Best in Class Agents for Global HCV Eradication Raymond F. Schinazi, PhD, DSc Frances Winship Walters Professor Director, Scientific Working Group on Viral Eradication, Emory University CFAR/VAMC University of Miami Emory Institute for Drug Discovery Boston June 27, 2013 [email protected]
Transcript
Best in Class Agents for Global HCV Eradication
Raymond F. Schinazi, PhD, DSc Frances Winship Walters Professor
Director, Scientific Working Group on Viral Eradication, Emory University CFAR/VAMC
University of Miami Emory Institute for Drug Discovery
• ~170 million infected with HCV worldwide (USA: 2.7-‐3.9 million) • Six different genotypes worldwide • Chronic disease leads to liver cirrhosis and cancer • No latency – hence curable • Virus dynamic
• Standard of care: Ribavirin + peg-‐INF-‐α + Protease Inhibitors – Treatment complicated – coinfecUon even more complicated – Side effects, subopUmal efficacy, genotype-‐dependent, injectable
• Oral, direct acUng anUvirals (DAA): – NS5B, Entry, Protease, NS5A, Cyclophilins, microRNA, etc.
• Nucleoside Analog Inhibitors (NAI) are Best in Class: – High potency – Pan-‐genotypic – High barrier to resistance – Low pill burden and orally bioavailable
• 2
Ultimate Goal For HCV Therapy One size fits all
♦ Once a day oral Rx - Easier for doctors & patients
♦ Pan-genotypic ♦ No clinical resistance ♦ No response guided therapy ♦ Short duration – 12 weeks or less ♦ Safe with no or manageable side effects ♦ High cure rates - Lowers cost to healthcare ♦ Suitable for all populations at low cost
In a 28 day Phase IIa clinical study of genotype 1 treatment-naïve HCV patients dosed in combination with peg IFN/RBV at 100 mg, 200 mg, and 400 mg: RVR rates of 88%, 94%, and 93% respectively. 14 day monotherapy of genotype 1 treatment-naïve HCV patients showed an average of -5.0 log10 decline in viral load with 88% of patients reaching undetectability (<15 IU/mL) after 14 days.
OPO
NH
CH3O
O CH3FHO
NNH
OOH3C
CH3O
O
Diastereomericaly Pure Nucleotide Phosphoramidates for HCV*
• *Summarized in part from: 1) J Org Chem. 2011 Sep 14. [Epub ahead of print], Synthesis of Diastereomerically Pure Nucleotide Phosphoramidates. Ross BS, Reddy PG, Zhang HR, Rachakonda S, Sofia MJ.; 2) J. Med. Chem. 2010, 53, 7202-7218, Discovery of a β-D-2-Deoxy-2-α-fluoro-2-β-C-methyluridine Nucleotide Prodrug (PSI-7977) for the Treatment of Hepatitis C Virus. Sofia MJ, Bao D., Chang W, et al. and Antivir. Chem. Chemoth. 2011, 22, 23-49, Nucleotide prodrugs for HCV therapy. Sofia MJ.
§ Sofosbuvir + GS-‐5885 + RBV (Gilead) (G2 and G3)
§ Asunaprevir + daclastavir + BMS-‐791325 (BMS)
Inter/Intra-Company Combinations Good Example: Two Molecules QD
(Truvada-like for HCV)
GILD/PSI Sofosbuvir nuc
(GS-7977; 400 mg QD)
BI-201335 PI or TMC-435 PI
(120 mg or 75 mg QD)
Bristol Myers Squibb NS5A inhibitor
(BMS-790052; Daclatasvir 20 mg QD)
Gilead NS5A inhibitors
(GILD-5885 or 5816; 25-100 mg QD)
AASLD 2012: 7977+5885+ Riba = 100% SVR4
v Assuming Sofosbuvir (PSI/GS-7977) is approved by Q4 2013; new IND are behind by < 3 years.
v Gilead may be able to treat at most half a million people per year. With only 1.5 – 2 MM people treated over 3 yrs, there is still majority of the world and US market available.
v > 60 MM people who can pay will be available for treatment
v No pan-genotypic regimen has advanced to Phase 3. No effective combo for cirrhotic yet
The Game is not over
• 16
Several unmet needs remain: • DAA/PR failures – DONE • Null-responders – DONE • Co-infected with HIV or HBV – ALMOST DONE • non-GT1, especially GT3 – DONE • IFN intolerant or contraindicated - DONE • Cirrhosis • Bleeding disorders (hemolysis) • Pediatrics & transplant subjects • Opiate substitution therapy Too few Tx persons to come to any definitive conclusion – Real World
There are still other opportunity: Shift in focus to difficult to treat persons
Adapted from A. Kwang
Three Waves of DAA Treatments with Sofosbuvir Leading to Cure Tsunamis
• Sofosbuvir as a single DAA plus Riba • Sofosbuvir/NS5a or PI for genotype 1
• Final regimen, short in duration, one size fits all that is pangenotypic and SVR rates > 90% in the real world (nuc as backbone + PI/NS5a or two nucs or perhaps one v potent nuc).
