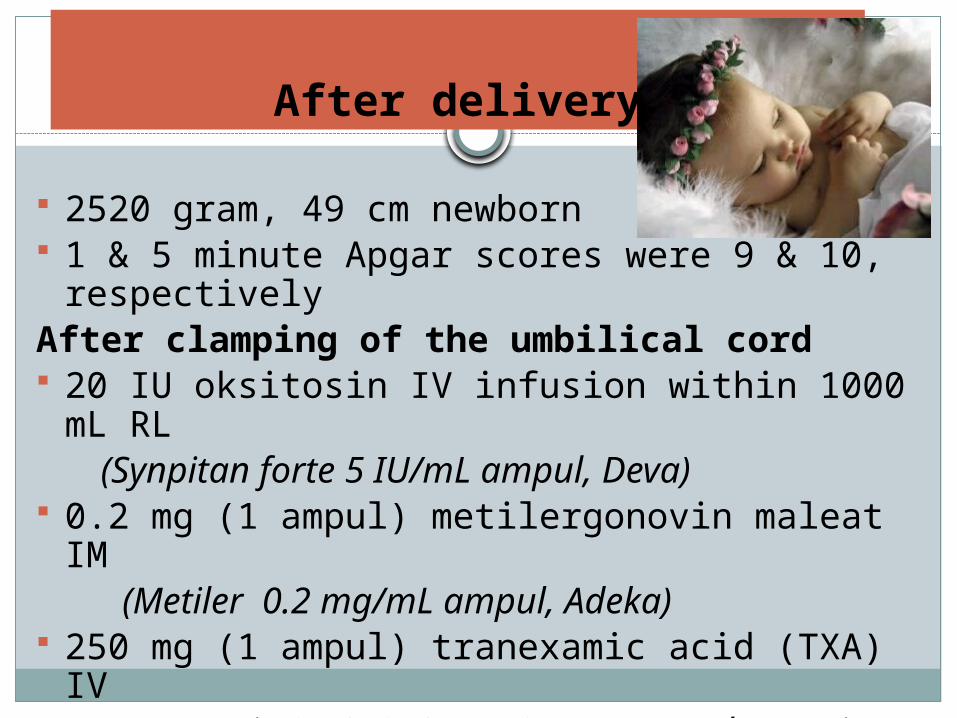
After delivery
2520 gram, 49 cm newborn 1 & 5 minute Apgar scores were 9 & 10, respectivelyAfter clamping of the umbilical cord 20 IU oksitosin IV infusion within 1000 mL RL (Synpitan forte 5 IU/mL ampul, Deva) 0.2 mg (1 ampul) metilergonovin maleat IM (Metiler 0.2 mg/mL ampul, Adeka) 250 mg (1 ampul) tranexamic acid (TXA) IV (Transamin %10, 250 mg, 2.5 mL ampul, Actavis)

