Page 1
Best of the Best in
Pediatrics
Recent Articles You’ve Got
to Know!
Mimi Lu, MD, FAAEM Clinical Assistant Professor
Assistant Residency Program Director
Director, Pediatric Emergency Medicine Education
University of Maryland School of Medicine
Baltimore, Maryland
Page 2
No relevant financial disclosures
Page 3
Outline Recent literature pertaining to
Fever
Bronchiolitis
Sedation
Questions? [email protected]
For a PDF copy of all slides, go to:
lectures.umem.org/AAEM [will be posted after AAEM for 1 month]
Page 6
Case: the febrile infant
18 day boy felt “warm” at home
◦ ROS negative
◦ T = 38.4 ºC rectal
◦Well-appearing
◦ unremarkable physical exam
9 week 9 month girl
39.4
Page 8
Infant Fever
Work-up:
Page 9
Infant Fever Work-up: ABC’s
• Full sepsis evaluation:
– Analysis of urine (UA, UCx)
– Blood (CBCD, BCx)
– CSF (cell count, protein, glucose, GS/Cx)
– ± CXR
– ± Antibiotics
Page 10
Rochester
Philadelphia
Boston
Page 11
Boston Philadelphia Rochester
Age (days) 28-89 29-56 0-60
Temp (0C) > 38.0 > 38.0 > 38.0
Infant Obs. Score Yes Yes No
Peripheral WBC < 20,000 < 15,000 5-15,000
CSF obtained Yes Yes No
Antibiotic given Yes No No
SBI in low risk pts (%) 5.4 0 1.1
NPV (%) 94.6 100 98.9
Sensitivity (%) Not stated 100 92.4
Component of fever protocols
Avner, Emerg Med Clin North Am, 2002
Page 12
UCx
UA
BCx
CBC
CSF
admit
UCx
UA
BCx
CBC
CSF
UCx
UA
BCx
CBC
UCx
UA
BCx
UCx
UA
Page 13
UCx
UA
BCx
CBC
CSF
admit
UCx
UA
BCx
CBC
CSF
UCx
UA
Future….
Viral tests?
Inflam markers?
Page 16
Changing epidemiology
Greenhow, Pediatr Infect Dis J, 2014
Population study
◦ Impact of prenatal screen and immunizations
SBI < 90 days
◦ 13% overall incidience
◦ 92% SBI are UTI
No Listeria or meningococcus
Page 17
Greenhow, 2014
Clinical appearance, WBC: poor predictors
Page 18
Greenhow, 2014
Table 3: Bacterial Pathogens Detected in 129 Blood, 823 Urine and 16 CSF cultures
Greenhow et al, Pediatr Infect Dis J, 2014
Page 19
Listeria in neonates
Hassoun et al, Pediatr Emerg Care, 2014
Epidemiology and ampicillin sensitivity of
listeria and enterococcal infections
2 center retrospective review, 2006-2010
1192 neonates
Page 20
Listeria in neonates
Results
6% SBI
◦ 1/1192 (0.08%) enterococcal bacteremia
◦ 1/1192 (0.08%) listeria bacteremia
◦ 15/1192 (1.4%) enterococcal UTI
◦ UA less helpful for enterococcal UTI vs E coli
◦ Increasing resistance to ampicillin
Page 21
Listeria in neonates
Conclusion:
Listeria is uncommon cause of neonatal
SBI in febrile neonates presenting to ED
Empiric use of ampicillin may need to be
reconsidered
Page 22
Occult bacteremia
Hernandez-Bou, Acta Paediatr, 2015
Rate of bacteremia after 13-valent
pneumococcal conjugated vaccine
591 pts, 3 mo to 36 mo
1% bacteremia, 2.7% contamination
Page 23
Occult bacteremia
Conclusion
Occult bacteraemia is an uncommon
event in well-appearing febrile children
aged three to 36 months
Close follow-up should replace blood
analysis
Page 24
The $$ is in the pee!!!