19
One prodrug provides two active metabolites that are incorporated by HCV polymerase as G- and A-like NTP analogs.
Inhibition of NS5B and
Chain Termination!
TP 2’-C-Me-G
DAPN-PD1
TP DAPN
Novel Multi-metabolite Prodrug Approach for HCV Inhibition
Conclusions • DAPN prodrugs represent new investigational compounds against HCV • Potent and non-toxic in several cell culture systems
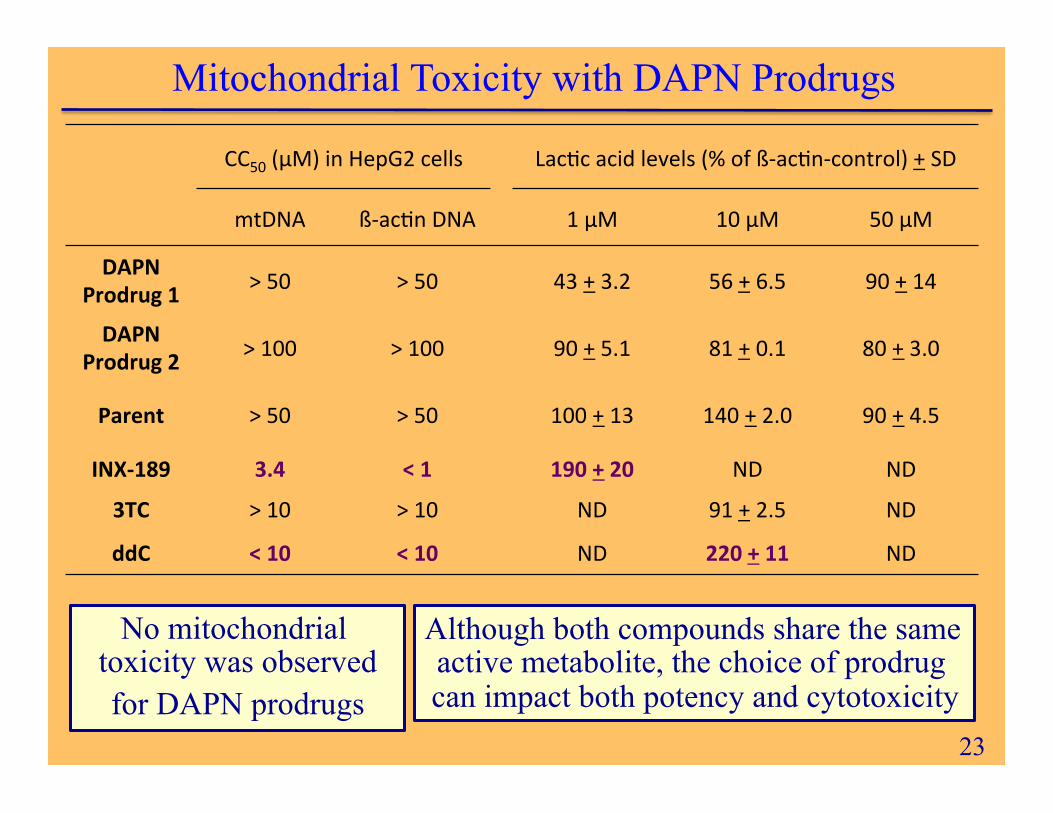
§ Novel prodrug produced non-toxic metabolite (food additive) § No mitochondrial toxicity or lactic acid increase (below 100) § Choice of prodrug reduces cytotoxicity when compared to INX-189
• Two active metabolites were observed intracellularly:
§ Prodrug group may modulate ratio of active metabolites § 2’-C-methyl-GTP metabolite acts as a G analog § DAPN-TP metabolite acts as an A analog § Combined delivery of nucleotide analogs with different viral RNA
incorporation profiles – may be synergistic and prevent selection of mutant viruses
§ Advanced toxicological studies with a DAPN prodrug is proceeding towards an IND in 1Q2014
• 24
DAPN-PD Additional Highlights
v DAPN-PDs exhibit prolonged stability in gut (SGF) and intestine (SIF) similar to GS-7977.
v In human microsomes, DAPN-PD rapidly metabolized suggesting high liver exposure.
v DAPN-PD2 is a more lipophilic and more metabolically stable follow-up prodrug of DAPN-PD1. It has similar potency to DAPN-PD1 in the HCV 1b replicon assay with no toxicity in Huh-7, CEM, human PBM, or Vero cells.
v The phosphorous diastereomers of DAPN-PD2 are equipotent in vitro; thus, no need to separate diastereomers resulting in >significant cost savings in manufacturing.
v 1 kg of non-GMP DAPN-PD1 and DAPN-PD2 parent nucleoside prepared (97.4% pure).
v Extensive exploration of nucleoside prodrugs and unique IP portfolio.
….The US and EU are Only ~15% (11 MM) of the Total Worldwide HCV Population (170 MM)