Surgery
Hysterotomyfor delivery
Hysterectomy
(TAH+BSO)
Lower midline incision
After hysteretomy placenta was left in situ, anterior wall of the uterus was seen. Arrow shows the previous uterine incision and the PLACENTA INCRETA (myometrial invasion)
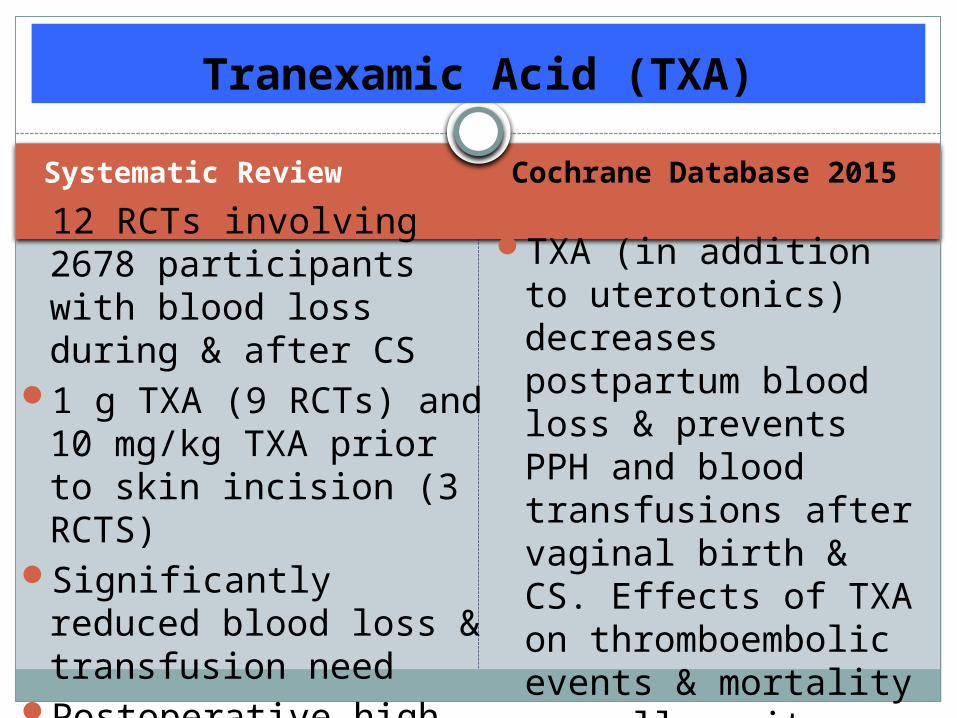
Systematic Review Cochrane Database 2015
12 RCTs involving 2678 participants with blood loss during & after CS
1 g TXA (9 RCTs) and 10 mg/kg TXA prior to skin incision (3 RCTS)
Significantly reduced blood loss & transfusion need
Postoperative high Hb levels + no serious side effects & complications
TXA (in addition to uterotonics) decreases postpartum blood loss & prevents PPH and blood transfusions after vaginal birth & CS. Effects of TXA on thromboembolic events & mortality as well as its use in high-risk women should be investigated further
Tranexamic Acid (TXA)
SUSPECTED Placenta Previa - Increta
We performed an elective cesarean delivery under spinal anesthesia at 36 weeks’ gestation and hysterectomy for our patient
According to a retrospective study, it is considered to be a traditional approach for the management of placenta accreta with a hysterectomy rate of 98%
(Obstet Gynecol 2009)We prepared 4 units of matched RBC+ 4 unıts of FFP2 large bore IV cannula were inserted CV and/or arterial lines were consideredRapid infusor devices and warmers were kept ready
Case 2. SUSPECTED Placenta Previa
GG 33 yr old, secretary, at 38 weeks gestation59 kg, 156 cm, Repeat CS with placenta previaUneventful CS under spinal anesthesiaShe was readmitted to the OR because of bleeding (Hb 4
g/dL), hypotension (60/30 mmHg) at postpartum 3 hoursGeneral anesthesia using ketamine (0.5 mg/kg) +propofol
(1 mg/kg) with rocuronium (0.6 mg/kg) 4 units of matched RBC+ FFP & 2.5 L IV ınfusionIn addition to 2 large bore IV cannula, CV and arterial
lines were placedRapid infusor devices and warmers were used
A case with placenta percrata underwent emergency CS under general anesthesia due to vaginal bleeding
Total abdominal hysterectomy + partial cystectomy were performed because of the persistent massive hemorrhage
Bleeding could be controlled after bilateral internal iliac artery embolization using a cell salvage device for stabilization of hemodynamics
Patient was discharged on the 32nd postoperative day without any major complications
Kume et al. A case of placenta percreta with massive hemorrhage during CS..J Med Invest 2014;61: 208-212
Placenta Percreta

Although national guidelines advise preoperative placement of internal iliac artery occlusion balloon catheters to reduce haemorrhage, to avoid caesarean hysterectomy and to preserve fertility, it may cause puncture-site complications, arterial thrombosis and/or ischaemic nerve injury.
Teare et al. Sciatic nerve ischaemia after iliac artery occlusion balloon catheter placement for placenta percreta. IJOA 2014;23(2):178-81
Placenta Percreta
Antenatal diagnosis
Prophylactic methods to reduce blood loss (balloon occlusion)
Take home messages
Preoperative preparation
Close team work to reduce maternal mortality & morbidity
Aggressive intervention for massive blood loss (ligation & volume replacement)

19th European Veteran Athletics Championship (EVACS) 2014
THANK YOU

