AAP Clinical Practice Guideline, 2011
Page 25
UTI
Frumkin, J Emerg Med, 2014
Retrospective observational 5 year study
4403 urine cultures
Age 0-36 months
Boys: cultured less but higher positive culture rate; more gram-positive organisms
TMX/SMP and amoxicillin/clavulanic acid effective against all isolates
Page 26
UTI and Bacteremia
Schnadower et al, Pediatrics, 2010
PECARN retrospective review
29-60 day infants with UTI
Conclusion
Low risk: adverse events and bacteremia
Consider brief hospitalization or
outpatient management
Page 27
UTI and Bacteremia
Averbuch, Pediatr Infect Dis J, 2014
Hernandez-Bou, Pediatr Infect Dis J, 2014
Conclusion
Afebrile young infant with UTI still at risk
for bacteremia
Well-appearing infants with UTI with PCT
< 0.7 ng/ml at very low risk bacteremia
Page 28
UTI and Meningitis
Paquette, Pediatr Emer Care, 2011
Tebruegge, PLoS One, 2011
Greenhow, Pediatr Infect Dis, 2014
Risk of co-existing UTI and meningitis is
small (except neonates!). More selective
approach warranted.
Page 29
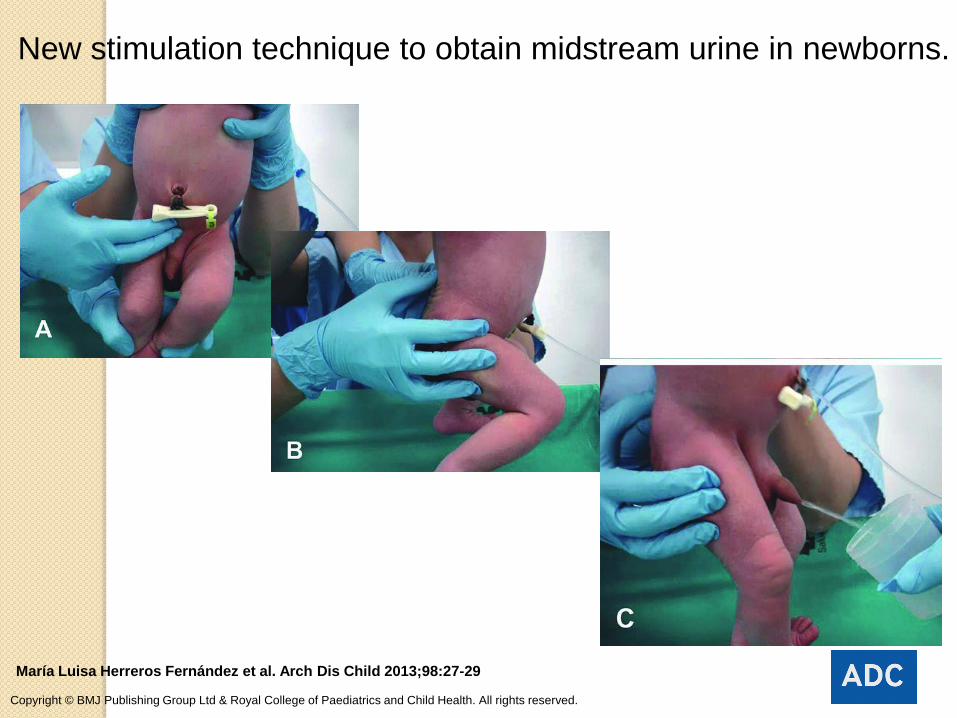
New stimulation technique to obtain midstream urine in newborns.
María Luisa Herreros Fernández et al. Arch Dis Child 2013;98:27-29
Copyright © BMJ Publishing Group Ltd & Royal College of Paediatrics and Child Health. All rights reserved.
Page 30
UCx
UA
BCx
CBC
CSF
admit
UCx
UA
BCx
CBC
CSF
UCx
UA
Future….
Viral tests?
Inflam markers?
Page 31
Inflammatory markers
White Blood Cell (WBC)
Absolute Neutrophil Count (ANC)
C Reactive Protein (CRP)
Procalcitonin (PCT)
Page 32
© 2007 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 5
FIGURE 2 . ROC for PCT, CRP, WBC count, and ANC for prediction of SBI.
Andreola, Pediatr Infect Dis J, 2007
Page 33
WBC and height of fever inaccurate
predictors of SBI in infants 3-24 months.
Fever and White Count
Rudinsky, Acad Emerg Med, 2009
De et al, Arch Dis Child, 2014
Greenhow, Pediatr Infect Dis J, 2014
Page 34
CRP and PCT
CRP and PCT strong predictors of SBI
Nijman, Pediatr Infect Dis J, 2014
Segal et al, Arch Dis Child, 2014
Page 35
Procalcitonin
Pierce, Curr Opin Pediatr, 2014
Review of diagnostic and prognostic utility
of PCT in children
England, J Emerg Med, 2014
Meta-analysis of febrile infants <90 days
Page 36
Procalcitonin and SBI
Mahajan et al, Acad Emerg Med, 2014
Prospective multicenter study
226 febrile children < 36 months
13.3% SBI
Conclusion
Procalcitonin more accurate biomarker for identifying young febrile infants and children with SBIs
Page 37
RSV and SBI risk
RSV positive RSV negative
Any SBI 17/244 7% (4.1%-10.9%)
116/925 12.5% (10.5%-14.8%)
UTI 14/261 5.4% (3.0%-8.8%)
98/966 10.1% (8.3%-12.2%)
Bacteremia 3/267 1.1% (0.2%-3.2%)
22/968 2.3% (1.4%-3.4%)
Meningitis 0/251 0% (0%-1.2%)
8/938 0.9% (0.4%-1.7%)
Levine, Pediatrics, 2004
Page 38
Conclusion: Febrile infants with bronchiolitis
have lower risk of SBI … but check for UTI
Bronchiolitis and SBI risk
Melendez and Harper, 2003
Levine, 2004
Titus and Wright, 2003
Ralston, 2011
Page 39
Influenza and SBI risk
Influenza + (N = 123) Influenza - (N = 721)
Any SBI 3/119 2.5% (0.5%-7.2%)
92/690 13.3% (10.9%-16.1%)
UTI 3/123 2.4% (0.5%-6.9%)
77/712 10.8% (8.6%-13.3%)
Bacteremia 0/123 0% (0%-2.4%)
16/715 2.2% (1.3%-3.6%)
Meningitis 0/119 0% (0%-2.5%)
6/698 0.9% (0.3%-1.9%)
Enteritis 0/3 0% (0%-56.2%)
1/60 1.7% (0.3-8.9%)
Krief, Pediatrics, 2009
Page 40
Fever: sources decreasing SBI risk
Focal bacterial infection
◦ AOM, cellulitis
Named viral infection
◦ Bronchiolitis, croup
◦ Infant < 3 months: still consider UTI
◦ Infant > 3 months: SBI/UTI unlikely
Page 41
Summary
OUT with the
and IN with the
Page 42
UCx
UA
BCx
CBC
CSF
admit
UCx
UA
BCx
CBC
CSF
UCx
UA
Future….
Viral tests?
Inflam markers?
Page 44
Clinical Practice Guideline
Diagnosis
Based on H&P
No routine labs or radiographs
Risk factors:
◦ age < 12 weeks, prematurity, underlying CP
disease, immunodeficiency
Ralston et al, Pediatrics, 2014
Page 45
Clinical Practice Guideline
Treatment
Albuterol?
Epinephrine?
Steroids?
Hypertonic saline?
Ralston et al, Pediatrics, 2014
Page 46
Clinical Practice Guideline
Treatment
Supplemental oxygen?
Continuous pulse oximetry?
Antibiotics?
Fluids?
Ralston et al, Pediatrics, 2014
Page 47
Oximetry in bronchiolitis
Schuh et al, JAMA, 2014
Randomized, double-blind, parallel group
2008 to 2013
213 healthy infants 4 wks to 12 mo
Mild to moderate bronchiolitis
Page 48
Oximetry in bronchiolitis
Results
Hospitalization rates using true saturation vs altered display (41% vs 25%)
No difference: use of supplemental oxygen, LOS ED, unscheduled visits within 72 hrs
Conclusion
Oxygen saturation should not be only factor in decision, to admit; may need to re-evaluate its use
Page 49
HFNC on Wards?
Mayfield et al, J Paediatr Child Health, 2014
Prospective pilot study
Safety and impact on ward
Responders identified within 60 minutes
HFNC 4 times less likely to need PICU
No adverse events
Conclusion:
HFNC treatment on the paediatric ward is safe
Page 50
HFNC vs nCPAP
Metge et al, Eur J Pediatr, 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR, HR, FiO2, CO2 in management of severe bronchiolitis in PICU
Page 51
Summary so far…
Out with the “L”, in with the “P”
Continued supportive care with
bronchiolitis
Early intervention with HFNC or NIPPV
Page 53
Ideal sedative agent(s)
Safe
Easy to administer
Effective and predictable
Rapid onset of action
Rapid recovery
Minimal adverse effects
Page 54
Sedative agents
Ketamine
Midazolam
Morphine
Fentanyl
Meperidine
Methohexital
Clonidine
Propofol
Etomidate
Dexmedetomidine
Diphenhydramine
Chloral hydrate
Pentobarbital
Page 55
Ketamine
Reliable
Dissociative agent
Amnesia
Analgesic properties
Favorable safety profile
Page 56
Ketamine
Hypertension
Tachycardia
Prolonged recovery period
Emergence reaction
Laryngospasm
Emesis
Page 57
Ketamine
Kinder et al, Pediatr Emerg Care, 2012
◦ Higher BMI associated with higher risk of
vomiting
Street,and Gerard, J Pediatr, 2014
◦ Fixed dose ketamine
Chinta et al, Ann Emerg Med, 2015
◦ Rapid administration
Page 58
Sedative-hypnotic agent
Rapid onset
Rapid recovery
Short duration of action
Amnestic properties
Antiemetic
Propofol
Page 59
Propofol
No analgesia
Transient hypotension
Dose-dependent respiratory depression
Bradycardia
Hypoxia
Page 61
Ketamine-Propofol
Analgesic/ anesthetic synergy
◦ Reduced total dose required of each agent
◦ Less toxicity
Complementary effects
◦ Sympathomimetic effects counter
hemodynamic depression
◦ Analgesic effects of ketamine
◦ Antiemetic effects of propofol
Sharieff, Peds Emerg Care, 2007
Shah, Ann Emerg Med, 2011
Alletag, Pediatr Emerg Care, 2012
Page 63
Dexmedetomidine
Highly selective alpha agonist
Adjunctive agent for sedation and sedation
Rapid recovery
Safe
Effective
Phan and Nahata, Paediatr Drugs, 2008
Teshome et al, Hosp Pediatr, 2014
Sheta et al, Paediatr Anesth, 2014
Yuen et al, Anesth Analg, 2014
Pasin et al, Paediatri Anesth, 2015
Page 64
Nitrous oxide
Pasaron et al, Pediatr Surg Int, 2015
Provides safe sedation and amnesia
Decreased pain and anxiety
No fasting or postoperative monitoring
Page 65
Inhaled nitrous oxide vs IV ketamine
Lee, Pediatr Emeg Care, 2012
Prospective randomized study
Results for nitrous oxide:
◦ Less total sedation time
◦ Less recovery time
◦ Longer induction times
◦ Lower sedation level
◦ Comparable pain scales and satisfaction
Page 66
iNO vs ketamine
Conclusion:
Nitrous oxide inhalation was preferable
to injectable ketamine
Safe, faster recovery, maintains sufficient
sedation time, and does not induce
unnecessarily deep sedation.
Page 67
Del Pizzo and Callahan, Pediatr Emerg Care, 2014
Page 68
Intranasal ketamine
Tsze et al, Pediatr Emerg Care, 2012
Andolfatto et al, Acad Emerg Med, 2013
Nielsen et al, Paediatr Anesth, 2014
Graudins et al, Ann Emerg Med, 2015
PICHFORK Trial
Page 69
Comparison?
Surendar, J Clin Pediatr Dent, 2014
◦ Triple blind randomized study
◦ Intranasal dexmedetomidine, midazolam and
ketamine for their sedative and analgesic
properties: a triple blind randomized study.
Conclusion:
◦ All study drugs can be used safely and
effectively through IN route
Page 71
Withdrawl of OTC CCM
Alternatives:
◦ Fluids
◦ Humidified air?
◦ NSAIDS?
◦ Anti-histamines?
◦ Echinacea
◦ Zinc
◦ Honey
◦ Vitamin C?
2.5 mL qhs (>1 year of age)
Page 72
Summary
Fever
◦ Decrease: Listeria and LPs
◦ Increase: Urine cultures, Procalcitonin
Bronchiolitis
◦ Continued supportive care
◦ High flow nasal cannula
Sedation
◦ Dexmedetomidine
◦ Intranasal meds
Page 73
Questions?
[email protected]
For a PDF copy of all slides, go to:
lectures.umem.org/AAEM [will be posted after AAEM for 1 month]

















































































![Welcome! [meded.ucsf.edu] - UCSF Medical Education · PDF fileWelcome! Carolyn Bradner Jasik, MD . Assistant Professor of Pediatrics . Assistant Medical Director of Informatics . UCSF](https://static.documents.pub/doc/80x56/5aa6e2617f8b9a54748b4f30/welcome-mededucsfedu-ucsf-medical-education-carolyn-bradner-jasik-md-assistant.jpg)


